Embed Size (px)
Citation preview

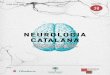
Figure e-1, related to Figure 1: The E276X ATAD1 variant is not located in a known functional domain, but substantially decreases ATAD1 expression.A: The functional domain structure of ATAD1-encoded Thorase. The ATPase function is mediated by the ATP-binding Walker A (WA) domain and ATP-hydrolysis Walker B (WB) domain (White and Lauring, 2007). An N-linker (NL) region transduces energy from ATP hydrolysis to the rest of the protein in order to perform work. Finally, there is a second region of homology (SRH) that is present in classically defined AAA proteins. The p.E276X variant was outside of these known domains. B: Results from quantitative PCR analysis of mRNA from lymphoblastoid cell lines. There is 78% reduction in ATAD1 mRNA expression in human p.E276X lymphocytes as compared to controls (p <0.05). C There is a reduced level of ATAD1-encoded Thorase protein by western blotting of cell lysates prepared from human p.E276X lymphocytes as compared to controls. Whole mouse brain Thorase levels are also shown as a positive control.
1

Figure e-2, related to Figure 3: Dose and age-dependent sedation, growth impairment and subsequent death can occur in perampanel-treated wild-type mice. A: The survival curve of wild-type mice treated with differing doses of perampanel from age P2 is shown. No survival difference was noted between the 0.5 mg/kg/day perampanel dose (red) and vehicle-treated mice (black). B: The average growth rate of mice undergoing no treatment, or treatment with vehicle or 0.5 mg/kg/day perampanel from age P2 (left) or P5 (right) is shown. Growth was significantly impaired in mice treated with perampanel from age P2 (n = 3, p < 0.001, two-way ANOVA with Sidak’s multiple comparison test) but not mice treated from P5. Therefore, a perampanel dose of 0.5 mg/kg/day starting from age P5 was chosen for further investigations.
2

Figure e-3, related to Figure 3: ATAD1-/- mice do not demonstrate differences in duration of time engaged in rearing activity or average speed.On behavioral analysis ATAD1-/- mice (red diamonds) did not differ from wild-type animals (black filled-in circles) in (A) total rearing activities or (B) average speed (6 animals per group). Two mice in the ATAD1-/- perampanel and phenobarbital-treated groups seized during this observation. The seizures were characterized by high-speed involuntary movements, therefore they are shown in the figure (symbol surrounded by a black circle), but they are not included in the statistical analysis. One-way ANOVA with Tukey post-hoc test was performed, and a multiplicy-adjusted p value was calculated. For both panels and all comparisions p > 0.05.
3

Figure e-4, related to Figure 4: Perampanel therapy dose response curve A: Perampanel dosing protocol (solid line) used in patient IV-6 and resultant functional status score (dashed line). A functional status score of 6 represents normal functioning, while a score of 30 represents maximal impairment (Pollack et al., 2009). B: Clinical improvements observed in patient IV-6. Onset of the solid black bar corresponds to the day of therapy (as delineated on the x-axis of panel B) that a behavior was first observed. For example, improved tone was first noted on day 8 of therapy and continued throughout the therapeutic trial. Patient IV-6 attained new basic neurologic functions in a dose-dependent manner. Improvement in functional status plateaued at a perampanel dose of roughly 0.4-0.6 mg/kg/day. C: Perampanel dosing protocol (solid line) used in patient IV-3 and resultant functional status score (dashed line). D: Clinical improvements and deterioration seen in patient IV-3.
4

Figure e-5, related to Figure 4: Plasma concentrations of perampanel Perampanel was given as a daily dose, and plasma concentrations during chronic therapy were obtained (patient IV-6 green squares, patient IV-3 purple circles). Levels were drawn at times as indicated on the x-axis above and plotted against normative levels provided by the drug manufacturer. The patients routinely had serum concentrations greater than the 50th percentile. Norms were provided from adolescent patients given standard dosing of 12mg daily.
5

