-
Supplement to May/June 2015
A roundtable discussion among retina experts that includes
treatment options and management strategies for diabetic
retinopathy
and diabetic macular edema in their respective countries.
DME DIAGNOSIS AND MANAGEMENT
NEW PARADIGMS IN
Supported via advertising by Allergan and Carl Zeiss Meditec
-
Dinn
er w
ill
be se
rveD
Educational program developed in collaboration with:
Find and register for an upcoming meeting near you at
www.DMe2020.com Diabetic macular edema (DME) is the leading cause
of visual impairment in the diabetic population.
By 2020, more than 42 million people will be living with
diabetes in the US. Given these alarming statistics, understanding
the complex mechanisms of DME and the clinical implications is
critical.
PrOGrAM eDUCATiOnAl ObJeCTives Gain understanding of diabetes
mellitus and the effects of
systemic disease
Gain insights into the effects of diabetes on retinal and
vascular components of the eye
Learn about the emerging understanding of the multifactorial
pathophysiology of DME and potential clinical implications
Quan Dong nguyen, MD, MscProgram Chair, University of Nebraska
Medical Center
nicola Abate, MD The University of Texas Medical Branch
Jay Ambati, MDUniversity of Kentucky
David s. boyer, MDRetina-Vitreous Associates Medical Group
Diana v. Do, MDUniversity of Nebraska Medical Center
Pravin Dugel, MDRetinal Consultants of Arizona
seenu Hariprasad, MDUniversity of Chicago Medicine
Untitled-1 1 5/1/15 3:35 PM
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 3
As rates of diabetes are projected to rise in coming years, so
will the increasing number
of patients with ocular complications from diabetes. Retina
Today convened a panel of
world-renowned experts to discuss the treatment options and
management strategies of
diabetic retinopathy and diabetic macular edema in their
respective countries.
DME DIAGNOSIS AND MANAGEMENT
NEW PARADIGMS IN
PANELISTS:
Rishi P. Singh, MD, ModeratorDr. Rishi is Staff Physician at
Cole Eye Institute and Medical Director of the Clinical Systems
Office at The Cleveland Clinic. He is also Assistant Professor of
Ophthalmology at Case Western University in Cleveland, Ohio. He
serves as a consultant for Alcon, Bayer, Genentech, Regeneron,
Shire, and Thrombogenics. Dr. Singh may be reached at
[email protected].
Paolo Lanzetta, MD, is an Associate Professor in the Department
of Ophthalmology at the University of Udine, Italy. He reports
having a financial relationship with Alcon, Alimera, Allergan,
Bausch + Lomb, Bayer, Genentech, Lutronic, Novartis, Roche, and
Teva. Dr. Lanzetta may be reached at [email protected].
Anat Loewenstein, MD, is Director of the Department of
Ophthalmology at Tel-Aviv Medical Center, and a Professor and Vice
Dean of the Sackler School of Medicine at Tel-Aviv University,
Israel. She reports having a financial relationship with Allergan,
Alcon, Bayer, Lumenis, NotalVision, and Novartis. Dr. Loewenstein
may be reached at [email protected].
Edoardo Midena, MD, PhD, is Professor and Chairman of the
Department of Ophthalmology at University of Padova in Italy. He
reports no financial interests. Dr. Midena may be reached at
[email protected].
Gisèle Soubrane, MD, PhD, is Professor and Chair In
Ophthalmology at the Eye University Clinic of Créteil in France.
She reports having a financial relationship with Allergan, Bayer,
Biocodex, and Théa. Dr. Soubrane may be reached at
[email protected].
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
4 SUPPLEMENT TO RETINA TODAY MAY/JUNE 2015
A Roundtable Discussion onNew Paradigms in DME Diagnosis and
Management
Dr. Singh: To begin, let us discuss diabetic patients in your
region. How do diabetic patients get to you as a specialist in your
region?
Prof. Midena: At our clinic in Italy, we see patients after a
telemedicine screening. Most of that occurs in the diabetes
clinics, so patients are not attending our clinics for naïve
evaluation. They are already pre-screened for DR, which, of course,
means they need immediate treatment.
Prof. Soubrane: At my hospital in France, we have a special unit
called diabetic ophthalmology. The endo-crinology department refers
all patients (diabetic or sus-pected diabetics) to that unit where
they will be seen on a regular basis, depending on their initial
presenting state of retinopathy.
Prof. Loewenstein: In Israel, we have a combination of
telemedicine and direct retinal examinations. There is a great
system of primary care physicians who are all fel-lowship trained,
and they know they need to screen the patients. These patients are
usually fairly well controlled systemically, know their A1c level
and they are informed about treatments. But we also have a growing
popula-tion of immigrants, mainly from Russia and Ethiopia, who
present with extremely poor vision and advanced disease. So, we
address the combination.
Prof. Lanzetta: In Udine, patients are either referred by
general ophthalmologists or by a diabetologist in the medical
department. Similar to what Prof. Loewenstein discussed with her
first patient group, we are rela-tively lucky because we usually
see very well-controlled
According to the International Diabetes Federation, there are
cur-rently 387 million people living with diabetes (a preva-lence
rate of 8.3%), and this figure is expected to top 590 million by
2035.1 Europe has the highest prevalence of type 1 diabetes in
children.1 The prevalence of diabetes is slightly lower than the
world-wide figures, at 7.9%.
