Embed Size (px)
Citation preview

Case Report
New Sonographic Appearance of HepaticMesenchymal Hamartoma in Childhood
Chrisoula Koumanidou, MD, Marina Vakaki, MD, Marina Papadaki, MD, George Pitsoulakis, MD,Despina Savvidou, MD, Konstantinos Kakavakis, MD
Radiology Department, Children’s Hospital Agia Sofia, Thibon and Livadias TT11527, Athens, Greece
Received 20 February 1998; accepted 14 October 1998
ABSTRACT: We present clinical, radiographic, andsonographic findings in 3 children with hepatic mes-enchymal hamartoma, a rare benign tumor of child-hood. The presence of round hyperechoic parietalnodules within the cystic spaces of the hamartomas isa new sonographic finding. © 1999 John Wiley &Sons, Inc. J Clin Ultrasound 27:164–167, 1999.
Keywords: mesenchymal hamartoma; liver; infant;child; ultrasonography
Mesenchymal hamartoma is a rare benign he-patic lesion most often encountered in in-
fants.1–3 Approximately 25% of benign hepatic tu-mors in infants are mesenchymal hamartomas.4
The lesion is considered a developmental anomalyrather than a true neoplasm.5–8 A hepatic mesen-chymal hamartoma in a 6-month-old boy found inassociation with a mesenchymal tumor of the pla-centa during fetal life supports the theory thatthis lesion is a developmental anomaly that canaffect more than 1 organ during fetal life.8 How-ever, the presence of a specific translocation inthe long arm of chromosome 19 in some patientswith mesenchymal hamartomas suggests that aneoplastic process cannot be ruled out.9 We reporta new sonographic feature of mesenchymal ham-artoma in 1 infant and 2 children with this con-dition.
CASE 1
A 3-month-old girl presented with progressive ab-dominal enlargement and respiratory distress. A
palpable mass in the right upper quadrant of theabdomen was detected on physical examination.All laboratory data, including results of liverfunction tests and serum a-fetoprotein level, werewithin normal limits. A chest radiograph was nor-mal. A plain abdominal radiograph demonstrateda large, noncalcified intrahepatic mass displacingthe intestinal loops to the left and inferiorly.
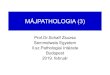
Sonographic examination of the abdomen re-vealed a large, well-circumscribed mass withoutan identifiable capsule. The mass consisted ofmultiple cysts involving predominantly the righthepatic lobe and part of the left. The cystic spacesranged from 3 to 4 cm in diameter and containedthin mobile septations and round echogenic pari-etal nodules (Figure 1). A second sonographic ex-amination performed a few days later revealed nochange in either the size or echogenicity of theparietal nodules. Given the cystic nature of themass and the presence of parietal nodules, thediagnosis of hepatic teratoma was considered themost likely.
At surgery, a large, soft, cystic mass was re-sected. On gross examination, the 850-g lesionwas well demarcated from the surrounding nor-mal hepatic parenchyma. The lesion was com-posed of 5 cysts, each measuring approximately 4cm in diameter and containing viscous materialand septae. Three cysts each contained 1 parietalnodule, the greatest diameter of which was ap-proximately 8 mm. Histologic examination re-vealed that the lesion consisted of edematous ma-ture connective tissue and multiple cystic cavitiescontaining viscous fluid. The cyst walls consistedof fibrotic tissue, and the parietal nodules werecomposed of islands of edematous hepatic paren-
Correspondence to: C. Koumanidou, Aiantos 41, Pal Phaliro,Athens GR-17562, Greece
© 1999 John Wiley & Sons, Inc. CCC 0091-2751/99/030164-04
164 JOURNAL OF CLINICAL ULTRASOUND

chyma with scattered plasma cells and eosino-phils, indicative of chronic inflammation.
CASE 2
A 28-month-old girl presented with progressiveabdominal enlargement and a 3-day history ofvomiting. A palpable right upper quadrant masswas detected on physical examination. All labora-tory data, including results of liver function testsand a-fetoprotein level, were within normal lim-its. A plain abdominal radiograph demonstratedhepatomegaly and displacement of intestinal gasto the left and inferiorly.
