Embed Size (px)
Citation preview

1
NIAGARA REGION HEALTH SERVICES RESTRUCTURING REPORT
March 4, 1999
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
i
TABLE OF CONTENTS INTRODUCTION 1
BACKGROUND ................................................................................................................................................ 1 REPRESENTATIONS TO THE HSRC ................................................................................................................... 3 OVERVIEW OF THE REPORT ............................................................................................................................. 4
SECTION I: PLANNING ASSUMPTIONS 5 POPULATION PROJECTIONS.............................................................................................................................. 5 SITE CAPACITY ............................................................................................................................................... 5 AMBULATORY CARE ACTIVITY ....................................................................................................................... 6 GROWTH IN EMERGENCY SERVICES................................................................................................................. 7 PHYSICIAN SHORTAGES .................................................................................................................................. 7 SPECIALIZED SERVICES ................................................................................................................................... 8 LONG-TERM CARE BED ALLOCATIONS...........................................................................................................10
SECTION II: SITING OF CLINICAL SERVICES IN NIAGARA 11 PRINCIPAL ISSUES IN THE REPRESENTATIONS..................................................................................................11 THE HSRC’S DELIBERATIONS ........................................................................................................................11 SUMMARY OF SITING DECISIONS ....................................................................................................................19 DEVELOPMENT OF THE HÔTEL DIEU SITE AS AN AMBULATORY CARE CENTRE AND LONG-TERM MENTAL HEALTH PAVILLION .....................................................................................................................................................19
SECTION III: GOVERNANCE OF NIAGARA REGION HOSPITALS 23 PRINCIPAL ISSUES IN THE REPRESENTATIONS..................................................................................................23 THE HSRC’S DELIBERATIONS ........................................................................................................................23 LABORATORY SERVICES ................................................................................................................................29
SECTION IV: OTHER ISSUES 30 COORDINATION OF MENTAL HEALTH SERVICES .............................................................................................30 FRENCH LANGUAGE SERVICES .......................................................................................................................30 RURAL AND NORTHERN HEALTH CARE FRAMEWORK .....................................................................................30 CURRENT AND PROPOSED ACADEMIC ACTIVITIES IN ST. CATHARINES ............................................................31
SECTION V: SAVINGS AND REINVESTMENTS 32 PRINCIPAL ISSUES IN THE REPRESENTATIONS..................................................................................................32 THE HSRC’S DELIBERATIONS ........................................................................................................................32 CAPITAL REINVESTMENT ...............................................................................................................................32 REINVESTMENTS IN OTHER SERVICES.............................................................................................................33 SUMMARY OF REQUIRED REINVESTMENT .......................................................................................................35 ESTIMATED OPERATING SAVINGS FROM RESTRUCTURING...............................................................................36 OPERATING DEBT ..........................................................................................................................................36
SECTION VI: SUMMARY OF DIRECTIONS 38 SITING OF CLINICAL ACTIVITY ......................................................................................................................38 SUMMARY OF CLINICAL SERVICE CHANGES ...................................................................................................40 COSTS AND SAVINGS......................................................................................................................................40 REINVESTMENT .............................................................................................................................................41 GOVERNANCE AND MANAGEMENT.................................................................................................................41 HUMAN RESOURCES IMPACT ..........................................................................................................................42 SUMMARY OF NIAGARA REGION’S HOSPITALS’ ROLES ...................................................................................42 CONCLUSION .................................................................................................................................................43
APPENDIX 1: CAPITAL ESTIMATES 45
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
1
INTRODUCTION Background This is the second report issued for the Niagara Region by the Health Services Restructuring Commission (HSRC). It includes the HSRC's directions for hospital restructuring in Niagara Region following the Notices of Intention issued on October 27, 1998.1 The HSRC has made changes as a result of new information obtained and responses received from the community. This report should be read in conjunction with the HSRC's first Niagara Region restructuring report. The HSRC makes decisions about hospital restructuring and advises the Minister of Health on restructuring other aspects of Ontario's health services system. The HSRC's four-year mandate consists of three specific and closely related components: • to work with communities and
district health councils, and make decisions about restructuring hospitals to make them more effective and efficient;
• to make recommendations to the Minister of Health about which health services will require funding reinvestment as a result of changes to the hospital system and changing needs of the population; and
• to make recommendations to the Minister on restructuring other components of the health care system to improve overall quality of care, outcomes and efficiency.
The HSRC's approach to restructuring in Niagara Region is consistent with that in every other community reviewed. Factors relating to the delivery of health services are analyzed, the particular characteristics of the community and the future needs of the population are assessed, and decisions are made about the most appropriate mix of health services, their location and their governance.
1Niagara Region Health Services Restructuring Report and Notices of Intention to Issue Directions and Advice For the Niagara Region Health Services Restructuring Report, October 1998.
