Embed Size (px)
Citation preview

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
New Payment Models:How Prepared are You?
AAHAM
Doug Emery
May 5th, 2011

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
ACO Proposed Rule Released
An ACO is a program “that promotes accountability for a patient population and coordinates items and services under Parts A and B, and encourages investment in infrastructure and redesigned care processes for high quality and efficient delivery of services”
• Better care for individuals (STEEP)
• Better health for populations
• Lower growth in expenditures

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
ACO Proposed Rule
• Two-sided risk model
• Partial or virtual capitation
• Retrospective payment and attribution
• Open network FFS benefits
• Cannot restrict patient flow to non-ACO
• Cannot violate anti-trust rules

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
ACO Investment Requirements• Must use EBG
• Must describe and report patient engagement process
• Must ensure care coordination processes through entire episode of care and transitions of care
• Must use predictive modeling for each patient
• Must use case managers in primary care office
• Must provide remote monitoring
• Must implement telehealth
• Must install system-wide HIT, EMR and summary of care records
• Must have population health management systems
• Must have point-of-service reminder systems
• Must submit to CAHPS patient satisfaction survey
• Must create governance board with 75% physician mix
• Must appoint Medicare beneficiary in governance
Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
ACO Trade Off
• You are asked, for all this upfront investment, to give up trend in hopes of profitable margins
• You must give up 25% in withholds (third year?)
• You need at least 5,000 beneficiaries
• CMS expects 1.5 to 4 million to participate (of 35 million)

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Difficult ACO Break Even
Source: The ACO Model – A Three Year Financial Loss?, NEJM, Heywood and Kosel

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Difficult ACO Break Even – Cont.
“Absent changes to the design of the ACO model, (our) analysis suggests that before agreeing to become part of an ACO, physician group practices must conduct due diligence and explore participation such as other initiatives involving bundled payments for episodes of care”
Source: The ACO Model – A Three Year Financial Loss?, NEJM, Heywood and Kosel

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Patient-centered continuum of care
Source: Sustaining the Medical Home: How Prometheus Payment Can Revitalize Primary Care, RWJ publication

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Amplitude of cost along the continuum
Source: Sustaining the Medical Home: How Prometheus Payment Can Revitalize Primary Care, RWJ publication
Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
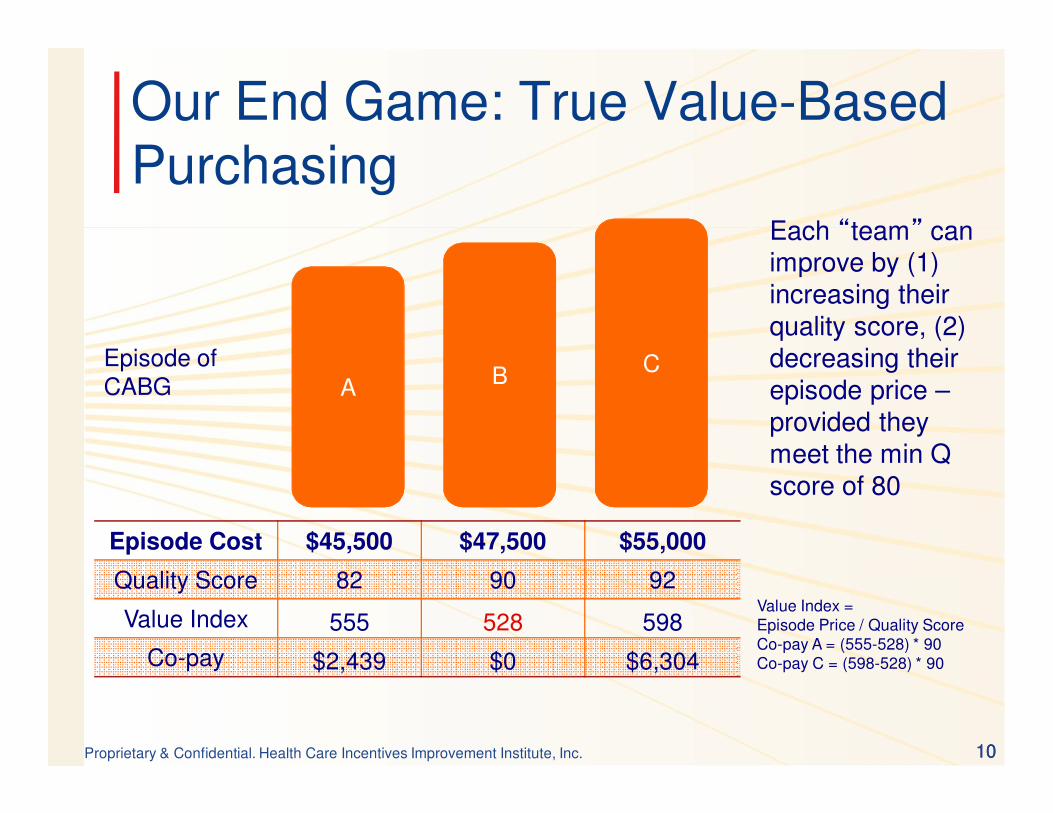
Our End Game: True Value-Based Purchasing
A BC
Each “team” can improve by (1) increasing their quality score, (2) decreasing their episode price –provided they meet the min Q score of 80
Episode of CABG
Episode Cost $45,500 $47,500 $55,000
Quality Score 82 90 92
Value Index 555 528 598
Co-pay $2,439 $0 $6,304
Value Index = Episode Price / Quality ScoreCo-pay A = (555-528) * 90Co-pay C = (598-528) * 90
1010

