Embed Size (px)
Citation preview
New Treatments and Combinations for Relapsed
Chronic Lymphocytic Leukemia (CLL)
Susan O’BrienUC Irvine Health

Susan O’Brien, MD1,2, Richard R. Furman, MD3, Steven Coutre, MD4, Ian W. Flinn, MD, PhD5, Jan Burger, MD, PhD1, Kristie Blum, MD6,
Jeff Sharman, MD7, William Wierda MD, PhD1, Jeffrey Jones MD, MPH6, Weiqiang Zhao, MD, PhD6, Nyla A. Heerema, PhD6, Amy J. Johnson, PhD6,
Ying Luan, PhD8, Danelle F. James, MD, MAS8, Alvina D. Chu, MD8, John C. Byrd, MD6
Five-Year Experience With Single-Agent Ibrutinib in Patients With Previously Untreated and
Relapsed/Refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Leukemia

Best Response
87% 89% 89%
Median DOR, months (range) NR (0.0+ to 65.5+) 56.8 (0.0+ to 65.5+) NR (0.0+ to 65.5+)Median follow-up, months (range) 62 (1 – 67) 49 (1+ – 67) 56 (1+ – 67)
CRPRPR-L
TN (n=31) R/R (n=101) Total (N=132)
NR, not reached. O’Brien SM, et al. Blood. 2016;128: Abstract 233.

Survival Outcomes: Overall Population
NR, not reached.
Median PFS 5-year PFSTN (n=31) NR 92%R/R (n=101) 52 mo 43%
Progression-Free Survival Overall Survival
Median OS 5-year OSTN (n=31) NR 92%R/R (n=101) NR 57%
O’Brien SM, et al. Blood. 2016;128: Abstract 233.
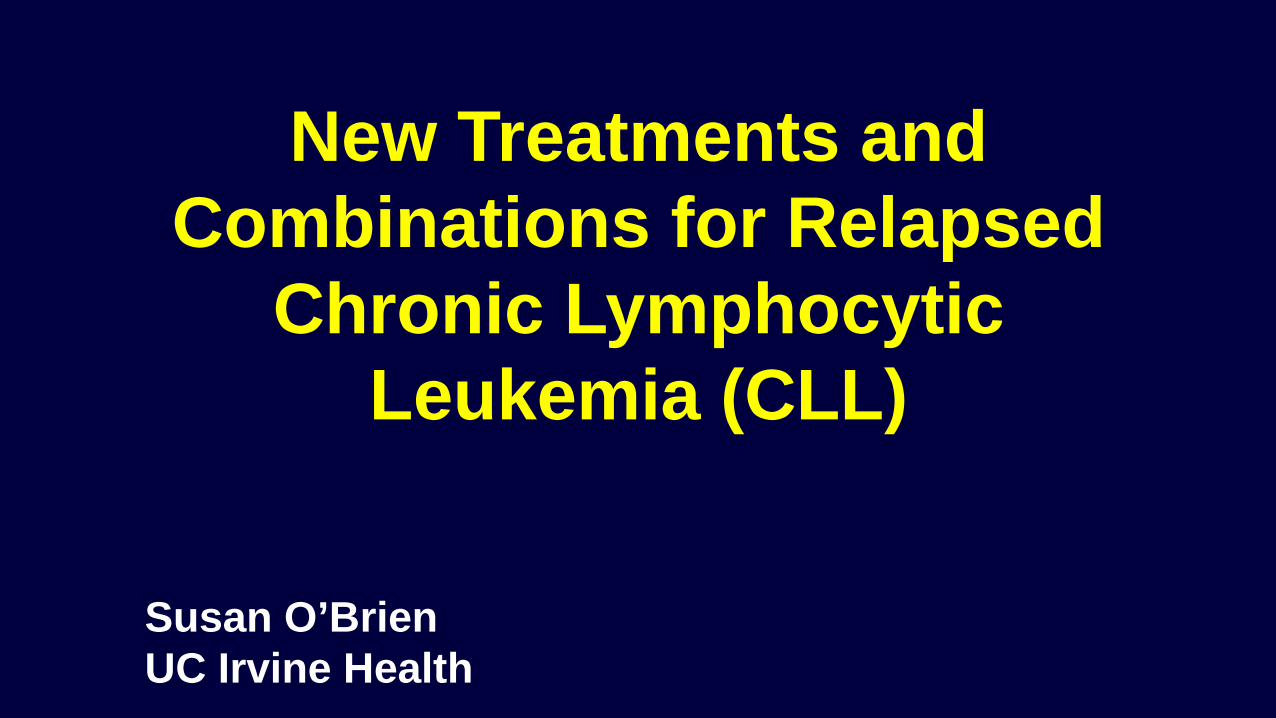
Survival Outcomes by Chromosomal Abnormalities Detected by FISH in R/R Patients*
**No del17p, del11q, del13q, or trisomy 12; in hierarchical order for del17p, and then del11qNR, not reached.
Progression-Free Survival Overall Survival
*Only 2 patients in the TN group showed PD or death. Subgroup analyses, therefore, focused on the R/R population.
Median OS 5-year OS
Del17p (n=34) 57 mo 32%Del11q (n=28) NR 61%Trisomy 12 (n=5) NR 80%Del13q (n=13) NR 91%No abnormality** (n=16) NR 83%
Median PFS 5-year PFS
Del17p (n=34) 26 mo 19%Del11q (n=28) 55 mo 33%Trisomy 12 (n=5) NR 80%Del13q (n=13) NR 91%No abnormality** (n=16) NR 66%
O’Brien SM, et al. Blood. 2016;128: Abstract 233.

