Embed Size (px)
Citation preview

New treatments in the era of HCV infection
Maria Buti
Hospital Universitario Valle Hebron. Barcelona. Spain

Disclosures
I have received honoraria as a speaker or a member of a speaker bureau or as an advisor or consultant or have received grants for clinical research from:
• AbbVie, BMS, Gilead, Janssen, and MSD

Next-generation HCV treatments can offer several clear advantages compared with currently approved regimens
What characteristics are most desirable for next-generation HCV treatments?
Pan-genotypic (GT1–6)
Shorter treatment durations
Limited drug–drug interactions
Highly efficacious in most populations
including “difficult-to-treat” patients
High barrier to resistance
Convenient dosing with co-formulated
pills
RBV sparing

Next-generation drugs for HCV treatment
NS3/4AProtease inhibitor
NS5A
ABT-493
ABT-530
Velpatasvir
GS-9587
Elbasvir
Grazoprevir
NS5B polymerase
Sofosbuvir
MK-3682
MK-8408

ABT-493 (NS3/4A PI) + ABT-530 (NS5A inhibitor)

SURVEYOR-I + -II study overview
Poordad F, et al. Hepatology 2015; 62(Suppl):228A (oral presentation);Wyles DL, et al. Hepatology 2015; 62(Suppl):339A (oral presentation).
Phase 2 – SURVEYOR clinical study overview
Pan-genotypic
ABT-493 ABT-530
NS5A inhibitor
Pan-genotypic
NS3/4A protease inhibitor
SURVEYOR-II
SURVEYOR-IABT-493 + ABT-530
± RBV(8–12 weeks)
ABT-493 + ABT-530± RBV
GT1GT4, 5, or 6
(non-cirrhotic)
Cirrhotic or non-cirrhotic, treatment-naive or pegIFN/RBV null-responders
GT2 or GT3Cirrhotic or non-cirrhotic,
treatment-naive or pegIFN/RBV failures
Primary completion date:*
March 2016
Primary completion date:*
February 2016

SURVEYOR-I: High SVR rates in HCV GT1 non-cirrhotic, treatment-naive, or pegIFN/RBV null-responders (Part 1)
* 1 patient experienced a decrease in blood phosphorus considered to be related to the study drugs.Poordad F, et al. Hepatology 2015;
62(Suppl):228A (oral presentation).
SVR12
100 97
0
20
40
60
80
100
ABT-493 200 mg +ABT-530 120 mg
ABT-493 200 mg +ABT-530 40 mg
HCV GT1, treatment-naive, or pegIFN/RBV null-responder, non-cirrhotic patients received ABT-493 + ABT-530 for 12 weeks (N=79)
81% GT1a 37% pegIFN/RBV null-responders
12 weeks
100% treatment-experienced and 98% -naive patients achieved SVR12
All patients with baseline NS3 and/or NS5A variants achieved SVR12
1 patient reported an SAE (not related to study drug)
3 patients had severe AEs*
SVR
12
(%
)
4040
3839

SURVEYOR-I: HCV GT1, non-cirrhotic, treatment-naive, or pegIFN/RBV treatment-experienced (Part 2)
* Due to abdominal adenocarcinoma. Poordad F, et al. Hepatology 2015; 62(Suppl):1388A (poster presentation).
ABT-493 300 mg + ABT-530 120 mg
HCV GT1, treatment-naive, or pegIFN/RBV-experienced, non-cirrhotic patients received ABT-493 + ABT-530 for 8 weeks (N=34)
97% SVR12 with 8 weeks of treatment
All patients with baseline NS3 and/or NS5A variants achieved SVR12
1 patient discontinued at Week 4* (not related to study drugs)
100 97
0
20
40
60
80
100
SVR4 SVR12
3434
3334
8 weeks
SVR
(%
)
71% GT1a15% pegIFN/RBV
treatment-experienced

