Embed Size (px)
Citation preview

Columbus pediatrician William
Cotton, MD, received the ElizabethSpencer Ruppert Outstanding Pedia-trician of the Year Award at the 2010Ohio AAP Annual Meeting on Nov.6. Dr. Cotton was recognized for hisdistinguished achievements and out-standing contributions to the ad-vancement of pediatric care and edu-cation for patients and physicians inOhio.
Dr. Cotton’s easy-going, welcom-ing personality has helped him to be-come a great leader. Under his lead-ership, the Chapter secured an$800,000 grant to initiate the Chap-ter’s Autism Diagnosis EducationPilot Program. During his presidency,the Chapter received the OutstandingChapter of the Year Award for Very
care professional; first vaccine/toxoidcomponent• 90461 Immunization administra-tion through 18 years of age via anyroute of administration, with counsel-ing by physician or other qualifiedhealth-care professional; each addi-tional vaccine/toxoid component.(List separately in addition to codefor primary procedure.)
Certain other administration codes(CPT 90471 through 90474) will re-main, but now will only be used toreport immunization administrationfor children performed without physi-cian counseling and for all immu-nizations for those 19 years of ageand older.
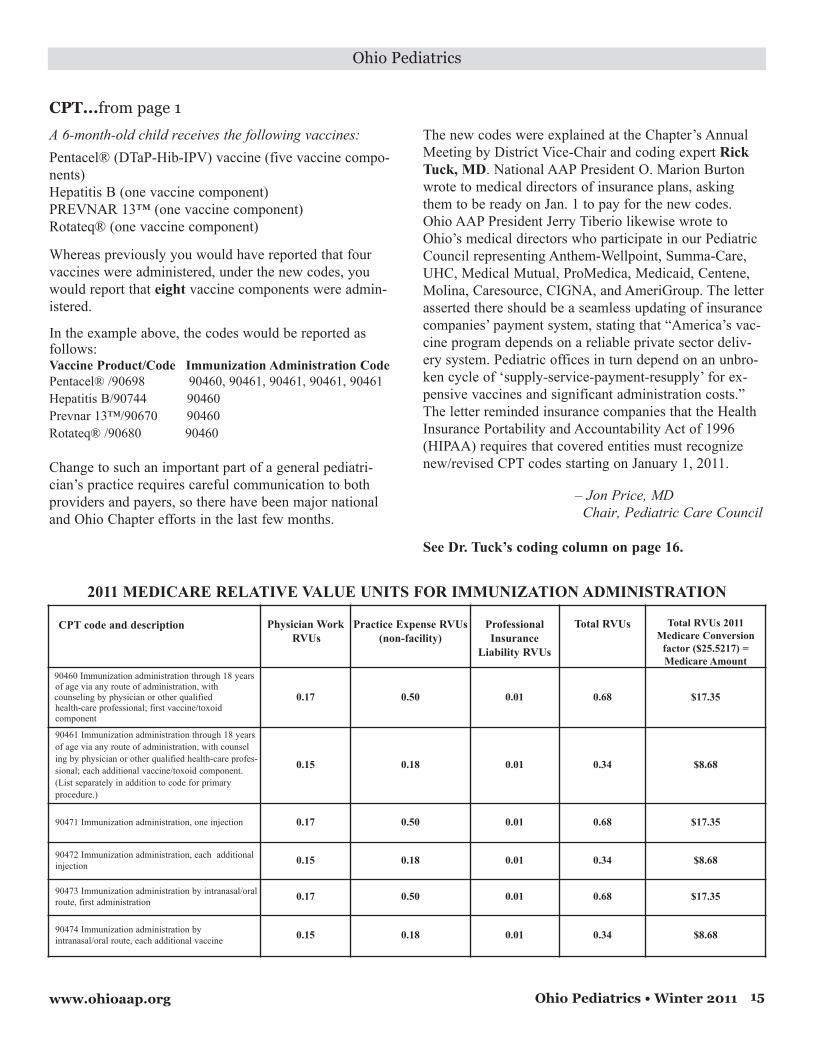
The 2011 Relative Value Unitshave been assigned for all of thesecodes. (See chart on page 15.)
Here’s an example of how somecommon vaccines would be coded:
Newsmagazine of the Ohio Chapter, American Academy of Pediatrics Winter 2011
In this issue:
• Case Study: ACL tears
• New Council formed
• Coding Corner - IA codes
• Ounce of Prevention
• Annual Meeting PhotosSee Award...on page 17
See CPT...on page 15
New immunization codes can increase reimbursement
Ohio AAP Past President William
Cotton, MD, Columbus, received the
Chapter’s highest award at its Annual
Meeting for distinguished achievement
and outstanding contributions to pedi-
atric care in Ohio.
Dr. Cotton receivesPediatrician of Year
Starting January 1, the way youroffice reports your vaccine counsel-ing changed. For several years, manypediatricians have asked to charge forcounseling by the vaccine componentthat they have to explain and not bythe injection. In 2011, CPT reportingfor vaccines for minors does just that.This allows you to get payment forcounseling for newer combinationvaccines that deliver necessary com-ponents in fewer injections.
It is important to note that the pre-vious codes for physician counselingfor vaccine doses, which applied onlyto patients younger than 8 years, willbe abolished. The new codes apply tocounseling, per component, for pa-tients younger than 19 years.
The Ohio AAP’s Pediatric Councilsent letters prior to Jan. 1 to all themajor Ohio medical plans explainingthat the new codes better reflect thework associated with administeringvaccines, including increased coun-seling inherent with administeringvaccines, particularly those with mul-tiple components and asked for theirhelp in making the process a seam-less transition.
The new codes are:• 90460 Immunization administrationthrough 18 years of age via any routeof administration, with counseling byphysician or other qualified health-
In December, Ohio AAP’s Pediatric Care Council took a proactiveapproach and sent letters to Ohio’s major medical plans urgingappropriate payment for immunization administration.

See Legislation...on page 23
Ohio Pediatrics • Winter 20112
Ohio Pediatrics
A Publication of the Ohio Chapter,
American Academy of Pediatrics
Officers
President....Gerald Tiberio, MD, FAAP
President-Elect.....Judith Romano, MD, FAAP
Treasurer....Andrew Garner, MD, PhD, FAAP
Delegates-at-large:
Jill Fitch, MD, FAAP
Allison Brindle, MD, FAAP
Robert Murray, MD, FAAP
Executive Director:Melissa Wervey Arnold450 W. Wilson Bridge Road, Suite 215
Worthington, OH 43085
(614) 846-6258, (614) 846-4025 (fax)
Lobbyist:Dan Jones Capitol Consulting Group
37 West Broad Street, Suite 820
Columbus, OH 43215
(614) 224-3855, (614) 224-3872 (fax)
Editor:Karen Kirk(614) 846-6258 or (614) 486-3750
www.ohioaap.org
Now is the time for pediatricians to form relationships with new leaders
After months of hard-hitting poli-tics, the 2010 election wrapped upwith some dramatic changes in thepolitical landscape. Voters sent aclear message to elected officialsthat it is time for a change in stateand federal policies. Although Re-publicans had a clear sweep in keypolitical offices, the upsets seemedto be based on the need for changeand not a simple endorsement of apolitical party.
What lies ahead for Ohio’s
pediatricians?
For this new session, Ohio AAPleadership and legislative consul-tants will be meeting and getting toknow new legislators and preparingfor an important budget debate. Witha strong Republican state govern-ment, policymakers will likely beready to take on issues such as addi-tional tort reforms, but less likely totake on issues that reform or man-date insurance. Additionally, this Re-publican majority is less likely tolook at increasing taxes to balancethe state budget. Additional cuts inMedicaid and throughout state gov-ernment are expected.
Pediatricians On Call
This would be an excellent time tobecome involved in the Ohio AAP’sPediatricians On Call program – anetwork of pediatricians who inter-act with their state representative orsenator on behalf of pediatrics. Readmore about this program in “ThePresident’s Message” on page 3. Formore information on how you can
get involved, contact the Ohio AAPat [email protected] or call theoffice at (614) 846-6258.
The new players include:Ohio Governor – John Kasich
In the contentious battle for theGovernor’s office that ran close dur-ing the many months of campaign-ing, former Republican Congress-man John Kasich beat incumbentDemocrat Gov. Ted Strickland 49 to47 percent.
U.S. Senate – Rob Portman
Former Republican CongressmanRob Portman held a solid lead overDemocratic Lieutenant GovernorLee Fisher throughout most of theelection season. The final tally:Portman 57 percent; Fisher 39 per-cent. Despite turnover in this and afew other key races, Democrats con-tinue to hold a majority in the U.S.Senate.
U.S. House of Representatives
Of the 18 Ohio members of theU.S. House, currently 10 are Demo-crats and eight are Republicans.With five key Republican victoriesin Ohio, the majority in our state’scongressional team shifts to 13-5 inthe Republicans favor. With similarsurges across the country, the U.S.House has shifted to a Republicanmajority. Also important to Ohio,Congressman John Boehner (R-WestChester) has the support of his col-leagues to serve as Speaker of theHouse in the new session.
Ohio House
The Ohio House also faces a swingin power as Republicans win a ma-jority of the 99 races across the state.The current House tally for the newGeneral Assembly in January is 59Republicans, 40 Democrats. Of inter-est, Dr. Terry Johnson, a Republicanphysician and colonel in the OhioNational Guard from Portsmouth,won a seat in the Ohio House, 89thDistrict. It will be refreshing to havea “doctor in the House” this session.
Update from the statehouse