Venetoclax Monotherapy for Patients with Chronic Lymphocytic Leukemia (CLL) who
Relapsed After or Were Refractory to Ibrutinib or Idelalisib
Jeffrey Jones,1 Michael Y. Choi,2 Anthony R. Mato,3 Richard R. Furman,4 Matthew S. Davids,5Leonard Heffner,6 Bruce D. Cheson,7 Nicole Lamanna,8 Paul M. Barr,9 Herbert Eradat,10
Ahmad Halwani,11 Brenda Chyla,12 Maria Verdugo,12 Rod A. Humerickhouse,12 Jalaja Potluri,12 William G. Wierda,13 Steven Coutre14
American Society of Hematology ● San Diego, California ● 5 December 2016

• To mitigate TLS risk, patients received prophylaxis with uric acid lowering agents and hydration starting at least 72 hours before first venetoclax dose
• Patients with high tumor burden were hospitalized for first dose at 20 and 50 mg and received IV hydration and rasburicase
• Laboratory values were monitored at first dose and each subsequent dose increase
Venetoclax Dosing Schedule and TLS Mitigation
7
High tumor burden: any lymph node ≥10 cm; or both lymph node ≥5 cm and ALC ≥25x109/LJones J, et al. Blood. 2016;128: Abstract 637.

Patient CharacteristicsArm An=43
Arm Bn=21
Age, median (range), years 66 (48 – 80) 68 (56 – 85)Unmutated IGVH,* n/N (%) 25/29 (86) 11/13 (85)del(17)(p13.1),* n/N (%) 21/43 (49) 2/21 (10) Baseline laboratory values, median (range)
CrCl, mL/minHemoglobin, g/dLPlatelet count, x109/LNeutrophil count, x109/LLymphocyte count, x109/L
83 (54 – 119)11.2 (5.8 – 14.6) 117 (20 – 446)
3.5 (0 – 24) 19 (.2 – 263)
75 (44 – 140) 12.2 (7.1 – 14.4)115 (30 – 439)
2.4 (0 – 49)14 (.3 – 407)
Bulky nodal disease, n (%)≥5 cm≥10 cm
15 (35)7 (16)
11 (52)5 (24)
Prior therapies, median (range) 4 (1 – 12)† 3 (1 – 11)†
Prior ibrutinib, n (%)Months on ibrutinib, median (range)Refractory, n (%)
43 (100)17 (1 – 56)
39 (91)
5 (24)6 (2 – 11)
2 (10)Prior idelalisib, n (%)
Months on idelalisib, median (range)Refractory, n (%)
4 (9)10 (2 – 31)
2 (5)
21 (100)8 (1 – 27)14 (67)
*Site reported data.†2 received only frontline ibrutinib; 2 received only frontline idelalisib.
Jones J, et al. Blood. 2016;128: Abstract 637.