The World Health Organization now counts dia-betes among the top
10 causes of death worldwide, respon-sible for 1.7 million deaths
in 2012 (up from 1.0 million in 2000).2 The numbers are just as
dire when it comes to the ophthalmic complications of
diabetes—there are about 93 million people with diabetic
retinopathy (DR), 17 mil-lion with proliferative DR, 21 million
with diabetic macular edema (DME), and 28 million with
vision-threatening DR.3
It is clear that retina specialists around the world will
continue to see increasing numbers of patients with ocu-lar
complications from diabetes. Retina Today convened a panel of
world-renowned experts to discuss the treat-ment options and
management strategies of DR and DME in their respective countries.
Here is what they had to say.
−Rishi P. Singh, MD
Source: International Diabetes Federation. Reprinted with
permission.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 5
patients. Additionally, we have started a pilot project to
screen for DR with the aim of increasing awareness of this
condition among diabetic patients and decreasing the rate of severe
cases.
Dr. Singh: It sounds as though a subset of patients are aware of
their diabetes diagnosis and what is needed to manage it. But how
much awareness is there of their diabetic eye disease in these
patient populations?
Prof. Soubrane: In France, there are patient associations for a
number of diseases, which educate them on diabetes or diabetic
complications, including diabetic eye dis-ease. But a more
challenging issue is that not all the diabetic patients belong to
these associations. Some of the younger patients with type 1
diabetes and some newly diagnosed adult patients are not as aware,
depending on the information provided by their general practitioner
or diabetologist.
Prof. Loewenstein: In Israel, most patients are very much aware
of their diabetic eye disease. The physicians make it their
business to know that patients need to get their systemic disease
and their diabetic eye disease under control. Physicians are
incentivized to refer diabetic patients to an ophthalmologist,
because it is a parameter considered in the quality-of-care
evaluation. So, patients are very aware they need to have their
eyes examined regularly.
Prof. Midena: The amount of awareness depends on the patient,
and I think this will change over time. Right now, health care
professionals in a diabetic clinic are fol-lowing about 50% of the
diabetic population, so they are being educated about eye disease.
But in our healthcare system, the general practitioner will have a
major role in the future diagnosis and treatment of diabetes. I
expect the number of patients who are aware of diabetic eye disease
will be reduced in the upcoming years if general practitioners are
not aware of the importance of patient education.
Prof. Lanzetta: In my region, the majority of the diabetic
population is unaware of very specific details of ocular
complications like DR. However, they are well aware that if they
can better manage their diabetes over-all, they may reduce their
complications in general.
Dr. Singh: We have a lot of diagnostic tools in our
armamentarium. Do you routinely run angiography
on your patients? Do you perform optical coherence tomography
(OCT) on all your patients when they present for diabetic eye
evaluations? What other diag-nostic tests and tools do you
typically use during the initial evaluation?
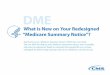
Prof. Loewenstein: We know that DME occurs very rarely, unless
the patient has at least moderate non-proliferative diabetic
retinopathy (NPDR). If I do not see signs of DR when I see a
patient, or if it is really very mild retinopathy (less than 5
microaneurysms), I would not do an OCT if I do not see a thickened
retina on clini-cal exam (Figure 1). But if I see any signs, even
if I am not convinced there is retinal thickening, I would do an
OCT because it is more sensitive than my eye. So, if the patient
presents with more than mild NPDR, I do an OCT. I do not use
fluorescein angiography (FA) unless I think that the patient needs
treatment.
Prof. Soubrane: In adult patients, we typically perform FA and
get an OCT initially in order to have a baseline document. After 5
to 10 years of active systemic disease, or if abnormalities are
observed on a biomicroscopy exam in young and adult patients, we
will always take another OCT. If we are considering treatment, we
take another FA then as well.
Dr. Singh: So, duration of diabetes is more important than
classification of the patient’s DR state.
Prof. Soubrane: I think that it is a good cut-off. Not in every
case, but as a general rule of thumb.
Prof. Loewenstein: Do you do an OCT even if the patient has
nothing?
Figure 1. Example of very mild edema for laser or for
observation.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
6 SUPPLEMENT TO RETINA TODAY MAY/JUNE 2015
Prof. Soubrane: If nothing shows up on biomicros-copy, I do not
do an OCT. There has to be some progres-sion of disease first.
Prof. Midena: Most of our patients are referred to us after
already being diagnosed with retinopathy, so we check everyone with
OCT. FA is limited to patients with DME; we perform FA at baseline
to determine treatment plans for those with DME and to see what—if
any—involvement there is in the periphery. But if there is no sign
of DR, we will not use FA.
Prof. Lanzetta: FA is not part of our routine diagnos-tic
workup, unless the patient has proliferative disease or we need it
to confirm DME progression. For us, our standard evaluation and
monitoring regimen includes a visual acuity exam and an OCT (even
if the patient does not have major signs of DR). I believe OCT
should be part of our standard work-up screening program.
Dr. Singh: What about ultra-widefield FA? Where do you see its
role in your patients right now?
Prof. Midena: The use of widefield FA is an advantage because it
is easier for a clinician to perform. Even in the past, we were
checking the periphery of the retina. We never limited FA to the
posterior pole, even as far back as 20 years ago. But the advantage
of widefield FA is that just one shot will encompass the entire
retina, including the periphery.
Prof. Soubrane: Examining the periphery with ultra-widefield
imaging is an interesting concept—it is easy, and it provides us
with more documentation. But if ultra widefield imaging is not
available, at the mini-mum, clinicians should be performing
biomicroscopy. More and more patients are being followed for their
macular edema on OCT, but only taking into account the posterior
pole and neglecting the periphery until there are symptoms. It is
more and more of a trend that we presently do not pay enough
attention to the peripheral ischemia.