When I started
practice, member-
ship in the AAP
was an integral
part of being a
pediatrician. There
was never a ques-
tion as to whether
to join and pay
dues upon com-
pletion of training.
For a number of years I was not
active in the Ohio Chapter. In the
early 1990s, I received a Healthy
Tomorrow’s grant improving access
for indigent children. Chapter Presi-
dent Libby Ruppert asked me to
present the work at the Ohio Chap-
ter’s Annual Meeting. Shortly after,
Ed Rushton (then director of Com-
munity Pediatrics) at National, ask-
ed for an encore.
What I began to experience was
an opportunity for networking. Im-
portant work was accomplished, in-
novative ideas were shared, and
friendships were made. Another
world existed outside the exam
room and the hospital committee
structure. This phenomenon occurs
whether you are a generalist, a sub-
specialist, or a surgeon.
Another benefit of Chapter mem-
bership is education. Staying in-
formed via this publication, the
Chapter website, E-newsletter, the
Annual Meeting – the list continues.
Many of you attended the Novem-
ber Annual Meeting where immu-
nization coding, parental refusal of
vaccines, and immunizations and
infectious disease were discussed.
The three QI/MOC programs the
Chapter currently maintains provide
opportunities for learning, improv-
ing quality, and maintaining certifi-
cation. Think about it, asthma, de-
velopment/autism, and obesity are
all nuts and bolts in day-to-day
pediatrics.
A third benefit is an opportunity
for legislative and advocacy activi-
ties. The Chapter website has a vid-
eo (under the Advocacy link) of Dr.
Terry Barber (immediate past pres-
ident) and Melissa Wervey Arnold,
Ohio AAP’s Executive Director,
describing “Pediatricians On Call.”
It is a network of pediatricians who
interact with their state representa-
tive or senator on behalf of children.
Pediatricians enjoy a favorable repu-
tation with legislators, and as consti-
tuents can influence policy. The plan
is to connect pediatricians with key
legislators around the state. You will
receive communications through the
E-newsletter, personal e-mail and a
newsletter summarizing important
bills. The sign-up process is on our
website.
During the past year, the chapter
gave testimony for required menin-
gococcal vaccine, worked with the
Governor’s office for enhanced
Medicaid reimbursement, supported
obesity legislation, supported school
bus seatbelts, and the inclusion of
pediatrics in the Medical Home leg-
islation. We also dealt with various
vaccine issues.
A fourth benefit is leadership and
leadership development. Serving as
a chairperson or member of a chap-
ter-level committee in an area of in-
terest or expertise is quite reward-
ing. Spearheading a specific chapter
project and/or initiative is always a
worthwhile endeavor. I have been
involved with the My Story Foster
Care initiative. We have improved
the lives of countless foster care
children and their families. The pro-
gram has helped me grow profes-
sionally and has been the source of
great personal satisfaction.
Some pediatricians ask the ques-
tion, what has the AAP done for me
lately? I never asked the question
because my mentors taught me the
answer. The AAP was the advocate
for children. It represents the inter-
ests of pediatricians in a world that
often does not value its children.
Remember the “pizza boxes” in the
AAP Strategic Plan. Topics like im-
munizations, obesity, CYSHCN,
foster care, are, or will be, integrat-
ed into the very fabric of our Acad-
emy.
The Committee on Infectious Di-
seases compiles and publishes the
most important reference on pedi-
atric immunizations and infectious
disease, the Red Book, used on a
daily basis by all doctors who care
for children. There are countless
other examples.
Before I was invited to present my
Healthy Tomorrow’s grant, I was a
dues-paying supporter of “the”
voice for children and pediatricians.
What would our profession be with-
out the AAP? Please remember
these four – Networking, Education,
Advocacy and Leadership. They are
the cornerstones of your career in a
profession unlike any other. Re-
member the adage, “One pediatri-
cian CAN make a difference.”
– Gerald Tiberio, MD
Ohio AAP President
Ohio Pediatrics • Winter 2011 3
Ohio Pediatrics
www.ohioaap.org
President’s Message
Gerald Tiberio, MD
Benefits to your Ohio AAP membership

Ohio Pediatrics • Winter 20114
Advertisement
www.ohioaap.org
Ohio Pediatrics • Winter 2011 5
Ohio Pediatrics
www.ohioaap.org
Case Study: ACL tear in a female athlete
Editor’s note: The author of this
case study, Anastasia Fischer, MD,
is a pediatrician in the Department
of Sports Medicine at Nationwide
Children’s Hospital in Columbus.
Case presentation:
A 17-year-old female basketball
player presents with a knee injury.
She injured her knee last night, dur-
ing a game, when coming down
from a rebound and landing unbal-
anced on her right leg. She felt a
pop internally in her knee and fell to
the ground. She was unable to con-
tinue play and needed to be assisted
off of the court. She noted immedi-
ate swelling in the knee. She dili-
gently iced the knee last night, as
well as this morning, and had ap-
plied an ACE wrap for support. She
was seen by her PCP this morning,
who was concerned about internal
derangement of the knee. She has
never sustained an injury to this
knee before.
Physical Examination:
A bright, healthy, happy young ladywho walks with a severely limitedgait secondary to pain. Examinationof the right knee shows a mild intra-articular effusion without ecchymo-sis. There is minimal tenderness topalpation over the lateral and pos-terolateral side of the knee at thefibular head, as well as lateral jointline and lateral collateral ligamentstructures. Range of motion of theknee is limited, with the patientlacking approximately 15 degrees ofextension and only able to flex theknee to approximately 90 degrees.
Strength is limited secondary topain. On special tests, the patienthas a loose Lachman’s test, as wellas pain with an anterior drawer test.There is no obvious posterior sagsign. Valgus and varus testing of theknee reveals intact ligamentousstructures, but with reproduction ofpain. Meniscal testing is difficultdue to patient discomfort, but amodified Apley’s test is negative –flexion pinch, McMurray’s and thebounce home test are unable to beperformed. No pain with manipula-tion of the patella. Neurovascularexamination of the lower extremityis intact.
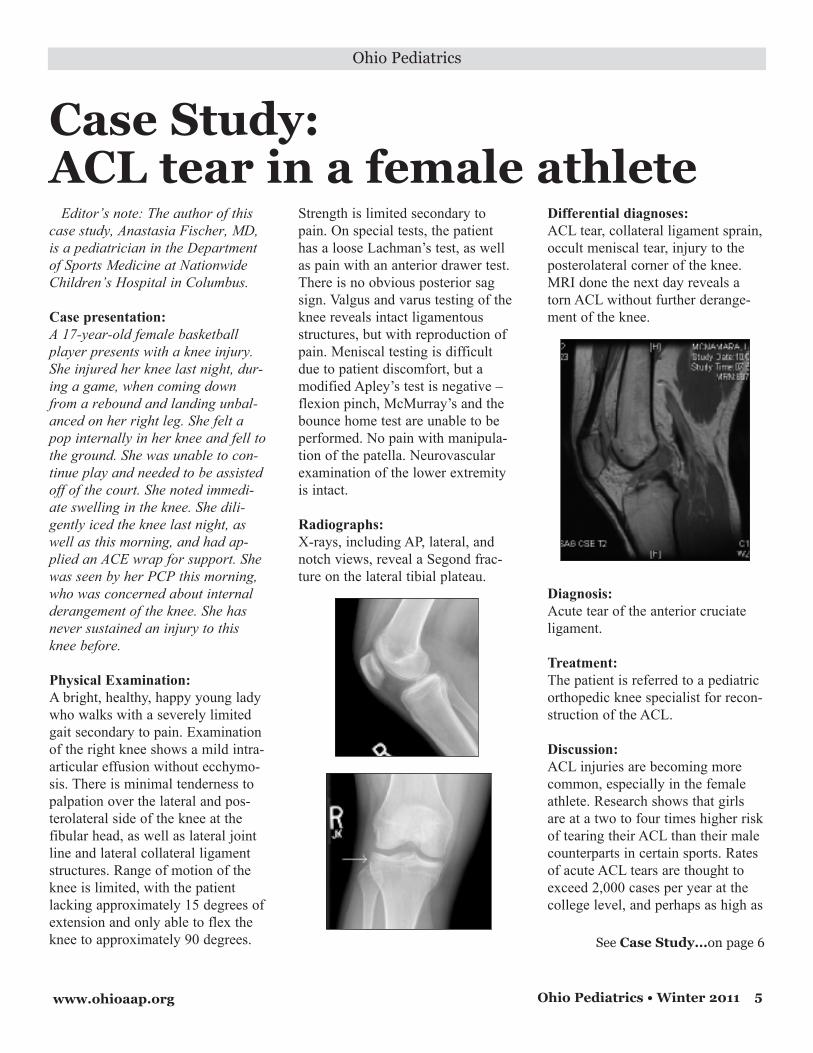
Radiographs:
X-rays, including AP, lateral, andnotch views, reveal a Segond frac-ture on the lateral tibial plateau.
Differential diagnoses:
ACL tear, collateral ligament sprain,occult meniscal tear, injury to theposterolateral corner of the knee.MRI done the next day reveals atorn ACL without further derange-ment of the knee.
Diagnosis:
Acute tear of the anterior cruciateligament.
Treatment:
The patient is referred to a pediatricorthopedic knee specialist for recon-struction of the ACL.
Discussion:
ACL injuries are becoming morecommon, especially in the femaleathlete. Research shows that girlsare at a two to four times higher riskof tearing their ACL than their malecounterparts in certain sports. Ratesof acute ACL tears are thought toexceed 2,000 cases per year at thecollege level, and perhaps as high as
See Case Study...on page 6