SURVEYOR-II: High SVR rates with ABT-493 + ABT-530 in non-cirrhotic, treatment-naive, and -experienced patients with HCV GT2 infection
* Atrial fibrillationLTFU = lost to follow up. Wyles DL, et al. Hepatology 2015; 62(Suppl):339A (oral presentation).
HCV GT2, treatment-naive, or pegIFN/RBV failures, non-cirrhotic patients received ABT-493 + ABT-530 ± RBV for 12 weeks (N=75)
96 100 100
0
20
40
60
80
100
300 mg+
120 mg
200 mg+
120 mg
200 mg+
120 mg+
RBV
SVR
12
(%
) HCV GT2
1 LTFU
2425
2424
2525
1 patient had an SAE
(not related to study drugs)
No virologic failures in 74 patients
All patients with baseline NS3 or NS5A variants achieved SVR12
ABT-493+
ABT-530

SURVEYOR-II: High SVR rates with ABT-493 + ABT-530 in non-cirrhotic, treatment-naive, and -experienced patients with HCV GT3 infection
*2 study drug-related severe AEs were reported: decreased hemoglobin (+ RBV); blood Creatinine phosphokinase increased (ABT-493 200 mg + ABT-530 40 mg arm).
Kwo P, et al. Hepatology 2015; 62(Suppl):337A (oral presentation).
ITT SVR12 rates
1 patient discontinued due to an AE
7 patients reported severe AEs*
ABT-493 (300 mg QD) and ABT-530 (120 mg QD) have been
selected for further studies
>90% SVR12 rates in
GT3-infected patients
HCV GT3, treatment-naive, or pegIFN/RBV failures, non-cirrhotic patients received ABT-493 + ABT-530 ± RBV for 12 weeks (N=121)
ABT-493+
ABT-530
93 93 94
82
0
20
40
60
80
100
300 mg+
120 mg
200 mg+
120 mg
200 mg+
120 mg+
RBV
200 mg+
40mg
SVR
12
(%
) HCV GT3
2830
2830
2931
2530

GZR/EBR + MK-3682or
GZR + MK-3682 + MK-8408

Phase 2 – Part A of C-CREST-1 & 2: GZR + MK-3682 (NS5B polymerase inhibitor) with either EBR or MK-8408 (NS5A inhibitor) in patients with HCV GT1, 2, or 3 infection
* 100% SVR12 with GZR/EBR + MK-3682 (300 mg or 450 mg) and GZR + MK8408 + MK3682 (300 mg).EBR = elbasvir; GZR = grazoprevir. Gane E, et al. Hepatology 2015; 62(Suppl):1389A (poster presentation).
HCV GT1-, 2-, or 3-infected patients treated for 8 weeks with GZR/EBR + MK-3682 or GZR + MK-8408 + MK-3682
SVR12 rates by regimen
GT1% (n/N)
GT2% (n/N)
GT3% (n/N)
GZR/EBR + MK-3682 (300 mg)
100 (23/23)
69 (11/16)
90 (19/21)
GZR/EBR + MK-3682 (450 mg)
100 (23/23)
60 (9/15)
86 (19/22)
GZR + MK-8408 + MK-3682 (300 mg)
100 (24/24)
71 (10/14)
95 (20/21)
GZR + MK-8408 + MK-3682 (450 mg)
91 (21/23)
94 (15/16)
91 (20/22)
Treatment-naive Non-cirrhotic
100% SVR12 with 8 weeks of treatment in
GT1-infected patients*
SVR12 100% (21/21) in GT1-infected patients with
baseline NS5A RAVs