Table e-1: Percentage of homozygosity identified in subjects by genome wide array
Individual% homozygosity of autosome
(includes regions >=3Mb)III-1 0III-2 0III-3 0.31III-4 4.24IV-1 4.61IV-2 1.69IV-3 5.21IV-4 6.27IV-5 2.97IV-6 2.77IV-7 5.39
6

Table e-2: Exome sequencing coverage of all genes found in the shared region of homozygosity found in all affected individuals (chr10:83,619,940-90,095,915, hg19 coordinates)
Gene name Transcript ID Number of exons
% of genes covered at >=20X
Number of exons covered at <20X
NRG3 NM_001010848.3 9 100 0NRG3 NM_001165972.1 9 100 0NRG3 NM_001165973.1 11 100 0RGR NM_001012720.1 7 100 0RGR NM_001012722.1 6 100 0RGR NM_002921.3 7 100 0
CCSER2 NM_001284240.1 9 100 0CCSER2 NM_001284241.1 2 100 0CCSER2 NM_001284242.1 6 100 0CCSER2 NM_001284243.1 7 100 0CCSER2 NM_018999.3 10 100 0WAPAL NM_015045.2 18 100 0LDB3 NM_001080115.1 7 100 0LDB3 NM_001080116.1 8 100 0LDB3 NM_001171611.1 8 100 0
MMRN2 NM_024756.2 7 100 0SNCG NM_003087.2 5 100 0ADIRF NM_006829.2 3 100 0
PAPSS2 NM_001015880.1 13 100 0MINPP1 NM_001178117.1 3 100 0MINPP1 NM_001178118.1 5 100 0MINPP1 NM_004897.4 5 100 0
PTEN NM_000314.4 9 100 0KLLN NM_001126049.1 1 100 0RNLS NM_001031709.2 7 100 0RNLS NM_018363.3 7 100 0
CDHR1 NM_001171971.2 17 94.12 1CDHR1 NM_033100.3 17 94.12 1GRID1 NM_017551.2 16 93.75 1LDB3 NM_001080114.1 13 92.31 1LDB3 NM_001171610.1 13 92.31 1LDB3 NM_007078.2 13 92.31 1
ATAD1 NM_032810.2 9 88.89 1GHITM NM_014394.2 8 87.5 1OPN4 NM_001030015.2 11 81.82 2
BMPR1A NM_004329.2 11 81.82 2LRIT2 NM_001284223.1 4 75 1LRIT2 NM_001017924.3 3 66.67 1
GLUD1 NM_005271.3 13 61.54 5LRIT1 NM_015613.2 4 50 2
AGAP11 NM_133447.1 4 50 2FAM35A NM_019054.2 7 42.86 4NUTM2A NM_001099338.1 7 0 7FAM25A NM_001146157.2 3 0 3
7

Table e-3: Known disease-associated genes contained in the shared region of homozygosity found in all affected individuals (chr10:83,619,940-90,095,915, hg19 coordinates)
Gene Gene Name OMIM Disorders OMIM Phenotypes
CDHR1 Cadherin-related family, member 1 609502 Cone-rod dystrophy 15,
Retinitis Pigmentosa 65 613660
RGR Retinal G protein coupled receptor 600342 Retinitis pigmentosa 44 613769
LIM LIM domain binding 3 605906Dilated cardiomyopathy 1C,
Hyertrophic cardiomyopathy 24,Left ventricular noncompaction 3
601493
BMPR1A Bone morphogenetic protein receptor, type IA 601299 Polyposis syndrome, juvenile and infantile forms 174900, 610069
GLUD1 Glutamate dehydrogenase-1 138130 Hyperinsulinism-hyperammonemia syndrome 606762
MINPP1Multiple inositol polyphosphate phosphatase 1
605391 Thyroid carcinoma, follicular 188470
PAPSS23'-phosphoadenosine 5'-
phosphosulfate synthase 2
603005 Brachyolmia 4 612847
KLLN Killin 612105 Cowden syndrome 4 615107
PTEN Phosphatase and tensin homolog 601728
Cowden syndrome 1,Bannayan-Riley-Ruvalcaba syndrome,
Macrcocephaly/autism, etc.
153480, 158350, 605309, etc.
LIPN Lipase family, member N 613924 Ichthyosis, congenital, autosomal recessive 8 613943
ACTA2 Actin, alpha-2, smooth muscle, aorta 102620
Familial aortic aneurysm,moyamoya disease 5,
multisystemic smooth muscle dysfunction syndrome
611788, 614042, 613834
FAS Fas cell surface death receptor 134637 Autoimmune lymphoproliferative syndrome IA,
burn-scar related squamous cell carcinoma 601859
LIPA Lipase A, lysosomal acid, cholesterol esterase 613497 Cholesterol ester storage disease, Wolman disease 278000
SLC16A12 Solute carrier family 16, member 12 611910 Cataract, juvenile, with microcornea and glucosuria 612018
8