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Transparency only Programs
Fixed fee/bonus-based Programs
Shared savings-based Programs
Episode of Care payment
A glide path for provider management of financial risk
11
Provider Financial Risk
Sa
vin
gs
Global Capitation?
FFS
Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
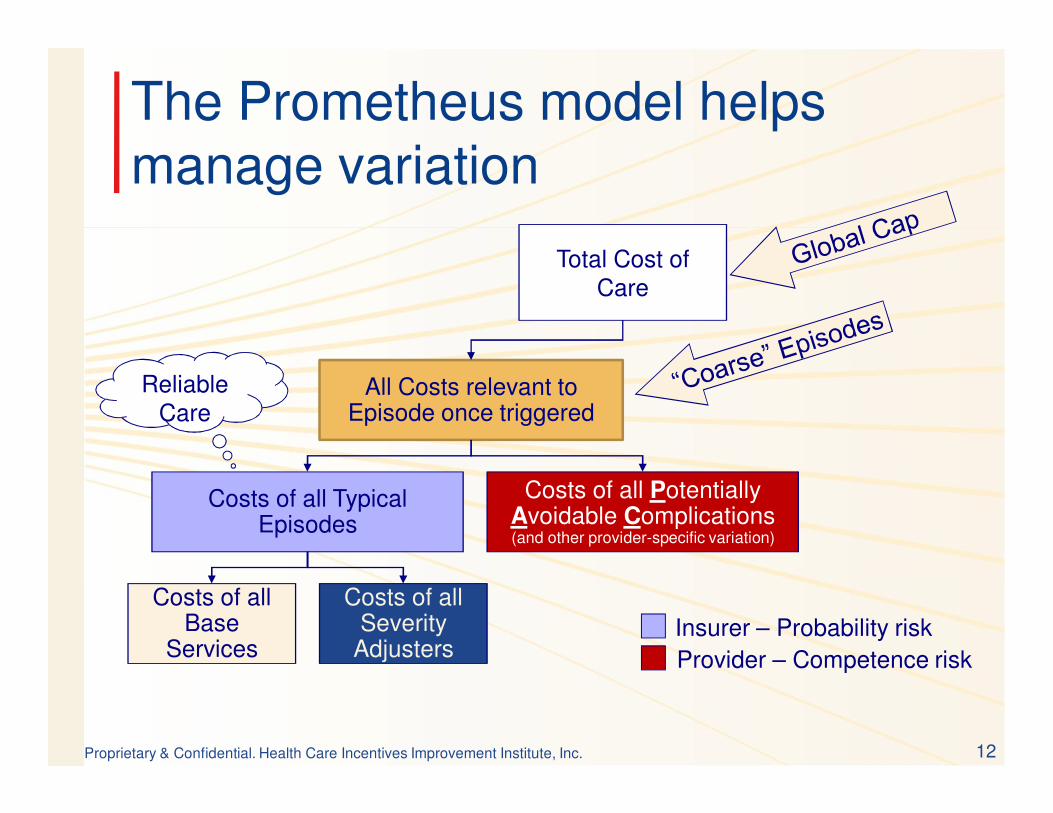
The Prometheus model helps manage variation
12
All Costs relevant to Episode once triggered
Total Cost of Care
Costs of all Typical Episodes
Costs of all Potentially Avoidable Complications(and other provider-specific variation)
Costs of all Base
Services
Costs of all Severity
AdjustersInsurer – Probability risk
Provider – Competence risk
Reliable Care

