Embed Size (px)
Citation preview

NEW GUIDELINES
ON NUTRITIONAL
INTERVENTION IN THE ICU —
ASPEN, ESPEN OR LOCAL?
Mirosław Czuczwar
II Department of Anesthesiology and Intensive Therapy

DISCLOSURE
I have received honoraria for lectures and advisory groups on enteral and parenteral nutrition from the following pharmaceutical companies:
B Braun
Baxter
Fresenius Kabi
Nestle
Nutricia


Initial resuscitation protocole milestones:
Sepsis and septic shock are medical emergencies and we
recommend that treatment and resuscitation begin immediately
Specific anatomic diagnosis of infection requiring emergent source
control be identified or excluded as rapidly as possible
Administration of IV antimicrobials should be initiated as soon as
possible after recognition and within 1 h for both sepsis and septic
shock
In the resuscitation from sepsis-induced hypoperfusion, at least
30ml/kg of intravenous crystalloid fluid be given within the first 3
hours
Using albumin in addition to crystalloids when patients require
substantial amounts of crystalloids
SURVIVING SEPSIS CAMPAIGN
GUIDELINES

We recommend against the administration of early parenteral
nutrition alone or parenteral nutrition in combination with enteral
feedings (but rather initiate early enteral nutrition) in critically ill
patients with sepsis or septic shock who can be fed enterally
We recommend against the administration of parenteral nutrition
alone or in combination with enteral feeds (but rather to initiate IV
glucose and advance enteral feeds as tolerated) over the first 7 days
in critically ill patients with sepsis or septic shock in whom early
enteral feeding is not feasible
We suggest the early initiation of enteral feeding rather than a
complete fast or only IV glucose in critically ill patients with sepsis or
septic shock who can be fed enterally
SURVIVING SEPSIS CAMPAIGN
GUIDELINES - NUTRITIONAL SUPPORT

We suggest the use of prokinetic
agents in critically ill patients with
sepsis or septic shock and feeding
intolerance
We suggest against routinely
monitoring gastric residual volumes in
critically ill patients with sepsis or
septic shock
SURVIVING SEPSIS CAMPAIGN
GUIDELINES - NUTRITIONAL SUPPORT

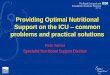
SEPSIS ASSOCIATED MORTALITY
Copyright 2014 American Medical Association. All rights reserved.
Figure1. Mean Annual Mortality in PatientsWith SevereSepsis
40
35
30
25
20
15
10
5
0
No. of patients
Mort
alit
y, %
Year
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 20112010 2012
2708 3783 4668 5221 6375 6987 7627 8529 8797 10 277 12 21311 367 12 512
Error bars indicate95% CI.
Table2. Mortality Rate Among SevereSepsisPatientsOverall and Within Subgroupsin 2000 and 2012a
2000 2012 Risk Reduction
No. ofEvents
No. ofPatients
Mortality, %(95%CI)
No. ofEvents
No. ofPatients
Mortality, %(95%CI) Absolute Relative
All patientswith severesepsis 949 2708 35.0 (33.2-36.8) 2300 12 512 18.4 (17.8-19.0) 16.7 (14.8-18.6) 47.5 (44.1-50.8)
Without comorbiditiesb 529 1800 29.4 (27.2-31.6) 1136 8110 14.0 (13.2-14.8) 15.4 (13.2-17.7) 52.3 (47.9-56.4)
With comorbiditiesb 420 908 46.3 (43.0-49.6) 1164 4402 26.4 (25.0-27.8) 19.8 (16.3-23.3) 42.8 (37.7-47.5)
Severesepsiswithout shock 426 1411 30.2 (27.8-32.6) 815 5755 14.2 (13.2-15.2) 16.0 (13.5-18.6) 53.1 (48.1-57.6)
Septic shock 523 1297 40.3 (37.6-43.0) 1485 6757 22.0 (21.0-23.0) 18.3 (15.5-21.2) 45.5 (41.0-49.7)
Medical admissions 784 2052 38.2 (36.0-40.4) 1959 9824 19.9 (19.1-20.7) 18.3 (16.0-20.5) 47.8 (44.1-51.2)
Surgical admissions 165 656 25.2 (21.9-28.5) 341 2688 12.7 (11.5-13.9) 12.5 (9.0-16.1) 49.6 (40.5-57.2)
Respiratory failurec 652 1642 39.7 (37.3-42.1) 1106 4603 24.0 (22.8-25.2) 15.7 (13.0-18.4) 39.5 (34.5-44.1)
Acute renal failured 445 805 55.3 (51.8-58.8) 1069 3100 34.5 (32.7-36.3) 20.8 (17.0-24.6) 37.6 (32.5-42.3)
APACHEscore
II <25 370 1679 22.0 (20.0-24.0) 1079 9537 11.3 (10.7-11.9) 10.7 (8.7-12.9) 48.7 (42.9-53.8)
II ≥25 554 942 58.8 (55.7-61.9) 1177 2732 43.1 (41.3-44.9) 15.7 (12.0-19.3) 26.7 (21.5-31.6)
III Q1 47 498 9.4 (6.9-11.9) 77 3486 2.2 (1.8-2.6) 7.2 (4.9-10.1) 76.6 (66.8-83.5)
III Q2 103 544 18.9 (15.6-22.2) 317 3254 9.7 (8.7-10.7) 9.2 (5.9-12.8) 48.5 (37.0-58.0)
III Q3 215 607 35.4 (31.7-39.1) 634 3149 20.1 (18.7-21.5) 15.3 (11.3-19.4) 43.2 (35.4-50.0)
III Q4 498 819 60.8 (57.5-64.1) 1258 2591 48.6 (46.6-50.6) 12.3 (8.4-16.1) 20.2 (14.6-25.4)
Age, y
≤44 98 443 22.1 (18.2-26.0) 130 1778 7.3 (6.1-8.5) 14.8 (11.0-19.1) 66.9 (58.0-74.0)
45-64 226 742 30.5 (27.2-33.8) 524 3660 14.3 (13.1-15.5) 16.1 (12.7-19.7) 53.0 (46.2-58.9)
65-84 537 1326 40.5 (38.0-43.0) 1260 5806 21.7 (20.7-22.7) 18.8 (16.0-21.7) 46.4 (41.9-50.6)
≥85 88 197 44.7 (37.6-51.8) 386 1268 30.4 (27.9-32.9) 14.2 (7.0-21.6) 31.9 (18.7-42.9)
Sepsis
Other than urinary tract origin 131 412 31.8 (27.3-36.3) 470 2770 17.0 (15.6-18.4) 14.8 (10.3-19.7) 46.6 (37.1-54.7)
Urinary tract origin 26 113 23.0 (15.2-30.8) 66 982 6.7 (5.1-8.3) 16.3 (9.3-25.0) 70.8 (56.0-80.6)
With shock, other than urinary tract 365 747 48.9 (45.4-52.4) 703 2419 29.1 (27.3-30.9) 19.8 (15.8-23.8) 40.5 (34.5-46.0)
Urinary tract origin with shock 26 93 28.0 (18.8-37.2) 104 686 15.2 (12.5-17.9) 12.8 (4.2-23.0) 45.8 (21.4-62.6)
Abbreviations:APACHE,AcutePhysiologyandChronicHealthEvaluation;Q,quartile.
a Therisk reduction from 2000 to 2012 wasstatistically significant for all
categories: P< .001.
b Comorbidityasdefinedby theAPACHEII23or APACHEIII24 classificationsystem.
c Respiratory failurewasdefined by mechanical ventilation and intubation.
d Acute renal failurewasdefined by highest creatinine 3.39 mg/dLor urine
output <410 mL/24 h or all of the following: urine output <410 mL/24 h and
creatinine 1.50 mg/dLand no long-term dialysis.
Research Original Investigation Mortality Related to SevereSepsisand Septic Shock
1312 JAMA April 2, 2014 Volume 311, Number 13 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by M iroslaw Czuczwar on 01/31/2016