Phase 2 – Part A of C-CREST-1 & 2: GZR + MK-3682 (NS5B polymerase inhibitor) with either EBR or MK-8408 (NS5A inhibitor) in patients with HCV GT1, 2, or 3 infection
EBR = elbasvir; GZR = grazoprevir. Gane E, et al. Hepatology 2015; 62(Suppl):1389A (poster presentation).
SVR12 rates by regimen
GT1% (n/N)
GT2% (n/N)
GT3% (n/N)
GZR/EBR + MK-3682 (300 mg)
100 (23/23)
69 (11/16)
90 (19/21)
GZR/EBR + MK-3682 (450 mg)
100 (23/23)
60 (9/15)
86 (19/22)
GZR + MK-8408 + MK-3682 (300 mg)
100 (24/24)
71 (10/14)
95 (20/21)
GZR + MK-8408 + MK-3682 (450 mg)
91 (21/23)
94 (15/16)
91 (20/22)
SVR12 94% (15/16) in GT2-infected patients with
GZR + MK-8408 + MK3682 (450 mg)
Treatment-naive Non-cirrhotic
94% of GT2-infected patients had baseline
NS5A RAVs
HCV GT1-, 2-, or 3-infected patients treated for 8 weeks with GZR/EBR + MK-3682 or GZR + MK-8408 + MK-3682

Phase 2 – Part A of C-CREST-1 & 2: GZR + MK-3682 (NS5B polymerase inhibitor) with either EBR or MK-8408 (NS5A inhibitor) in patients with HCV GT1, 2, or 3 infection
EBR = elbasvir; GZR = grazoprevir. Gane E, et al. Hepatology 2015; 62(Suppl):1389A (poster presentation).
SVR12 rates by regimen
GT1% (n/N)
GT2% (n/N)
GT3% (n/N)
GZR/EBR + MK-3682 (300 mg)
100 (23/23)
69 (11/16)
90 (19/21)
GZR/EBR + MK-3682 (450 mg)
100 (23/23)
60 (9/15)
86 (19/22)
GZR + MK-8408 + MK-3682 (300 mg)
100 (24/24)
71 (10/14)
95 (20/21)
GZR + MK-8408 + MK-3682 (450 mg)
91 (21/23)
94 (15/16)
91 (20/22)
>90% SVR12 in GT3-infected patients with
GZR + MK-8408 + MK3682 (300 or 450 mg)
Treatment-naive Non-cirrhotic
47% of GT3-infected patients had baseline
NS5A RAVs
HCV GT1-, 2-, or 3-infected patients treated for 8 weeks with GZR/EBR + MK-3682 or GZR + MK-8408 + MK-3682

Sofosbuvir/velpatasvir

99 99 100 100 97 100
0
20
40
60
80
100
Overall GT1 GT2 GT4 GT5 GT6
ASTRAL-1: SOF/VEL in HCV GT1, 2, 4, 5, or 6 in treatment-naive or -experienced patients with or without cirrhosis
VEL = velpatasvir (GS-5816).Feld JJ, et al. Hepatology 2015; 62(Suppl):1379A–1380A (abstract LB-2);
Feld JJ, et al. N Engl J Med 2015; ePub ahead of print].
HCV GT1-, 2-, 4-, or 6-infected patients were randomized to receive SOF/VEL (400 mg/100 mg) or placebo for 12 weeks; HCV GT5-infected patients received SOF/VEL (400 mg/100 mg) for 12 weeks
32% treatment experienced (includes pegIFN/RBV and PI + pegIFN/RBV failures)
19% compensated cirrhosis
2 GT1 patients relapsed, no GT2, 4, 5, or 6 patients relapsed
Frequency and severity of AEs and laboratory abnormalities were similar between SOF/VEL and placebo groups
741 patients enrolled at 81 sites in North America, Europe, and Hong Kong
SOF/VEL for 12 weeks
618624
nN
323328
104104
116116
3435
4141
Overall 99% SVR12
The presence of NS5A RAVs did not impact SVR12 (99% [255/257])
SVR
12
(%
)