EfficacyArm An=43
Arm Bn=21
Best response, n (%)Assessed by Assessed by
IRC Investigator IRC InvestigatorORR 30 (70) 29 (67) 13 (62) 12 (57)
CR/CRi 0/1 (2) 2 (5)/1 (2) 0/0 2 (10)/1 (5)
nPR 0 2 (5) 0 0PR 29 (67) 24 (56) 13 (62) 9 (43)
Non-responder*SDPDD/C‡
13 (30)–––
14 (23)9 (21)1† (2)4 (9)
8 (38)–––
9 (43)8 (38)1† (5)
0*Non-responder category for IRC includes both SD or PD, which were not identified as separate categories per IRC.†CLL progression and discontinued due to progression.‡D/C, patient discontinued the study prior to assessment.
Jones J, et al. Blood. 2016;128: Abstract 637.

• Median DoR, PFS, and OS had not been reached after 11.8 months of follow up• Estimated 12 month PFS for all patients: 80% (95% CI: 67%, 89%)
Efficacy Per Independent Review
0 2 4 6 8 1 0 1 2 1 40
2 5
5 0
7 5
1 0 0
D u ra t io n o f R e s p o n s e
M o n th s s in c e f irs t d o s e
Pa
tie
nts
wit
h R
es
po
ns
e (
%)
N o . a t r is k 3 0 2 9 2 3 1 8 1 0 11 0 8 6 5 2
4 0 3 7 2 9 2 3 1 2 1
A rm A (R /R ib ru t in ib )
A rm B (R /R id e la lis ib )
A ll p a t ie n ts
0 2 4 6 8 1 0 1 2 1 40
2 5
5 0
7 5
1 0 0
P ro g re s s io n -F re e S u rv iv a l
M o n th s s in c e f irs t d o s e
Pro
gre
ss
ion
-fre
e s
urv
iva
l (%
)
4 3 3 7 3 6 2 8 2 7 1 5 32 1 1 7 1 5 6 5 26 4 5 4 5 1 3 4 3 2 1 7 3
A rm A (R /R ib ru t in ib )
A rm B (R /R id e la lis ib )
A ll p a t ie n ts
Data as of 10June2016Jones J, et al. Blood. 2016;128: Abstract 637.
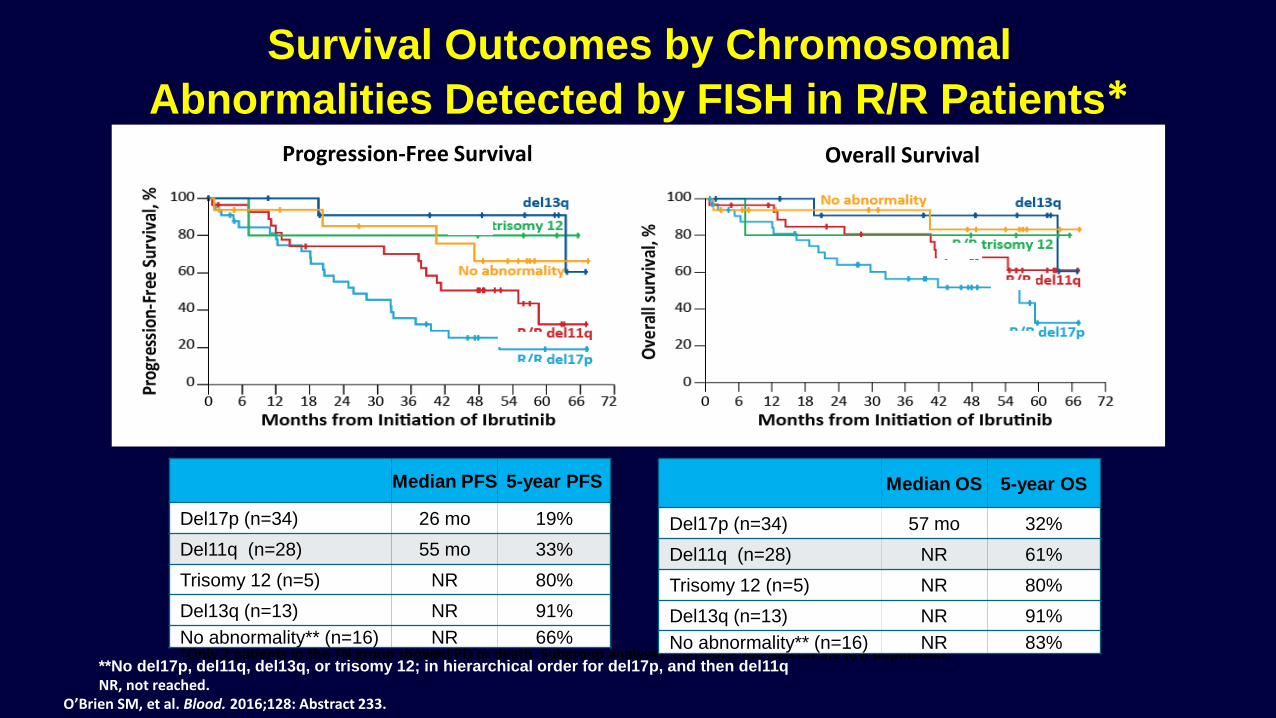
Minimal Residual Disease in Peripheral Blood
11
• 14/31 (45%) patient samples have demonstrated MRD-negative peripheral blood between Weeks 24 – 48
• 5 patients demonstrating sustained MRD negative status in blood had subsequent marrow evaluations; 1 patient was MRD negative in bone marrow
*Patient had persistent splenomegaly and thrombocytopenia; categorized as stable disease by investigator.#Also had confirmed bone marrow MRD-negative assessment.
Data as of 10June2016
0 .0 1
0 .2 50 .5 00 .7 5
1 0
2 0
3 0
A rm A (R /R ib ru t in ib )
P a tie n ts
% C
LL
Ce
lls
0 .0 1
0 .2 50 .5 00 .7 5
12345
A rm B (R /R id e la lis ib )
P a tie n ts
% C
LL
Ce
lls
* #
MRD-positive MRD-negative CRi PR Non-responder by IRC
Jones J, et al. Blood. 2016;128: Abstract 637.