MORTALITY IN SEPSIS AND SEPTIC
SHOCK
Figure 1. Immunoinflammatory response of three hypothetical patients with sepsis
The individual immune response in sepsis is determined by many factors including pathogen
virulence characteristics, size of the bacterial inoculum, patient comorbidities, etc. The
initial immune response is hyperinflammatory but the response rapidly progresses to
hypoinflammatory. In the healthy individual who develops meningococcemia, there is a
robust hyperinflammatory response. Death may occur rapidly due to a hyperinflammatory
state and, antiinflammatory treatments may improve survival. If infection resolves, there is
only a minimal hypoimmune state. In the elderly patient with malnutrition who develops
diverticulitis, the initial response is limited and, if the infection persists, a prolonged
hypoinflammatory response develops followed by recovery or death. In the patient with
diabetes, chronic renal failure, and pneumonia, the initial response is blunted and there is a
prolonged depression of immune function. (Modified with permission from N Eng J Med
2003; 348:138–50)
Skrupky et al. Page 21
Anesthesiology. Author manuscript; available in PMC 2012 December 01.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
t
Advances in the Management of Sepsis and in the
Understanding of Key Immunologic Defects of the Disorder
Lee P. Skrupky, Pharm.D., B.C.P.S.*, Paul W. Kerby, M.B B.S.†, and Richard S. Hotchkiss,
M.D.‡
*Clinical Pharmacist, Barnes Jewish Hospital, Department of Anesthesiology and Critical Care,
Washington University School of Medicine; St Louis, MissouriFrom the Department of
Anesthesiology, Washington University School of Medicine
†Fellow, Department of Anesthesiology and Critical Care, Washington University School of
Medicine; St Louis, MissouriFrom the Department of Anesthesiology, Washington University
School of Medicine
‡Professor, Department of Anesthesiology and Critical Care, Washington University School of
Medicine; St Louis, MissouriFrom the Department of Anesthesiology, Washington University
School of Medicine
Abstract
Anesthesiologists are increasingly confronting the difficult problem of management of patients
with sepsis both in the operating room and in the intensive care unit. Sepsis occurs in over 750,000
patients in the United States annually and is responsible for more than 210,000 deaths.
Approximately 40% of all intensive care unit patients either have sepsis on admission to the
intensive care unit or develop sepsis during their stay in the intensive care unit. There have been
significant advances in both understanding of the pathophysiology of the disorder as well as in
therapy. Although deaths due to sepsis remain stubbornly high, new treatment algorithms have
lead to a reduction in overall mortality. Thus, it is important for anesthesiologists and critical care
practitioners to be aware of these new therapeutic regimens. The goal of this review is to include
both practical points on important advances in current therapy of sepsis as well as provide a vision
of future new immunotherapeutic approaches.
Introduction
Advances in Understanding the Host Immunologic Response in Sepsis
Sepsis is defined as the systemic inflammatory response that occurs during severe
infection.1–4 Severe sepsis is the syndrome of sepsis that is complicated by the development
of organ failure.5–7 Patients with sepsis often present in dramatic fashion with high spiking
fevers, shock, and respiratory failure.2–7 Due in part to this striking presentation, the
prevailing theory of sepsis for many years had been that sepsis represented an uncontrolled
inflammatory response.5,6 Lewis Thomas popularized this concept when he hypothesized
that it was the host response rather than the microorganisms that were most responsible for
the morbidity and mortality of the disorder. As he conjectured: “the microorganisms that
seem to have it in for us turn out to be more like bystanders …. It is our response to their
presence that makes the disease. Our arsenals for fighting off bacteria are so powerful …that
we are more in danger from them than the invaders .”8 The discovery of a number of potent
Address correspondence to: Dr. Hotchkiss: Department of Anesthesiology, Washington University School of Medicine, Campus Box8054, 660 South Euclid, St. Louis, Missouri 63110. [email protected]; Phone: 314-362-8560; Fax: 314-362-8571.
NIH Public AccessAuthor ManuscriptAnesthesiology. Author manuscript; available in PMC 2012 December 01.
Published in final edited form as:
Anesthesiology. 2011 December ; 115(6): 1349–1362. doi:10.1097/ALN.0b013e31823422e8.
NIH
-PA
Au
tho
r Ma
nu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t

Clinical Nutrit ion (2006) 25, 210–223
ESPEN GUIDELINES
ESPEN Guidelines on Enteral Nutrit ion:
Intensive care$
K.G. Kreymanna, , M.M. Bergerb, N.E.P. Deutzc, M. Hiesmayrd, P. Jolliet e,G. Kazandj ievf, G. Nitenbergg, G. van den Bergheh, J. Wernermani,DGEM:$ $ C. Ebner, W. Hart l, C. Heymann, C. Spies
aDepartment of Intensive Care Medicine, Universit y Hospit al Eppendorf , Hamburg, GermanybSoins Intensifs Chirurgicaux et Cent re des Brules, Cent re Hospital ier Universit aire Vaudois (CHUV)-BH
08.660, Lausanne, Swit zerlandcDepartment of Surgery, Maast r icht Universit y, Maast richt , The NetherlandsdDepart ment of Anaesthesiology and Intensive Care, Medical Universit y of Vienna, Vienna, Aust riaeDepartment of Intensive Care, Universit y Hospit al Geneva, Geneva, Swit zerlandfDepart ment of Anaesthesiology and Intensive Care, Mil i t ary Medical Universit y, Sofia, BulgariagDepart ment of Anaesthesia, Intensive Care and Infect ious Diseases, Inst i t ut Gust ave-Roussy,
Vil lej uif , FrancehDepartment of Intensive Care Medicine, Universit y Hospit al Gasthuisberg, Leuven, BelgiumiDepart ment of Anaesthesiology and Intensive Care Medicine, Karolinska Universit y Hospit al, Huddinge,
Stockholm, Sweden
Received 20 January 2006; accepted 20 January 2006
KEYWORDSGuideline;
Clinical pract ice;
Evidence-based;
Enteral nut rit ion;
Tube feeding;
Oral nut rit ional sup-
plements;
Parenteral nut rit ion;
Immune-modulat ing
nut rit ion;
Summary Enteral nut rit ion (EN) via tube feeding is, today, the preferred way of
feeding the crit ically ill pat ient and an important means of counteract ing for the
catabolic state induced by severe diseases. These guidelines are intended to give
evidence-based recommendat ions for the use of EN in pat ients who have a
complicated course during their ICU stay, focusing part icularly on those who develop
a severe inflammatory response, i.e. pat ients who have failure of at least one organ
during their ICU stay.
These guidelines were developed by an interdisciplinary expert group in
accordance with officially accepted standards and are based on all relevant publica-
t ions since 1985. They were discussed and accepted in a consensus conference.
EN should be given to all ICU pat ients who are not expected to be taking a full oral
diet within three days. It should have begun during the first 24h using a standard
ARTICLE IN PRESS
ht tp:// int l.elsevierhealth.com/ journals/ clnu
0261-5614/ $ - see front matter & 2006 European Society for Clinical Nutrit ion and Metabolism. All rights reserved.
doi:10.1016/ j .clnu.2006.01.021
$ For further informat ion on methodology see Schutz et al. 69 For further informat ion on definit ion of terms see Lochs et al. 70
Corresponding author. Tel.: +494042803 7010; fax: +49 4042803 7020.
E-mail address: [email protected] (K.G. Kreymann).$ $ The authors of the DGEM (German Society for Nutrit ional Medicine) guidelines on enteral nutrit ion in intensive care are
acknowledged for their contribut ion to this art icle.
Kreymann KG et al. Clinical Nutrition (2006) 25, 210–223