Prof. Loewenstein: Because I examine the patients carefully, and
I always look at the periphery, I know wide-field photography gives
beautiful images. But remember that also, even in the EDTRS, we
just did the panretinal photocoagulation (PRP) up to the equator,
so we did not reach the far periphery, and it still worked. I think
as of right now, we do not have enough evidence-based data to
determine if widefield imaging is really crucial in the treatment
of the patients. It is nice to have the addi-
tional information, but I do not know if it would influ-ence me
in my treatment decisions.
Prof. Lanzetta: The idea of checking the far periphery in DR in
search of retinal ischemia or new vessels has been widely accepted
in Europe for years now, even in times when widefield angiography
was not available. This has been taught for years by well-known
experts such as Prof. Brancato and Prof. Coscas. We have been
carefully checking the periphery for years. As a consequence, I do
not think of widefield angiography as a “must-have” instrument, but
I do like the idea that with one image you can see the whole
retina, including the periphery.
Prof. Soubrane: To recognize retinal ischemia clini-cally, you
need proper training, but not all ophthalmolo-gists are so
specialized.
Dr. Singh: Generally speaking, what are your treat-ment
algorithms for a patient with DME?
Prof. Midena: That is a very complicated story. There are
probably too many algorithms for the treatment of DME. I have a
personal view, but this is very personal and limited: I think about
DME as a retinal disorder with different retinal (local)
phenotypes. And fundus biomi-croscopy is not the right way to
differentiate them. So we need at least spectral domain OCT,
analyzed in detail, not limited to central retinal thickness. There
are differ-ent growing hypotheses now: VEGF is prevalent, but it is
not the only driver of DME. The studies are showing a higher rate
of nonresponders compared with patients who have age-related
macular degeneration. We are now checking patients to differentiate
if there is more inflam-mation or more VEGF.
Dr. Singh: Everyone here agrees that VEGF is not the only
mediator of this disease state. So, how do you approach the
patient?
Prof. Midena: I use the OCT to determine if there is more
inflammation, and if so, I do not treat with an anti-VEGF.
Dr. Singh: What are the situations where you do not treat with
an anti-VEGF?
Prof. Midena: We do not think VEGF is the most prevalent
mechanism of DME in an individual patient. If we believe patients
have more retinal inflammation, our first line of therapy is
corticosteroid or a combined treat-ment, mainly if the patient is
pseudophakic.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 7
Prof. Loewenstein: I usually start with an anti-VEGF and, unless
a specific patient cannot come for frequent, monthly dosing for
those first few months. If I do not see any improvement, I usually
do not wait the 6 months suggested in the DRCR.net Protocol I.4 If
I see that there is no response after 3 months, I may switch to
another anti-VEGF, but I would tend to immediately prescribe a
steroid. And we get very good results using this strategy.
Prof. Soubrane: If we find a serous retinal detachment on OCT,
it would be a good sign to prescribe a steroid.
Dr. Singh: Serous retinal detachment on the OCT is an indicator
that VEGFs are present. There is much more inflammatory stimulus
than you would see with use of a corticosteroid.
Prof. Soubrane: A retinal serous detachment is a sign of rupture
of the outer retinal barrier. This breakdown is not VEGF-dependent
and suggests inflammatory players. Improved glycemic and systemic
hypertension control is, therefore, a part of our treatment.
Prof. Lanzetta: This year at the Macula Society meet-
ing,5 an interesting presentation showed that the addition of
personalized education and risk assessment during retinal
ophthalmology visits do not result in improved diabetes control.
However, during my first visit with dia-betic patients, I still
extensively discuss the role of optimal disease control with the
aim to limit DR progression. In selected patients with DME with
very good visual acuity and minor thickening at OCT, I may consider
observation at first, trying to improve metabolic control.
Dr. Singh: Would you summarize that presentation?
Prof. Loewenstein: Basically, Protocol M from the DRCR.net
looked at the influence of the ophthalmolo-gists to educate the
patient on the control of the disease. And unfortunately, the
ophthalmologist’s education was not very helpful. And it did not
cause any difference in patients’ blood control or their glucose
control.
Prof. Lanzetta: There were a number of questions from that
presentation that need to be answered. One must ask why
ophthalmologists are less efficacious in guiding the patient toward
a better management of diabetes compared with diabetologists. In
other words, which instruments should we use to “convince” our
patients on the importance of improving their A1c levels?
Dr. Singh: My presentation at the Macula Society meeting was a
post hoc analysis of the RISE and RIDE studies with regard to the
treatment response of patients with anti-VEGF therapy in light of
their base-line factors.6 The study demonstrated that there was no
difference in patients within the trial, with no change noted in
hemoglobin A1c from the time they entered the trial until the end.
So, 2 years later, after all the intervention, they did not realize
any difference in their A1c values.
Prof. Lanzetta: We are also learning that A1c, renal function,
or blood pressure do not influence visual improvement after
anti-VEGF treatment. This is different from the common observation
that patients with most difficult to control disease have worse
outcomes after laser treatment.
Prof. Midena: At a certain point in DME, more advanced
retinopathy appears in the patient, which this is not really
related to the patient’s general situation. There are a lot of hard
exudates all around the posterior pole, or perhaps numerous
cotton-wool spots. At this point, none of our treatments is
effective.
Prof. Soubrane: Ophthalmologists need to intervene much, much
earlier. By the time the patient presents with DME or proliferative
DR, it is already too late. In our department, the waiting room
chatter among patients with various levels of DR is what clicks for
those with milder disease. They hear how much worse their vision
can become and start to realize that systemic control of their
disease is necessary.
Dr. Singh: Your first-line treatment for patients is anti-VEGF
therapy, and you would consider anti-VEGF in patients with serous
retinal detachment and pseudo-phakia. Are there any situations in
which anti-VEGFs are not your first-line therapy? For example, how
would you treat a patient with clinically significant DME but did
not involve the fovea?