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
PAC Percents across ECRs
Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
How ECRs and Measures Fit Together

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Unique features of the PROMETHEUS model
• Margins improve as potentially avoidable complications are reduced – change the industry focus from chasing volume to chasing margin/value.
• Patient-level severity adjustment to minimize the potential for cherry-picking.
• Optimizes new and powerful feedback loops
15

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
PROMETHEUS Payment today
• Prospective budgets, FFS payments (with or without withholds), and retrospective reconciliations – mostly gain sharing formulas
• Use of BTE measures for scorecards (when implementations focus on chronic care episodes)
• Some emerging implementations use the prospective budgets as means to inform plan members of episode cost and move market share through co-pays/co-insurance
16

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
NQF Framework of episodes
17
ECRs look at all clinically related services for a discrete condition for the entire continuum of care: management, surgery, ancillary, lab, pharmacy services for a given time frame (one-year, start of symptoms to finish )

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
NQF Endorsement of PACs as Outcomes Measure
• We have submitted the definitions for Chronic care PACs and the three acute medical episodes – AMI, Stroke and Pneumonia – Passed through the Technical Advisory Panels– Voted in by the Steering Committee– Passed through the open public comment period – Passed through the Q&A session– Voted in through NQF member voting– Passed through CSAC Oct 14th discussion and
voted in by CSAC
• NQF releases endorsement in Feb 2011
18

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 191919
• PAC Type 1:– PACs related to the index condition (e.g. ER visit for diabetic
emergency such as hypo/hyper glycemia in a diabetic patient)– Best controlled by treating provider
• PAC Type 2:– PACs related to a co-morbid conditions (e.g. hospitalization for
pneumonia in a diabetic patient) – Best controlled by care-coordination
• PAC Type 3 –– PACs suggesting patient safety failure (e.g. adverse drug
events, such as drug interactions in a diabetic patient)– Includes CMS defined HACs (hospital acquired conditions) and
AHRQ defines PSIs (patient safety indicators)– Best controlled by process improvement
19
How do we define PACs?

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 20
PACs across Chronic Conditions
PAC Type ASTHMA CAD CHF COPD DM HTN All Chronics
Type 1 (Index Condition) 35.26% 0.00% 10.52% 34.09% 9.22% 21.30% 18.48%
Type 2 (Comorbidities) 44.71% 77.15% 62.19% 45.69% 67.06% 55.00% 58.76%
Type 3 (Patient Safety) 20.03% 22.85% 27.29% 20.22% 23.72% 23.70% 22.76%

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Top Drivers of PACs for Chronic Conditions (2)
TYPE OF PAC
PAC DESCRIPTION Diabetes CHF CAD HTN COPD Asthma
Emergency Room Visits 10.60% 22.20% 2.14% 23.23% 11.60% 31.40%
1 Acute Flare-up of Index Condition 8.37% 5.46% 16.81% 15.22%
2 Diabetic Emergency, Hypo- Hyper-Glycemia 3.37% 13.67% 1.52% 0.95%
2Subarachnoid And Intracerebral Hemorrhage
(Stroke, CVA)2.81% 3.36% 5.28% 0.07% 1.72% 0.76%
2 Cellulitis, Skin Infections 27.38% 13.56% 24.83% 23.28% 13.11% 10.02%
2 Gastritis, Ulcer, GI Hemorrhage 9.73% 6.21% 14.58% 13.31% 8.25% 6.24%
2 Syncope, Hypotension, Dizziness 7.42% 7.25% 12.09% 16.88% 1.84% 1.22%
2 Pneumonia, Lung Complications 14.31% 7.69% 4.95% 2.17% 6.89% 3.70%
2 Cardiac Dysrhythmias 7.95% 5.18%
3 Urinary Tract Infections 9.80% 5.06% 8.16% 11.43% 6.81% 5.95%
3 Phlebitis, DVT, Pulm Embolism 3.91% 7.02% 4.35% 2.57% 3.47% 1.85%
Total 94.34% 81.18% 90.04% 92.94% 79.98% 82.49%
21