Singer P et al. Clinical Nutrition 28 (2009) 387–400

Taylor BE i wsp. Crit Care Med 2016; 44: 390–438


AREAS OF UNCERTAINTY
risk assessment
energy and protein requirement
tolerance of gastric feeding
prokinetics
optimal timing of nutritional intervention
GRV monitoring
PN initiation
optimal composition of PN
CURRENT HOT TOPICS IN THE ICU
NUTRITION
Patient Admitted to the ICU
“Assess for nutritional risk”
“Calculate energy and protein requirement”
“Take steps to improve tolerance to gastric feeding”
“Implement enteral feeding protocol”
“Do not use gastric residual volumes as part of routine care”
“Start PN when EN is not feasible or sufficient in high-risk patients”
• How to identify patients at highest nutritional risk?
• What is the role of the existing nutritional risk scores?
• Does nutrition guided by measuring EE affect patient outcome?
• What is the approach for estimating EE that is associated with improved outcome?
• What is the optimal calorie dose?
• What is the optimal protein dose?
• What is the role of novel pro-motility agents?
• Which patients benefit from post-pyloric feeding tube placement?
• What is the optimal timing for initiation of artificial feeding?
• What is the optimal strategy for managing EN?
• Does gastric residual monitoring have a role in the identification of patients with gastrointestinal dysfunction?
• What is the role of pro-motility agents?
• Does improving gastric emptying result in improved clinical outcomes?
• What is the optimal timing of initiating PN?
• What is the optimal caloric dose of PN?
• What is the optimal composition of PN? Lipids? Micronutrients?
• Who is at “high risk”? Does it mean more risk of harm by underfeeding or more risk of harm by EN/PN???
Fig. 1 Flowchart highlighting some of the uncer tainties in the nutritional support decision-making. The boxes on the left are based on the “bundle
statements” from the Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN) Guidelines for the
Provision and Assessment of Nutritional Support therapy in the Adult Critically Ill Patient [5]. The boxes on the right represent corresponding areas of
uncertainties


Critical illness
Metabolic stress
sarcopenia
malnutrition
early optimal
nutrition
Negative protein-
energy balance
starvation
immobilization
catabolism Inadequate delivery of
protein and calories
Increased morbidity
Increased mortality
Longer length of stay
Longer recovery
increased
costs
NUTRITION IN THE ICU

NUTRITIONAL RISK ASSESSMENT
• INTERVIEW
• CLINICAL EVALUATIONS
• physical examination
• risk factors
• LABORATORY FINDINGS
• lymphocyte count
• <900 mm3 - severe malnutrition
• albumin - T1/2 - 18 days
• transpherine - T1/2 - 7 days
• prealbumin - T1/2 - 2 days
NRS-2002
≥ 3 feed
≥ 5 intensive nutritional
intervention

WHO SUPPORTS EARLY ENTERAL
FEEDING IN THE ICU?
• Society of Critical Care Medicine
• American Society of Parenteral and
Enteral Nutrition (ASPEN)
• Canadian Critical Care Clinical
Practice Guidelines Committee
• European Society for Clinical
Nutrition and Metabolism
• Brain Trauma Foundation

PITFALLS DURING EARLY ENTERAL
FEEDING IN THE ICU
• Regurgitation and vomiting (PONV)
• Delayed gastric emptying (increased
gastric residual volume)
• Abdominal distension
• Diarrhea
• GI bleeding
• High output GI tract fistula
less than 70% of
patients receive
adequate EN
Chest, vol. 125, 2004

TO FEED OR NOT TO FEED
(ENTERALLY)?
• Check electrolyte levels
• Prokinetics
• metoclopramide
• erythromycin
• Jejunal feeding

maintains gut integrity
maintains microbiom diversity
sustains functioning of GALT and
production of IgA
sustains functioning of MALT
stimulates Th2 lymphocytes and
T-regulatory cells
THE BENEFITS OF TROPHIC ENTERAL
FEEDING
30% of calculated demand

HYPOCALORIC FEEDING - PERMIT TRIAL

• acute phase of critical illness - up to 7 days
• suitable for well nourished patients
HYPOCALORIC FEEDING
n engl j med 372;25 nejm.or g June 18, 20152402
The n ew en g l an d j o u r n a l of med i c i n e
ence in the probability of survival between the
two groups (P = 0.43 by the log-rank test) (Fig. 2).
Other End Points
Serial SOFA scores, nitrogen balance, body
weight, and levels of C-reactive protein, prealbu-
min, creatinine, bilirubin, partial pressure of
arterial carbon dioxide, hemoglobin, lipids, po-
tassium, magnesium, phosphate, transferrin,
and urinary nitrogen excretion did not differ
signif icantly between the two groups (Fig. 1,
and Fig. S5 through S10 in the Supplementary
Appendix). The number of days free from me-
chanical ventilation and the number of ICU-free
VariablePermissive Underfeeding
(N = 448)Standard Feeding
(N = 446)
Age — yr 50.2±19.5 50.9±19.4
Female sex — no. (%) 156 (34.8) 164 (36.8)
Body-mass index† 29.0±8.2 29.7±8.8
Diabetes — no. (%) 159 (35.5) 153 (34.3)
Admission category — no. (%)
Medical 336 (75.0) 335 (75.1)
Surgical 19 (4.2) 12 (2.7)
Nonoperative trauma 93 (20.8) 99 (22.2)
Severe sepsis at admission — no. (%) 159 (35.5) 133 (29.8)
Traumatic brain injury — no. (%) 55 (12.3) 63 (14.1)
APACHE II score‡ 21.0±7.9 21.0±8.2
SOFA score§ 9.9±3.5 9.8±3.5
Mechanical ventilation — no. (%) 436 (97.3) 429 (96.2)
Vasopressor therapy — no. (%) 255 (56.9) 243 (54.5)
Glycated hemoglobin — mmol/ liter 0.07±0.06 0.07±0.08
C-reactive protein — mg/ liter 131±80 125±82
Serum lipid levels — mmol/ liter
Triglycerides 1.56±1.07 1.58±1.17
Total cholesterol 2.66±1.07 2.77±0.98
Low-density lipoprotein 1.29±0.78 1.34±0.72
High-density lipoprotein 0.59±0.33 0.64±0.40
Albumin — g/ liter 28±7 28±6
Prealbumin — g/ liter 0.15±0.13 0.14±0.12
Transferrin — g/ liter 1.36±0.49 1.38±0.50
24-hour urinary nitrogen excretion — mmol 284±176 303±219
Time from eligibility to randomization — hr 8.3±11.6 7.9±12.3
* Plus–minus values are means ±SD. There were no significant between-group differences. Data on laboratory values were not available for some patients; the numbers of patients with available data in the permissive-underfeeding group and the standard-feeding group, respectively, were as follows: glycated hemoglobin, 268 patients and 284 patients; C-reactive protein, 357 patients and 360 patients; triglycerides, 375 patients and 376 patients; total cholesterol, 373 pa-tients and 372 patients; low-density lipoprotein, 366 patients and 363 patients; high-density lipoprotein, 374 patients and 375 patients; prealbumin, 334 patients and 341 patients; transferrin, 359 patients and 361 patients; and 24-hour urinary nitrogen excretion, 305 patients and 292 patients.
† The body-mass index is the weight in kilograms divided by the square of the height in meters.‡ Scores on the Acute Physiology and Chronic Health Evaluation (APACHE) II range from 0 to 71, with higher scores in-
dicating more severe disease.§ Scores on the Sequential Organ Failure Assessment (SOFA) range from 0 to 24, with higher scores indicating a greater
degree of organ failure.
Table 1. Baseline Characteristics of the Patients, According to Study Group.*
The New England Journal of Medicine
Downloaded from nejm.org on May 8, 2016. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.