Table e-4: LOD scores calculated using a multipoint genetic linkage analysis of eight SNPs in the region of ATAD1
Marker Distance (cM) LOD scorers791881 89.191 3.7241rs941830 89.24 3.725
rs2038554 89.317 3.7256rs1234219 89.432 3.7259
kgp1166559 89.492 3.7259rs11202607 89.51 3.7259rs4603211 89.603 3.7228rs2184697 89.635 3.7215
9

SUPPLEMENTARY EXPERIMENTAL PROCEDURESClinical genetic testing:Lymphocyte DNA was extracted from both patients and all available family members. Clinical single nucleotide polymorphism (SNP) microarray analysis (CHOP, Philadelphia PA, Illumina CRC BeadChip) was used to evaluate for aneuploidy and regions of homozygosity (ROH) in individuals III1-4 and IV1-7. Clinical exome sequencing (GeneDx, Gaithersburg MD, and CHOP) of the patient IV-6, his unaffected parents and older brother was completed. Comparison of shared regions of ROH was used to evaluate variants identified by whole exome sequencing.
Clinical molecular testing of the nonsense variant c.826G>T (p.E276X) in the ATAD1 gene, was completed in all available samples (CHOP). Genomic DNA was extracted from peripheral blood using an automated DNA extractor or a commercially available kit (QIAGEN) according to manufacturer's instructions. Exon 8 of the ATAD1 gene was amplified by polymerase chain reaction. DNA sequencing was performed using a commercially available kit (ABI) with di-deoxy terminators. Sequences were analyzed on an automated DNA sequencer (ABI) and compared to control sequences. Nucleotides are numbered starting with the first base of the initiator methionine. To assess ATAD1 expression levels, RNA was extracted from a lymphoblastoid cell lines obtained from patient IV-6 and converted to cDNA by random priming (Life Technologies). Real-time PCR was performed to determine the expression of ATAD1 relative to GAPDH (Life Technologies). ATAD1-encoded Thorase protein levels were also assessed in cell lysates prepared from the cell line obtained from patient IV-6. Western blots analysis was completed as previously described with a primary antibody directed against ATAD1 (NeuroMab clone N125/10, Davis, CA) (Zhang et al., 2011) at a concentration of 1:100. A primary antibody directed against actin (Sigma A2066, St. Louis, MO) at a concentration of 1:100-1:200 was used as a loading control.
Linkage Analysis:Phenotypes were specified a priori. Direct LOD scores were calculated using the ATAD1 p.E276X mutation using the method described in the recent publication of Ott et al. (Ott et al., 2015). For multipoint marker analysis of the SNP data we employed the Superlink-Online SNP tool (http://cbl-hapw.cs.technion.ac.il/superlink-snp). This is a previously published, publically available web-based program that uses massively parallel computing to run an algorithm optimized to extract meaningful linkage data from SNP array results (Silberstein et al., 2013). For the algorithm, an eight marker window which covered the region including and surrounding the ATAD1 gene was chosen. Markers spanned the region of chromosome 10 from 89,407,996-89,851,565 (Table e-4). ATAD1 is located at chr10:89,512,875-89,577,917.
Mouse behavior and survival:ATAD1-/- C57BL/6 knockout mice and wild type littermates were obtained by mating heterozygous mice as previously reported (Zhang et al., 2011). Littermates were compared in all experiments. Mouse behavioral testing occurred in the Johns Hopkins University School of Medicine Behavior Core using approved protocols. All behavioral experiments were done at P19-P20, which is considered equivalent to the juvenile human(Markowitz et al., 2010). Both male and female mice were used. Pups were kept in their home cages during experiments and separated from parents at P40-42.
Perampanel was synthesized and provided by Eisai Co., Ltd. (Tokyo, Japan). Phenobarbital, sodium salt, was purchased from Sigma-Aldrich Co. (St. Louis, MO, U.S.A.). Perampanel was reconstituted to 0.4 mg/ml in sterile 0.1 M HCl in saline as previously described (Hanada et al., 2011), and phenobarbital to 40 mg/ml in sterile saline. Littermates were randomly assigned to receive vehicle (sterile 0.1M HCl in saline) or drug in equal volumes.
For injections, mice were carefully removed from home cages (with minimum potential discomfort), weighed, given drugs, and placed in an observation cage. All treated mice were warmed under a heat lamp during experimental procedures to maintain body temperature and were visually monitored for injury and seizure activity before returning them back to their home cages. Starting at age 5 days (P5), ATAD1-/- and ATAD1+/+ mice were injected intraperitoneally in parallel with perampanel (0.5 mg/kg), phenobarbital (50mg/kg) (Markowitz et al., 2010) or vehicle daily. Drugs were administered at the same time (16:00-17:00 EST) every 24 hours. The dose for perampanel was increased to 0.75 mg/kg at P15. Dosages were optimized to minimize sedative effects while maximizing response (Figure e-2 ).
10