Highlights of the October 1998 Report: • Provide notice of intention to direct St. Catharines General,
Greater Niagara General, Niagara-on-the-Lake, Shaver, Niagara Rehabilitation, Welland County, Port Colborne General and Douglas Memorial hospital boards to amalgamate to become the Niagara Health Care System
• Standing Committees to be established for the rural hospitals in Niagara-on-the-Lake, Port Colborne, Fort Erie and the amalgamated Shaver/Niagara Rehabilitation Centre
• West Lincoln Memorial Hospital will continue to be linked with Hamilton Health Sciences Corporation through its management contract.
• Transfer long-term mental health beds for Niagara residents from Hamilton to St. Catharines.
• In St. Catharines, consolidate all acute inpatient and outpatient services including emergency services at the St. Catharines General Hospital site.
• Hôtel Dieu site in St. Catharines to cease as a public hospital.
• The Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines to manage long-term mental health services of the Niagara health Care System.
• Maple Hurst Private Hospital to close. • Provide regional rehabilitation beds and transition-to-
independent-living places for Niagara residents in Hamilton
• Savings of $28.7 million of operating expenses.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
2
The HSRC used as its starting point the hospital restructuring project that the Niagara District Health Council (NDHC) completed in December 1996. The NDHC strongly supported a significant, planned reconfiguration of hospital services in Niagara. Both the NDHC and hospital providers have called for decisions on hospital restructuring to be made as quickly as possible. The HSRC acknowledges the urgency of the task. The HSRC believes that its directions will form the basis for a sustainable health services delivery model. This model will be characterized by a strong hospital system linked with other elements of the health system capable of meeting the future needs of the community. The health care system cannot afford duplication, redundancy and inefficiency if serv ices are to be maintained and enhanced to meet the needs of the population to 2003 and beyond. The decisions of the HSRC are intended to improve accessibility and quality of care, and to create a system that is affordable and sustainable. The accompanying directions and advice to the Minister of Health will continue a process of coherent, constructive change and modernization that will strengthen the health system in the Niagara Region. The HSRC takes a long-term view of the system. It acknowledges that restructuring is an evolving process, not an endpoint, and that the change process is not a simple one. It involves organization cultures, people and physical resources. The HSRC recognizes the importance of establishing appropriate strategies and structures to facilitate change. It also appreciates that in the short term these changes will have a profound impact on the affected communities. Organizations possess distinct cultures and may have different approaches to the delivery of health care services. Integrating services requires fostering new cultures, appreciating organizational histories, and nurturing the positive attributes of each organization. It is imperative that traditions of excellence of individual organizations become inherent compone nts of the culture of newly-created organizations. The common link in health services is a commitment to provide the best possible service to those who need it. The HSRC's goal of creating a high-quality health services system is contingent upon reinvestment in community-based health services and high-quality, accessible hospitals. It is critical that appropriate community structures and support services be established before beds are closed. The HSRC has identified areas of reinvestment in community-based services to support the restructuring of local hospital services. It has identified the need to upgrade or expand hospital buildings to ensure that the infrastructure is in place for the future. Through its recommendations to the Minister of Health, the HSRC is fostering an unprecedented capital renewal program across the province to establish the necessary physical structures to support the restructured system. The magnitude and impact of these reinvestments will contribute to developing a vigorous health services system. The HSRC believes that the status quo is not an option. Although individual hospitals and other health care services have responded positively to the challenges facing them, there are limitations to what individual organizations can accomplish. Without a system approach, the future will be characterized by further fragmentation of hospital and other health services, reduced accessibility, and compromised quality of care at a high cost to the general public.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
3
The restructured hospital system envisioned by the HSRC for Niagara Region consolidates expertise and resources to minimize excess capacity and support a strong full -service hospital. The result is improved access to services, a hospital sector that is well-positioned to meet increasing demands resulting from population growth and changing demographics, and a more affordable system that facilitates additional investments in community-based services and other areas of health care. Representations to the HSRC In response to its first report on the Niagara Region, the HSRC received 119 representations from hospitals, health agencies and organizations, labour, individuals and other groups. The representations provided additional data and information for consideration. The number of representations and the obvious time and thought that went into their development are indicative of the keen interest in health services restructuring in Niagara Region. The following is a summary of the principal issues and topics raised in the representations: • request that child and adolescent mental health beds, regional rehabilitation beds, transition -