HIGH NUTRITIONAL RISK
• Significant malnourishment or obesity
• Significant loss of body weight (>10%) in
the past 3 months
• Hypercatabolism
• Increased loss of nutrients
• GI tract fistula
• Diarrhea
• Malabsorption
the lowest in the entire survey cohort reported, being8–9 kcal/kg with about 0.4 g/kg protein. Despite recom-mendations that obese patients receive high-protein diets,the actual intake was very low, and few patients receivedsupplemental protein. Hence, these patients had the mostsevere discrepancy between needs and receipt of nutri-tion, a form of iatrogenic malnutrition—iatrogenic in thesense that they do not start their critical illness malnour-ished, but develop protein and energy deficits through thecourse of their ICU stay. Under these circumstances, anyincrease in nutritional intake would be of benefit. In thisobese group, the inadequacy of protein intake in relationto lean body mass would lead to erosion of lean bodymass and depletion of key amino acids and micronutri-ents, which are essential for immune function [23]. Thus,the benefits of increased nutrition in this group could bedue to the increased protein intake, which reached a moreacceptable intake of up to 1.2 g/kg/day, while the maxi-mum energy delivered of 22 kcal/kg/day remainedhypocaloric.
Our overall findings are consistent with the publishedliterature describing an association between worseclinical
outcomes and increasing caloric debt [1–3], but are dis-cordant with the findings of Krishnan and colleagues thatshowed that 33–66% of goal calorieswereassociated with
Table 5 Relationship between increased nutrition and 60-day mortality
(a) Increased energy intake
BMI group Unadjusted (n = 2,772) Adjusted (n = 2,729a)
Odds ratio 95% CI p value Odds ratio 95% CI p value
LCL UCL LCL UCL
Overall 0.73 0.62 0.87 0.001 0.76 0.61 0.95 0.014\ 20 0.48 0.28 0.83 0.009 0.52 0.29 0.95 0.03320 to \ 25 0.61 0.45 0.82 0.001 0.62 0.44 0.88 0.00725 to \ 30 1.01 0.75 1.36 0.960 1.05 0.75 1.49 0.76830 to \ 35 0.84 0.54 1.30 0.439 1.04 0.64 1.68 0.88935 to \ 40 0.47 0.23 0.95 0.036 0.36 0.16 0.80 0.012C40 0.78 0.41 1.47 0.442 0.63 0.32 1.24 0.180
(b) Increased protein intake
BMI group Unadjusted (n = 2,771b) Adjusted (n = 2,728a)
Odds ratio 95% CI p value Odds ratio 95% CI p value
LCL UCL LCL UCL
Overall 0.83 0.75 0.92 \ 0.001 0.84 0.74 0.96 0.008\ 20 0.60 0.43 0.84 0.003 0.60 0.41 0.87 0.00720 to \ 25 0.79 0.66 0.94 0.008 0.81 0.66 0.99 0.03625 to \ 30 0.95 0.80 1.14 0.609 0.97 0.79 1.19 0.75830 to \ 35 0.92 0.72 1.19 0.533 1.04 0.79 1.37 0.77435 to \ 40 0.70 0.47 1.04 0.075 0.62 0.39 0.98 0.039C40 0.82 0.59 1.14 0.237 0.72 0.51 1.03 0.072
Odds of 60-days mortality per increase of 1,000 kcal (a) and 30 gof protein (b) received per day both unadjusted and adjusting fornutrition days, BMI, age, admission category, admission diagnosis,and APACHE II score. Estimates are from the generalized linear(logistic) mixed effects model with a random ICU effect. Interac-tion terms were used to produce BMI-specific estimates. p valuesare Wald type t tests
CI confidence interval, LCL lower confidence limit, UCL upperconfidence limit, BMI body mass index, APACHE acute physiologyand chronic health evaluation, ICU intensive care unita Forty-three (1.6%) patients are excluded due to missing one ormore covariates in the adjusted modelb One patient missing protein intake
Fig. 1 Therelationship between increasing calories/day and 60-daymortality by BMI. BMI body mass index
1734

HIGH NUTRITIONAL RISK

SUPPLEMENTAL PARENTERAL
NUTRITION
• 1372 ICU patients
• Early PN
• shorter MV

Lancet, vol. 381, 2013
SUPPLEMENTAL PARENTERAL
NUTRITION

SUPPLEMENTAL PARENTERAL
NUTRITION
Oshima et al 5
the third day. Adding supplemental PN to fulfill the energy
needs resulted in fewer late nosocomial infections and a trend
for shorter mechanical ventilation.
These results support the concept that EN should be started
as soon as patients are hemodynamically stabilized with the
goal of gradually testing the GI tolerance. With the resolution
of the catabolic response, which generally occurs around 3–4
days after ICU admission, energy provision needs to be
increased to meet the energy requirements. In case of EN intol-
erance with a high risk of underfeeding, supplemental PN
should be prescribed to bridge the gap and to reach the energy
targets, ideally determined by indirect calorimetry (Figure 2).
Indirect calorimetry should be repeated during the ICU stay to
evaluate the dynamic changes in the metabolic rate of critically
ill patients and to fine-tune the prescriptions of nutrition
according to the changes.
Conclusion
Adequate feeding is beneficial during and after the ICU stay.
Our pragmatic approach is to start early EN to progressively
test the gut tolerance and to add supplemental PN on day 3 or
4 after ICU admission, only if EN does not meet the energy
targets. Supplemental PN plays a pivotal role in the optimiza-
tion of feeding of critically ill patients with incomplete toler-
ance to EN and does not cause any harm if overfeeding is
avoided by careful prescription, ideally based on EE measured
by indirect calorimetry.
Statement of Authorship
T. Oshima, C.-P. Heidegger, and C. Pichard contributed to the
conception and design of the manuscript. All authors drafted the
manuscript, critically revised the manuscript, agree to be fully
T able 2. Equations Used to Derive EE in Indirect Calorimetry.
Names and Purposes Equations
VO2 and VCO
2 calculation VO
2 (L/min) = (Vi × FiO
2) – (Ve × FeO
2)
VCO2 (L/min) = (Ve × FeCO
2) – (Vi × FiCO
2)
Haldane transformation (to simplify Vi measurement) Vi = [FeN2/ FiN
2] × Ve
FeN2 = (1 − FeO
2− FeCO
2), FiN
2 = (1 − FiO
2− FiCO
2)
Weir’s equation EE (kcal/d) = [(VO2 × 3.941) + (VCO
2 × 1.11)] × 1440
EE, energy expenditure; FeCO2, fraction of expired carbon dioxide; FeN 2, fraction of expired nitrogen; FeO2, fraction of expired oxygen; FiCO2, fraction
of inspired carbon dioxide; FiN2, fraction of inspired nitrogen; FiO2, fraction of inspired oxygen; Ve, expired volume (L/min); Vi, inspired volume (L/
min); VO2, O
2 consumption; VCO
2, CO
2 production.
Figure 2. Optimal combination of enteral nutrition (EN) and parenteral nutrition (PN) avoids overfeeding and underfeeding:
supplemental PN plays a pivotal role in the optimization of feeding of critically ill patients with incomplete tolerance to EN and does not
cause any harm if overfeeding is avoided by careful prescription, ideally based on energy expenditure measured by indirect calo rimetry.
at UNIV NEBRASKA LIBRARIES on June 2, 2016ncp.sagepub.comDownloaded from
Nutr Clin Pract. 2016(4):432-7.