Prof. Lanzetta: I am not fully convinced that anti-VEGF is the
first-line therapy in patients with diabetes now that we have
dexamethasone implant 0.7 mg (Ozurdex, Allergan) approval.
Prof. Midena: I agree—it depends on the population.
Prof. Lanzetta: To be honest, I do not know what is first-line
therapy. I use both approaches. There are advantages and
disadvantages to both treatments.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
8 SUPPLEMENT TO RETINA TODAY MAY/JUNE 2015
Dr. Singh: Do you have the fluocinolone implant (Iluvien,
Alimera) approved in your countries? In the US, it is approved for
treatment of DME in patients who have been previously treated with
a course of corticoste-roids and did not have a clinically
significant rise in intra-ocular pressure (IOP).7
Prof. Midena: I do not think that Iluvein is a good option for
patients because it is coming from purely pre-specified analysis.8
The 3-year cut-off is theoretical. I have asked different
clinicians presenting these data how one can be sure about the
duration of DME. In the UK, where there is a 1- or 2-year screening
process in all diabetic patients, they know the duration of
disease. But in most of the other countries, we do not. We do not
know the duration before presentation.
Prof. Soubrane: In France, there is strict record-keep-ing about
the exams, so physicians will know within a certain time frame when
the DME began.
Prof. Lanzetta: The problem is what we see in clinical trials
does not really correspond to what we obtain in real-life
scenarios. If you look at the RISE and RIDE trials,9 36 months of
continuous monthly anti-VEGF injections result in the best outcomes
in terms of 3-line or more improvement in visual acuity. Although
this is remarkable, few clinics may have the capacity to inject on
a monthly basis for 3 years. Real-life management is a different
story, with fewer injections and visits. Therefore, outcomes are
usually less favorable. The possibility to use a long-lasting drug
such as the dexamethasone implant 0.7 mg may allow fewer injections
still with reasonable outcomes.
Dr. Singh: Are you finding your therapy outcomes haven’t matched
what they’ve found in the studies or that you need to inject more
frequently to continue the outcomes? In other words, how are your
real-life expecta-tions/experiences differing from the clinical
study results?
Prof. Loewenstein: We know that we have to inject more
frequently than was done in all the Ozurdex clinical trials.
Ozurdex does not hold for 6 months. The COMO study is the first
head-to-head comparison of ranibizumab (Lucentis, Novartis and
Roche/Genentech) to Ozurdex, but that was in patients with retinal
vein occlusion.10 There is also a study comparing the two drugs in
DME, but these results are not yet available.
Dr. Singh: It sounds as though some of us here are evaluating
combining an anti-VEGF with a steroid. How do you manage that?
Prof. Loewenstein: We are not using both simultane-ously right
now. I do know some groups in Germany are investigating
simultaneous dosing, but we are not. We will use one, and if there
is no response after a month or so, we will consider the other, but
that is not quite the same as simultaneously dosing.
Dr. Singh: If we term it “multimodality,” then, how are you
incorporating that into your treatments?
Prof. Lanzetta: I think in Europe many people still use
intravitreal therapy plus laser, even though we are lack-ing
evidence that using a laser adds anything beneficial to a drug
regimen. Obviously, today, we are using the laser very differently
than how we have used it in the past. We are treating less
invasively and less destructively by applying less energy or by
using subthreshold modalities.
Prof. Soubrane: I use photocoagulation laser for lesions not
involving the center of the macula.
Prof. Midena: I began using subthreshold micropulse (diode, and
then yellow) laser in the past 8 years to avoid the possibility of
damaging the retina.
Dr. Singh: What are some of its benefits of using a micropulse
laser, aside from not being photodestructive?
Prof. Midena: From a dosing frequency, it is the same as with
standard laser (every 3 months), even though the likely
pathophysiology of the micropulse laser is likely dif-ferent. We
have worked on this topic for years, and now, we are trying to show
this clinically.
Prof. Loewenstein: I have used the Lumenis Novus Spectra
(Sigmacon) micropulse laser, but I have a pro-totype. So there is a
relatively large spot size of 200 microns, which means I will limit
the use to extrafoveal lesions. In the few dozen or so patients in
whom we have used it, however, we have had excellent
responses..
Prof. Midena: Even today, when there are poor or limited
results, we deem it the ceiling effect. Even in the RESTORE study,
there did not seem to be much benefit to adding laser.11
Prof. Soubrane: I used micropulse lasers a long time ago (and
with the caveat that it is not the same technol-ogy as we have
today), but I was not really overwhelmed by their efficacy.
Prof. Lanzetta: I have been using subthreshold irradia-
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 9
tion since the early 2000s with various modalities, such as
micropulse, or continuous wave and low energy. I am fully convinced
that this is the way we should use lasers today. Up to now, only a
single study has shown that micropulse subthreshold high-density
laser irradiation may provide outcomes similar or superior to
anti-VEGF therapy.12
What should be known is that a subset of patients with DME may
benefit from laser, that it takes time for the beneficial effect to
manifest, and that multiple treat-ment sessions may be
necessary.
FOLLOW-UPDr. Singh: How are you managing your follow-up? Let
us presume the patient has center-involving DME with elevated
retinal thickness, and you have initiated anti-VEGF therapy, with
the multimodal therapy with combi-nation Ozurdex.
Prof. Soubrane: It is pre-planned every month, with Ozurdex
every 4 to 6 weeks and every month for anti-VEGFs.
Prof. Midena: We do not see the patient even after the loading
phase. I see the patient at baseline, they have three injections
promptly, and then I see them at 4 months.
Dr. Singh: Is someone else doing the injections for you?