Abdominal sonography revealed the presenceof 3 cystic masses in the right hepatic lobe. Thediameter of the largest mass was 5 cm. The cysticspaces contained thin septations and round echo-genic nodules (Figure 2). The preoperative differ-ential diagnosis, based on the cystic nature of thelesion and the presence of parietal nodules, in-cluded cystic teratoma and mesenchymal hamar-toma.
The patient underwent a right hepatic lobec-tomy, and a large, soft, well-circumscribed masswas resected. No identifiable capsule was foundon gross examination. The mass, weighing 1,000g, was composed of 3 cystic spaces and loose mes-enchymal connective tissue. The cystic spaces,measuring 4–5 cm in diameter, were thick-walledand contained clear fluid. Parietal nodules mea-suring 5 mm in diameter were noted in 2 of the 3cystic spaces. Histologic examination showed the
lesion to be composed of hepatic parenchyma andloose connective tissue. Bile duct proliferation,edematous fibroblasts, and cells indicative ofchronic inflammation were identified in the solidpart of the mass. The parietal nodules consisted ofbile ducts and small clusters of hepatocytes.
CASE 3
A 3-year-old boy presented with a 3-week historyof massive abdominal distention. Physical exami-nation revealed a huge, firm, right-quadrantmass. All laboratory data, including a-fetoproteinlevel and results of liver function tests, were nor-mal. A plain radiograph of the abdomen showed ahuge hepatic mass displacing the intestinal gasinferiorly and to the left.
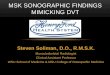
Sonography revealed a mass consisting of mul-tiple cystic spaces occupying the right lobe andpart of the left lobe of the liver. Thin echogenicseptae, low-level internal echoes, and a small pa-rietal nodule were demonstrated within the cysticspaces (Figure 3). CT confirmed the sonographicfindings but did not visualize the thin septae orthe parietal nodule. Repeat sonography carriedout 2 weeks later showed no change in the size orfeatures of the tumor.
At surgery, a well-delineated 1,500-g massarising from the hepatic parenchyma was re-moved en bloc. Pathologic examination showedthe specimen to be predominantly cystic, contain-ing 1 10-cm cyst and several 2–3-cm cysts. Allcysts contained myxoid material. The largest cystcontained septae and 3 parietal nodules, the larg-est measuring 10 mm in diameter and the other 2
FIGURE 1. Case 1. Mesenchymal hamartoma in a 3-month-old girl.Transverse sonogram through the right lobe of the liver demon-strates multiple cysts occupying the right lobe. One cyst contains around echogenic parietal nodule (arrowhead).
FIGURE 2. Case 2. Mesenchymal hamartoma in a 28-month-old girl.Longitudinal sonogram through the right hepatic lobe shows a cysticmass with a round echogenic parietal nodule (arrowhead).
HEPATIC MESENCHYMAL HAMARTOMA
VOL. 27, NO. 3, MARCH/APRIL 1999 165

less than 5 mm. Sonography had revealed onlythe largest of these nodules. The solid mass be-tween the cystic spaces was white and fibrous. Onmicroscopic examination, the mass was found tobe composed of loose myxoid and connective tis-sue with islands of normal hepatic parenchyma.The walls between the cystic spaces were thin andlined with endothelium. The parietal noduleswere composed of elongated tortuous bile ductsand normal hepatocytes.
DISCUSSION
Mesenchymal hamartoma of the liver is a rare,benign, predominantly cystic tumor.6 It usuallyoccurs between the ages of 4 months and 2 years(mean, 16 months) and rarely affects older chil-dren.5,10 The condition occurs slightly more oftenin male children than in female children.5,10,11
Most patients present with painless abdominalenlargement or a palpable abdominal mass andmay have other symptoms such as vomiting, di-arrhea, or constipation.5 Large tumors can causerespiratory distress,7,12 and ruptured cystic tu-mors can cause ascites.11 The respiratory distressthat brought 1 of our patients to medical atten-tion was secondary to abdominal enlargement, asshown by the radiographic finding of a right el-evated hemidiaphragm but no other abnormali-ties. The serum a-fetoprotein level and other labo-ratory test results typically are normal.