ENDOGENOUS ENERGY PRODUCTION
(CATABOLISM) 706 Journal of Parenteral and Enteral Nutrition 37(6)
amount of useable substrates, and the severity of disease.
Conceptually, the use of a composite score could help to quan-
tify the nutrition risk and a nutrition intervention.13 However,
large-scale prospective validation of an approach using this
score is still needed.
Among the methods developed to assess EE, estimation
through simple rules of thumb or complex predictive formulas
is the most popular. The measurement of EE with indirect calo-
rimetry (IC) is less accessible, although warmly recommended
by some experts. Finally, the current gold standard is the
doubly labeled water method. Each method has its drawbacks.
In this review, we will detail the determinants of EE and the
different methods of evaluation by increasing the level of
sophistication and complexity; thereafter, we will discuss the
issue of the possible influence of the method used on the results
of clinical trials.
Energy Expenditure
Total EE (TEE) includes 3 components: basal energy expendi-
ture (BEE or basal metabolic rate [BMR]), diet-induced ther-
mogenesis (DIT), and the energy required for physical
activity14,15 (Figure 2). BEE is the energy required to maintain
the body’s basic cellular metabolic activity and organ func-
tions, such as respiration and normal body temperature in the
absence of recent food intake, physical activity, and psycho-
logical stress.15 Resting energy expenditure (REE) has been
used to describe BEE in a post-absorptive state. In sedentary
healthy subjects, REE accounts for about two-thirds of TEE.
This could not be extrapolated for all critically ill patients14;
since nutrition is usually delivered continuously, body tem-
perature could be modified by the illness (eg, fever, shivering,
tachypnea) or by treatment (eg, therapeutic hypothermia, seda-
tive agents, β-blockers). These circumstances could increase or
decrease EE.
Determination of Energy Expenditure
Rule of Thumb
The simplest recommendations, widely disseminated by some
professional societies, advocate a fixed amount of calories per
kg of body weight (BW).16-18 These guidelines are indeed very
simple and used to define a standard average caloric target for
most critically ill patients. However, variations of EE over time
and between different categories of patients are not taken into
Figure 1. Imaginary example of energy expenditure, caloric
needs, and debt in a critically ill patient. X-axis represents
time from admission (days). Y-axis represents energy (kcal/
day). (A) The thick black line represents energy expenditure
(EE); each lighter bar represents the daily endogenous non-
inhibitable production of calories. Caloric needs are shown as
the difference between EE and endogenous calories. (B) Each
darker bar represents daily caloric intake. Caloric debt is shown
as the difference between EE and caloric intake. (C) Each bar
represents the sum of endogenous calories plus caloric intake.
Overfeeding is achieved on each day, as the sum of endogenous
calories plus caloric intake exceeds EE.
Figure 2. Different components of energy expenditure.
by guest on October 1, 2014pen.sagepub.comDownloaded from
706 Journal of Parenteral and Enteral Nutrition 37(6)
amount of useable substrates, and the severity of disease.
Conceptually, the use of a composite score could help to quan-
tify the nutrition risk and a nutrition intervention.13 However,
large-scale prospective validation of an approach using this
score is still needed.
Among the methods developed to assess EE, estimation
through simple rules of thumb or complex predictive formulas
is the most popular. The measurement of EE with indirect calo-
rimetry (IC) is less accessible, although warmly recommended
by some experts. Finally, the current gold standard is the
doubly labeled water method. Each method has its drawbacks.
In this review, we will detail the determinants of EE and the
different methods of evaluation by increasing the level of
sophistication and complexity; thereafter, we will discuss the
issue of the possible influence of the method used on the results
of clinical trials.
Energy Expenditure
Total EE (TEE) includes 3 components: basal energy expendi-
ture (BEE or basal metabolic rate [BMR]), diet-induced ther-
mogenesis (DIT), and the energy required for physical
activity14,15 (Figure 2). BEE is the energy required to maintain
the body’s basic cellular metabolic activity and organ func-
tions, such as respiration and normal body temperature in the
absence of recent food intake, physical activity, and psycho-
logical stress.15 Resting energy expenditure (REE) has been
used to describe BEE in a post-absorptive state. In sedentary
healthy subjects, REE accounts for about two-thirds of TEE.
This could not be extrapolated for all critically ill patients14;
since nutrition is usually delivered continuously, body tem-
perature could be modified by the illness (eg, fever, shivering,
tachypnea) or by treatment (eg, therapeutic hypothermia, seda-
tive agents, β-blockers). These circumstances could increase or
decrease EE.
Determination of Energy Expenditure
Rule of Thumb
The simplest recommendations, widely disseminated by some
professional societies, advocate a fixed amount of calories per
kg of body weight (BW).16-18 These guidelines are indeed very
simple and used to define a standard average caloric target for
most critically ill patients. However, variations of EE over time
and between different categories of patients are not taken into
Figure 1. Imaginary example of energy expenditure, caloric
needs, and debt in a critically ill patient. X-axis represents
time from admission (days). Y-axis represents energy (kcal/
day). (A) The thick black line represents energy expenditure
(EE); each lighter bar represents the daily endogenous non-
inhibitable production of calories. Caloric needs are shown as
the difference between EE and endogenous calories. (B) Each
darker bar represents daily caloric intake. Caloric debt is shown
as the difference between EE and caloric intake. (C) Each bar
represents the sum of endogenous calories plus caloric intake.
Overfeeding is achieved on each day, as the sum of endogenous
calories plus caloric intake exceeds EE.
Figure 2. Different components of energy expenditure.
by guest on October 1, 2014pen.sagepub.comDownloaded from