Prof. Midena: Yes, and I see the patient in 6 months because I
perform the loading phase and then I see the patient. I never see
the patient monthly.
Dr. Singh: Another ophthalmologist is doing the injections?
Prof. Midena: Yes, absolutely an ophthalmologist. In my case, if
I prescribe a steroid, and someone else is check-ing the pressure,
then I am completely comfortable for 2, even 3 months—unless I did
not see any response from previous injections. With anti-VEGF, I do
give monthly injections for 3 months, and then I see the patient
the month after the third injection. However, the person who is
providing the injections has make sure there is no
endo-phthalmitis, detachment, or other complications.
Prof. Soubrane: While I may not personally see my patients every
month, I want them to be seen just to ensure that the treatment is
working.. Just to be sure the treatment the working.
Prof. Midena: Theoretically speaking, I would like to see the
patients receiving anti-VEGF therapy on a
monthly basis, after the loading phase and even with
cor-ticosteroid implant. I typically like to see these patients
within 1 month to check for IOP changes. After the first month, I
might check these patients between 2 to 3 months.
Dr. Singh: If you are bringing the patient back to check the
IOP, what is your ideal time frame?
Prof. Loewenstein: Ozurdex peaks in 6 weeks. But I also think
that the patients need to have the pressure checked after 2 weeks
to determine if there is an increase in IOP.
Prof. Lanzetta: I do not think IOP increases are a dra-matic
problem for most patients treated with dexameth-asone implant 0.7
mg but can be for some, probably the younger individuals. I do not
want to miss those patients, so I usually ask them to come back and
have their IOP checked after 2 weeks.
Dr. Singh: How do you treat/manage the patient with an IOP
spike?
Prof. Loewenstein: I consult with my glaucoma special-ist if the
patient does not improve on topical medications. I prescribe
beta-blockers, or perhaps a prostaglandin.
Prof. Soubrane: If there is a huge rise—up to 50 mm Hg, despite
three IOP-lowering drops—I will try to push for a vitrectomy to
remove the implant rather than having a trabeculectomy
performed.
Dr. Singh: Would anyone else remove the Ozurdex implant rather
than perform incisional glaucoma surgery?
Prof. Loewenstein: I would not. I have one such patient who had
a trabeculectomy and then needed Ozurdex, and I was completely
comfortable prescribing Ozurdex.
Prof. Lanzetta: I had a female patient who spiked up to 50 mm
Hg. She did very well immediately after dorzol-amide and timolol
and prostaglandin analog drops.
Prof. Soubrane: I had one patient who did not improve with
medical treatment and went onto under-going a trabeculectomy. This
patient now has a severe hypotensive globe.
Prof. Midena: If you have a patient whose IOP spikes and still
has recurrent edema after 5 or 6 months, are
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
10 SUPPLEMENT TO RETINA TODAY MAY/JUNE 2015
you comfortable injecting again with Ozurdex, or do you change
your treatment?
Prof. Lanzetta: I probably would consider switching.
Prof. Loewenstein: So would I.
Dr. Singh: What about the patient with an IOP rise but
improvement in the edema, who then has a recurrence?
Prof. Loewenstein: If his or her IOP is really easy to con-trol,
and for some reason the patient is more comfortable with receiving
Ozurdex, it would not be a big, big problem.
Dr. Singh: By “easy to control,” we mean one or two topical
drops?
Prof. Loewenstein: Yes.
OTHER TREATMENTSDr. Singh: What are your thoughts on some of
the
newer agents we have been hearing about? Should we be
considering these as another potential therapy? Are there other DME
therapies you are looking forward to hearing about in the
future?
Prof. Loewenstein: I am not convinced any other treatment will
replace what we have now. There is very little data on the
angioinhibitors, for example, even though they are higher up on the
VEGF pathway.
Dr. Singh: I agree—very little data. How about phar-macological
vitreolysis? One of the theories is that vit-reolysis in those
patients (without traction) can actually prevent DR/DME from
progressing.
Prof. Midena: It is a very nice idea. Physiologically, it is a
very consistent concept. Vitreolysis is not useful when thickening
of internal retinal membrane or epireti-nal membranes are present
in patients with diabetes, because the membranes are not purely
collagenous material, but neurites or glial cells are present in
the epiretinal/retinal thickened area.
Prof. Loewenstein: I think the most important thing recently has
been the Protocol T trial13 results that have just been
published.
TAKE-AWAY POINTS FROM PROTOCOL TDr. Singh: What was your
take-away point from the
Protocol T study?
Prof. Loewenstein: The most important take-away point was that
the three treatments worked very well. We now have data on as
needed p.r.n. regimens that we did not have before. Finally, we now
know when afliber-cept 2.0 mg will work better than ranibizumab 0.3
mg.
Dr. Singh: Did that surprise you?
Prof. Loewenstein: Yes—all the other trials had shown no
differences between the two compounds. However, Protocol T used 0.3
mg.13 It is unclear what the results would have been if they had
studied 0.5 mg. In RIDE and RISE,7 there was a small difference in
effi-cacy between those two concentrations. But again, in Protocol
T it was a p.r.n. regimen, even if it was a very strict p.r.n.
regimen. So, for me, in lower visual acuities if the cost is the
same between the two compounds, I have to lean toward the more
efficacious one.
Prof. Soubrane: I am also frustrated we do not have results with
the 0.5-mg concentration. However, it is obvious that our patients
do not lose their chance for improvement if we inject aflibercept.
To me, that is a major point.
Prof. Lanzetta: I fully agree. One other observation is from a
practicality perspective—we do not really have to give five initial
monthly injections before moving to a dif-ferent regimen. We can
probably start p.r.n. much sooner.