Mesenchymal hamartoma occurs usually in theright lobe of the liver (65% of cases) and less often
in the left lobe (20%) or in both lobes (10%).10 Oneof our patients had a tumor in the right lobe, andthe other 2 had tumors in both lobes. Lesionsmost often present as large, solitary masses witha mean diameter of 16 cm5,6 and often weigh inexcess of 1,000 g.12 Occasionally masses are at-tached to the liver by a pedicle.5,10–12 Lesions areeasily distinguished from hepatic parenchyma,as they grow by expansion rather than infiltra-tion. Lesions are often—but not always2,7—nonencapsulated. All masses in our series werenonencapsulated.
Cystic mesenchymal hamartoma of the liver ischaracterized by an intrahepatic mass containingcysts ranging in diameter from a few millimetersto 15 cm. The cysts contain thin or semisolid ge-latinous material.5 Microscopic examination re-veals that the lesions are composed of loose mes-enchymal tissue with blood vessels, dilated bileducts, and well-differentiated hepatocytes.6,12
Abdominal radiography may demonstrate thepresence of a soft tissue mass in the right upperquadrant, as was true for our patients. The mass,if large enough, can extend to the pelvis, cross themidline, or displace the colon to the left and infe-riorly.1,5 Calcification is usually not detected,10,13
as was true for our patients.On abdominal sonography, mesenchymal ham-
artoma may appear as a mass consisting of mul-tiple small cysts surrounded by solid areas(edematous stroma or ‘‘Swiss cheese’’ appear-ance),3,5 with thick internal septations within thecysts12; a multiloculated cystic mass with mul-tiple thin echogenic septa,3,5,11,12 sometimes withscattered low-level echoes within these spaces1;or a solid mass that is slightly hyperechoic rela-tive to liver parenchyma.6,12 All of our cases in-volved masses consisting of large cystic spaceswith thin, mobile septations within the cysts. Thepresence of mobile septations in the cystic spacesof mesenchymal hamartoma, reported in only 1other case, is considered to be a distinctive sono-graphic finding for this tumor.14 The low-levelechoes detected inside the cystic spaces in 1 of ourpatients’ lesions probably reflected their gelati-nous contents.1 Round hyperechoic parietal nod-ules were seen in the cysts in all 3 of our patients.These nodules were not considered to be bloodclots, as neither their echogenicity nor their sizehad changed at a second sonographic examina-tion conducted a few days after the first. In 2cases, the number, size, and location of the nod-ules were correctly identified by sonography; inthe third, sonography identified only 1 of 3 nod-ules, probably because the cyst was large and thenodules were small. Histologically, these parietal
FIGURE 3. Case 3. Mesenchymal hamartoma in a 3-year-old boy.Transverse sonogram through the right hepatic lobe reveals a largecystic mass with scattered low-level internal echoes, septa (arrows),and a small round parietal nodule (arrowhead).
KOUMANIDOU ET AL
166 JOURNAL OF CLINICAL ULTRASOUND

nodules consisted of normal or edematous hepa-tocytes and normal or elongated and tortuous bileducts. One previous report on the histologic fea-tures of mesenchymal hamartoma described thepresence of small nodules of residual hepatic pa-renchyma at the periphery of the cystic spaces ofthe lesion.16 However, to our knowledge, the pres-ence of parietal nodules as a specific sonographicsign has not been reported. The location of thesenodules led us to regard cystic teratoma as themost likely diagnosis, the rarity of such a tumorbeing found in the liver15 notwithstanding.
Determining that a mesenchymal hamartomaoriginates from the liver parenchyma is not al-ways possible, especially for large tumors. Forlarge or pedunculated tumors, differentiationfrom loculated ascites,5,11 lymphatic malforma-tion, cystic duplication,5 and choledochal cyst12
should not be difficult. For tumors originatingfrom the liver, the differential diagnosis includessimple hepatic cyst (very rare in children),11 cys-tic hepatoblastoma (also very rare and associatedwith elevated a-fetoprotein level),5 malignantmesenchymoma (occurring in older children),2,3
abscess (associated with fever),5,12 and echinococ-cus cyst (positive anti-echinococcal antibodies).