Outcomes of CLL Patients Treated With Sequential Kinase Inhibitor
Therapy: A Real World Experience
Mato AR, Nabhan C, Barr PM, Ujjani CS, Hill BT, Lamanna N, Skarbnik AP, Howlett C, Pu JJ, Sehgal AR, Strelec LE, Vandegrift A,
Fitzpatrick DM, Zent CS, Feldman T, Goy A, Claxton DF, BachowSH, Kaur G, Svoboda J, Nasta SD, Porter D, Landsburg DJ,
Schuster SJ1, Cheson BD, Kiselev P, Evens AM
Mato et al. Blood. 2016 Nov 3;128(18):2199-2205. Epub 2016 Sep 6;
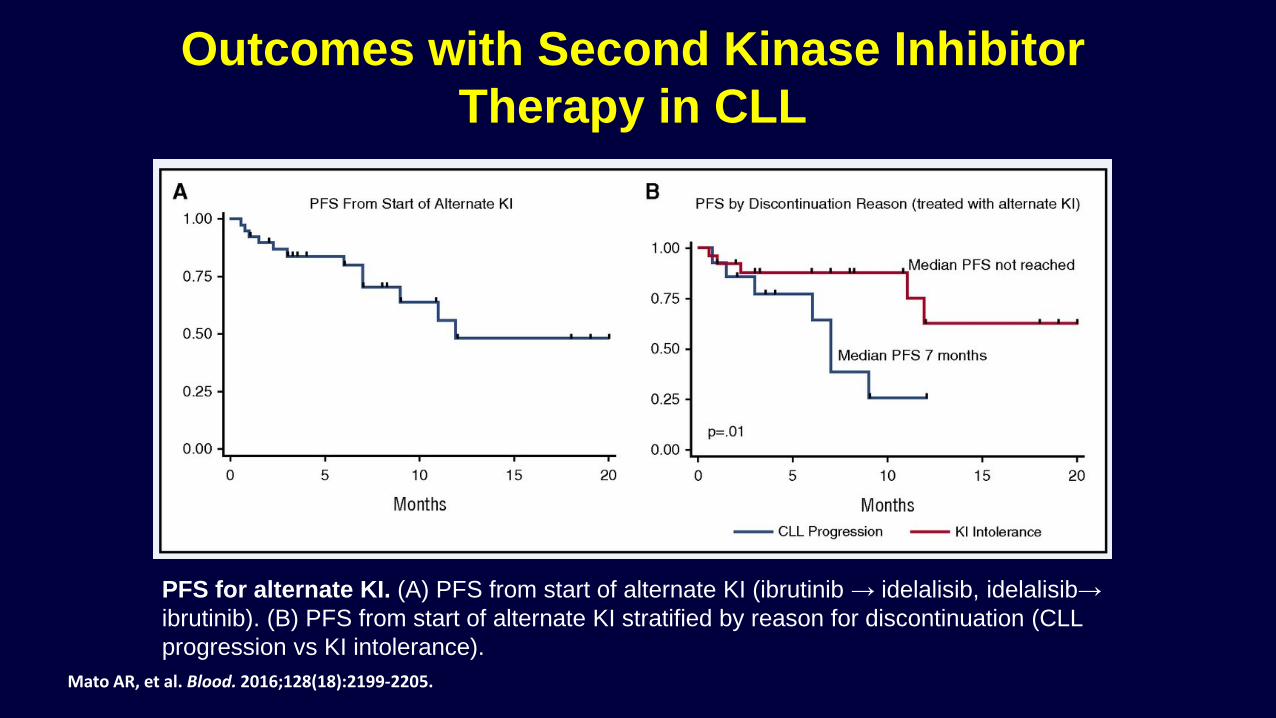
PFS for alternate KI. (A) PFS from start of alternate KI (ibrutinib → idelalisib, idelalisib→ ibrutinib). (B) PFS from start of alternate KI stratified by reason for discontinuation (CLL progression vs KI intolerance).
Outcomes with Second Kinase Inhibitor Therapy in CLL
Mato AR, et al. Blood. 2016;128(18):2199-2205.