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Setting up the Regression Model for Typical care
• Unit of analysis: ECR (“typical” claims in time window) • Dependent Variable: “Cost”
– We used “allowed amounts” as a surrogate for “cost”
• Independent Variables:– Baseline patient characteristics:
• Patient demographics: age, gender• Co-morbidities: asthma, thyroid disease
– Markers of disease progression, disease severity : • Diabetic retinopathy, nephropathy, neuropathy, peripheral vascular disease
– Procedures / services as markers of patient severity: • Durable medical equipment (DME) as a surrogate for how frail the patient is• Need for invasive diagnostic cardiovascular studies – disease severity
– Drugs:• Insulin – surrogate for severity, comorbidity
Note: Pharmacy variables are important determinants of variance in our models
22

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Prometheus Risk-Adjustment Methodology
23
• Risk adjustment only on typical claims:– PAC claims are removed before severity modeling
• Risk-Adjustment specific for user’s data:– The severity scores are built from the user’s own data based
on their own specific fee schedules and practice patterns either built from scratch or normalized to their own population
– Not based on reference population coefficients that are updated every 2 -3 years
• Risk adjustment on a continuum:– Severity scores are built on a patient-by-patient basis– Not stratified by arbitrary strata

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 24
Severity-adjusted Costs for Typical Care (CABG Stay model)
Adjusted R-Square = 0.19, N = 2,263 Low Med HighDescription Estimate Patient 1 Patient 2 Patient 3
INTERCEPT 9.55148 1 1 1
CRF0- OPEN CABG 0.8949 1 1 1
CRF14- CARDIAC ARRTHYTHMIAS AND CONDUCTION DISORDERS
0.27669 0 1 1
CRF16- AMI, SEQUELAE, RUPTURED CHORDA TENDINAE, PAPILLARY MUSCLES
0.19349 0 0 1
CRF4- HEART VALVE REPLACEMENT 1.1508 0 0 0
CRF5- OPEN HEART VALVULOPLASTY, REPAIR OUTFLOW TRACT
1.28781 0 0 0
CRF6- VENTRICLUAR, AORTIC ANEURYSM RESECTION, SURGICAL ABLATION, POST INFARCTION VSD
0.97005 0 0 0
M4- DIABETES MELLITUS WITHOUT COMPLICATION 0.09007 0 1 1
M5- FLUID AND ELECTROLYTE DISTURBANCES 0.10571 0 0 1
M8- ANEMIA, COAGULATION, HEMORRHAGIC DISORDERS 0.1289 0 0 1
Severity-adjusted Inpatient Stay Price of ECR $ 34,420 $ 49,669 $76,210
Severity-adjusted Professional Price of ECR (R-square =0.402) $ 6,210 $ 12,152 $32,131
Total ECR price for Typical portion of CABG care $ 40,629 $ 61,822 $108,341

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
Summary: Clinical logic for ECRs
– Starts with understanding what constitutes good care, consistent with available guidelines. Guidelines are used to determine the core set of services that will be needed to care for the patient
– Clinical logic tries to parse out causes of warranted and unwarranted variation. Unwarranted variation is variation caused by errors and bad care / potentially avoidable complications
– Statistical analyses determine the risk factors that signal a need for increased resources (ex ante patient factors such as age, gender, comorbid conditions)

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 2626
Chronic Care ECRs
• Risk Factors and PACs
• Cost and Occurrence of PACs by Type
• Top drivers and drill downs of PACs

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 27
Risk Factors and Total PAC Costs
27
It is difficult to predict when any one patient will have a PAC and what the total cost of that PAC might be.
R=.17R=.17 R=.19R=.19
R=.24R=.24

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 282828
Risk Factors and PACs: GERD
Here, patients are grouped in cohorts by count of risk factors. The percentage of patients with a PAC increases with count of risk factors.
On average, PAC costs increase with count of risk factors also.
It is still difficult to predict if any one patient will have a PAC, since between 30 and 40% of patients with <5 risk factors have a PAC.
R=.93R=.93
% of Patients with at least 1 PAC
0%
20%
40%
60%
80%
100%
0 10 20 30 40
Count of Risk Factors
Perc
enta
ge o
f P
atients
with P
AC
s
R=.95R=.95

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 2929
Similar trends in other chronics
29
Percentage of patients with a PAC and PAC costs increase as count of risk factors increase.
R=.94R=.94
R=.97R=.97
R=.97R=.97
R=.97R=.97

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 3030
Chronic Conditions: PAC types
30
Look at which PAC Types are the most costly. Here, Type 2 PACs are the driver of PAC costs for most of the chronic ECRs, especially CAD and CHF. Note that GERD has the highest PAC costs of all the chronic ECRs.