Prof. Midena: There are three main points from Protocol T.13 The
number of injections of aflibercept in the p.r.n. regimen was the
same as in VISTA.14 So we do not need a p.r.n.; a fixed regimen is
much simpler for my patients. The working population does not like
to be checked every month; it is a lot of time away from work.
Second, we need to stop considering aflibercept as a pure
anti-VEGF. It is a completely different molecule. If
pharmacologists consider it a different drug, we should, too. And I
think that is the story behind why the results are much
better—aflibercept also has another property. Third, there was an
astonishing number of laser treat-ments. More than 30% of patients
underwent some type of laser therapy in each eye? Laser is not
dead!
Dr. Singh: What does everyone else think? After read-ing
Protocol T, is laser dead?
Prof. Soubrane: I think laser may still have a role in treatment
of DME, but not everywhere. In France, afliber-cept is presently an
acceptable treatment for DME and will be reimbursed soon, but not
yet.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 11
Prof. Midena: In Italy, it is registered, but we just received
reimbursement.
NONRESPONDERS OR LIMITED RESPONDERSDr. Singh: Now that we have
discussed several thera-
py options, how do you define treatment failure? What are your
criteria?
Prof. Loewenstein: I consider a treatment failure as a patient
whose visual acuity does not improve or if his or her retinal
thickness does not improve. There may be several reasons for
limited visual acuity improvement, but if there is no response on
OCT at all, especially if there is also no visual acuity
improvement, that is a treatment failure. For me, the OCT is the
most impor-tant parameter.
Prof. Soubrane: Do you treat OCTs or do you treat patients? Just
OCT is not enough. I want an FA to try to identify the reason of
lack of response.
Prof. Loewenstein: For me, OCT is the most impor-tant
parameter.
Prof. Soubrane: If the patient’s vision improved, and he or she
is more comfortable, that is equally important.
Dr. Singh: Is vision as important as the OCT?
Prof. Soubrane: Both are important. I take into con-sideration
OCT and vision when I am considering treat-ment. The problem arises
when there is a discrepancy.
Prof. Loewenstein: I think you have to treat the retina—if it
remains thick for a long time, vision decreases.
Prof. Lanzetta: Defining the so-called low responders is really
the most difficult part of our job. I agree that OCT is the major
guidance to determine if we should keep injecting. But you also
have to combine the mor-phology with visual acuity. If you cannot
decrease the retinal thickness, you need to keep injecting for a
reason-able time.
Prof. Soubrane: What is a reasonable amount of time?
Prof. Lanzetta: At least 4 to 6 months. On the other hand, there
are some other patients who are responders, but do not have visual
acuity improvement. A very thin retina and no visual acuity change
may suggest macular atrophy. In this case, I would stop
injecting.
Prof. Midena: I think the two parameters are equal. We can have
visual acuity improvement if the retina is not atrophic, but this
is not as common in patients with diabetes as it is in those with
wet AMD. If one of the two parameters is not improving after four
injections, we will switch treatments. We cannot show which
patients will continue to progress over the long term. We need to
be on the patient’s side, but in Italy, we cannot spend so much
money at the end of 1 year, after nine or 10 injec-tions, unless
there is a clear improvement.
Dr. Singh: Let us talk about the financial impact—how are these
drugs reimbursed in your countries?
Prof. Lanzetta: Laser would be a much better option, of course.
In Italy, intravitreal therapy will be an issue, but not yet,
because we just started treating DME with reim-bursed drugs. We
have many more patients with bilater-al disease as compared to
those with wet AMD, however, which means a relatively large number
of injections per year, so it is going to be an issue. And the
solution is to allocate more resources to ophthalmology given the
fact that the newer therapies can significantly decrease the
incidence of legal blindness due to macular diseases.
Prof. Midena: Since just last year, we have been forced by law
to move from Lucentis and Eylea to Avastin. That is not for
patients with diabetes, but we did not have Protocol T results,
either. That will be against us—we may be told that for people with
relatively good visual acuity, we have to use Avastin. Protocol T
did not show enough of a difference between the drugs.
Dr. Singh: So Protocol T will be used to create a step
therapy?
Prof. Midena: It may be. One of the consequences may be that
more patients will be treated later, even with the right drug.
Prof. Soubrane: In France, there is no obligation to use
Lucentis or Avastin. Eylea is approved but not yet reimbursed for
DME. The choice would have been dif-ficult without Protocol T.
Dr. Singh: How about Ozurdex for your cases?
Prof. Soubrane: Ozurdex is reimbursed in France.
Prof. Midena: In Italy, Ozurdex is approved but not officially
reimbursed. It is reimbursed through a different bureaucratic
system.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
12 SUPPLEMENT TO RETINA TODAY MAY/JUNE 2015
Prof. Lanzetta: Limitations with the dexamethasone implant 0.7
mg in Italy are very similar to the original US limits. Only
patients who are pseudophakic or non-responders to anti-VEGF
treatment will be reimbursed.
Prof. Loewenstein: In Israel, regardless of the disease, we have
to start with Avastin for at least three injec-tions. And we have
to prove Avastin does not work by showing the exact OCT
measurements and visual acuity before and after treatment. Only
then can we switch.
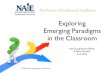
CASE STUDYDr. Singh: Let us discuss this one case (full
disclosure:
he was my patient). This is a 53-year-old male with a 10-year
history of systemic diabetes. He has 20/50 visual acuity in the
right eye, 20/40 in the left eye. He has bilateral, moderate,
nonproliferative disease. See Figure 2 for the OCT images. How
would you treat this patient?