Phase 1b Results of a Phase 1b/2 Study of Obinutuzmab, Ibrutinib, and Venetoclax in Relapsed/Refractory
Chronic Lymphocytic Leukemia (CLL)Jeffrey A. Jones, MD, MPH1; Jennifer Woyach, MD1;
Farrukh T. Awan, MD1; Kami J. Maddocks, MD1; Thomas Whitlow, BA2; Amy S Ruppert, MAS1; and John C. Byrd,
ASH 2016

Treatment Schema
Jones JA, et al. Blood. 2016;128: Abstract 639.

Cycle 9 Treatment Response
Jones JA, et al. Blood. 2016;128: Abstract 639.

Safety
17
Event, n (%)All Patients
N=64
Any grade AE 64 (100)Common all-grade AEs
(≥20% patients)
Neutropenia
Thrombocytopenia
Diarrhea
Nausea
Anemia
Fatigue
Decreased WBC
Hyperphosphatemia
37 (58)
28 (44)
27 (42)
26 (41)
23 (36)
20 (31)
14 (22)
14 (22)
Event, n (%)All Patients
N=64
Grade 3/4 AEs 53 (83)Common grade 3/4 AEs (≥10% patients)
NeutropeniaThrombocytopeniaAnemiaDecreased WBCFebrile neutropeniaPneumonia
29 (45)18 (28)14 (22)8 (13)7 (11)7 (11)
Serious AEs 34 (53)Febrile neutropeniaPneumoniaMulti-organ failureSeptic shockIncreased potassium
6 (9)5 (8)2 (3)2 (3)2 (3)
• No clinical TLS was observed; 1 patient with high tumor burden met Howard criteria for laboratory TLS
Data as of 10June2016Jones JA, et al. Blood. 2016;128: Abstract 639.

Conclusions• Obinutuzumab, ibrutinib, and venetoclax can be safely
administered at each single agent dose• Dose-limiting toxicity was not observed • Adverse events were manageable and largely consistent with
those reported in studies of the single-agents– Hematologic toxicity was common but manageable– Grade 3/4 non-hematologic toxicity was uncommonly
observed• Responses were recorded at Cycle 9 in all patients assessed
– MRD negativity at cycle 9 was achieved in PB for 7 of 10 and in BM for 4 of 10 patients assessed
• Accrual is nearly completed to parallel phase 2 cohorts of relapsed/refractory (n=25) and treatment-naive (n=25) patients.
Jones JA, et al. Blood. 2016;128: Abstract 639.