Sedation is a known side effect of perampanel therapy. A postnatal day 20 (P20) ATAD1-/- mouse treated with 1.0 mg/kg perampanel experienced more severe and prolonged sedation than a wild-type littermate. Furthermore, the ATAD1-/- mouse that began therapy at P20 died within a few days (i.e. within a similar timeframe as untreated mice).
In order to identify a well-tolerated dose of perampanel that could be used in further survival experiments, wild-type P2 mice were treated in parallel with different doses of perampanel (0.5, 1.0, 2.0, 5.0 mg/kg) or vehicle. Sedation recovery times for the 1.0, 2.0 and 5.0 mg/kg perampanel doses were 3-4, 6-7, and >8 hours, respectively. This sedation led to early dose-dependent death (Figure e-2A). Mice treated with 0.5mg/kg experienced less sedation and had similar survival to vehicle-treated mice. However, initiation of the 0.5 mg/kg dose at P2 resulted in slower growth rates. If perampanel initiation was delayed until P5, there was no difference in average growth rate between perampanel and vehicle-treated pups (Figure e-2B). Wild-type mice also tolerated an escalation of the perampanel dose to 0.75 mg/kg at P15. This mimics the slow escalation in dosing that was completed in the human ATAD1 patients. Therefore, the standard dosing protocol used in this study was initiation of perampanel therapy on day P5 at 0.5 mg/kg/day with an increase to 0.75 mg/kg/day at P15.
Novelty induced activity and general locomotor activity were measured in the open field test as previously described (Crawley, 2004). Horizontal and vertical movements where tracked by infrared beams using the PAS Open Field System (San Diego Instruments, San Diego, CA). Beam breaks occurring 4 cm from any wall was considered activity in the periphery, while breaks in the rest of the chamber was considered central activity. Vertical motion was used as a measure of rearing activity. Locomotor activity was tested and measured as previously described (Pletnikov et al., 2008). Horizontal and vertical beam breaks during the test were counted by the PAS Open Field System and converted to distance traveled and speed using the PAS Reporter (San Diego Instruments, San Diego, CA) software. The resting time (period without any activity) was also measured.
To obtain brain tissue, mice were anesthetized with sodium pentobarbital and then transcardially perfused with 4% paraformaldehyde (PFA) in PBS (phosphate buffer, pH 7.4). The brain was then removed and post fixation was performed in 4% PFA in PBS overnight, followed by cryoprotection by immersion in PBS containing 4% sucrose and 0.01% sodium azide for 48 hours.
Mouse ex-vivo brain MRI:Prior to the MRI the samples were immersed for at least 24h in a PBS 1X solution containing 0.2mM GdDTPA. At the time of scanning the samples were removed from the PBS/GdDTPA solution, rinsed with pure PBS and introduced in a short 11 mm glass tube containing Fomblin to provide a susceptibility match and a black background for the images. Bubbles were carefully removed by tapping gently on the tube. An inverted Pasteur pipette was inserted on top of the brain to maintain the tissue immersed in the Fomblin. MRI was performed at 9.4T in a vertical bore magnet (Avance III Bruker-Biospin Inc) using the micro 2.5 self-shielded gradients (2.5G/cm/A) and a 15 mm RF coil. The image acquisition and reconstruction was performed with the Paravision software 5.1 (Bruker Biospin Inc.). Imaging was performed at room temperature. T2 weighted 3D images of the brain tissue were obtained with the 3D turboRARE Bruker protocol and the following parameters: FOV 19.2 x 12.8 x 9.6 mm, SI 256 x 176 x 128, giving an isotropic resolution of 75 μ6 NEX, TR 1500 ms, Te 17 ms, echo train 8 which results in an effective echo time TE of 51 ms and a 6 hour long experiment. Three mice were imaged for each condition (ATAD1+/+, ATAD1-/-, perampanel treated-ATAD1-/-).
Coronal MRI images were analyzed using Osirix imaging software (Pixmeo). For volume measurements equivalent regions were identified across mice and volumes were calculated over serial sections. For example, cortical measurements were made by first identifying the most rostral slice containing the olfactory limb of the anterior commissure. A region of interest (ROI) containing the entire right hemicortex was delineated for every third slice for 30 consecutive images caudal to this initial image. The ROI for the remaining slices was then interpolated and a 3D volume was calculated. Volumes were then normalized to the mean volume of the anatomical region in ATAD1 +/+ mice. In order to investigate mutation-induced differences in T2-signal intensity, mean intensities of the ROIs described above were obtained. In order to compare images from different subjects, intensities were scaled to normalize the mean maximum signal intensity for each condition. This was necessary as the imaging was ex vivo so normalization to typical landmarks such as bone or CSF was not possible.
Human perampanel studies: Both patients were treated with the selective non-competitive AMPAR antagonist, perampanel (Fyompa, Eisai). Perampanel is FDA- approved for treatment of adults with partial onset seizures. Given the patients’ low body weight, both were started on perampanel suspension (rather than tablets). The sample size of two subjects was
11