Ohio Pediatrics
6 www.ohioaap.orgOhio Pediatrics • Winter 2011
Case Study...from page 5
9,000 cases per year at the highschool level nationally. Girls arethought to have this increased riskfor several reasons:• Anatomical differences in the kneecompared to boys – girl’s genu val-gus (knock-kneed) stature and nar-rower femoral notch may result inhigher static tension to the ACL,making it easier to tear.
• Biomechanical factors and landingmechanics – girls have less musclemass, are slower at the rate of mus-cle force development (ms), have astronger, quicker reacting quadricepsrelative to hamstrings, tend to bemore upright when landing, and tendto be “quad dominant” – all factorsthat will increase anterior translationof the tibia relative to the femur, putting the athlete at risk for an ACLtear.
• Hormonal differences from boys –some previous studies have shownthat ACL tears are more commonduring the ovulatory phase of themenstrual cycle than the follicularphase, but recent evidence is con-flicting.
• Neuromuscular differences – girlstend to be more “ligament domi-nant,” meaning that they rely ontheir ligaments to absorb the force oflanding, rather than muscular con-trol, and more “quad dominant,”again, increasing the risk of anteriortibial translation with respect to thefemur.
In women, four out of five ACLtears are non-contact injuries, hap-pening very often during decelera-tion activities, (i.e. landing from ajump or planting and cutting) andare due to being in the “position ofno return” – a position in which thepelvis is tilted forward, the hips
extended and internally rotated, theknee in valgus and extension, andlanding in a position of poor bal-ance.
By teaching female athletes howto avoid this position, ACL tear pre-vention programs have been seen toreduce the incidence of non-contactACL tears by about 70-80% in girlsages 14-18. Programs concentrate onavoiding the “position of no return”by increasing flexibility andstrength, improving balance throughagility training, and including sportsspecific training in the program togive more “real time” experience.Programs typically meet three timesper week for six to eight weeks andare best done before the next up-coming season, although the techni-ques learned in the course should beperformed two to three times perweek for the season to keep skillsfresh.
When ACL tears do occur, mostathletes will find that surgical recon-struction is the best option for themto continue with their sporting ca-reer, even if only recreationally.Knees without an intact ACL areprone to recurrent instability withcutting and pivoting motions, put-ting their menisci at risk for futureor further damage. Instability alsooften causes bony bruises with asso-ciated pain, effusion, and limitationin the short term. Surgical recon-struction is best done when the kneehas regained range of motion andeffusion is minimal, and recovery isdependent upon the extent of dam-age in the joint, as meniscal or otherligamentous or capsular injuries areoften repaired concurrently. Estimat-ed time back to full sports is aboutsix months from the time of surgeryto allow for development of full
Save The Date!
Ohio AAP 2011
Annual Meeting
Aug. 25-27 at
Cherry Valley Lodge
in Newark
Highlights:
• Quality Improvement
Roundtable
• American Board of Pediatrics
representative discusses MOC
• Medical Home Reimbursement
Visit the Ohio AAP website
www.ohioaap.org
for more information
strength in the ACL graft, and to in-corporate a rehabilitation programthat not only concentrates on regain-ing strength and motion of the knee,but also a healthy helping of injuryprevention.
– Anastasia Fischer, MD
Department of Sports Medicine
Nationwide Children’s Hospital
ReferencesGilchrist J, etal. A Randomized Controlled Trial to
Prevent Noncontact Anterior Cruciate Ligament
Injury in Female Collegiate Soccer Players. Am J
Sports Med. 2008;36(8):1476-1483.
Meyer GD, Ford KR, Hewett TE. Rationale and
Clinical techniques for Anterior Cruciate Ligament
Injury Prevention Among Female Athletes. Journal
of Athletic Training. 2004;39:352-363.
Mandelbaum BR, Silvers HJ, et al. Effectiveness of
a Neuromuscular and Proprioceptive Training
Program in Preventing Anterior Cruciate Ligament
Injuries on Female Athletes. Am J Sports Med.
2005;33:1003-1010.
Olsen OE, Myklebust, et al. Exercises to Prevent
Lower Limb Injuries in Youth Sports: Cluster
Randomized Controlled Trial. British Medical
Journal. 2005;330:449-452

Ohio Pediatrics
7www.ohioaap.org Ohio Pediatrics • Winter 2011
Ounce of Prevention materialsnow available in Spanish
Last year, the Ounce of Prevention
is Worth a Pound toolkit was updatedand expanded to include obesity pre-vention information for children frombirth through 18 years of age. Infor-mation on healthy serving sizes,healthy snacking, sports nutrition,and calcium were also developed andadded to the toolkit. Most recently,the complete set of 25 handouts havebeen translated into Spanish for fur-ther reach and usage.
“The best part of these new materi-als is not that they are just translatedinto Spanish, but that they have beenmodified to address the cultural andfamily traditions of Latino families,”says Amy Sternstein, MD, coordina-tor of the Ounce of Prevention pro-gram at Nationwide Children’s Hos-pital Center for Healthy Weight andNutrition.
The Ounce of Prevention toolkitwas developed in 2007 to address thegrowing epidemic of childhood obe-sity. The goal is to provide primarycare providers with simple tools to
educate parents in obesityprevention strategies bymaking good nutritionaland physical activitydecisions for their chil-dren.
The handouts are de-signed to highlight fourareas during each well-child visit from the new-born visit through 18years. Those areas are:
• Food for Thought• Feeding Advice• Be Active• Notes
The Ounce of Preven-
tion is Worth a Pound
program was developedin collaboration with theOhio Chapter, AmericanAcademy of Pediatrics;the Ohio Department ofHealth, Office of HealthyOhio; the American DairyAssociation Midwest; theOhio Dietetic Associa-tion; and NationwideChildren’s Hospital.
Last January, the OhioDepartment of Healthawarded a StatewideWellness and ObesityPrevention ProgramGrant to the Ohio AAP tospread the Ounce of Pre-vention materials. Eightwebinars and five region-al trainings were held aspart of the grant. Further fundingmay be available in the near future toprovide additional office-based train-ings throughout the state.
Carole Lannon, MD, PhD, introduces attendees of thefull-day learning session for Healthy Kids Ohio –Ounce of Prevention to the basics of quality improve-ment work, including reviewing the key driver dia-gram which will be used by practices participating inthe obesity prevention learning collaborative. Prac-tices from across Ohio came together in Columbus inNovember to kick off their participation in a qualityimprovement learning collaborative.
“The best part of these new materials is not that theyare just translated into Spanish, but that they havebeen modified to address the cultural and family tra-ditions of Latino families,” says Amy Sternstein, MD,shown here during a regional training at the Cuya-hoga County Board of Health in October.
As part of the Statewide Obesity Pre-vention and Wellness grant the OhioAAP received, Robert Murray, MD,(pictured above) along with AmySternstein, MD, have presented AnOunce of Prevention information tonearly 250 health-care professionalsthroughout Ohio.
For more information on the Ounceof Prevention toolkit, or to downloadthe handouts in English and in Span-ish, visit the website at: www.theounceofprevention.org.

Ohio Pediatrics • Winter 20118 www.ohioaap.org
Ohio Pediatrics
Spring forum addresses specificneeds of young physicians, residents
Residents across Ohio connectedfor the third year in a row at theAnnual Meeting in November. TheYoung Physicians and ResidentsCommittee held a roundtable discus-sion on various topics pertinent toresidents including potential for astatewide resident advocacy cam-paign, and transition from residency.Ohio AAP President Gerald Tiberio,
MD, thanked the residents for theircommitment and pledged the Chap-ter’s support for their initiatives.
Many who attended the AnnualMeeting had previously attended thespring Advocacy Training held inMay 2010. At the spring conference
speakers introduced residents to leg-islative advocacy and the Ohio leg-islative process.
Residents and young physicianswith continued interest in these topicsmay consider attending the AAPLegislative Conference in Washing-ton, D.C. March 13-15, or considerapplying for AAP department of fed-eral affairs internship program. TheAcademy individualizes the intern-ship, which is primarily designed forthose interested in child health poli-cy, the legislative process, federaladvocacy, and public affairs. Infor-mation on these opportunities, aswell as advocacy grant opportunities
available to young physicians andresidents, can be found at http://www. aap.org/sections/ypn/.
Many attendees at the Novembermeeting expressed interest in devel-oping a forum for residents in spring2011. Potential topics of interest in-clude pediatric obesity, access to careand adolescent health, job searchingpost-residency, and transitioning tofellowship. Please stay tuned formore details on this upcoming freeprogram. Additionally, we want yourinput related to topics of interest andpotential speakers.
If you are a resident, or young phy-sician, interested in helping to planthis event, please contact leaders ofthe YP&R Committee for more infor-mation.Allison Brindle, MD – Co-Chair([email protected])Emily Decker, MD – Co-Chair ([email protected]) Norah Ledyard, DO – Co-Chair([email protected])
– Norah Ledyard, DO
Co-Chair, YP&R Committee
Members of the Young Physicians andResidents Committee met at the OhioAAP Annual Meeting in November todiscuss issues pertinent to residents.
SERVING STUDENTS WITH LANGUAGE-BASED LEARNING DIFFERENCES AND ATTENTION DEFICIT DISORDERS
TEACH | IGNITE | INSPIRE
LAWRENCE SCHOOL
AL
OLHOCSENCEWRAAWR
H | ICAET
RIPSNE | ITINGH | I
ER
T
H | I
SGNIVRSENEREFFIG DNINRAEL
CAET
A
R
B-EGAUGNA LHTI WSTENDUTICIFEN DOITNETTD A ATNS AECN
IPSNE | ITINGH | I
D
E
SEASREDROSIT DI
R