to-independent living places be located in Niagara; • more long-term care beds; • two full-service hospitals and two full-service emergency departments in St. Catharines; • need for local radiation oncology services; • location of longer-term mental health beds; • capital cost of one-site and two-site full-service hospital options in St. Catharines; • limitations of the full-service acute care site selected (space constraints and soil conditions); • adequacy of the governance model to meet the needs of smaller rural and specialty hospitals
and their communities; • regional/municipal governance model more appropriate than proposed model; • regional service role for Hôtel Dieu and a joint executive committee between Hôtel Dieu and
the Niagara Health Care System; • impact of population growth and aging on the need for health services underestimated
(especially for dialysis and emergency care); • need for French language services in the region; and • additional funds for MRI services, capital expansion and improvements. • Local support from physicians for improved critical mass and clinical coherence through
consolidation of services and amalgamation of governance The HSRC carefully reviewed the representations, undertook further analysis and reassessed the intentions released in October 1998. As a result of these further deliberations, changes have been made to intended directions and advice to the Minister of Health.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
4
Overview of the Report The HSRC's October 1998 report for Niagara Region presented intended directions for acute care, mental health, rehabilitation and long-term care services. This report presents the highlights of these intentions, a summary of the principal issues raised in the representations, the HSRC's deliberations, and its final directions and advice. Section I presents a review of the HSRC’s planning assumptions. Section II focuses on the HSRC's deliberations on siting, followed by governance in Section III. Section IV presents other issues, Section V savings and reinvestments required to support restructuring, and Section VI provides a summary of the HSRC's directions. The HSRC believes that the directions in this report achieve the objectives of quality, accessibility and affordability, and facilitate the development of a vibrant hospital sector that is capable of effectively meeting the needs of patients into the 21st century. The HSRC also believes that its directions and recommendations for reinvestment will facilitate positive change. They will position Niagara Region's hospitals to meet increasing pressures while continuing to ensure the public access to high quality care. They will preserve and enhance the health care system, address future financial challenges, and establish a solid foundation for the system-wide integration of hospital services.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
5
SECTION I: PLANNING ASSUMPTIONS Since the release of its restructuring report in October 1998 and in response to issues raised in the representations, the HSRC reviewed a number of its planning assumptions. Population Projections The HSRC further examined the size of the elderly population and future population growth in the Niagara Region. Population data used by the HSRC are age-weighted, which means that they take into account the age structure of a population when projecting the need for health services. The 1996 census indicates that 15.9% of the Niagara Region’s population was 65 years of age or older. Although Niagara had a higher proportion of this age group compared to the provincial average, the proportion is comparable to, or lower than, other areas of the province. With regard to future population growth, the HSRC uses a standardized approach to projecting future population levels based on Statistics Canada census data. This approach is used by the Ministry of Health and by municipal planning departments in Ontario, including the Region of Niagara. Based upon the 1996 census, it is estimated that the population of Nia gara Region will grow by 5.7% to 2003, for a total population of 426,505. Ontario is projected to grow by 13.8% over the same period. Between 1991 and 1996, Niagara’s population grew by only 2.4% compared to 6.6% in Ontario. Another method for projecting population growth uses estimates of job creation. This methodology calculates potential job creation based upon proposed capital development projects in a region. A certain percentage of these jobs are regarded as permanent, and having the effect of drawing individuals and their families into the region to live. It is the HSRC’s view that this non-standardized methodology presents an overly optimistic population projection due to assumptions about the total number of jobs created, the local multiplier effect and in-migration. The HSRC confirms the use of its methodology, concluding that it is a more realistic prediction of future population levels in the Niagara Region. Site Capacity Prior to releasing its October 1998, the HSRC conducted an extensive review of all facilities in St. Catharines using information provided by the hospitals, the Niagara DHC’s facilities assessment, and assessments by two independent consultants contracted by the HSRC. Further analysis of the Hôtel Dieu and St. Catharines General sites indicates that the total useable acreage of the two sites is similar. While the Hôtel Dieu site is larger in area, approximately 2.8 acres is designated green space and cannot be developed. The HSRC concludes that either location is capab le of physically accommodating all acute services on one site. In accordance with the assessment by the HSRC the addition of a cancer C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
6