The recommended treatment of mesenchymalhamartoma has been surgical excision.12,17 How-ever, some authors recommend resection onlywhen tumor growth interferes with respiration orcompresses adjacent organs, noting that the earlyprogressive growth of mesenchymal hamartomamay be followed by a decrease in size and devel-opment of calcification.18,19 We recommend ap-proaching each case on an individual basis. Nei-ther chemotherapy nor radiotherapy is necessaryafter resection because malignant transforma-tion, local relapse, and metastasis have neverbeen reported.5,12
REFERENCES
1. Donovan AT, Wolverson MK, deMello D, et al. Mul-ticystic hepatic mesenchymal hamartoma of child-hood. Pediatr Radiol 1981;11:163.
2. Federici S, Galli G, Cuoghi D. Cystic mesenchymalhamartoma of the liver. Pediatr Radiol 1992;22:307.
3. Pobiel RS, Bissett GS. Pictorial essay: imaging ofliver tumors in the infant and child. Pediatr Radiol1995;25:495.
4. Kwok WK, Spitz L, Brereton RJ, et al. Mesenchy-mal hamartoma of the liver. Pediatr Surg Int 1989;4:296.
5. Ros PR, Goodman LTC, Ishak KG, et al. Mesen-chymal hamartoma of the liver: radiologic-pathologic correlation. Radiology 1986;158:619.
6. Wholey MH, Wojno KJ. Pediatric hepatic mesen-chymal hamartoma demonstrated on plain film, ul-trasound and MRI, and correlated with pathology.Pediatr Radiol 1994;24:143.
7. Raffensperger JG, Gonzalez-Crussi F, Skeehan T.Mesenchymal hamartoma of the liver. J PediatrSurg 1983;5:585.
8. Alwaidh MH, Woodhall CR, Carty HT. Mesenchy-mal hamartoma of the liver: a case report. PediatrRadiol 1997;27:247.
9. Otal TM, Hendrics JB, Pharis P, et al. Mesenchy-mal hamartoma of the liver. DNA flow cytometricanalysis of eight cases. Cancer 1994;74:1237.
10. Kenney IJ, Hendry MA, Mackinlay GA. Spontane-ous regression of mesenchymal hamartoma: obser-vations using ultrasound. J Clin Ultrasound 1986;14:72.
11. George JC, Cohen MD, Tarver RD, et al. Rupturedcystic mesenchymal hamartoma: an unusual causeof neonatal ascites. Pediatr Radiol 1994;24:304.
12. Stanley P, Hall TR, Woolley MM, et al. Mesenchy-mal hamartomas of the liver in childhood: sono-graphic and CT findings. AJR Am J Roentgenol1986;147:1035.
13. Abramson SA, Lack EE, Teele RL. Benign vasculartumor of the liver in infants. Sonographic appear-ance. AJR Am J Roentgenol 1982;138:629.
14. Marti-Bonmati L, Olague R, Cortina H. Mesenchy-mal hamartoma of the liver in childhood [letter].AJR Am J Roentgenol 1987;148:1275.
15. Quinn SF, Erickson S, Black WC. Cystic ovarianteratomas: the sonographic appearance of the der-moid plug. Radiology 1985;155:477.
16. Lennington WJ, Gray GF, Page DL. Mesenchymalhamartoma of liver: a regional ischemic lesion of asequestered lobe. Am J Dis Child 1993;147:193.
17. Demaioribus CA, Lally KP, Sim K, et al. Mesen-chymal hamartoma of the liver. A 35-year review.Arch Surg 1990;74:598.
18. Barnhart DC, Hirschi RB, Garver KA, et al. Con-servative management of mesenchymal hamarto-ma of the liver. J Pediatr Surg 1997;32:1495.
19. Leary DL, Weiskittel DA, Blane CE, et al. Follow-up imaging of benign pediatric liver tumors. Pedi-atr Radiol 1989;19:234.
HEPATIC MESENCHYMAL HAMARTOMA
VOL. 27, NO. 3, MARCH/APRIL 1999 167