ASTRAL-2: SOF/VEL or SOF + RBV for 12 weeks in HCV GT2-infected patients
VEL = velpatasvir (GS-5816); FDC = fixed dose combination.Sulkowski MS, et al. Hepatology 2015; 62(Suppl S1):313A (abstract 205);
Foster GR, et al. N Engl J Med 2015; ePub ahead of print.
1 patient (SOF/VEL) discontinued due to AEs
2 patients died; neither were related to study drugs
The incidence of AEs was lower in the SOV/VEL arm compared with SOF + RBV
15% treatment experienced (with an IFN-containing regimen)
14% compensated cirrhosis
Overall 99% SVR12 with SOF/VEL
The presence of NS5A RAVs did not impact SVR12 (100% [80/80])
269 HCV GT2-infected patients were randomized 1:1 to receive eitherSOF/VEL FDC for 12 weeks (n=134) or SOF + RBV for 12 weeks (n=132)
9994
0
20
40
60
80
100
SOF/VEL12 weeks
SOF + RBV12 weeks
SVR
12
(%
)
133134
nN
124132
6 relapses

ASTRAL-3: SOF/VEL (12 weeks) or SOF + RBV (24 weeks) in HCV GT3-infected patients
VEL = velpatasvir (GS-5816).Mangia A, et al. Hepatology 2015; 62(Suppl S1):338A–339A (abstract 249);
Foster GR, et al. N Engl J Med 2015; ePub ahead of print.
No patients (SOF/VEL) discontinued due to AEs
3 patients died; none were related to study drugs
SVR12 (89% [33/37]) in treatment-experienced, cirrhotic patients
SVR12 (88% [38/43]) in patients with baseline NS5A RAVs
26% treatment experienced(with an IFN-containing regimen)
30% compensated cirrhosis
552 HCV GT3-infected patients received eitherSOF/VEL FDC for 12 weeks (n=277) or SOF + RBV for 24 weeks (n=275)
The incidence of AEs was lower in the SOV/VEL arm compared with SOF + RBV
95
80
0
20
40
60
80
100
SOF/VEL12 weeks
SOF + RBV24 weeks
SVR
12
(%
)
264277
nN
221275

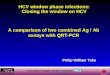
ASTRAL-4: SOF/VEL ± RBV in HCV GT1, -2, -3, -4, or -6 infected patients with decompensated cirrhosis
CP = Child Pugh; MELD = Model For End-Stage Liver Disease;VEL = velpatasvir (GS-5816). * Patients that had received treatment with any NS5A or N55B inhibitor were excluded.
Charlton E, et al. Hepatology 2015;62(Suppl):1387A (poster presentation);
Curry MP, et al. N Engl J Med 2015; ePub ahead of print.
55% treatment experienced(pegIFN/RBV or PI regimen*)
Median CP score 8 (range 5–10) MELD score range 6–24
No RBV RBVAmong patients who
achieved SVR, 47% and 51% had improvements in
CP and MELD scores86
92
75
50
100 100
Overall GT1 GT2 GT3 GT4 GT6
7790
6571
34
612
22
11
SOF/VEL 24 weeks
3.4% (9/267) discontinued due to AEs
9 deaths (all unrelated to SOF/VEL)
HCV GT1-, 2-, 3-, 4-, or 6-infected patients with CP B cirrhosis were randomized to receive SOF/VEL (400 mg/100 mg) for 12 weeks, SOF/VEL + RBV for 12 weeks, or SOF/VEL for 24 weeks
8388
100
50
10094 96
100
85
100
0
20
40
60
80
100
Overall GT1 GT2 GT3 GT4
7590
nN
8287
6068
6568
44
44
714
1113
44
22
SOF/VEL ± RBV 12 weeksSVR
12
(%
)

Summary
Despite the high cure rates observed with currently approved DAA regimens, research into improved
HCV treatments continues
Next-generation HCV treatments may offer several significant advantages compared with currently approved treatments
Efficacy against all HCV genotypes across all patient populations
Convenient co-formulations and reduced pill burdens
Reduced potential for DDIs
High barriers to resistance
Combination regimens in late-stage clinical development have shown high SVR rates across different genotypes, in cirrhotic and non-cirrhotic patients, and in both
treatment-naive and -experienced patients