9www.ohioaap.org Ohio Pediatrics • Winter 2011
Ohio Pediatrics
Reach Out and Read and APA announce Young Investigator Award
Research to focus on strategies for promoting early literacy and school readiness
Reach Out and Read and theAcademic Pediatric Association(APA) have announced the creationof a new Young Investigator AwardProgram for Primary Care Strategiesfor the Promotion of Early Literacyand School Readiness. The awardwill provide financial support foryoung investigators whose researchprojects focus on interventions inprimary care intended to support theearly stages of literacy developmentand school readiness among chil-dren at risk for reading problems orschool failure.
The Young Investigator AwardProgram may grant up to $15,000 toone selected project annually, begin-ning in 2011.
"Pediatricians and other primarycare providers can play a criticalrole in helping parents help theiryoung children grow up with booksand reading, and truly ready forschool," said Perri Klass, MD, Na-tional Medical Director of ReachOut and Read.
"We believe that this new awardwill stimulate new explorations ofthe potential power of that primarycare encounter, and encourage newinvestigators to launch exciting newexplorations in literacy research,"she continued.
Through this award, the primarygoal is to foster development ofyoung investigators who will ad-vance a research agenda related to:
1. Improving early literacy andschool readiness among children,especially those at risk for language
delay and school problems, throughprimary care-based interventionsincluding Reach Out and Read andrelated programs.
2. Understanding home environ-mental and other influences (bothsocial and biological) related toearly literacy and school readiness,in order to inform development andrefinement of primary care interven-tions.
The Academic Pediatric Associa-tion is a leading child health profes-sional organization that promoteseducation, research, and advocacy.Preference will be given to new in-vestigators, including those in train-ing. New investigators are definedas: 1) faculty members who are nomore than five years out from com-pletion of all training (fellowship orpost-doc); 2) fellows; 3) post-doc-toral trainees; 4) residents; 5) gradu-ate students.
Questions about this program canbe directed to Connie Mackay at theAPA central office by calling 703-556-9222, or e-mailing [email protected].
Reach Out and Read promotesearly literacy and school readiness
by working through pediatric prima-ry care providers who give newbooks to children and advice to par-ents about the importance of readingaloud at regular medical checkups.The model includes providing acarefully-selected, new, age-appro-priate book for each child to takehome from every checkup from 6months through 5 years.
Currently, there are 14 peer-re-viewed, published research studiesdemonstrating the efficacy of theReach Out and Read model. Thissimple intervention results in chil-dren entering kindergarten with larg-er vocabularies and stronger lan-guage skills.
For more information on becom-ing a Reach Out and Read site,please contact Heather Hall at (614)846-6258 or [email protected].
YoungPhysicians
and Residents
Advocacy DayMay 17, 2011
Riffe CenterColumbus
Watch Ohio AAP websiteand publications for more
information.

10 Ohio Pediatrics • Winter 2011 www.ohioaap.org
Ohio Pediatrics
New Council supports strong Chapterprogramming, promotes accountability
The first biannual meeting of thePlanning, Implementation, and Per-formance (PIP) Council was held atthe 2010 AnnualMeeting. TheBoard of Directorsfelt this newCouncil was need-ed to continue theChapter's strongprogramming andto promote com-munication andaccountabilitybetween theBoard, the medical directors of thevarious Chapter programs, and theChairs of the numerous Ohio AAPCouncils and Committees.
The rationale for forming this newCouncil was multifaceted. First, in-creasingly complex financial auditsare requiring additional documenta-tion of specific and objective deliver-ables and deadlines to "justify" thesalaries the Chapter pays its MedicalDirectors. The PIP Council hopes tomake this process more "transparent"to outsiders by requiring the MedicalDirectors to submit a yearly report.This report will be similar to the"balanced scorecard" used by theChapter in its reports to the NationalAAP, and its completion will allowthe Chapter's finances to be "beyondreproach."
The PIP Council will also serve asa means of tapping the expertise ofthe Chapter's current Medical Direc-tors to inform the development ofnew programming. With the Chap-ter's recent commitment to provideits members with interesting andmeaningful ways to obtain Part IV
MOC credit, future programs will be-nefit from the trailblazing leadershipof the current Medical Directors.The PIP Council will also attempt todraw upon the experience of pastleaders within the Chapter (e.g.,alumni of the Board) when planningand designing new programs forMOC credit or otherwise.
Another reason for forming thisnew Council is to improve communi-cation between the Board of Direc-tors and the Councils/CommitteeChairs. While Councils and Com-mittees remain autonomous and areencouraged to pursue their self-iden-tified goals and objectives, increasedcommunication with the Board ofDirectors should allow for more col-laboration to ensure that the pressingneeds of the Chapter are addressed aswell. Council/Committee Chairs willalso be asked to submit an annualreport prior to the Annual ExecutiveCommittee retreat that outlines theirgoals, objectives and budget for thecoming year. Completion of this re-port will be necessary for the Chap-ter's continued financial support ofeach Council/Committee.
No one familiar with the activitiesof the Ohio Chapter would ever ques-tion the dedication and hard work ofits Medical Directors or its Council/Committee Chairs. Hopefully, thePIP Council will serve as a coordi-nating and oversight body to ensureeffective collaboration and to pro-mote communication and account-ability as the Chapter continues toexpand its service to its members.
Questions and suggestions can bee-mailed to Andrew Garner, MD,PIP Chair, at [email protected].
PIP Vision Statement:
All projects and programs within
the Ohio AAP are well planned,
properly implemented, and perform
as expected.
PIP Mission Statement:
To assist in the planning, implemen-
tation and oversight of Ohio AAP
programs and projects to ensure
their initial and continued success.
PIP Membership:
Meetings are open to all Chapter
members and invited guests, but
will include:
• The current Chapter Treasurer
(Committee Chair)
• The current Delegates-at-Large
• Medical Directors or leaders of
current or planned Ohio AAP pro-
jects or programs
• Council and Committee Chairs
• All Chapter members as interested
PIP Meetings:
At least biannually, at Annual Meet-
ing and the Executive Committee
Retreat
The Annual Meeting discussion will
focus on the Chapter’s Programs
and Projects. (This is an excellent
time to propose that new project
that you’ve been planning)
At the Executive Committee Retreat
the focus will be on the Councils’
and Committees’ plans for the up-
coming year. (This is an excellent
way to ensure that your concerns
are heard by the appropriate Council
or Committee.)
Andrew Garner, MD

www.ohioaap.org Ohio Pediatrics • Winter 2011 11
Advertisement

“I have thoroughly enjoyed my time as President of the Ohio
AAP Foundation. We have increased services to children
through starting the My Story Foster Care program, hosting
Healthy, Strong and Ready for Teens and expanding the
Reach Out and Read program. For that, I am especially
proud.” – John Duby, MD
Ohio Pediatrics • Winter 201112 www.ohioaap.org
Ohio Pediatrics
Ohio AAP Foundation will continueto flourish under new leadership
After serving four years as thePresident of the Ohio AAP Foun-dation, John Duby, MD, has formal-ly stepped down to explore other op-portunities.
“I have thoroughly enjoyed mytime as President of the Ohio AAPFoundation,” states Dr. Duby. “Wehave increased services to childrenthrough starting the My Story FosterCare program, hosting Healthy,Strong and Ready for Teens – a full-day symposium for parents and med-ical providers of pre-teen girls – andexpanding the Reach Out and Readprogram. For that, I am especiallyproud.”
In addition to supporting new pro-grams, under Dr. Duby’s leadership,the Foundation has expanded by-laws; increased Board membership toinvolve new physicians, as well asnon-physician community members;and hired a development officer tocoordinate Foundation activities andfundraisers.
The first Ohio AAP FoundationGolf Outing and Breakfast for Books(a fundraiser for Reach Out and ReadOhio) events were both held in 2007,in direct response to the increaseddevelopment of the Foundation.
The number of children served byReach Out and Read programsthroughout Ohio has nearly doubledin the past four years, now servingapproximately 155,000 childrenannually. “When I started as Foun-dation president, I always hoped wecould have at least 150 programs inOhio by 2012. With 144 sites now, Ithink we are definitely on pace toreach that goal,” he said.
“I feel the Foundation is poised to
flourish in the next few years,” hecontinued, “especially under theskillful leadership of Dr. Duffee,”who replaced Dr. Duby as presidentin January.
Jim Duffee, MD, is the founderand Chief Medical Officer of theRocking Horse Center, a FederallyQualified Health Center, in Spring-field. Dr. Duffee has previouslyserved on the Ohio AAP FoundationBoard of Trustees, has been activewith the Ohio AAP Chapter, and re-ceived the Chapter’s Outstanding
Welcome new Foundation board membersAt the most recent Ohio AAP Foundation Board meeting in November,
the Foundation also voted to accept the nominations of four new Boardmembers. Marisha Agana, MD; Michael McCabe, MD; Phil Heit; andJudy Romano, MD, were all unanimously voted to the Ohio AAPFoundation Board for a four-year term ending in 2014.
• Dr. Agana is a community pediatrician in Cortland, practicing at thePediatric Corporation of Warren.
• Dr. McCabe is a pediatrician at Aultman Health Foundation in Canton.
• Dr. Romano is serving on the Foundation board as president-elect of theOhio AAP, and is a pediatrician at Wheeling Hospital in Martins Ferry.
• Phil Heit is professor emeritus of Physical Activity and EducationalServices at The Ohio State University.
For more information on serving on the Ohio AAP Foundation Boardof Trustees, please contact Heather Hall, Assistant Executive Director,Ohio AAP Foundation at [email protected], or (614) 846-6258.
Pediatrician of the Year Award in2008.
“John has done a tremendous job ingrowing the Ohio AAP Foundationthe past few years, and I look for-ward to building on the groundworkhe has already created,” said Dr.Duffee. “It won’t be easy followingin his footsteps, but his vision andforward thinking has prepared theFoundation to be successful for yearsto come.”
“Thank You” to Ohio AAP Foundation
supporters can be found on page 22.