Kirsten Fischer, MD, Anna-Maria Fink, MD, Helen Bishop, Mark Dixon, Jasmin Bahlo, Michael Y.Choi, MD, Robert Weinkove, MD, PhD, Sue Robinson, MD, Martin Dreyling, MD, PhD, TillSeiler, MD, Stephen Opat, MD, Carolyn Owen, MD, Javier Lopez Sr., MD, PhD, Nadine Kutsch,MD, Eugen Tausch, MD, Matthias Ritgen, MD, Rod Humerickhouse, MD, Kathryn Humphrey,Michael K. Wenger, MD, Valentin Goede, MD, Barbara Eichhorst, MD, Clemens-MartinWendtner, MD, Stephan Stilgenbauer, MD, Thomas J. Kipps, MD, PhD and Michael Hallek, MD
496 Results of the Safety Run-In Phase of CLL14 (BO25323): A Prospective,Open-Label, Multicenter Randomized Phase-III Trial to Compare the Efficacyand Safety of Obinutuzumab and Venetoclax (GDC-0199/ABT-199) withObinutuzumab and Chlorambucil in Patients with Previously Untreated CLLand Coexisting Medical Conditions
ASH 2016
Fischer et al. Blood. 2017 May 11;129(19):2702-2705

*CIRS > 6and/ or
CrCl < 70mL/min
Patients with untreated active CLL & with coexisting medical conditions*
Obinutuzumab + Chlorambucil6 x Obinutuzumab + Chlorambucil
+ 6 x Chlorambucil
Obinutuzumab + Venetoclax6 x Obinutuzumab + Venetoclax
+ 6 x Venetoclax
Follow-up Phase
Independent Data Monitoring Commitee (iDMC)
Safety Run-In Phase: Obinutuzumab + Venetoclax
Design
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Stopping Criteria
One treatment-related death
One grade 4 adverse event related to a clinical tumor lysis syndrome despite protocol-specified prophylaxis
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Treatment Schedule: 12 cycles
*Venetoclax Ramp-up during course 1 and 2
Obinutuzumab (iv infusion)100 mg day 1, 900 mg day 2, 1000 mg day 8, day 15 of course 1, 1000 mg courses 2- 6, day 1Venetoclax (oral tablet) 20 mg daily during course 1, day 22-2850 mg daily during course 2, day 1-7100 mg daily during course 2, day 8-14200 mg daily during course 2, day 15-21400 mg daily during course 2, day 22-28400 mg daily courses 3 -12, day 1-28
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Patient CharacteristicsN=13Median age 75 years (59-88)
Binet stage
A 15%
B 23%
C 62%
Median CIRS score 8 (6-14)Median CreaClearance 58 mL/min (30-108)TLS risk categoryLow 0%Medium 62%High 39%
Fischer K, et al. Blood. 2017;129(19):2702-2705.

AE Term Percentage
Neutropenia 58%IRR 8%Syncope 17%Thrombocytopenia 17%TLS 17%Febrile Neutropenia 25%Bradycardia 8%Hyperglycaemia 8%Influenza 8%Leukopenia 8%Pyrexia 8%Respiratory Tract Infection 3%Transaminases Increased 8%
N=13
Grade 3-4 Adverse Events
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Overall Response Rate
At Month 15
ORR 100%
CR 58%
PR+ 42%
N=12
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Minimal Residual Disease
At Month 15
MRD Level PB BM
Negative (< 10-4) 11/12 5/7
Intermediate (≥ 10-4 and < 10-2) 1/12 2/7
N=11
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Summary
None of the protocol defined stopping criteria were met
Initiating treatment with obinutuzumab followed by venetoclax appears safeolerable in this population
The treatment induced substantial responses with a high number of MRD negative responses
The main phase completed recruitment in August 2016 after 432 patients had been randomized
Run-in phase
Fischer K, et al. Blood. 2017;129(19):2702-2705.