selected due to subject availability. Perampanel has a long half-life that ranges from 24-105 hours, depending on the presence of other inducer medications (Krauss, 2013); therefore, the patients underwent a slow up-titration of the medication (Figure e-4). Drug levels, neurological exam, EEG and development were monitored. Patient IV-6 weighed 11.3 kg at discharge and was maintained on a perampanel dose of 8mg daily (0.7 mg/kg/day). Patient IV-3 weighed 7.3 kg at discharge and was maintained on a perampanel dose of 8mg daily (1.1 mg/kg/day).
Functional status measurement on perampanel:Improvement was measured by the Functional Status Score, a validated pediatric outcome measurement (Pollack et al., 2009). This outcome assesses six functional domains (mental status, sensory, communication, motor, feeding, and respiratory function) each on a scale from 1 (normal) to 5 (severely impaired) and a composite score is calculated. Fully functioning children receive score of 6, while maximal impairment is assigned a score of 30. Scores were retrospectively assigned by a single scorer on the basis of physical examination documentation from daily progress notes in the electronic medical record.
12

SUPPLEMENTARY CASE REPORT INFORMATION: The proband (Figure 1, IV-6) was a nine-month old male with a history of hypertonia, seizures and respiratory failure, presenting from Kuwait for further evaluation. He was hypertonic at birth. His hypertonia progressed and seizures developed in the first weeks of life. He was intubated and required tracheostomy for respiratory failure. Several anti-epileptic drugs (AEDs) and muscle relaxants were initiated, including phenobarbital, diazepam, topiramate, and baclofen without impact on his neurological symptoms.
Physical exam at nine months showed a non-dysmorphic, sedated child with extreme hypertonia, contractures of all extremities, and no spontaneous movement. He had minimally reactive pupils and absent gag and corneal reflexes. He did not withdraw to painful stimuli and was hyperreflexic throughout with substantial clonus.
Extensive evaluation completed in Kuwait was unrevealing (Table 1). Prior electroencephalography (EEG) demonstrated seizure activity. On arrival to our center, despite treatment with multiple AEDs, the patient’s repeat EEG showed hypsarrhythmia, a chaotic interictal pattern suggestive of severe brain dysfunction. Brain MRI at two weeks of life was normal, but a repeat at nine months showed marked interval reduction in cerebral volume, especially affecting the brainstem. There was also interval dilatation of the ventricular system reflecting a combination of cerebral volume loss and alterations in CSF dynamics. Given the lack of diagnosis, clinical WES of multiple family members in conjunction with SNP microarray analysis was completed.
The patient was the product of a highly consanguineous family (Figure 1). His sister died at two years from respiratory failure secondary to her hypertonia. She had an extensive, unrevealing evaluation. Three other first cousins with similar features died by age of 6 months.