EXOGENOUS ENERGY SOURCES IN THE
ICU (NOT DIRECTLY LINKED TO
NUTRITION)
• Citrate anticoagulation
• 1 mmol citrate - 0,59 kcal
• 1 mmol glucose - 0,74 kcal
of a calcium-containing lactate-buffered replacement fluid
and ACD as citrate source represents an unwanted modality.
Caloric load of citrate CRRT can be reduced by using
TSC as citrate source (avoiding glucose delivery), by
increasing dialysate flow and associated citrate removal, by
using bicarbonate-buffered solutions (avoiding lactate deliv-
ery), calcium-free solutions (reducing citrate dose), using an
isotonic calcium-free citrate-buffered predilution replace-
ment fluid [17], or lowering blood flow (reducing citrate
delivery). If we would have used a similar low blood flow
with the ACD/Caplus/lactate modality as used in the TSC/
Camin/bicarbonate modality, we would have reduced the
energy delivery from glucoseand citrate to atotal delivery of
about 188 kJ/h, a reduction of 29%. When ACD would have
been used with bicarbonate-buffered fluids and ablood flow
of 100 mL/min, but still containing calcium, thebioenergetic
delivery might be further reduced to about 116 kJ/h, that is,
2794 kJ/24 h, a reduction of 56%. If we would have used
ACD with a calcium-free bicarbonate buffered fluids and a
blood flow of 100 mL/min, median estimated daily
bioenergetic delivery would likely be about 1910 kJ/24 h
(1120 kJ/24 h from glucoseand 816 kJ/24 h from citrate), ie,
a reduction of 68% (see Table 3). Even though, the
extrapolated delivery would still require adjustment of
daily nutritional intake.
The present study also shows excellent metabolic control
when using citrate anticoagulation. We found no hypo- or
hypernatremia with citrate, and only one patient with
metabolic alkalosis in each of thecitrategroups. This finding
corresponds to the literature [1,4,9,10,12]. Despite the high
citrate concentrations in the ACD/Caplus/lactate group, we
did not find signsof citrate accumulation asevidenced by an
increased total to ionized calcium ratio (datanot shown). Our
systemic citrate concentrations were comparable to those
found by Hetzel [23], but substantially higher than those of
Mariano [11], who used a lower blood flow and therefore a
lower citrate flow. Although patientswith primarily elevated
lactate levels weregiven bicarbonatebuffered fluids, lactate-
Table 3 Comparison of estimated daily citrate anticoagulated CVVHDF substrate delivery and bioenergetic gain not corrected for filter
downtime and adjusted for the unified blood flow of 100 mL/min
ACD/Caplus/lactate TSC/Camin/bicarb ACD/Camin/bicarb MW-U test P
(Group 1) (Group 2) (Group 3) 1 vs 2 1 vs 3 2 vs 3
Substrate delivery (+) or loss (−), corrected for a Qb of 100 mL/min
Citrate (mmol/24 h) 455 (416-498) 354 (298-458) 329 (295-360) b.01 b.01 0.33
Glucose (mmol/24 h) 567 (501-613) −146 (−172 to −62) 366 (328-401) b.01 b.01 b.01
Lactate (mmol/24 h) 1260 (1181-1418) −67 (−105 to −41) −70 (−110 to −43) b b.01 b.01 0.35
Bioenergetic gain (+) or loss (−)
Citrate (kJ/24 h) a 1128 (1031-1235) 878 (738-1136) 816 (732-893) b.01 b.01 0.28
Glucose (kJ/24 h) a 1735 (1532-1877) −447 (−525 to −189) 1120 (1004-1227) b.01 b.01 b.01
Lactate (kJ/24 h) a 1727 (1618-1943) −92 (−144 to −57) −96 (−148 to −59) b b.01 b.01 0.31
Total (kJ/24 h) a 4510 (4115-4913) 480 (192-602) 1910 (1568-2085) b.01 b.01 b.01
The right column shows the results of a theoretical group using ACD with calcium free bicarbonate buffered fluid.a For conversion to kcal, divide by 4.184.b Estimated as lactate loss in TSC/bicarbonate group and corrected for the CVVHDF dose in ACD/lactate group. All values are medians and IQRs.
Table 4 Comparison of estimated costs between the three modalities of CVVHDF
ACD/lactate TSC/bicarbonate Hep/lactate MW-U test P
(Group 1) (Group 2) (Group 3) 1 vs 2 1 vs 3 2 vs 3
Estimated costs (EUR/24 h)
Citrate solution 53.82 (48.3-55.89) 32.22 (28.43-37.9) N/A b.01 N/A N/A
Replacement fluids 63 (63-84) 135.3 (135.3-135.3) 79.8 (63-84) b.01 0.11 b.01
Calcium chloride 11.13 (6.36-14.31) 11.13 (9.54-15.9) N/A 0.38 N/A N/A
Heparin N/A N/A 7.47 (5.81-8.72) N/A N/A N/A
Postfilter Ca2+ (6 per 24 h) 13.74 13.74 N/A N/A N/A N/A
Extra APTT (4 per 24 h) N/A N/A 12.56 N/A N/A N/A
Total costs/24 h excluding circuits 142 (128-161) 195 (191-224) 100 (82-104) b.01 b.01 b.01
Daily circuit cost a 58 (44-83) 48 (30-75) 85 (64-106) b.01 b.01 b.01
Total costs/24 h including circuits 200 (186-219) 243 (239-273) 185 (167-189) b.01 b.01 b.01
a Estimated from circuit life. The costs of the arterial Ca2+ measurement were not calculated because they were provided with the standard blood gas
determination. All values are in median (IQR). Daily circuit costs were calculated as 24/circuit lifetime (h) in individual patient and then converted into
expenses without correction for circuit down time.
93Comparing 2 citrate modalit ies and unfractionated heparin
Bioenergetic gain of citrate anticoagulated continuous
hemodiafi ltration—a comparison between 2 citrate
modalities and unfractionated heparin☆,☆☆
Martin Balik MD, PhDa,⁎, Mykhaylo Zakharchenko MDa, Pavel Leden MDa,Michal Otahal MDa, Jan Hruby MDa, Ferdinand Polak MD, PhDa,Katerina Rusinova MDa, Zdenek Stach MDa, Monika Tokarik MDb,Jaroslava Vavrova PhDc, Antonin Jabor MD, PhDd,Heleen M. Oudemans-van Straaten MD, PhDe
aDepartment of Anaesthesiology and Intensive Care, First Faculty of Medicine, Charles University and
General University Hospital, U nemocnice 2, Prague 2, 120 00, Czech RepublicbPrague Burn Centre, 3rd Faculty of Medicine, Charles University, Prague, Czech RepubliccDepartment of Clinical Biochemistry, Faculty Hospital Hradec Králové, Hradec Králové, Czech RepublicdDepartment of Clinical Biochemistry, Institute for Clinical and Experimental Medicine, Prague, Czech RepubliceDepartment of Intensive Care Medicine, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands
Keywords:Acute renal failure;
Anticoagulation;
Citrate;
Hemodiafiltration;
Renal replacement therapy
Abstract
Purpose: To determine bioenergetic gain of 2 different citrate anticoagulated continuous hemodiafiltra-
tion (CVVHDF) modalities and a heparin modality.
Materials and Methods: We compared the bio-energetic gain of citrate, glucose and lactate between 29
patients receiving 2.2% acid-citrate-dextrose with calcium-containing lactate-buffered solutions (ACD/
Caplus/lactate), 34 on 4% trisodium citrate with calcium-free low-bicarbonate buffered fluids (TSC/
Camin/bicarbonate), and 18 on heparin with lactate buffering (Hep/lactate).
Results: While delivered CVVHDF dose was about 2000 mL/h, total bioenergetic gain was 262kJ/h
(IQR 230-284) with ACD/Caplus/lactate, 20 kJ/h (8-25) with TSC/Camin/bicarbonate (P b .01) and
60 kJ/h (52-76) with Hep/lactate. Median patient delivery of citratewas31.2 mmol/h (25-34.7) in ACD/
Caplus/lactate versus 14.8 mmol/h (12.4-19.1) in TSC/Camin/bicarbonate groups (P b .01). Median
delivery of glucosewas36.8 mmol/h (29.9-43) in ACD/Caplus/lactate, and of lactate52.5 mmol/h (49.2-
59.1) in ACD/Caplus/lactate and 56.1 mmol/h (49.6-64.2) in Hep/lactate groups. The higher energy
delivery with ACD/Caplus/lactate was partially due to the higher blood flow used in this modality and
the calcium-containing dialysate.
☆ ClinicalTrials.gov Identifier: NCT01361581.☆☆ Conflict of interest to declare: None.⁎ Corresponding author. Tel.: +420 224962244; fax: +420 224962118.
E-mail address: [email protected] (M. Balik).
0883-9441/$ – see front matter © 2013 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.jcrc.2012.06.003
Journal of Critical Care (2013) 28, 87–95

• OVERNUTRITION
• refeeding syndrome
• hypercapnia
• HIGH PROTEIN LOAD
• uremia
• hypertonic dehydration
• metabolic acidosis
• HIGH CARBOHYDRATE LOAD
• hyperglycemia
• hypertriglyceridemia
• fatty liver
NUTRITION RELATED SIDE EFFECTS
(EN<SPN<TPN)