www.ohioaap.org Ohio Pediatrics • Winter 2011 13
WHAT CAN THE PHYSICIAN DO TO START TREATMENT?
Initial treatment includes rest, ice, and the use of crutches until the
athlete can walk without a limp. Knee immobilizers are not neces-
sary and use should be limited to one to two weeks. Early range-of-
motion exercises are important. Full extension and flexion should be
regained as soon as pain and swelling permit and can easily be moni-
tored in the athletic training room of high schools or colleges that
have a full time ATC on staff. Physical therapy after surgery is im-
perative to regain knee strength and function for sport, teach the ath-
lete to use the knee correctly in sports-specific movements, and train
the athlete in safe landing techniques to help prevent future injury or
re-injury. ACL braces are poor at controlling translational or rota-
tional forces but are useful for initial treatment and post-operatively.
The use of a brace will not substitute or avoid the need for surgery
for those desiring to return to agility sports. Nonoperative treatments
have limited success and often result in recurrent instability and irre-
versible damage to intra-articular cartilage or meniscal structures.
WHY ARE FEMALES MORE PRONE TO ACL INJURIES?
Hormonal (estrogen levels during various stages of the menstrual
cycle), anatomic, and neuromuscular differences between girls and
boys, although controversial, are thought to play a role in the in-
creased ACL injury risk to female athletes, but biomechanical fac-
tors appear to be the most important. Females are more likely to per-
form cutting maneuvers and land from jumps in a more erect posi-
tion than males with extended knees and hips and drop their knees
into a more valgus position. This generates abnormally high tension
on the ACL, making it more prone to non-contact tears. ACL tear
prevention programs have been seen to reduce the incidence of non-
contact ACL tears by about 70-80% in girls ages 14-18. Programs
concentrate on avoiding the “position of no return” by increasing
flexibility and strength, improving balance and landing techniques
through agility training, and including sports-specific training in the
program to give more “real time” experience.
SUMMARY
WHAT IS THE ACL (ANTERIOR CRUCIATE LIGAMENT)?
The ACL is an intra-articular ligament in the center of the knee joint,
providing the majority of stability in the knee. It is the primary re-
straint to anterior translation of the tibia relative to the femur and is a
secondary restraint to rotation and angulation; particularly during
weight bearing. Stability in the knee joint with cutting and pivoting
motions is important to help avoid meniscal and other ligamentous
tears, articular cartilage damage, and other internal derangement of
the knee.
WHEN SHOULD ONE SUSPECT AN ACL TEAR?
A knee injury that occurs while cutting, pivoting, or landing from a
jump, is described as a “pop” and swells within the first two to six
hours (indicating a hemearthrosis) has a high likelihood of including
an ACL tear. Most athletes are unable to continue to play, but some
may be able to finish the game or practice. The ACL can also be
injured when an athlete sustains a hit or direct contact to the knee.
Physical examination can be difficult due to patient discomfort and
guarding. A mobile joint effusion is common, although, rarely, the
ACL can be torn without producing an effusion. The Lachman test, a
test to evaluate integrity of the ACL, may be loose or noted to lack a
firm endpoint. Examination of the contralateral knee is helpful to
compare ACL integrity to an injured knee, if that knee has not been
previously injured. A false negative Lachman test can be produced
when hamstring spasm (due to pain and guarding) masks anterior
translation of the tibia on the femur.
WHAT IMAGING IS NECESSARY?
A four-view radiograph series, including an AP, lateral, tunnel or
notch view, and a sunrise/Merchant view should be done to assess for
possible fracture, physeal (growth plate) damage, osteochondral le-
sions and loose bodies. A Segond fracture (small fleck fracture from
the lateral tibia seen just proximal to fibular head on the AP radio-
graph), can indicate an ACL tear on plain film. An avulsion fracture
of the tibial spine can indicate instability of the ACL in the very
young athlete. MRI is indicated in cases of suspected ligamentous
instability, possible meniscal or cartilage injury or persistent symp-
toms of swelling, pain and/or instability for more than three weeks.
WHAT IS THE TREATMENT?
An athlete with a suspected ACL injury should not be allowed to re-
turn to sports participation without an evaluation by a primary care
sports medicine specialist or an orthopedic surgeon. For young, ac-
tive individuals, ACL reconstruction provides the best opportunity for
a successful return to agility sports. Young athletes with open physes
or growth plates should still be referred early for surgical consulta-
tion – depending on the stage of growth, reconstruction may be de-
layed to allow for closure of the physes and a traditional repair, ver-
sus a physeal-sparing procedure done by orthopedic specialists.
Sports ShortsGuidelines for Pediatricians
This information is available on the Ohio Chapter, American Academy of Pediatrics’ website at www.ohioaap.org
ACL Injuries in Female Athletes
Author: Anastasia Fischer, MD.
Sports Shorts is provided by the Home and School Health Committee of the Ohio Chapter,
American Academy of Pediatrics.
Mechanism of injuryNon-contact collapse into valgus (knock-kneed)
position +/-“pop”
Physical examination Effusion, decreased ROM, instability with Lachman test
ImagingX-rays often normal; MRI 85-90% accurate for
ACL tears
Initial treatmentIce, rest, ROM exercises, possible bracing, limitation
of activity
Definitive treatmentSurgical reconstruction of the ACL and repair to
any associated structures
Associated injuries
Meniscal tears, other cartilage or collateral ligament
injuries, consider growth plate injuries if skeletally
immature

14 Ohio Pediatrics • Winter 2011
WHAT IS ACL?
The ACL is an acronym for the Anterior Cruciate Ligament, a stabi-
lizing ligament of the knee that connects the femur (thigh bone) to
the tibia (shin bone). This ligament prevents the tibia from sliding
forward on the femur, and helps to protect the knee during pivoting
and shifting while running or jumping/landing. It is named cruciate
for “cross” because it crosses the posterior cruciate ligament (PCL)
inside the knee. Stability within the knee is important to protect
other structures in the knee, such as the meniscus (cartilage).
WHEN SHOULD ONE SUSPECT AN ACL TEAR?
A knee injury that occurs while cutting, pivoting, or landing from a
jump, is described as a “pop” and swells immediately has a high
likelihood of including an ACL tear and should be evaluated in the
very near future. Most athletes are unable to continue to play, but
some may be able to finish the game or practice. The ACL can also
be injured when an athlete sustains a hit or direct contact to the
knee.
WHEN SHOULD AN INJURED ATHLETE SEEK
MEDICAL CARE?
1. Any time there is moderate or severe pain, swelling and/or the
inability to bend or straighten the leg completely.
2. When an athlete cannot continue to play that day or has difficulty
with walking, running or jumping for the next few days after the
injury.
3. When an athlete complains of “looseness” or giving way in the
knee from either a new or an old injury. Any athlete with a suspect-
ed ACL injury should NOT be allowed to return to sport participa-
tion without an evaluation by a primary care sports medicine spe-
cialist or an orthopedic surgeon. Continuing to play sports with a
torn ACL can lead to further injury and/or permanent damage.
WHICH ATHLETES GET ACL TEARS?
Any athlete can tear their ACL. Common ages are 15-25 years old,
but ACL tears are now being seen in children as young as 10 years
old. Female athletes are injured four to five times more frequently
than males. ACL tears occur in all sports, but jumping, cutting, and
pivoting sports such as basketball, soccer and other court or field
sports are at higher risk.
WHY IS THE ACL MORE COMMONLY INJURED INFEMALES?
Hormonal (estrogen levels during various stages of the menstrual
cycle), anatomic, and neuromuscular differences between girls
and boys, although controversial, are thought to play a role in the
increased ACL injury risk to female athletes, but biomechanical
factors appear to be the most important. Females are more likely to
perform cutting maneuvers and land from jumps in a more erect
Sports ShortsGuidelines for Parents, Coaches, Athletes
This information is available on the Ohio Chapter, American Academy of Pediatrics’ website at www.ohioaap.org
ACL Injuries in Female Athleteposition than males with extended knees and hips and drop their
knees into a more valgus position. This generates abnormally high
tension on the ACL, making it more prone to non-contact tears. ACL
tear prevention programs have been seen to reduce the incidence of
non-contact ACL tears by about 70-80% in girls ages 14-18. Pro-
grams concentrate on avoiding the “position of no return” by increas-
ing flexibility and strength, improving balance and landing techni-
ques through agility training, and including sports-specific training in
the program to give more “real time” experience.
WILL TESTS NEED TO BE DONE?
Almost all suspected ACL injuries are severe enough that X-rays are
necessary. An additional test called an MRI (magnetic resonance
imaging) is often also done to confirm the ACL tear and look for
damage to associated cartilage (meniscus), ligaments, or the joint
capsule.
WHAT IS THE TREATMENT?
The most successful treatment for an ACL tear is arthroscopic
surgery. A new ligament is made to “reconstruct” the old injured
ACL, usually from a piece of the athlete’s own tendon. The surgery
is not performed emergently, and treatment is often initiated with
rest, ice, and crutches, if necessary. A brace may be used before
and/or after surgery to help support the knee. Physical therapy will
be very important after the surgery (and sometimes before) to help
the knee regain its motion and strength, train the athlete to return to
sports, and to do injury-prevention exercises to help protect the new
ACL graft.
IS SURGERY NECESSARY?
Nearly all ACL tears in a young athlete should be repaired to ensure
a safe return to activity. Return to sports generally takes about six
months to ensure that the new ACL graft has full strength and heal-
ing, and to ensure that the athlete is strong and healthy enough to use
the knee. In general, athletes are able to return to their previous level
of activity without pain or limitation once fully recovered. Athletes
who choose to avoid having recommended surgery can have prob-
lems with pain, weakness, giving out/instability and can develop
knee arthritis at a young age.
ARE ACL TEARS PREVENTABLE?
Many non-contact ACL tears are preventable by programs called
“ACL prevention programs.” These programs have been designed to
help athletes avoid positions that make the knee more prone to ACL
tears by strengthening the knee and teaching agility and positioning
during activity and sport.
Author: Anastasia Fischer, MD.
Sports Shorts is provided by the Home and School Health Committee of the Ohio Chapter,
American Academy of Pediatrics.
15www.ohioaap.org Ohio Pediatrics • Winter 2011
Ohio Pediatrics
A 6-month-old child receives the following vaccines:
Pentacel® (DTaP-Hib-IPV) vaccine (five vaccine compo-nents)Hepatitis B (one vaccine component)PREVNAR 13™ (one vaccine component)Rotateq® (one vaccine component)
Whereas previously you would have reported that fourvaccines were administered, under the new codes, youwould report that eight vaccine components were admin-istered.
In the example above, the codes would be reported asfollows:Vaccine Product/Code Immunization Administration Code
Pentacel® /90698 90460, 90461, 90461, 90461, 90461
Hepatitis B/90744 90460
Prevnar 13™/90670 90460
Rotateq® /90680 90460
Change to such an important part of a general pediatri-cian’s practice requires careful communication to bothproviders and payers, so there have been major nationaland Ohio Chapter efforts in the last few months.
The new codes were explained at the Chapter’s AnnualMeeting by District Vice-Chair and coding expert Rick
Tuck, MD. National AAP President O. Marion Burtonwrote to medical directors of insurance plans, askingthem to be ready on Jan. 1 to pay for the new codes.Ohio AAP President Jerry Tiberio likewise wrote toOhio’s medical directors who participate in our PediatricCouncil representing Anthem-Wellpoint, Summa-Care,UHC, Medical Mutual, ProMedica, Medicaid, Centene,Molina, Caresource, CIGNA, and AmeriGroup. The letterasserted there should be a seamless updating of insurancecompanies’ payment system, stating that “America’s vac-cine program depends on a reliable private sector deliv-ery system. Pediatric offices in turn depend on an unbro-ken cycle of ‘supply-service-payment-resupply’ for ex-pensive vaccines and significant administration costs.”The letter reminded insurance companies that the HealthInsurance Portability and Accountability Act of 1996(HIPAA) requires that covered entities must recognizenew/revised CPT codes starting on January 1, 2011.
– Jon Price, MD
Chair, Pediatric Care Council
See Dr. Tuck’s coding column on page 16.
CPT...from page 1
CPT code and description Physician Work
RVUs
Practice Expense RVUs
(non-facility)
Professional
Insurance
Liability RVUs
Total RVUs Total RVUs 2011
Medicare Conversion
factor ($25.5217) =
Medicare Amount
90460 Immunization administration through 18 yearsof age via any route of administration, withcounseling by physician or other qualified health-care professional; first vaccine/toxoid component
0.17 0.50 0.01 0.68 $17.35
90461 Immunization administration through 18 years
of age via any route of administration, with counsel
ing by physician or other qualified health-care profes-
sional; each additional vaccine/toxoid component.
(List separately in addition to code for primary
procedure.)
0.15 0.18 0.01 0.34 $8.68
90471 Immunization administration, one injection 0.17 0.50 0.01 0.68 $17.35
90472 Immunization administration, each additional
injection0.15 0.18 0.01 0.34 $8.68
90473 Immunization administration by intranasal/oral
route, first administration0.17 0.50 0.01 0.68 $17.35
90474 Immunization administration by
intranasal/oral route, each additional vaccine0.15 0.18 0.01 0.34 $8.68
2011 MEDICARE RELATIVE VALUE UNITS FOR IMMUNIzATION ADMINISTRATION