The second patient was a two-month old male cousin of the proband (individual IV-3, Figure 1). He was also severely hypertonic at birth. His two siblings had early seizures died by age three months. He developed clinical seizures in the first few days of life and was started on phenobarbital. Initial exam at our center at two and a half months of age demonstrated a non-dysmorphic, hypertonic infant with spontaneous respirations not requiring intubation. He was awake and alert with reactive pupils. He blinked to light but not threat. He had little spontaneous movement and tonic extension of all four extremities. When his foot was lifted off of the examination table, he maintained full body extension and would pivot on his occiput. He would vocalize to painful stimuli, but could not withdraw due to his hypertonia. He did not have clonus or hyperreflexia. EEG at presentation while on phenobarbital demonstrated no seizure activity but an abnormal background. Brain MRI was unremarkable (Figure 4). SNP microarray analysis was completed on this patient, his unaffected siblings, and his parents.
Exome sequencing and copy number variants:Exome sequencing of the proband, his parents, and unaffected brother was completed by two clinical laboratories (GeneDx, Gaithersburg, Maryland and CHOP, Philadelphia, PA). Both laboratories identified the p.E276X ATAD1variant as a variant of unknown significance. The variant is absent from controls in multiple databases including the Exome Variant Server (http://evs.gs.washington.edu/EVS), the 1000 Genomes Project (http://browser.1000genomes.org), and the Exome Aggregation Consortium (http://exac.broadinstitute.org/).
One of the clinical laboratories also identified compound heterozygote variants of unknown significance (VUS) in SZT2 (p.R2767H / p.P2844L). These variants were inherited in trans from each unaffected parent. Homozygous mutations in SZT2 have been reported to early infantile epileptic encephalopathy type 18 (OMIM #615476) (Basel-Vanagaite et al., 2013). Several features of our patients did not match this phenotype. Specifically, the two previously reported patients had facial dysmorphisms including a high forehead, downslanting palpebral fissures, ptosis, and arched, laterally extended eyebrows that were not present in our patients. All of the previously reported patients had brain MRI findings of a short, thick corpus callosum and persistent cavus septum pellucidum. Most notably, patient with SZT2 mutations demonstrated profound hypotonia, while very pronounced hypertonia was seen in our patients.
The p.R2767H SZT2 variant has not been previously reported to cause disease. The variant is present in 0.018% of healthy controls in the Exome Aggregation Consortium database (http://exac.broadinstitute.org/). The variant leads to a nonsynonymous substitution of arginine to a histadine at a residue that is conserved in mammals; both amino acids are basic. It is predicted to be tolerated by SIFT and mutation-causing by MutationTaser.
The p.P2844L SZT2 variant has also not been reported to cause disease. The variant is present at 0.1% of individuals in the Exome Aggregation Consortium database. The variant leads to a nonsynonymous substitution of proline to a leucine at a residue that is conserved in mammals; both amino acids are hydrophobic. It is predicted to be tolerated by SIFT and a polymorphism by MutationTaser.
13