Prof. Lanzetta: This is a relatively young patient with what I
consider to be significantly decreased visual acu-ity. Because of
the lens status and patient’s age, I would not consider using a
dexamethasone implant because of the potential for cataract and
elevated IOP. I would consider the anti-VEGFs first, and based on
the Protocol T results, I would prefer aflibercept.
Prof. Lanzetta: I would either use the DRCR.net treat-ment
scheme, or I would be tempted to give the first injection and then
to switch to an individualized regimen.
Prof. Loewenstein: I would initially start with an FA, just to
have a baseline to figure out if there is nonperfu-sion in the
macula. (Based on the images here, I do not believe he does, but I
would like to ensure that.) Then I would start with an anti-VEGF.
As I mentioned, in Israel, I
have to start with Avastin, although now Protocol T has provided
us with the weapons we need to get the gov-ernment to approve
aflibercept and ranibizumab. If I had the choice, then I would
start with aflibercept if a patient has a relatively low visual
acuity.
Prof. Soubrane: In the right eye, the vision is not that great,
and it seems as though there is a little serous detachment. Because
of that, my first treatment strategy would be to use the Ozurdex
implant in his right eye. But in his left eye, I would use Eylea. I
would not treat the two eyes simultaneously, either.
Prof. Midena: My preference is a drug with some
anti-inflammatory properties.
Prof. Soubrane: I would use both. But as an important caveat, I
tend not to treat both eyes on the same day unless out of necessity
for the patient.
Dr. Singh: In your own practices, are you doing bilat-eral
injections?
Prof. Midena: Never.
Dr. Singh: Never.
Prof. Soubrane: Sometimes.
Prof. Loewenstein: I did always bilateral the same day. Last
month, I had my first case of endophthal-mitis in a patient
bilaterally injected with afliber-cept. Luckily, it only happened
in one eye, but it was extreme enough that the patient lost visual
acuity. I am trembling from the thought the patient could have lost
vision in both eyes. So, now I have stopped per-forming bilateral
injections.
Prof. Lanzetta: I usually do not inject bilaterally unless the
patient is elderly and cannot travel back and forth to the office
in a timely manner.
Dr. Singh: One last point—Lucentis and Eylea were recently
approved in the US for DR. Protocol S will look at both panretinal
photocoagulation (PRP) and anti-VEGFs in the DR population. How
would you use either of the anti-VEGFs if they were approved for DR
in your countries?
Prof. Midena: I have been involved in the protocol in Europe for
both PRP eyes and anti-VEGF: one arm is PRP and the other is
combined PRP and anti-VEGF. It is
Figure 2. Long-standing systemic diabetes in a patient with
moderate nonproliferative diabetic retinopathy.
-
NEW PARADIGMS IN DME DIAGNOSIS AND MANAGEMENT
MAY/JUNE 2015 SUPPLEMENT TO RETINA TODAY 13
similar to the DRCR’s Protocol S, but this is the European group
(http://evicr.net/). We do not have a standard treatment for
anti-VEGF in proliferative DR yet.
Dr. Singh: Prof. Soubrane, what would you do if you had that
approval? Would that change anything for you? Or do you still
maintain that PRP is the preferred meth-od to treat patients with
DR?
Prof. Soubrane: I do not have a crystal ball, but it will really
depend on the result of the study.
Prof. Midena: I am not fully convinced we have the best
treatment yet. It is a long, long treatment. In DME, we have seen a
high number of first-year injections. The idea of treating
proliferative DR that is unresponsive to PRP… well, PRP is an
inexpensive treatment. I have patients who have had type I diabetes
for more than 20 years, with more than 20 years of follow-up. And
they have 20/20 visual acuity with PRP.
Prof. Loewenstein: We do know that the standard of care
treatment for neovascular disease is PRP. However, nowadays, if I
see a patient who has even a mild form of the disease, I am
comfortable injecting him or her and then following. I am not
necessarily running to PRP immediately, even though there is no
proof yet that the anti-VEGFs are better. For now, I am comfortable
doing an injection and seeing the patient again in 2 or 3 weeks. If
the patient has some regression, I am comfort-able not doing
PRP.
Prof. Lanzetta: I am relatively concerned by the approval of
anti-VEGFs to treat DR. Even though it has been proven that
anti-VEGF therapy may be beneficial on the DR severity scale, there
is an efficacious therapy for the proliferative form of DR, and
that is PRP—which is definitely much less expensive than
anti-VEGFs.
Prof. Midena: What about the US? Can you treat patients with
NPDR?
Dr. Singh: In the US, the stage of retinopathy does not matter.
We can treat at every level. Patients have to have DME, but how
they define DME in this setting is unknown. Can the patient have a
cyst on hir or her retina? Can they have an increase in retinal
thickness? No one defines what DME means.
Prof. Lanzetta: Before using anti-VEGF for delaying the
progression or for regressing DR, I would really like to see more
data on the visual acuity outcomes.
Prof. Soubrane: One of the remaining problems is a
classification of DME, because we lump them all togeth-er. One cyst
or multiple cysts or serous detachment … we treat them the
same.
FINAL THOUGHTS ON TREATING DMEProf. Midena: Intravitreal drugs
have significantly
modified our approach. Visual acuity recovery is now better than
it was with laser treatment. Laser could only stabilize, but now we
can actually improve the visual acuity; that is our core
message.
Prof. Soubrane: That has been the revolutionary treatment—I do
not think anyone ever expected to be able to improve vision. But we
need to remember we still do not have long-term data.
Prof. Loewenstein: We can now tell our patients that they
definitely have more than a 95% chance of avoiding severe vision
loss through their lifetime with treatment.
Prof. Lanzetta: There are two major messages. First, we are
using less laser and more intravitreal drugs. We perform less FA.