16 Ohio Pediatrics • Winter 2011 www.ohioaap.org
Ohio Pediatrics
Understanding and using new IA codes will increase your practice’s bottom line
Coding Corner
The major 2011CPT change forpediatricians is theaddition of newpediatric immu-nization adminis-tration codes. Im-plementing thesecodes will be sub-ject to predictableturmoil. However,understanding the application andlimitations of the codes will providean opportunity for increased reim-bursement for the immunization ser-vices that are central to providingquality pediatric care.
The new immunization codeswere developed at the request ofpracticing pediatricians who wereexperiencing significant decreasedincome related to the loss of immu-nization administration fees usingthe newer combination vaccines.The new codes, if used, recognized,and paid properly, should makepediatricians financially whole forthe combination vaccines they pro-vide.
As of Jan. 1, the old 90465-90468pediatric immunization codes havebeen deleted and replaced by thenew 90460-90461 code set. The newcodes are for patients who arethrough 18 years of age, receivingimmunizations delivered by anyroute of administration, and involv-ing counseling by a physician orother qualified health-care person-nel. The codes are determined bythe number of disease componentsin the vaccine. A component is de-
fined as the antigen in a vaccine thatprevents disease caused by one or-ganism. Examples of the number ofcomponents in a vaccine:IPV 1 componentMMR 3 componentsDTaP-HIB-IPV 5 components
The code specifics:90460 – Immunization administra-tion through 18 years of age via anyroute of administration, with coun-seling by physician or other quali-fied health-care professional; firstvaccine/toxoid component.
90461 – Immunization administra-tion through 18 years of age via anyroute of administration, with coun-seling by physician or other quali-fied health-care professional; eachadditional vaccine/toxoid compo-nent. (List separately in addition tocode for primary procedure.)
CPT has simplified vaccine ad-ministration by providing the 90460universal base code for each vaccineprovided.
The two new requirements forthese codes, in addition to age, de-serve some attention. “Counseling”requires discussion with the parents,addressing concerns and questionsregarding each vaccine product ad-ministered, as well as, how to treatassociated vaccine reactions. Thiswould be supported by discussingthe use and dosage of acetamino-phen or ibuprofen, if needed. Spe-cific documentation of this counsel-ing should be made. The definitionof “other qualified health-care pro-fessional” is determined by individ-
ual state scope of practice. As ofthis printing, Ohio AAP was unableto get a definitive answer from oursources on who qualifies. We willcontinue to research this and keepyou informed on the Chapter’s web-site and in our e-newsletters.
Understanding the coding billingissues for the new codes is impor-tant. The administration codesshould be “paired” with the productprovided. They should be listed asline items below the product on thesame CMS 1500 page. The initial90460 for each vaccine will be fol-lowed by 90461, listed multipletimes, or documented in units, asdetermined by each payer. You willalways report the +90461 in addi-tion to 90460. The AAP is workingwith claims management companiesto clarify and encourage this multi-ple unit claim procedure.
The 90471-90474 immunizationadministration code series remainunchanged in CPT to use for youngadults ≥19 years if age, or whencounseling is not provided by thephysician or other qualified health-care professional.
The AAP has also made the ICD-9diagnosis coding recommendation touse V06.8 for the six combinationvaccine products. For all other prod-ucts, continue using the V03-V05specific codes. Remember that forvaccinations provided at a preven-tive medicine visit, linking them toV20.2 (well infant/child visit) re-mains the payer accepted and easiestmethod of diagnosis billing.
Richard Tuck, MD
See Coding...on page 20

www.ohioaap.org 17Ohio Pediatrics • Winter 2011
Ohio Pediatrics
Award...from page 1
Large Chapters from the AAP;membership in general increased;and attendance at meetings andevents also increased. He was in-strumental in Reach Out and ReadOhio receiving $200,000 from thestate budget, and in increasing theMedicare reimbursement for Ohiophysicians.
Dr. Cotton serves on the OhioAAP Foundation Board, as well asthe Advisory Board of Reach Outand Read Ohio. Dr. Cotton hasmade the commitment to get in-volved in a wide range of relatedorganizations as well, including theOhio State Medical Association, theColumbus Medical Society, Emer-gency Medical Society and nationalAAP. He has also been a leader atthe hospital level serving as presi-dent of Nationwide Children’s Hos-pital Medical Staff demonstratinghis leadership skills.
As advocacy chair of Ohio AAP,Dr. Cotton has testified on numerouslegislative issues for the well-beingof Ohio’s children including boosterseats, immunization funding and theMedicaid budget. As chair of the ad-vocacy committee, Dr. Cotton’s tire-less efforts increased the primarycare reimbursement rate for Medi-caid and vaccine immunizationfunding by 100%.
Dr. Cotton’s great sense of humorand quick wit makes him adored bypatients and staff. The OutstandingPediatrician Award focuses on long-term achievement. Dr. Cotton’scommitment to the Ohio AAP; hisnotable contributions to pediatrics;his educating of patients and physi-cians in Ohio; and patient care madehim an ideal recipient of this award.
Immediate Past President Terry
Barber, MD, was recognized for hisleadership, achievements, and out-
standing contributions to the ad-vancement of the Ohio AAP duringhis term as Chapter president from2008-2010.
During his tenure as president, Dr.Barber’s infectious positive attitudeled to major accomplishments. Dr.Barber tackled the growing child-hood obesity epidemic initiating theOunce of Prevention Program; tookmajor strides in treating childrenwith asthma in the asthma qualityimprovement program; provided lit-erature focusing on parental refusalof vaccines through a HealthyPeople 2010 grant; and re-energizedthe Young Physicians and ResidentsCommittee. He also took the Chap-ter’s communications to the nextlevel by encouraging growth in so-cial media and electronic publica-tions.
Others receiving awards were:Rep. John Carney, a member of
the Ohio House of Representatives,
received the Antoinette Parisi EatonAdvocacy Award, for advocating forchildren and furthering the missionof the Ohio AAP in 2010. He willformally receive his award at theBreakfast for Books event this sum-mer.
Cooper White, MD, and Kim
Spoonhower, MD, received theLeonard P. Rome Award. This awardis presented to a Chapter member,or members, whose leadership fur-thers the mission of the Ohio AAPthrough a specific program or pro-ject. Drs. White and Spoonhowerwere honored for their work withthe Chapter’s Quality NetworkAsthma Pilot Project. During thisproject, the physicians have guided13 Ohio practices in improving asth-ma care for children.
The Outstanding Committee ChairAward was presented to Emily
Decker, MD, Nationwide Children’sHospital; Norah Ledyard, DO, TheRocking Horse Center; and Allison
Brindle, MD, Cleveland Clinic.These three women dedicated theirtime to increasing involvement ofyoung pediatricians and residents atOhio AAP meetings and in state leg-islative initiatives. They also assem-bled an outstanding, sold out, Advo-cacy Day in May 2010. This work-ing mom team accomplished all ofthis in addition to their professionaland home commitments, includingtending to newborns.
Natalie Riedman, MD, Nation-wide Children’s Hospital, received aSpecial Achievement Award, for herunending work on the AdvocacyDay program and for her effortswith the Young Physicians Commit-tee.
David Roer, MD, member of theExecutive Committee at DaytonChildren’s Hospital, received theArnold Friedman Community Pedi-atrician Award. Dr. Roer focuses hisvolunteering primarily on child-re-lated issues. As a result of an inter-view with the Wall Street Journal in2003, Dr. Roer was able to get junkfood out of school vending ma-chines. Even before Ohio’s smokingban was established, he was able torid the Centerville City schools ofsmoking by teachers in all of theschool buildings. He also led ahealth initiative to improve thenutritional value of school lunches.Dr. Roer is chair and one of thefounding members of the SouthSuburban Coalition – a coalitionthat fights teenage drug and alcoholuse. In 2008, Dr. Roer and his wiferaised $100,000 for a March ofDimes event that they co-chaired.
Congratulations to all the recipi-ents.