treatment centre does not pose any significant barriers for either site. Soil conditions at both sites also do not present any barriers to construction. Ambulatory Care Activity Clinics and Day/Night Care In 1995/96, St. Catharines General and Hôtel Dieu had 95,871 clinic visits (including day/night care). Of these, 46% were performed at the General and 54% at Hôtel Dieu. When projecting ambulatory care activity to 2003, the HSRC methodology uses a ratio of ambulatory care visits to post-utilization acute beds, and extrapolates this ratio to acute beds needed in 2003. Due to the limitations of ambulatory care information reported by hospitals (specifically case type, acuity and demographic data), the impact of changing demographics on future ambulatory requirements cannot be estimated accurately. The HSRC, therefore, uses predicted changes in inpatient services as a proxy to estimate changes in ambulatory care. A ratio of ambulatory care to inpatient services is based on 1995/96 data, adjusted for utilization improvements. Estimated growth in inpatient activity due to changing demographics (e.g., aging population), increases ambulatory care activity in hospitals to 2003. Day Surgery In 1995/96, St. Catharines General and Hôtel Dieu hospitals performed 16,114 medical and surgical day procedures (as defined by the Ministry of Health/Joint Policy and Planning Committee funding formula). Of these, 37% were performed at the General and 67% at Hôtel Dieu. The total number of day surgical procedures does not include minor procedures performed at both hospitals that are not classified as ‘day surgery’. Hôtel Dieu was the dominant provider of ambulatory surgery in St. Catharines in 1995/96. The need for ambulatory care in St. Catharines’ hospitals is estimated to increase by 13.2% by 2003. Clinic volumes will increase from 95,871 in 1995/96 to 118,102 visits in 2003. Medical and surgical day procedures will increase from 16,114 in 1995/96 to 18,241 in 2003. The HSRC is aware that future patterns of practice, the extent to which ambulatory acute care is performed in primary care and other non-hospital settings, and clinical demand will ultimately determine the volume of ambulatory care services provided in hospital settings in the future.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
7
Ambulatory Care Volumes in St. Catharines Hospitals, 1995/96 and 2003 Type of Care 1995/96 2003 St. Catharines
General Hospital Hôtel Dieu Hospital
Total Volumes Estimated Growth Total Volumes
All Clinics 20,936 17,278 38,214 5,044 43,258 Medical Day Procedures
1,875 6,163 8,038 1,061 9,099
Surgical Day Procedures
4,087 3,989 8,076 1,066 9,142
Day/Night Care Dialysis* 0 16,459 16,459 11,749 28,208 Oncology 0 16,655 16,655 2,198 18,853 Medical Day Care
2,123 830 2,953 390 3,343
Psychiatry 21,194 0 21,194 2,798 23,992 Palliative 0 396 396 52 448
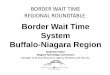
Emergency **48,578 33,679 82,257 ***13,057 95,314 Source: MIS Trial Balance, 1995/96 * Dialysis is increased 8% annually from 1995/96 volumes. ** St. Catharines General noted the its reported volume is higher than the revised number it provided. *** Emergency projection methodologies are discussed in the October 1998 Report. Growth in Emergency Services The HSRC used three methodologies to estimate the growth in emergency visits. A full discussion of these methodologies is contained in the October 1998 report. The three methodologies used by the HSRC have produced an estimate of emergency visits and are consistent with communities of comparable size. The HSRC projects a high volume of emergency visits for St. Catharines, most of which do not lead to an inpatient stay. The estimated volume of emergency visits for St. Catharines for 2003 is 95,314. The impact of this volume on a single emergency department was considered further in the HSRC’s deliberations of siting options. The HSRC analysis of emergency room visits indicates that there is no correlation between population growth and emergency volumes. In St. Catharines, as the population has increased the number of visits to emergency departments has decreased. A significant proportion of emergency room volumes have been appearing in walk-in clinics instead. This has increased the acuity level of visits to emergency departments. Physician Shortages The HSRC received representations from physician groups pointing out that there is an acute shortage of family physicians in Niagara. This fact is illustrated in the chart that follows. The region needs 72 more family physicians than are currently available. It is expected that many patients in St. Catharines are using emergency departments for routine family practice cases
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
8
because of the shortage of family physicians in the region. The chart2 also illustrates that there is a shortage of specialists in the region in 1997, which impacts on the provision of medical care.
The shortage of psychiatrists will have to be addressed quickly given the role being assumed by Niagara hospitals in long-term mental health. The HSRC advises the Minister of Health to establish a Task Force to address these shortages. Participants in this Task Force should include the Niagara Health Care System, Hôtel Dieu, local medical societies, McMaster University, University of Western Ontario, the Ministry of Health and the District Health Council. Specialized Services Magnetic Resonance Imaging (MRI) Services Representations from Niagara hospitals noted that an additional $1 million was needed to adequately fund MRI services. The HSRC has confirmed that a siting decision had been made by the Ministry of Health to site the service at the St. Catharines General Hospital site. HSRC deliberations on the siting of clinical activity follow this section. The HSRC intends to recommend to the Ministry of Health the full operating costs of the new MRI service as a reinvestment.