We regularly do OCTs on our patients. We have a very complete
diagnostic workup so we can better characterize every type of DME
patient. By doing that, we might better recognize the best
treatment for each patient. Second, we should improve our promotion
of screening programs. Effective screening programs will hopefully
lead to fewer patients who need treatment because they are being
diagnosed earlier. n
1. International Diabetes Federation. IDF Diabetes Atlas, 6th
ed. Brussels, Belgium: International Diabetes Federation, 2014.2.
World Health Organization. The top 10 causes of death: Fact Sheet
No 310. Geneva, Switzerland, 2014.3. Yau JW, Rogers SL, Kawasaki R,
et al. Global prevalence and major risk factors of diabetic
retinopathy. Diabetes Care. 2012;35(3):556-564.4. Diabetic
Retinopathy Clinical Research Network, Elman MJ, Qin H, et al.
Intravitreal ranibizumab for diabetic macular edema with prompt
versus deferred laser treatment: three-year randomized trial
results. Ophthalmology. 2012;119(11):2312-2318.5. Aiello LP.
Randomized Trial Assessing Personalized Point-of-Care Diabetes
Complication Risk Assessment during Ophthalmology Visits on
Diabetes Control. Presented at: 38th Annual Macula Society Meeting;
Feb. 25-28, 2015; Scottsdale, Arizona.6. Singh RS. The impact of
systemic factors on clinical response to ranibizumab for diabetic
macular edema. Presented at: 38th Annual Macula Society Meeting;
Feb. 25-28, 2015; Scottsdale, Arizona.7. Iluvien [package insert].
Atlanta, GA: Alimera Sciences Inc., 2014.8. Campochiaro PA, Brown
DM, Pearson A, et al. Sustained delivery fluocinolone acetonide
vitreous inserts provide benefit for at least 3 years in patients
with diabetic macular edema. Ophthalmology.
2012;119(10):2125-2132.9. Nguyen QD, Brown DM, Marcus DM, et al.
Ranibizumab for diabetic macular edema: results from 2 phase III
randomized trials: RISE and RIDE. Ophthalmology.
2012;119(4):789-801.10. Loewenstein A, Bandello F, Kampik A, et al.
Design and rationale of COMO, a 12-month study that compares the
safety and efficacy of dexamethasone intravitreal implant versus
ranibizumab in branch retinal vein occlusion. Acta Ophthalmologica.
2011;89(suppl s248); doi: 10.1111/j.1755-3768.2011.341.x.11.
Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE
study: ranibizumab monotherapy or combined with laser versus laser
monotherapy for diabetic macular edema. Ophthalmology.
2011;118(4):615-625.12 . Do DV, Nguyen QD, Khwaja AA, et al. READ-2
Study Group. Ranibizumab for edema of the macula in diabetes study:
3-year outcomes and the need for prolonged frequent treatment. JAMA
Ophthalmol. 2013;131(2):139-145.13. Diabetic Retinopathy Clinical
Research Network. Aflibercept, Bevacizumab, or Ranibizumab for
Diabetic Macular Edema. N Engl J Med. 2015; 372:1193-1203.14.
Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intravitreal
Aflibercept for Diabetic Macular Edema. Ophthalmology.
2014;21(11):2247-2254.
-
// CERTAINTY MADE BY ZEISS
The moment information becomes insight. The NEW Retina Workplace
from ZEISS.
The new Retina Workplace from ZEISS is redefining workflow
efficiency when reviewing patients with macular diseases.
• Efficiently evaluate and monitor macula disorders and effects
of anti-VEGF treatments
• Easily follow patients over their entire treatment history to
assess the progression of their disease
• Conveniently navigate up to three data sets simultaneously to
directly compare multiple points in time
Test drive
the future!
SOE, Hall F
,
Booth #15
Scan the QR code and
discover more today!
Test drive how the FORUM powered ZEISS Retina Workplace can
redefine your workflow efficiency. Visit us in hall F
booth #15 at SOE
or go online to www.zeiss.com/retina-workplace-ad.
-
// CERTAINTY MADE BY ZEISS
The moment information becomes insight. The NEW Retina Workplace
from ZEISS.
The new Retina Workplace from ZEISS is redefining workflow
efficiency when reviewing patients with macular diseases.
• Efficiently evaluate and monitor macula disorders and effects
of anti-VEGF treatments
• Easily follow patients over their entire treatment history to
assess the progression of their disease
• Conveniently navigate up to three data sets simultaneously to
directly compare multiple points in time
Test drive
the future!
SOE, Hall F
,
Booth #15
Scan the QR code and
discover more today!
Test drive how the FORUM powered ZEISS Retina Workplace can
redefine your workflow efficiency. Visit us in hall F
booth #15 at SOE
or go online to www.zeiss.com/retina-workplace-ad.
-
FOR RETINAOUR VISION
IS LONG TERM
©2015 Allergan, Inc., Irvine, CA 92612 Allergan.com
EAME/0202/2015 Date of prep June 2015
Developing treatments for retinal diseases
• Robust research and development program focused exclusively on
retinal therapeutics
• Investigational therapies that cover a range of retinal
diseases
• Active outreach for alliances to develop and commercialize new
agents
• Major Retina meetings, including: — Association for Research
in Vision and Ophthalmology (ARVO) — American Society of Retina
Specialists (ASRS) — Retina Society — American Academy of
Ophthalmology (AAO) — EURETINA — International Ocular Inflammation
Society — Macula Society
• Local and smaller Retina meetings
Advancing retinal medicine through ongoing support
151570 Supplement Journal ad_ST.indd 1 6/17/15 3:27 PM