Clinical Nutrit ion (2006) 25, 210–223
ESPEN GUIDELINES
ESPEN Guidelines on Enteral Nutrit ion:
Intensive care$
K.G. Kreymanna, , M.M. Bergerb, N.E.P. Deutzc, M. Hiesmayrd, P. Jolliet e,G. Kazandj ievf, G. Nitenbergg, G. van den Bergheh, J. Wernermani,DGEM:$ $ C. Ebner, W. Hart l, C. Heymann, C. Spies
aDepartment of Intensive Care Medicine, Universit y Hospit al Eppendorf , Hamburg, GermanybSoins Intensifs Chirurgicaux et Cent re des Brules, Cent re Hospital ier Universit aire Vaudois (CHUV)-BH
08.660, Lausanne, Swit zerlandcDepartment of Surgery, Maast r icht Universit y, Maast richt , The NetherlandsdDepart ment of Anaesthesiology and Intensive Care, Medical Universit y of Vienna, Vienna, Aust riaeDepartment of Intensive Care, Universit y Hospit al Geneva, Geneva, Swit zerlandfDepart ment of Anaesthesiology and Intensive Care, Mil i t ary Medical Universit y, Sofia, BulgariagDepart ment of Anaesthesia, Intensive Care and Infect ious Diseases, Inst i t ut Gust ave-Roussy,
Vil lej uif , FrancehDepartment of Intensive Care Medicine, Universit y Hospit al Gasthuisberg, Leuven, BelgiumiDepart ment of Anaesthesiology and Intensive Care Medicine, Karolinska Universit y Hospit al, Huddinge,
Stockholm, Sweden
Received 20 January 2006; accepted 20 January 2006
KEYWORDSGuideline;
Clinical pract ice;
Evidence-based;
Enteral nut rit ion;
Tube feeding;
Oral nut rit ional sup-
plements;
Parenteral nut rit ion;
Immune-modulat ing
nut rit ion;
Summary Enteral nut rit ion (EN) via tube feeding is, today, the preferred way of
feeding the crit ically ill pat ient and an important means of counteract ing for the
catabolic state induced by severe diseases. These guidelines are intended to give
evidence-based recommendat ions for the use of EN in pat ients who have a
complicated course during their ICU stay, focusing part icularly on those who develop
a severe inflammatory response, i.e. pat ients who have failure of at least one organ
during their ICU stay.
These guidelines were developed by an interdisciplinary expert group in
accordance with officially accepted standards and are based on all relevant publica-
t ions since 1985. They were discussed and accepted in a consensus conference.
EN should be given to all ICU pat ients who are not expected to be taking a full oral
diet within three days. It should have begun during the first 24h using a standard
ARTICLE IN PRESS
ht tp:// int l.elsevierhealth.com/ journals/ clnu
0261-5614/ $ - see front matter & 2006 European Society for Clinical Nutrit ion and Metabolism. All rights reserved.
doi:10.1016/ j .clnu.2006.01.021
$ For further informat ion on methodology see Schutz et al. 69 For further informat ion on definit ion of terms see Lochs et al. 70
Corresponding author. Tel.: +494042803 7010; fax: +49 4042803 7020.
E-mail address: [email protected] (K.G. Kreymann).$ $ The authors of the DGEM (German Society for Nutrit ional Medicine) guidelines on enteral nutrit ion in intensive care are
acknowledged for their contribut ion to this art icle.
Kreymann KG et al. Clinical Nutrition (2006) 25, 210–223

PROTEIN BALANCE IN THE CRITICALLY
ILL PATIENTS
Curr Opin Clin Nutr Metab Care 2016, 19:120 – 124

PROTEIN REQUIREMNET IN THE
CRITICALLY ILL PATIENTS
1,3 - 1,5 g/kg
1,2 – 2,0 g/kg

PROTEIN REQUIREMNET IN THE
CRITICALLY ILL PATIENTS
over the course of cri t ical i l lness. It is well described
that the early or ‘acute phase’ of cri t ical i l lness is
characterized by massive mobil izat ion of the body’s
calorie reserves as muscle, glycogen, and l ipid stores
are broken down to drive glucose product ion
[14,15]. This evolut ionari ly conserved response
allows the stressed or injured human (or animal)
to generate energy to escape its attacker and recover
from init ial in juries. This metabolic response to
stress can generate 50–75% of the glucose needs
during i l lness [15], and this glucose generat ion is
not suppressed by feeding or intravenous glucose
infusion [16]. This is described in much greater
detai l in this issue by Oshima et al. (pp. 292–298)
and in other recent data by our group [16]. Further,
we know that the early phases of sepsis and trauma
are not hypermetabolic states, but rather the
pat ients have a total energy expenditure (TEE)-
to-rest ing energy expendi ture (REE) rat io of 1.0
and 1.1 for sepsis and trauma, respect ively [17].
Thus, caloric need does not increase in the early
phases of injury (first few days post injury). In fact,
the more severe sept ic shock is, the lower the rest ing
energy is, as the body ‘h ibernates’ and shuts down
metabolism in response to severe stress [18]. During
the later chronic or recovery phase of cri t ical i l lness,
the body experiences a massive increase in
metabolic needs, with TEE increasing as much as
1.7-fold above REE [17]. These data suggest we
should consider feeding less nonprotein calories
early in the acute phase (first 24–96 h) of cri t ical
i l lnessand markedly increase calorie del ivery during
recovery asi l lustrated in Fig. 2. At the same time, it is
also well known that protein losses increase 4-fold
in the first 24 h of cri t ical i l lness [19] and we are
exceedingly poor at meeting these needs [19].
Unfortunately, large, internat ional surveys indicate
we as ICU pract i t ioners deliver an average of
0.6 g/kg/day of protein for the first 2 weeks fol low-
ing ICU admission [20]. This is one-third to half of
latest ICU guidel ine recommended protein delivery
of 1.2–2.0 g/kg/day [21]. In contrast to what isoften
taught, the delivery of addi t ional nonprotein calo-
ries does not significant ly improve nitrogen balance
in i l lness beyond delivery of 50% of predicted REE
[16]. Thus, an ideal ‘targeted’ feeding strategy is
perhaps 15 kcal/kg/day of total energy during early
ICU stay (acute phase), whereas ensuring pat ients
receive opt imal protein del ivery (1.2–2.0 g/kg/day)
as early as possible post-ICU admit (Fig. 2). The vital
role of early protein administrat ion is covered in
greater detai l in the review by Weijs et al. (pp. 299–
302) in this issue. Reduced calorie del ivery during
the acute phase is l ikely not applicable in malnour-
ished patents [i .e., pat ients with significant pre-ICU
weight loss or Nutri t ion Risk in Crit ical ly i l l
(NUTRIC) score (without IL-6) > 5] who are unlikely
to have the metabolic reserve to generate needed
endogenous energy [21,22]. Evaluat ion of nutri-
t ional status and apart from malnutri t ion diagnosis
is further covered in this issue by Simpson and Doig
(pp. 303–307). Ironical ly, our most recent Society
of Crit ical Care Medicine/American Society for
Parenteral and Enteral Nutri t ion (SCCM /ASPEN)
guidel inesemphasize these poin ts in updated guide-
l ines suggest ing hypocaloric parenteral nutri t ion
( 20 kcal/kg/day or 80% of est imated energy needs)
with adequate protein ( 1.2 g protein/kg/day) be
considered in pat ients requiring parenteral nutri-
t ion over the first week in ICU [21]. Further, in early
sepsis (or acute phase of cri t ical i l lness), the new
SCCM/ASPEN guidel ines suggest provision of tro-
phic feeds (defined as 10–20 kcal/h up to 500 kcal/
day) for init ial phase of sepsis, advancing as toler-
ated after 24–48 h to more than 80% of target energy
with early del ivery of 1.2–2 g protein/kg/day [21].
Given limited higher protein, lower ki localorie
enteral feeding opt ions commercial ly, total paren-
teral nutri t ion (TPN) or enteral protein supplements
wil l be required to achieve this. TPN isa significant ly
more viable opt ion now to achieve this as three
recent large trials of both supplemental and ful l
TPN support versus enteral nutri t ion in the ICU
sett ing have shown that TPN use in the ICU is
no longer associated with increased infect ion risk
[23–25]. This is l ikely because of improvements
in glucose control, central-l ine infect ion control
measures, and potent ial ly as a result of improved
(nonpure soy based) l ipid formulat ions as described
in detai l in this issue by Manzanares et al. (pp. 308–
315). In support of early TPN use, the new SCCM/
ASPEN guidel ines indicate in any patient at high
nutri t ion risk [Nutri t ion Risk Score 2002 5 or
45
Protein (g/kg/d)Kcal/kg/day
Proposal for targeted nutrition delivery in critical illness
2.5
2.0
1.5
1.0
0.75
Protein delivery
Sepsis
traumaSeverely
malnourished?
Total kcal
delivery in well
nourished P t
Acute phase
(0−5 d post ICU -admit)
Chronic phase
(5+ days post ICU -admit)
Recovery phase
(post-ICU discharge)
Activity/
rehab
increases
40
35
30
25
20
15
FIGURE 2. Proposal for targeted nutrition delivery across
phases of critical illness.
Delivering targeted nutrition to improve outcomes in ICU W ischmeyer
1070-5295 Copyright ß 2016 W olters Kluwer Health, Inc. All rights reserved. www.co-crit icalcare.com 281
Curr Opin Crit Care 2016, 22:279 – 284