2 Niagara Physician Human Resources, 1997, Niagara District Health Council, October 1997
Physician Resources in Niagara
34
48
12
292
21
14
14
239
0 50 100 150 200 250 300 350
Anaesthesia
Psychiatry
Orthopaedics
Family Physicians
Needed in Niagara Currently Available
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
9
Repatriation of Orthopaedics Representations received by the HSRC requested an examination of repatriation potential of tertiary orthopaedic cases from Hamilton to Niagara. Upon further analysis the HSRC noted that the Niagara Region (based on 1995/96 CIHI data) performs 75% of the orthopaedic cases for Niagara Region's population. In addition, 60% of all tertiary orthopaedic cases for Niagara Region are also performed in Niagara Region's hospitals. The HSRC commends Niagara on its ability to serve 60% of tertiary orthopaedic cases in Niagara. As a result, the HSRC concludes that there is very little repatriation potential of orthopaedic cases from Hamilton to Niagara. Cancer Services since the release of its initial report the HSRC received a recommendation from Cancer Care Ontario (CCO) that a three-bunker cancer centre would be required in St. Catharines by 2005 to serve the residents of Niagara Region. CCO has noted that the costs associated with the construction of 11 bunkers in Hamilton is prohibitive. The requirement for cancer services in Niagara is growing and Niagara currently utilizes radiation services in Hamilton. The construction of a 3 bunker radiation oncology facility in Niagara will be offset by reductions in the scope of project planned for Hamilton. It is the understanding of the HSRC that the position of Cancer Care Ontario regarding this recommendation is that the facility constraints at the Henderson site of the Hamilton Health Sciences Centre are such that the original project plan for the expansion of the regional cancer centre at that site would be at least as expensive as developing a facility in St. Catharines. Given the issue of local access the preference was for a St. Catharines site. The St. Catharines facility would require 65,000 square feet of total space and a footprint of 26,500 square feet. The HSRC accepted this recommendation based on the fact that there will be sufficient volumes to support 3 bunkers by 2005. The fact that a cancer centre must be sited in St. Catharines was an important consideration in the HSRC’s siting deliberations. The HSRC advises the Minister of Health to begin planning for a three bunker facility to begin operations in 2005. Dialysis The HSRC has concluded that the methodology used in its October report underestimated future demand for dialysis in the Niagara Region. A rate similar to the provin ce has now been applied to Niagara. The Ministry of Health has indicated that Niagara Region makes use of home dialysis at a much lower rate than the rest of the province. If the demand for dialysis services surpasses current projections, there will be opportunities to meet increased need through greater use of home dialysis programs. As well, the establishment of a satellite dialysis program(s) elsewhere in the region would address any unforeseen growth in demand for this service. The HSRC will correct the estimates for dialysis service and advise the Minister of Health to consider, where numbers warrant, other dialysis sites in the future to ensure access.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
10
Long-Term Care Bed Allocations In its October 1998 report, the HSRC noted that Niagara requires an additional 318 long-term care beds. As a result of further analysis, the HSRC has concluded that in fact 555 additional beds are required. The HSRC will advise the Minister of Health of this additional long-term care requirement for Niagara Region to 2003. Reinvestments to Support Restructuring The HSRC has consistently noted in its advice to the Minister of Health that long-term care and home care reinvestments must be made, and these services must be in place before acute care changes are implemented. The HSRC’s benchmarks for acute care are based on the premise that long-term care and home care services will be put in place to meet the needs created by reductions in acute and chronic care beds.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
11
SECTION II: SITING OF CLINICAL SERVICES IN NIAGARA Highlights of the Notices – October 1998 • All acute in and outpatient care, including emergency services in St. Catharines to be consolidated at the St.
Catharines General Hospital site. • The Welland County General and the Greater Niagara General sites to provide acute care, acute mental health,
short- and long-term local rehabilitation, complex continuing care and sub-acute care. • The Shaver Hospital site to provide long-term mental health, long-term local rehabilitation and complex
continuing care services. • Hôtel Dieu Hospital, St. Catharines to cease operating as a public hospital. • Advise the Minister of Health to revoke the license of Maple Hurst Private Hospital, and relocate its services to
other Niagara Region hospitals. • Niagara Rehabilitation site will continue to provide out-patient rehabilitation • Rural hospitals will apply the Rural and Northern Health: Parameters and Benchmarks.