Given that the SZT2 phenotype did not fit our patient’s clinical picture, and the ambiguous evidence regarding the variant’s pathogenicity, we decided this was not the likely etiology of his symptoms.
Patient IV-6 also had a de novo 1.25Mb duplication of 17p13.3 (ish dup(17)(p13.3p13.3)(G248P800863G5++).arr[hg19] 17p13.3(1,007,540-2,255,351)x3 dn) identified by microarray and confirmed by fluorescence in situ hybridization that was not present in any other affected family members. This duplication contains more than 25 genes including YWHAE (OMIM # 605066), HIC1 (OMIM # 603825), PRPF8 (OMIM # 607300) and SERPINF1 (OMIM # 172860). Overlapping duplications have been reported with variable phenotypes including mild dysmorphic features, learning disability, hypotonia, autism spectrum disorder and mild brain abnormalities (Curry et al., 2013). Given the extreme hypertonia seen in individual IV-6 we did not feel this could fully explain his phenotype. Furthermore it was not present in affected individuals IV-3 or IV-5 who both had very similar clinical presentations to patient IV-6.
Expanded details of perampanel response in humans:Perampanel therapy was initiated in the patient IV-6 at 16 months of age. Prior to therapy he was hypertonic with absent corneal, pupil, and gag reflexes. He required ventilator support to initiate and support all breaths. He also had a very abnormal brain MRI (Figure 4A) and EEG; therefore, we did not anticipate a full recovery of function. However, any improvement in function could indicate perampanel’s utility for future affected family members. We hypothesize that early initiation of therapy, ideally from birth, may prevent the structural and functional deterioration seen in the proband.
Within the first 10 days of perampanel therapy his tone improved and he developed pupillary response to light. Over a three-month period, a dose-dependent improvement in his neurologic status was observed (Figure 4C, Figure e-4). His status was measured by the Functional Status Score, a validated pediatric outcome measurement (Pollack et al., 2009). This outcome assesses six functional domains (mental status, sensory, communication, motor, feeding, and respiratory function) each on a scale from 1 (normal) to 5 (severely impaired) and a composite score is calculated. Fully functioning children receive score of 6, while maximal impairment is assigned a score of 30. Over the course of therapy patient IV-6 score improved from 29 to 24.
His EEG also improved and no longer showed hypsarrhythmia by 60 days of therapy (a perampanel dose of 4mg/kg/day). All non-perampanel anti-epileptic medications including topiramate, phenobarbital and diazepam were weaned, and he continued to be free from clinical or electrographic seizures.
Repeat brain MRI 21 months of age (5 months after starting perampanel) showed worsening cerebral volume loss and hydrocephalus (Figure 4A). It is unclear if earlier initiation of therapy could have prevented progression of structural brain damage. Endoscopic third ventriculostomy was completed for his worsening hydrocephalus. His enlargement in head circumference began months prior to starting perampanel and therefore was unlikely to be an adverse effect of the medication.
Patient IV-3 began therapy at two and a half months of age. His starting functional status score of 19 was substantially better than his cousin’s score of 29 (Figure e-4). He had improvement in tone and increased spontaneous movement by 1 week of therapy. He also had normalization of his EEG. However, at age 3 months he had worsening of his respiratory status due to chest wall rigidity and required intubation and subsequent tracheostomy. All previous affected relatives had similar respiratory decompensation at approximately the same age. It is unclear if earlier initiation of therapy would have prevented this outcome. Despite the need for respiratory support, by six months of age patient IV-3 had functional status score of 23 and continued to have markedly better neurologic function as compared to family reports of relatives and patient IV-6’s initial, untreated exam at nine months which showed a functional status score of 29. Notably, he has all brain stem reflexes, sleep/wake cycles, the ability to withdraw and vocalize to pain, and spontaneous movements of all extremities. Also, his phenobarbital was weaned as his dose of perampanel increased. Repeat brain MRI at five and a half (data not shown) and nine months of age (Figure 4B) did not demonstrate any parenchymal volume loss while on perampanel. This contrasts to his cousins MRI at 9 months with substantial volume loss and developing hydrocephalus (Figure 4A).
Sedation and mood changes are the major reported side effects of perampanel. Given our patients’ limited neurologic function and artificial airway, these were not of major concern. Drug concentrations were measured and compared to normative values provided by Eisai (Figure e-5). Both patients always demonstrated serum drug levels that were higher than the 50th percentile.
14