CLINICAL CONDITION PROTEIN REQUIREMENT
(g/kg IBW/day)
Normal (nonstressed)
0.8
Mild stress 1-1.2
Critical Illness/injury/moderate stress
1-1.5
Acute Renal Failure (dialyzed)
1.2-1.4
Infection, major surgery, cancer
1.4-1.6
Burn/Sepsis/ multiple trauma
1.5-2
CRRT/CVVHD
1.7-2.5

CRRT AND PROTEIN BALANCE
• 0,2 g of AA are lost per 1 liter
of UF
• daily loss of AA: 10 - 15 g

CRRT AND PROTEIN BALANCE
Umber, Wolley, Golper, et al. 96
and 37 at SLED inception. Two patients were
receiving concomitant intravenous hyperali-
mentation during SLED treatment, providing
each with an average of 50 g/day of amino
acid solution (Novamine; Baxter Healthcare
Corporation, Deerfie
l
d, IL, US A) .
Main results
Albumin was not detectable in dialy-
sate samples. Amino acids losses to di-
alysate are summarized in Tables 2 and 3.
Median losses per treatment ranged from
13.4 mg (129.6 μmol) for γ-aminobutyric
acid (GABA) to 5,285 mg (18,360 µmol)
for glutamine. The median (mean ± stan-
dard deviation) total amino acid loss was
15.7 (23.4 ± 19.2) g/treatment, or 122.1
(180.6 ± 148.5) mmol/treatment.
The patient with hepatic failure had high
dialysate levels of aromatic amino acids, glu-
tamate, glutamine, methionine, cystine, and
alanine, with a total amino acid loss via di-
alysate of 57 g per treatment, as compared to
a mean of 14.9 g per treatment for the other
patients (Figure 1).
There was no signific
a
nt difference in
amino acid losses between those who re-
ceived heparin during SLED compared to
those who did not (p = 0.38). The correla-
tion between Kt/V and amino acid losses was
high but not statistically significa nt (r = 0.72,
p = 0.166).
Two of the 5 patients were receiving
hyperalimentation during SLED. Exclud-
ing the outlying patient with hepatic failure
there were no signific
a
nt differences in total
amino acid loss between those who were re-
ceiving intravenous hyperalimentation and
those who did not (median 12.0 g vs. 17.9 g,
p = 0.245).
Discussion
In this study we quantified median
amino acid losses to dialysate of 15.7 g per
treatment in critically ill patients treated
with SLED. This is comparable to amino
acid losses during CRRT. We recommend
that protein supplementation is increased
in patients undergoing SLED in a similar
fashion to CRRT. Notably, albumin was not
detectable in dialysate, but we point out that
low-flux membranes were used in this study
and the use of high-flu
x
or reused mem-
branes is likely to result in detectable and
probably signific
a
nt los ses.
Nutritional requirements are increased
during critical illness accompanied by AKI,
and there is some evidence that optimal
nutritional support may improve outcomes
in these patients [4, 5]. Wide ranging meta-
bolic derangements occur, but in particular
a negative nitrogen balance is common,
with protein catabolism enhanced by fac-
tors such as stress, inflam ma t ion and acido-
sis [15]. Maintenance of a positive nitrogen
balance in this setting has been associated
with increased probability of survival in
some preliminary studies [16, 17]. Over-
all consensus guidelines suggest ensuring
a protein supply of between 0.8 and 1.7 g/
kg/day according to the clinical condition,
the degree of catabolism, and the modality
Table 3. Amino acid losses to dialysate per treatment, by individual patients.
Patient BCAAa,b ESSa,c Semi ESSa,c Non ESSa,c Totala
1 1,509 14,588 2,431 38,885 57,040
2 2,943 7,048 939 7,693 15,680
3 1,136 4,251 548 5,223 10,038
4 2,418 5,597 545 7,838 13,993
5 2,323 8,328 1,587 10,100 20,022
aResults in mg/treatment; bBCAA = branch chain amino acids; cESS = essen-
tial amino acids.
Figure 1. Amino acid losses to dialysate (mmol)
per treatment in subject with end-stage liver dis-
ease (black bars), compared with the other sub-
jects (grey bars).

PROTEIN ADMINISTRATION AND
MORTALITY

able to match > 50%
REE within 3 days? YES NO not a
problem
Contraindication
to EN?
przeciwwskazane
?
YES NO
malnourished
high risk start EN: gradually increase
infusion rate (target 25 kcal/kg/day)
and optimize delivery (promotility
agents, post pyloric tube)
DAY 5 -7
EN still
contraindicated? <80% of prescription
delivered by EN?
consider SPN to match caloric
debt
Lancet, vol. 381, 2013
YES NO
Parenteral
nutrition WAIT
malnourished
high risk
YES NO
YES
Parenteral
nutrition
NO

ENERGY 1 kcal/ml %ENERGY
PROTEIN
CARBOHYDRATES
FAT
OSMOLARITY
ENERGY 1,28 kcal/ml %ENERGY
PROTEIN
CARBOHYDRATES
FAT
OSMOLARITY
„NORMAL”
FORMULA
„BETTER”
FORMULA
ENERGY 1 kcal/ml %ENERGII
PROTEIN
CARBOHYDRATES
FAT
OSMOLARITY
„FUTURE”
FORMULA


• Hospital made or RTUs
• High protein content
• Low Q index (kcal/N)
PARENTERAL NUTRITION

SUMMARY
• Nutritional support in the ICU
• reduces disease severity
• diminishes complications
• decreases length of stay
• favorably impacts patient outcome
• There are many guidelines on nutritional intervention in the ICU
• One size fits all approach is not feasible for a challenging ICU patient
• Sometimes clinicians need to adapt them to different clinical scenarios

Thank You for your attention






![Supportive Nutritional Intervention in Pediatrie Cancer1 · [CANCER RESEARCH (SUPPL.) 42, 766s-773s, February 1982] 0008-5472/82/0042-OOOOS02.00 Supportive Nutritional Intervention](https://img.pdfslide.net/doc/110x75/5e54de10ae6c922dcf35ce94/supportive-nutritional-intervention-in-pediatrie-cancer1-cancer-research-suppl.jpg)




