Principal Issues in the Representations Representations on siting of clinical services addressed the consolidat ion of acute and emergency care at one site in St. Catharines and the ability of emergency services to meet current and future needs. A two hospital configuration model was proposed for St. Catharines by Hôtel Dieu Hospital. Hôtel Dieu would be the regio nal hospital with 132 acute beds focusing on cancer, cardiology and nephrology, 88 long-term and acute mental health beds, and long-term rehabilitation to serve the region. St. Catharines General Hospital would become the ‘local’ provider of acute care (1 71 beds) and complex continuing care (104 beds). Both sites would have 24-hour emergency departments and intensive care units. Subsequent to the HSRC’s October 1998 report, Cancer Care Ontario recommended that a three -bunker cancer centre would be required in St. Catharines by 2005 to serve the residents of Niagara Region. With regard to emergency services, several representations expressed concern about consolidating 95,000 emergency visits at one hospital site in St. Catharines. These representations noted that with the shortage of family physicians in the region, many patients use emergency departments for routine family practice cases. The HSRC also heard that most physician services would benefit from the consolidation of services on fewer sites. The HSRC’s Deliberations In the representations, the Welland County General and Greater Niagara General hospitals accepted their roles as proposed by the HSRC. With respect to siting of services in Welland and Niagara Falls the HSRC confirms its intended directions for the Welland County General and the Greater Niagara General hospital sites. C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
12
Further planning in the context of the Rural and Northern Health Care Framework may result in future changes to the configuration of services at each site.. Since the release of the October 1998 report, the Minister of Health has accepted the advice of the HSRC and has announced the decision to close Maple Hurst Private Hospital. As noted in its October report, the HSRC developed a two-stage approach to the Ministry of Health’s Rural and Northern Health Care Framework. The rural hospitals in Niagara were excluded from stage one since they were already being considered in the deliberations on restructuring. The HSRC expects that the Niagara Region will review bed capacities of the rural hospitals based on the rural and northern benchmarks developed by the Ministry, and will determine siting of acute and non-acute services for these facilities in stage two. It is expected that this siting will employ the criteria of accessibility, quality and affordability. Niagara hospitals should also consider critical mass and clinical coherence in its siting decisions. In addition to this, the HSRC noted that it had included rural populations in siting some services in the October 1998 report. This has been adjusted and the adjustments are reflected in the bed numbers for the Welland County and Greater Niagara sites. The remaining deliberations in this section address siting of services in St. Catharines for: • acute inpatient and ambulatory services; and • non-acute services. Siting of Acute Inpatient and Ambulatory Programs in St. Catharines Since the release of its October 1998 report, the HSRC has further considered acute care activity in St. Catharines. The need to site a new cancer centre as well as accommodate large emergency care volumes without compromising access have been important considerations in these deliberations. The HSRC considered three main options for the siting of acute inpatient and ambulatory programs. These options were: 1. Siting all inpatient and ambulatory acute care programs including cancer services, at one site. 2. Siting selected inpatient and ambulatory programs at both the St. Catharines General and
Hôtel Dieu sites. 3. Siting acute ambulatory programs at one hospital site, and inpatient and ambulatory patient
programs at a second hospital site.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
13
Option 1: Siting all inpatient and ambulatory acute care programs including cancer services, at one site. Both acute hospitals in St. Catharines provide a similar range of inpatient programs. 3 Two-thirds of acute inpatient activity occurs at St. Catharines General, with the remaining one-third at Hôtel Dieu (1995/96). Neither of these hospitals has the critical mass of inpatients and outpatients that would be expected of a full-service community hospital. Current and projected volumes are insufficient to maintain two inpatient acute care facilities in St. Catharine’s. From a quality of care perspective, the HSRC’s analysis indicates that all inpatient services should be consolidated at one location in the city. Consolidating inpatient service will optimize critical mass and facilitate the recruitment and retention of specialists and other health care providers. From the perspective of accessibility, improvements would occur with one inpatient facility since patient transfers between two acute facilities would be eliminated. Geographic accessibility to inpatient care would remain the same regardless of which site was chosen. However, accessibility for emergency walk-in and ambulatory care is not as optimal as with only one site. From the perspective of affordability, greater operating savings would be achieved with this option (See the HSRC’s October 1998 report for a full discussion). However, capital costs would be higher. The capital costs of a single acute care site that could accommodate all inpatient and ambulatory acute services ranges from $84.2 to $183 million. Although the capital costs would be lower for the St. Catharines General and Hôtel Dieu sites, both are landlocked and do not allow sufficient flexibility for future expansion beyond 2003. As well, the need for additional parking spaces and traffic concerns present further difficulties. Option 2: Siting selected inpatient and ambulatory programs at both the St. Catharines General and Hôtel Dieu sites This option sites inpatient and ambulatory programs at both of the current acute care facilities in St. Catharines. The HSRC considered potentially siting a 24-hour emergency department, an ICU/CCU, the cancer centre and a sufficient number of acute beds that would be required to admit patients seen in the emergency department at the St. Catharines General site. At Hôtel Dieu, 51 elective surgical beds would provide general surgery, orthopaedic, urological, gynaecological and vascular surgery services.
3 Exceptions are obstetrics and psychiatry (provided only at St. Catharines General) and to a lesser ext ent oncology (Hôtel Dieu has a greater inpatient volume and a designated oncology ambulatory care program). The two hospitals have similar ambulatory care programs except for dialysis, which is at the Hôtel Dieu site.