Supplementary References:
Basel-Vanagaite, L., Hershkovitz, T., Heyman, E., Raspall-Chaure, M., Kakar, N., Smirin-Yosef, P., Vila-Pueyo, M., Kornreich, L., Thiele, H., Bode, H., et al. (2013). Biallelic SZT2 mutations cause infantile encephalopathy with epilepsy and dysmorphic corpus callosum. Am. J. Hum. Genet. 93, 524–529.
Crawley, J.N. (2004). Designing mouse behavioral tasks relevant to autistic-like behaviors. Ment Retard Dev Disabil Res Rev 10, 248–258.
Curry, C.J., Rosenfeld, J.A., Grant, E., Gripp, K.W., Anderson, C., Aylsworth, A.S., Saad, T.B., Chizhikov, V.V., Dybose, G., Fagerberg, C., et al. (2013). The duplication 17p13.3 phenotype: analysis of 21 families delineates developmental, behavioral and brain abnormalities, and rare variant phenotypes. Am J Med Genet A 161A, 1833–1852.
Hanada, T., Hashizume, Y., Tokuhara, N., Takenaka, O., Kohmura, N., Ogasawara, A., Hatakeyama, S., Ohgoh, M., Ueno, M., and Nishizawa, Y. (2011). Perampanel: a novel, orally active, noncompetitive AMPA-receptor antagonist that reduces seizure activity in rodent models of epilepsy. Epilepsia 52, 1331–1340.
Krauss, G.L. (2013). Perampanel: a selective AMPA antagonist for treating seizures. Epilepsy Curr 13, 269–272.
Markowitz, G.J., Kadam, S.D., Boothe, D.M., Irving, N.D., and Comi, A.M. (2010). The pharmacokinetics of commonly used antiepileptic drugs in immature CD1 mice. Neuroreport 21, 452–456.
Ott, J., Wang, J., and Leal, S.M. (2015). Genetic linkage analysis in the age of whole-genome sequencing. Nature Publishing Group 16, 275–284.
Pletnikov, M.V., Ayhan, Y., Nikolskaia, O., Xu, Y., Ovanesov, M.V., Huang, H., Mori, S., Moran, T.H., and Ross, C.A. (2008). Inducible expression of mutant human DISC1 in mice is associated with brain and behavioral abnormalities reminiscent of schizophrenia. Mol. Psychiatry 13, 173–86–115.
Pollack, M.M., Holubkov, R., Glass, P., Dean, J.M., Meert, K.L., Zimmerman, J., Anand, K.J.S., Carcillo, J., Newth, C.J.L., Harrison, R., et al. (2009). Functional Status Scale: New Pediatric Outcome Measure. Pediatrics 124, e18–e28.
Silberstein, M., Weissbrod, O., Otten, L., Tzemach, A., Anisenia, A., Shtark, O., Tuberg, D., Galfrin, E., Gannon, I., Shalata, A., et al. (2013). A system for exact and approximate genetic linkage analysis of SNP data in large pedigrees. Bioinformatics 29, 197–205.
White, S.R., and Lauring, B. (2007). AAA+ ATPases: achieving diversity of function with conserved machinery. Traffic 8, 1657–1667.
Zhang, J., Wang, Y., Chi, Z., Keuss, M.J., Pai, Y.-M.E., Kang, H.C., Shin, J.-H., Bugayenko, A., Wang, H., Xiong, Y., et al. (2011). The AAA+ ATPase Thorase regulates AMPA receptor-dependent synaptic plasticity and behavior. Cell 145, 284–299.
15