Tolerability and activity of chemo-free triplet combination of umbralisib
(TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
Loretta Nastoupil, MD1, Matthew A. Lunning, DO2, Julie M. Vose, MD2, Marshall T. Schreeder, MD3, Tanya Siddiqi, MD4, Christopher R. Flowers, MD5,
Jonathon B. Cohen, MD5, Jan A. Burger, MD1, William G. Wierda, MD1, Susan O’Brien, MD6, Peter Sportelli7, Hari P. Miskin, MS7,
Michelle A. Purdom, RN, PhD7, Michael S. Weiss7 and Nathan H. Fowler, MD1
Presented at the 14th International Conference on Malignant LymphomaLugano, Switzerland ● June 14 – 17, 2017

Ublituximab
Single agent activity observed in rituximab refractory patients1
90 minute infusion times

Umbralisib (TGR-1202)Next generation PI3Kδ inhibitor, with a unique structure and improved tolerability
Umbralisib(TGR-1202)
Idelalisib(GS-1101)
Duvelisib(IPI-145)
Delta Delta Delta/GammaQD BID BID
ON
O
F
N
N
N
H2N
O F
F
N
N
O
N
N
HNN
NH
F
N
O
N
N
HNN
NH
Cl
Burris HA, et al. J Clin Oncol. 2015;34(suppl): Abstract 7069.

• Both ibrutinib and TGR-1202 were administered QD starting on Day 1• Efficacy assessed at Week 8 and every 12 weeks thereafter• After Month 12, all patients remain on TGR-1202 and ibrutinib once-
daily
Nastoupil L, et al. Presented at: the 14th International Conference on Malignant Lymphoma. June 14-17, 2017. Lugano, Switzerland.
Study Design
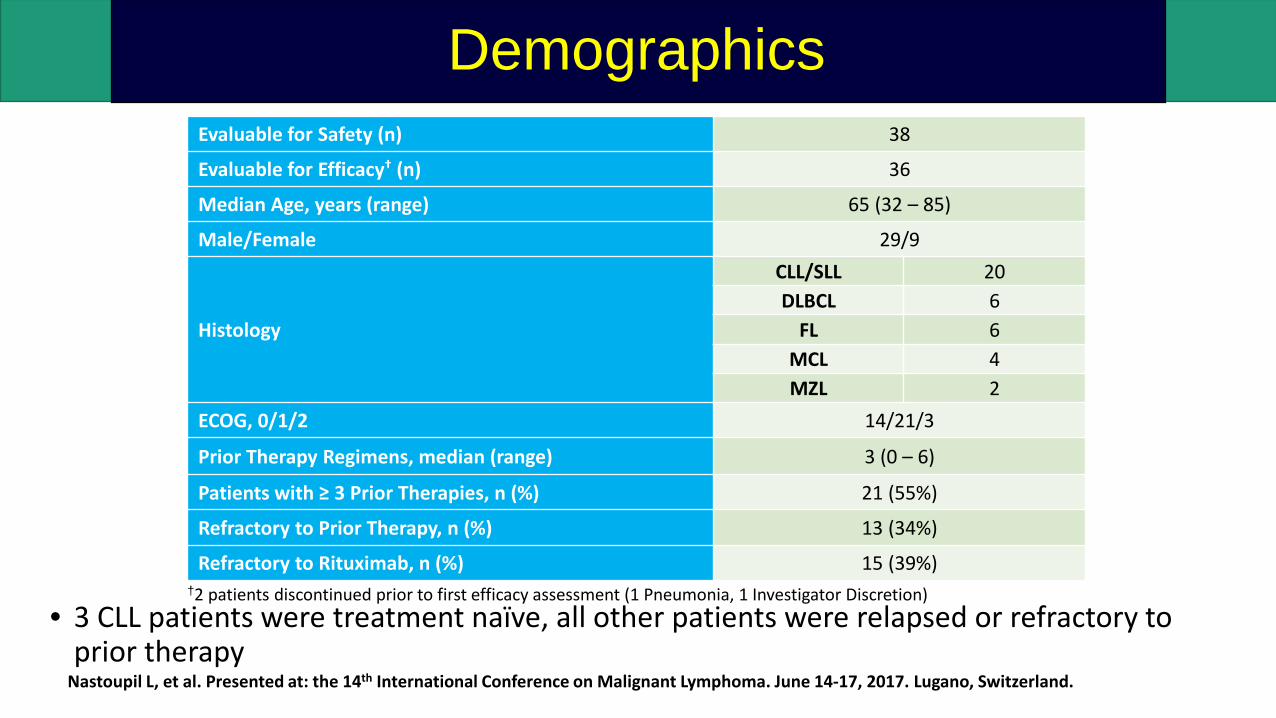
†2 patients discontinued prior to first efficacy assessment (1 Pneumonia, 1 Investigator Discretion)
Evaluable for Safety (n) 38
Evaluable for Efficacy† (n) 36
Median Age, years (range) 65 (32 – 85)
Male/Female 29/9
Histology
CLL/SLL 20DLBCL 6
FL 6MCL 4MZL 2
ECOG, 0/1/2 14/21/3
Prior Therapy Regimens, median (range) 3 (0 – 6)
Patients with ≥ 3 Prior Therapies, n (%) 21 (55%)
Refractory to Prior Therapy, n (%) 13 (34%)
Refractory to Rituximab, n (%) 15 (39%)
• 3 CLL patients were treatment naïve, all other patients were relapsed or refractory to prior therapy
Demographics
Nastoupil L, et al. Presented at: the 14th International Conference on Malignant Lymphoma. June 14-17, 2017. Lugano, Switzerland.