Capital Costs for One-Site Acute Care Option (millions) New site $183.0 St. Catharines General $84.2 Hôtel Dieu $113.9
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
14
From the perspective of quality of care, th is option presents issues of poor clinical coherence and critical mass. For the reasons the HSRC outlined in the October 1998 report, it is not feasible to divide inpatient programs clinical programs between two sites to serve a population the size of St. Catharines referral area. Clinical coverage and coordination of services would not be maximized in a two inpatient site scenario. Accessibility is also compromised since patients may need to be transferred between the two facilities. This is especially true for patients presenting in the emergency department who may need to be transferred to the services of the other hospital. Option 3: Siting acute ambulatory programs at one hospital site, and inpatient and ambulatory programs at a second hospital site This option recognizes the importance of having a critical mass of inpatients to ensure quality of care, and attract specialists and other health care providers. The inpatient site would be the centre of inpatient care in St. Catharines. It would provide critical care, emergency services and the cancer centre to be built by the year 2005. It is estimated that the inpatient site would receive up to 65,000 emergency visits per year. At this level, physician coverage will not be an issue. This option also recognizes the growing emphasis on ambulatory services and the increasingly important role that ambulatory care will play in health care delivery in the future. Developing a central focus for ambulatory programs at one site would help ensure the development of excellence in this model of care delivery. The Preferred Option For reasons of quality, accessibility and affordability, the HSRC supports Option 3, which is to site most acute ambulatory programs at one hospital site, and inpatient and related ambulatory programs at a second hospital site. Quality of inpatient services would be enhanced due to increased critical mass and clinical coherence of a full-range of services. Quality of ambulatory services would also increase due to the relatively large clinical volumes. (It is estimated that there would be 30,000 visits annually to the centre.) There would be sufficient critical mass for many specialties to provide ambulatory care, and to support a 14-hour urgent or prompt care service. Most importantly, this option helps to address the high volume of emergency visits projected in Niagara Region by providing a full-service emergency department and a 14-hour urgent or prompt care service. This latter service would alleviate the pressure on the full-service emergency which can focus on more acutely ill patients. The urgent or prompt care service could concentrate on treating those patients who require primary care. A designated ambulatory centre would improve access to ambulatory care, the majority of which are scheduled, elective visits. Having both a 24-hour emergency and 14-hour urgent or prompt care service will maintain accessibility to these services for residents of St. Catharines and Thorold. In terms of affordability, this option will increase operating costs although decreases will be evident by eliminating duplications in the infrastructure. Although there will be capital costs for
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
15
renovation and expansion, there will ultimately be a decrease in capital costs. In fact, this option maximizes the available capital resources in St. Catharines. Siting of the Preferred Option The HSRC considered the suitability of the St. Catharines General and Hôtel Dieu sites for accommodating the in-patient acute care services, and the ambulatory care centre. The following was determined: • St. Catharines General is a much larger acute care hospital with more than double the current
developed facility space available than at Hôtel Dieu. • St. Catharines General has 70% more bed capacity than Hôtel Dieu. • The capital cost to redevelop the St. Catharines General site is considerably less than the cost
to redevelop the Hôtel Dieu site. Although consolidating emergency services to a single site will require extensive renovations and expansion, the capital costs are less at the St. Catharines General site.
• Since St. Catharines General has a much larger overall acute inpatient and emergency volume, there would be far less disruption of services during the transition period since the majority of acute care activity is already at the site.
• Clinical coherence and critical mass are enhanced through consolidation of acute and related inpatient services at the St. Catharines site.
The HSRC concludes that all in-patient acute care in St. Catharines should be consolidated on the St. Catharines General site, and the ambulatory care centre be established on the Hôtel Dieu site.
The HSRC will direct the Niagara Health Care System to receive all inpatient acute care services from the Hôtel Dieu Hospital. The HSRC will direct Hôtel Dieu Hospital to transfer all inpatient programs to the St. Catharines General site of the Niagara Health Care System. The HSRC will direct St. Catharines General to transfer ambulatory programs to Hôtel Dieu Hospital.
The HSRC believes that the optimal range of programs provided at the Hôtel Dieu site must be determined locally taking into consideration: • critical mass and clinical coherence with the main full-service facility to ensure that quality
of care is maintained; • clinics and programs that can improve access and that can be provided efficiently in a free-
standing facility; • the types of day surgical procedures that can be performed safely in a free-standing
ambulatory care centre;
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
16
• ways to reduce duplication of capital and operating costs; and • ways to maximize the use of health care providers without making excessive demands on