18 Ohio Pediatrics • Winter 2011 www.ohioaap.org
Ohio Pediatrics
Ohio AAP Annual Meeting 2010
William Cotton, MD, left, receives thePediatrician of the Year Award fromOhio AAP President Gerald Tiberio,MD, at the Ohio AAP’s Annual AwardLuncheon in November.
In her presentation onParental Refusal ofVaccines, Ari Brown,MD, National AAPspokesperson, saidparents who delaytheir child’s vaccina-tions are playingRussian Roulette.
At the Opening Reception of the 2010Annual Meeting attendees of all ageswere entertained with visitors from theColumbus zoo and Aquarium.
David Roer, MD, left, receivedthe Arnold Friedman Commu-nity Pediatrician Award for hisnumerous hours of volunteerservices focusing primarily onchild-related issues. In 2008, Dr.Roer and his wife, raised$100,000 for a March of Dimesevent that they co-chaired.
The Outstanding Committee Chair Awardwent to the team of (from left) NorahLedyard, DO, Emily Decker, MD, andAllison Brindle, MD, for their work on theYoung Physicians/Residents Committee.They also assembled a sold out AdvocacyDay last year. Natalie Riedman, MD,(right, next to Dr. Tiberio) received aSpecial Achievement Award for her con-tributions to the Advocacy Day program.
Immediate Past President TerryBarber, MD, (left) was honoredfor his many accomplishmentsduring his term as president,and for challenging everyone tostep out of their comfort zoneand make changes to better theChapter.

Ohio Pediatrics
19www.ohioaap.org Ohio Pediatrics • Winter 2011
Attendees at the Annual Meeting Members-Only Breakfastreceived an update from Ohio AAP President Gerald Tiberio, MD,on Chapter activities, as well as legislative updates from theChapter’s lobbyists. Also, P. Cooper White, MD, gave a brief pre-sentation on the Asthma Quality Improvement Pilot Project.
President-Elect Judy Romano, MD,is pleased with the bottle of wineshe won in the fundraiser for theOhio AAP Foundation.
Robert Frenck, MD, left, andImmediate Past President TerryBarber, MD, discuss the days activ-ities at Friday’s Opening Receptionof the Ohio AAP Annual Meeting.
Meg Fisher, MD, right, of MonmouthMedical Center, one of the nationalspeakers at the Annual Meeting, talkswith attendees following her presenta-tion on “Vaccines, Not Just forBabies.”
Ohio AAP President Gerald Tiberio,MD, left, congratulates John Duby,MD, for his years of service as presi-dent of the Ohio AAP Foundation.After four years, Dr. Duby has steppeddown to explore other opportunities.
P. Cooper White, MD, right, receivedthe Leonard P. Rome Award for hiswork on the Chapter’s Quality Net-work Asthma Pilot Project. KimSpoonhower, MD, was also honoredbut unable to attend the luncheon.During this project, the physicianshave guided 13 practices from aroundthe state in improving asthma care forchildren.
Bob Murray, MD, brought mem-bers up-to-date on the activities ofthe Statewide Obesity Preventionand Wellness grant. Dr. Murrayalong with Amy Sternstein, MD,have presented Ounce of Preven-tion information to nearly 250health-care professionals in thestate.
Allison Brindle, MD, tries herhand with the Wine Ring Tossheld during the Opening Recep-tion of the 2010 Annual Meeting.All the proceeds from the ringtoss, as well as the wine raffle,went to the Ohio AAP Founda-tion.

Ohio Pediatrics
Critical decision support available 24/7To address a shortage of child and
adolescent psychiatrists in Ohio, theOhio Department of Mental Healthand provider organizations acrossthe state have launched PediatricPsychiatry Network, an easy-accessconsultation and support service forprimary care physicians.
The purpose of the network is tohelp primary care doctors deliverand coordinate care for Ohio’s youthby direct answers to physician ques-tions regarding mental health diag-nosis and treatment.
“Ohio youth with psychiatric dis-orders and their primary care physi-cians have had critical problemsgaining access to needed care,” saidMarion E. Sherman, MD, medicaldirector at the Ohio Department of
Mental Health. “This network pro-vides rapid access to professional re-sources for consultations. It enablesfamily doctors to better meet theneeds of Ohio’s children throughearly detection of psychiatric symp-toms and proactive positive inter-vention.”
The network provides primarycare physicians the ability to accesschild and adolescent psychiatry de-cision support, education and triageservices 24 hours a day, seven daysa week. Future services are plannedto include consultations using video,e-visits and telemedicine.
The network of providers is linkedthrough technology and can be ac-cesed through a call-center numberand website. The technology infra-
www.ohioaap.org20 Ohio Pediatrics • Winter 2011
structure and clinical protocols weredeveloped using Ohio’s Transforma-tion State Incentive Grant funds fromthe Substance Abuse and MentalHealth Services Administration.
Network providers taking calls in-clude Akron Children’s Hospital,Northeastern Ohio Universities Col-lege of Medicine, Cincinnati Chil-dren’s Hospital Medical Center, Uni-versity of Cincinnati, NationwideChildren’s Hospital, The Ohio StateUniversity, Toledo Children’s Hos-pital and University of Toledo. Addi-tional network development supportwas received through Wright StateUniversity, Cleveland Clinic andUniversity Hospitals/Rainbow Babies& Children’s Hospital.
To request a consultation, Ohio pri-mary care physicians may call 1-877-PSY-OHIO, or complete a requestform at www.pedpsychiatry.org.
The Ohio AAP Pediatric Council isaggressively addressing the HIPAArequired recognition and use of thenew codes and has sent out letters toour major state payers (see story onpage 1). National AAP is providing asummary of ongoing communicationwith the major national payers re-garding their policies related to thenew IA codes, as well as, a list ofFAQs from members seeking guid-ance with implementation of thecodes. You can find these at www.aap.org, members-only site, PMO(practice management online).
If we work together to pursue recognition of the new IA codes, theresult will be an increase in our prac-tice’s bottom line!
– Richard Tuck, MD, Zanesville
Ohio AAP Coding Expert
Coding...from page 16
100’s of Physiciansseeking jobs in Ohio
Medical Opportunities in Ohio (MOO) www.ohmoo.org – serves hospital employers
and private practices with an online recruitment
program, designed to connect Physicians,
Physician Assistants, and Nurse Practitioners
with jobs in Ohio. Job seekers register for
FREE! Our database of Physicians spans
more than 85 specialties!
Employers, contact us today to learn
more about how the MOO program can
work for you!
800.479.1666www.ohmoo.org

Ohio Pediatrics
The 2008 National ImmunizationSurvey, a survey of vaccination cov-erage among U.S. children by age36 months, was released in August2010. The most identifiable changein this years survey is the survey’sbenchmark for up-to-date percent-ages by age 36 months has changedfrom the prior 4:3:1:3:3:1 series (4DTaP, 3 Polio, 1 MMR, 3 Hib, 3Hepatitis B and 1 Varicella vac-cines) to a 4:3:1:3:3:1:4 serieswhich now includes 4 Pneumococ-cal vaccines.
The National Average for the4:3:1:3:3:1:4 series for 2008 was
63.3%. Ohio’s average for 2008 was68.8%. Once again Ohio is abovethe national average and 5th highestin the country. We should continueto be proud of Ohio’s coveragecompared to the national average,this is however a lower up-to-datepercentage than we have seen in thepast few years with the prior series.
The Ohio percentage for the4:3:1:3:3:1 in 2008 was 68.8% andin 2007 was 80.1%. For the past fewyears the AFIX measurements fromthe Ohio Department of Health havereported individual practice up-to-date percentages using both of the
series measurements. While the newseries may show a lower up-to-datepercentage compared to prior data,this will be the benchmark movingforward.
For practices that have had anAFIX measurement in the past fewyears, it may be beneficial to reviewthe prior data on up-to-date percent-ages and move forward as practicesreview their patients vaccine recordsto pay attention to their Pneumo-coccal (PCV) percentages.
– Ryan Vogelgesang, MD
MOBI Medical Director
Survey of vaccination coverage makeschange to benchmark PCV percentages
www.ohioaap.org 21Ohio Pediatrics • Winter 2011
We proudly announce that American Physiciansand � e Doctors Company have united.
Together, we set a higher standard. We aggressively defend your name. We protect good medicine. We reward doctors for their loyalty. We ensure members bene� t from our combined strength. We are not just any insurer. We are a company founded and led by doctors for doctors. We are the largest national insurer of physician and surgeon medical liability.
On October 22, 2010, � e Doctors Company and American Physicians o� cially joined forces. With the addition of American Physicians, we have grown in numbers, talent, and perspective__strengthening our ability to relentlessly defend, protect, and reward our nearly 55,000 members nationwide. To learn more about how we can protect your livelihood and reputation with our medical professional liability program, call (800) 666-6442, or visit us at www.thedoctors.com.
We relentlessly defend, protect, andreward the practice of good medicine. American Physicians
www.thedoctors.com