Adverse EventAll Grades Grade 3/4N % N %
Diarrhea 18 47% 1 3%Fatigue 18 47% - -
Dizziness 14 37% 1 3%Insomnia 13 34% - -
Nausea 13 34% - -Neutropenia 12 32% 7 18%
Cough 12 32% - -Infusion related reaction 12 32% - -
Thrombocytopenia 11 29% 3 8%Pyrexia 11 29% 1 3%
Rash 11 29% 1 3%Anemia 10 26% 1 3%Sinusitis 9 24% - -Dyspnea 8 21% 1 3%
Stomatitis 8 21% 1 3%
• 1 DLT (reactivated varicella zoster) occurred CLL cohort level 1. No other DLT’s were observed.
• Diarrhea majority Gr. 1 (32%) and Gr. 2 (13%), with no Gr. 4 event reported.
• Pneumonia (11% Gr. 3/4) and neutropenia were the only Gr. 3/4 AE’s in >10% of patients
• Two patients discontinued due to an AE (sepsis and pneumonia)
• Median time on study 11.1 months (range 0.4 – 30+ months)
Safety
Nastoupil L, et al. Presented at: the 14th International Conference on Malignant Lymphoma. June 14-17, 2017. Lugano, Switzerland.

• CLL• 8/16 (50%) had 17p and/or 11q deletion• All 3 treatment naïve patients achieved a PR• 3 had a prior BTK and/or PI3Kδ inhibitor, including one patient refractory to both idelalisib and ibrutinib (ongoing CR,
1.5+ years)
• FL patients were heavily pretreated including 2 with prior ASCT, 1 refractory to prior ibrutinib, and 1 with 5 prior lines ofrituximab based therapy
• DLBCL • Median of 4 prior therapies• 4/6 were of non-GCB subtype, including the sole responder
Type Pts (n)
CR†
(n)PR(n)
ORRn (%)
SD(n)
PD(n)
CLL/SLL 19 6 13 19 (100%) - -MZL 2 1 1 2 (100%) - -MCL 4 2 2 4 (100%) - -
FL 5 1 3 4 (80%) 1 -DLBCL 6 - 1 1 (17%) - 5Total 36 10 20 30 (83%) 1 5
†CLL: 4/6 CR’s pending bone marrow confirmation
Efficacy: Overall Response Rate
Nastoupil L, et al. Presented at: the 14th International Conference on Malignant Lymphoma. June 14-17, 2017. Lugano, Switzerland.

Conclusions• Ibrutinib produces very durable remissions in both relapsed
and frontline patients.
• Venetoclax is the treatment of choice in patients failing a B-cell receptor inhibitor
• Novel combinations producing very exciting results with high degree of MRD negativity• Ibrutinib, venetoclax and obinutuzumab, MRD negativity in
relapse: 7/10 in PB, 4/10 in BM at cycle 9 of 14• Ventetoclax and obinutuzumab, MRD negativity in
frontline at 15 mos ( EOT): 11/12 in PB, 5/7 in BM
• Umbralisib ( TGR-1202) is PI3K inhibitor with better safety profile.• Combination with ublituximab ( anti CD20) and ibrutinib in
relapsed CLL: 19/19 responses