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 31
Summary of PAC Hospitalizations and Professional Services
31
PAC Professional Services for Type 1 and Type 2 PACs are higher in PAC costs and occurrences than PAC hospitalizations among the chronic ECRs.

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 3232
Top Drivers of PAC professional costs: Chronic
PAC Description Asthma CAD CHF Diabetes HTN COPD GERD Total
Emergency Room Visits 23% 0% 11% 14% 18% 19% 0% 12%
Acute Flare-up of Index Condition 17% 5% 2% 2% 2% 15% 25% 12%
Urinary Tract Infections and other Hospital Acquired Infections
6% 6% 3% 4% 9% 5% 6% 6%
Diabetic Emergency, Hypo-Hyper-Glycemia
1% 5% 2% 14% 0% 2% 1% 5%
Subarachnoid And Intracerebral Hemorrhage (Stroke, CVA)
1% 5% 3% 2% 0% 2% 2% 2%
Cardiac Dysrhythmias 13% 1% 2% 1% 0% 13% 0% 4%
Pneumonia, Lung Complications, Respiratory Failure
7% 5% 6% 3% 1% 8% 3% 4%
Acute Renal Failure, other Kidney Problems
1% 1% 24% 5% 0% 1% 1% 3%
Gastritis, Ulcer, GI Hemorrhage 8% 13% 3% 9% 15% 10% 6% 9%
Syncope, Hypotension, Dizziness 4% 16% 9% 8% 24% 3% 8% 9%
Cellulitis, Skin Infections 8% 16% 8% 18% 16% 9% 4% 11%
Phlebitis, DVT, Pulm Embolism, Decubitus Ulcer
5% 13% 16% 15% 3% 6% 5% 8%
Adverse Drug Events, Complications of Medical Care
6% 15% 9% 6% 11% 8% 20% 11%
Total 100% 99% 100% 100% 100% 100% 81% 95%
Total Costs $5,378,832 $1,656,991 $1,739,690 $8,436,550 $2,997,458 $3,698,074$8,983,986 $32,891,581
32

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 3333
Top Drivers of Index Stay PACs
PAC DescriptionInpatient Medical
Inpatient Procedural
Outpatient Procedural
Complications directly related to Index Surgery 0.00% 32.89% 82.65%
Hospital Acquired Infections 22.62% 4.27% 1.53%
Diabetic Emergency, Hypo- Hyper-Glycemia 4.09% 3.12% 0.61%
Stroke, CVA, other Nervous System diseases 4.85% 0.48% 1.40%
Blood and Cardiovascular Problems 4.04% 3.05% 0.06%
Pneumonia, Lung Complications, Respiratory Failure 18.54% 28.06% 1.54%
Acute Renal Failure, Other Kidney Disease 2.03% 3.81% 0.21%
Gastritis, Ulcer, GI Disorders, Abdominal Pain 2.36% 3.74% 0.85%
Fluid and Electrolyte Disturbances, Syncope, Collapse 0.00% 0.00% 1.03%
Cellulitis, Skin Infections, Skin Disorders 2.63% 2.60% 1.78%
Falls, Orthopedic Problems 0.00% 0.00% 0.04%
Phlebitis, DVT, Pulm Embolism, Decubitus Ulcer 9.66% 5.64% 0.99%
Adverse Drug Events, Complications of Medical Care 17.66% 11.77% 7.24%
Acute Flare-up of Index Condition 11.29% 0.00% 0.00%
Total 99.76% 99.25% 99.94%
Total Costs $3,991,962 $7,786,668 $17,883,242
After reviewing the top drivers of Index Stay PACs among the Inpatient and Outpatient ECRs, a few PACs stand out as areas to target for quality improvement: Complications directly related to Index Surgey, Hospital Acquired Infections, Pneumonia/Lung Complications, and ADEs

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc. 34
Summary
• Becoming an ACO is not a slam dunk
• It may be best to view accountable care as a progressive “verb” rather than a pre-ordained noun
• Incremental planning and execution will prevent many organizational failures (Rome was not built in a day)
• Margins per patient is the hallmark of sound budget-based performance
• Understanding sources of variation on a per episode basis is critical (PMPMs reveal little actionable information)

Proprietary & Confidential. Health Care Incentives Improvement Institute, Inc.
For contact information:www.HCI3.orgwww.bridgestoexcellence.orgwww.prometheuspayment.org