www.ohioaap.org22 Ohio Pediatrics • Winter 2011
The Ohio AAP Foundation would like to thank the following
individuals, hospitals and companies for their support in 2010.
Marisha Agana, MD
Akron Children’s Hospital+
Alice Appel
Razan Alkhoury, MD
Wendy Anderson, MD
Kevin Arnold, PhD &
Melissa Wervey Arnold
Justin Baker
Terry Barber, Sr, MD & Jackie
Barber
John Barnard, MD
Sally Baronda
Claudia Barrett
Ken Barton
Greg Bates, MD
Kerry Bierman
Borders
Allison Brindle, MD
Luke Brown
Max Brown*
Vivian Brown
Jeff Brubaker
James Bryant, MD
Buckeye Community Health
Plan*
Shelley Callahan
Karen Carbaugh
Shareena Casey
Center for Cognitive and
Behavioral Therapy of
Greater Columbus+
Children’s Practicing
Pediatricians*
Jeff Combs
Frank Combs
Commerce National Bank*
William Cotton, MD and
Patricia Davidson, MD
Kim Davis
Emily Decker, MD
Isaac DeLeon
Mark Denny, MD & Sarah
Denny, MD
Emanuel Doyne, MD &
Ellen Doyne
Dan & Rebecca Dragin
John Duby, MD & Sara
Guerrero-Duby, MD*+
Jim Duffee, MD
Brian Engle
Matt Esker
Antoinette Eaton, MD
Kevin Farrell
Jill Fitch, MD
Diana Foreman
Carla Fountaine
Robert Frenck, MD
Mike & Bonnie Gahn
Gardiner Early Learning Center
Andrew Garner, MD
Jessica Gliha
Tamu Gibbs
Joan Griffith, MD
Dan Gusty
Donald Hairston
Edwin & Carol Hall+
Eric & Katherine Hall
Heather Hall
Ginny Haller, MD
Melissa Hook
John Howenstine*
Vera Humes
Industrial Technology
Solutions*
Tracy Intihar
Richard & Sally Jameson+
Leonard Janchar, MD
Todd Jenkins, MD
Johnny Buccelli’s*
John R. Green Company+
Rhonda Johnson
Tracey Johnson
Mike & Cecelia Jokerst
Glenn Karr
Lisa Kelch, MD
Elizabeth Kelleher
Kelly Kelleher, MD
Karen Kirk
Katalin Koranyi, MD
Nick Lashutka
Lori LeGendre+
George Leugers
Andrew Maciejewski
Thad & Barbara Matta*+
McDonalds, USA, LLC+
Jonna McRury, MD
Bruce Meyer, MD
Grant Morrow, MD
Cheryl Morrow-White, MD
Robert Murray, MD
Victor Nanagas, MD & Maria
Nanagas, MD
Nationwide Children’s
Hospital*+
Garey Noritz, MD
Ray & Kathleen Oakes
Ohio Children’s Hospital
Association*
Anahi Ortiz, MD
Jennifer Ortman
Panera*
Mary Ann Partlow
Bindi Patel, MPH
PNC Bank & Grow Up Great
Jennifer Powers
Jonathan Price, MD
Primrose Schools
Dru Qualman
Suzette Rathke
Rattlesnake Ridge Golf Club*
Red Lobster*
David Rich, MD
JoAnn Rohyans, MD
Judy Romano, MD
Elizabeth Ruppert, MD
Rusty Bucket*
Kevin Sheedy
Charles Spencer, MD
Joe Stack
Tom & Debbie Stahl
John Steketee
Amy Sternstein, MD
Nancy Strater
Tim Sullivan
Ben Teske
The Step 2 Company, LLC+
Olivia Thomas, MD
Gerald Tiberio, MD & Clare
Tiberio
University of Toledo Medical
Center, Department of
Pediatrics+
Ryan Vogelgesang, MD
Clare Ward
Lynn Warner
Sharon Werner
Kathy Westfall
Wanda Whipkey
John Wiley
P. Cooper White, MD
Tom York
Julie Zuzolo
Your support enables the Ohio AAP Foundation to sustain its three main programs:
Reach Out and Read Ohio, the My Story Foster Care Program, and the Parent Connection Series
+ Breakfast for Books Sponsor, Table Sponsor or Donor * Ohio AAP Foundation Golf Outing Sponsor or Donor
John Duby, MD, Ohio AAP
Foundation President 2006-2010
Ohio AAP Foundation Golf Outing
at Rattlesnake Ridge Golf Club
Guest Reader, Clark Kellogg, at
Breakfast for Books 2010
Ohio AAP Foundation Wine Raffle
at Ohio AAP Annual Meeting

Ohio Pediatrics
www.ohioaap.org Ohio Pediatrics • Winter 2011 23
Legislation...from page 2
Ohio Senate
Republicans grew their majority inthe Ohio Senate by two seats after avictory in Lorain County and theDayton area. North Ridgeville CityCouncilman Gayle Manning beat in-cumbent Sue Morano and Sen. FredStrahorn lost to Bill Beagle of TippCity. Republicans now hold a 23-10majority in this chamber.
Ohio’s Statewide Offices
Ohio Attorney General – DeWine
Former Republican U.S. Senatorand former lieutenant governor MikeDeWine challenged current Demo-crat Attorney General Richard Cord-ray to serve as Ohio’s lead attorney.DeWine won with 48 percent of thevote.
Ohio Auditor – Yost
Republican Delaware County Prose-cutor Dave Yost and Democrat DavidPepper battled for this seat in the fallelection. Many insiders predicted thisrace would fall to Pepper. However,Yost bested Pepper with a solid 51-44percent victory.
Ohio Secretary of State – Husted
State Sen. Jon Husted (R-Ketter-ing) beat Democrat MaryellenO'Shaughnessy for Ohio’s secretaryof state seat – 54-41 percent of thevote.
Ohio Treasurer – Mandel
Incumbent Democrat Kevin Boycefaced a strong challenge by StateRep. Josh Mandel (R-Lyndhurst).Rep. Mandel won the seat 55-40.
Ohio Supreme Court – Lanzinger,
O’Connor and Pfeifer
Justice Maureen O’Connor (R)won the Supreme Court’s Chief Jus-tice position, easily beating JusticeEric Brown. O’Connor will become
Ohio’s first female Chief Justice. Re-publican Justice Judith Lanzingerbeat back a challenge from DemocratMary Jane Trapp. Justice Paul Pfeiferwas also elected to the court as heran unopposed for his third term.
Key leadership posts announcedfor 129th General Assembly:
Ohio House Republicans
Rep. William Batchelder (R-Medina), speakerRep. Lou Blessing (R-Cincinnati),speaker pro temRep. Matt Huffman (R-Lima),majority floor leaderRep. Barbara Sears (R-Sylvania),assistant majority floor leaderRep. John Adams (R-Sydney),majority whipRep. Cheryl Grossman (R-GroveCity), assistant majority whip.
House Democrats
Rep. Armond Budish (D-Beach-wood), minority leaderRep. Matthew Szollosi (D-Toledo),assistant minority leader Rep. Tracy Heard (D-Columbus),minority whip.Rep. Debbie Phillips (D-Athens),assistant minority whip
Senate Republicans
Sen. Tom Niehaus (R-New Rich-mond), presidentSen. Keith Faber (R-Celina), presi-dent pro temSen. Jimmy Stewart (R-Albany),majority floor leader Sen. Shannon Jones (R-Springboro),majority whip.
Senate Democrats
Sen. Capri Cafaro (D-Hubbard) toremain as Senate minority leaderSen. Shirley Smith (D-Cleveland) is
the assistant minority leaderSen. Edna Brown (D-Toledo), mi-nority whipSen. Jason Wilson (D-Columbiana),assistant minority whip
128th General Assembly Wrap-up
The two-year 128th General As-sembly came to a close with manyreflecting on the inactivity of thissession more than anything. With aRepublican Senate and DemocratHouse and Governor, stalemateswere the standard in this session.Only 58 bills were signed into lawfor this session, compared to an aver-age of 247 bills during the previous20 years.
Ohio AAP did see two bills of in-terest become law. First, House Bill198, sponsored by Rep. Peggy Leh-ner (R-Dayton) to establish patient-centered medical home educationpilot programs for medical students.Additionally, Ohio AAP was also in-volved in SB 210, a bill that was en-acted in June 2010 to establish nutri-tional standards for foods and bever-ages sold in vending machines inschools, as well as creating a pilotprogram for daily physical activity.Ohio AAP also actively advocatedfor a number of agency-level fundingand policy decisions to ensure ade-quate reimbursement for pediatricprimary care and emergency care inlight of fiscal constraints as well astimely and adequate immunizationreimbursement.
Although many challenges lieahead, Ohio AAP and our consultantsat Capitol Consulting Group will beworking to make sure the voices ofOhio’s pediatricians and the childrenare heard loudly and clearly.
– Capitol Consulting Group
Ohio AAP Lobbying Team

The Ohio AAP announces the following meetings and events.
May 13, 2011 – Open Forum MeetingUniversity of ToledoTopics: Electronic Health Record Incentive
Program; and ADEPP - Autism Diagnostic
Learning Session
May 17 – Young Physicians & Residents “Advocacy Day”Riffe Center, Columbus
Aug. 2 – Breakfast for Books Huntington ParkFundraiser for the Ohio AAP FoundationBring your whole family and stay for the ballgame
with the Columbus Clippers following the event.
Aug. 25-27 – Ohio AAP Annual MeetingCherry Valley Lodge & CoCo Key Water ResortTopics: Quality Improvement Roundtable; American
Board of Pediatrics representative discussing MOC;
Medical Home Reimbursement
Calendar of Events
Dues remitted to the OhioChapter are not deductible asa charitable contribution, butmay be deducted as an ordi-nary and necessary businessexpense. However, $40 ofthe dues is not deductible asa business expense becauseof the chapter’s lobbyingactivity. Please consult yourtax adviser for specific infor-mation.
This statement is in refer-ence to fellows, associatefellows and subspecialty fel-lows.
No portion of the candidatefellows nor post residencyfellows dues is used for lob-bying activity.
Ohio ChapterAmerican Academy of Pediatrics450 W. Wilson Bridge Rd. Suite 215Worthington, OH 43085
PRESORTED
STANDARD
Permit No. 156
U.S. Postage
PAID
DUBLIN, OH
Dues disclosure
statement





