them to work in both settings. To be able to size the requirements of an off-site ambulatory care facility, the HSRC has developed a general estimate of the scope of ambulatory care services that can be provided at the Hôtel Dieu site. These services include day surgery, medical day procedures, day/night procedures, ambulatory care visits, other patient care services, and urgent care. The HSRC is proposing a range of services that could be provided at the ambulatory centre. The final configuration should be confirmed through detailed clinical planning. The HSRC’s Proposed Configuration of the Ambulatory Care Facility The HSRC’s estimate for sizing requirements included the following at the Hôtel Dieu site: Day Surgery The following surgical specialties currently have sufficient day surgery volumes to enable these procedures to be performed at the Hôtel Dieu site: ophthalmology; gynaecology; ear, nose and throat procedures; dental surgery; urological procedures; some general surgical procedures; and orthopaedic procedures (including a fracture clinic). Based on the projected volume of day procedures done at both hospitals by diagnostic procedure groups to 2003, the HSRC has estimated that 6,000 procedures (65%) can be performed at the Hôtel Dieu site. This does not include additional procedures done as a result of consolidation of programs across the region (i.e., developing a cataract surgery centre at the Hôtel Dieu site to service the region). Day Procedures (Medical) Day procedures are medical procedures that do not qualify as day surgery in that they do not employ the operating room facilities but are performed in procedure rooms or other suitable facilities. The HSRC assumes that most gastro-intestinal (GI) and ears, nose and throat (ENT) endoscopy will be done at the ambulatory care site. Day/Night Procedures4 These procedures are in the main medical in nature and most visits are to medical clinics within the hospital. Most day/night procedures are currently performed at the Hôtel Dieu site and will continue. These procedures include: dialysis & (34,000 plus procedures mostly at the Hôtel Dieu site, with a satellite at the St. Catharines General site for emergencies and inpatients); psychiatric day care (over 23,000 visits)*; transfusions; oncology (until 2005 when the cancer centre is built)*; palliative care*; diabetes management*; and other medical day/night procedures. 4The items noted with a * were suggested in the Hôtel Dieu Hospital’s submission to the HSRC.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
17
Ambulatory Care Visits The following clinics were assumed to stay at the Hôtel Dieu site: cancer clinics;* acute mental health clinics (transferred from the St. Catharines General site);* cardiac clinic;* gynaecology; and clinics associated with surgical specialtie s that will be performed as day surgery at the Hôtel Dieu site (e.g., eye care). The HSRC conservatively estimated that 40,000 clinic visits could be performed outside of the full service hospital (by 2003) for the purpose of assessing capital requirements for an off-site academic ambulatory care facility. These clinic volumes include other patient care services such as: general radiology for the ambulatory care patients treated; a 14 hour-a-day urgent or prompt care centre with a volume of 30,000 visits/year; laboratory (specimen collection centre); psychiatric day hospital for long-term mental health patients*; other diagnostic services (e.g., ECG, holter and treadmill); detoxification centre*; and a child development centre*. Emergency Care The HSRC assumed 14-hour daily urgent or prompt care service at the ambulatory care centre (42% less than a 24-hour operation. For capital planning purposes, the HSRC estimated 30,000 visits annually at the ambulatory care centre. The full-service SCGH site will have an estimated 62,000 to 67,000 visits annually by 2003. Siting of Non-Acute Patient Services in St. Catharines The HSRC’s deliberations on non-acute patient services addressed: • mental health: child and adolescent, and long-term services; • rehabilitation and complex continuing care. Mental Health Child and Adolescent Mental Health Services Representations to the HSRC recommended that the eight child and adolescent beds allocated to the region and sited in Hamilton should be located in St. Catharines. The HSRC examines critical mass and quality requirements when siting child and adolescent mental health beds in a community. Niagara currently does not have the specialized resources necessary to provide the level of service required for this service. In addition, the relatively small number of patients does not provide a critical mass to ensure a viable program of high quality. In 1995/96, slightly more than 600 patient days were attributed to paediatric psychiatry in Niagara Region. This amounts to less than two beds.
The HSRC confirms its intent to allocate eight child and adolescent beds for Niagara Region in Hamilton.
The HSRC anticipates that the Hamilton provider of child and adolescent mental health services will have outreach programs.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
18
Long-Term Mental Health Services In the Hamilton-Wentworth HSRC report, it was noted that over 80% of long-term mental health care for Niagara residents is provided at the Hamilton Psychiatric Hospital. 5 The HSRC recommended that 53 long-term mental health beds be sited in Niagara to meet these needs. Local siting of these beds would improve access for Niagara patients and their families, and would bring services closer to home. In determining the most appropriate site in St. Catharines for the 53 long-term mental health beds, the HSRC considered the need to optimize access and critical mass. This would support clinical and program expertise, which would help in the recruitment and retention of psychiatrists and other highly skilled mental health professionals. The sizing and capacity of physical facilities were also considered. Since the HSRC has determined that the St. Catharines General site will have all the acute care beds and the cancer centre, there is no additional capacity to house a 53-bed long-term mental health care facility. Two other St. Catharines’ sites were considered: Hôtel Dieu and the Shaver hospital sites. The HSRC determined that the 53 long-term mental health beds must be sited together to ensure critical mass. As well, the site must have sufficient capacity to accommodate associated ambulatory visits. Since the direction of mental health reform is towards greater community -based and outreach modes of service delivery, the HSRC determined that the long-term mental health program complements the proposed focus for the Hôtel Dieu site in ambulatory care for the region. This decision also makes use of available capacity and reduces capital costs.
The HSRC will direct the establishment of 53 long-term mental health beds at the Hôtel Dieu site.
Local Rehabilitation and Complex Continuing Care The HSRC considered three options for siting local rehabilitation and complex continuing care services. These options were: 1. Siting complex continuing care at the St. Catharines General site and rehabilitation at the
Hôtel Dieu site. 2. Siting complex continuing care and rehabilitation at the Hôtel Dieu site. 3. Siting complex continuing care and rehabilitation at the Shaver Hospital site. A review of the Shaver site indicates that is has recently been upgraded. The buildings and the location are more suitable for complex continuing care and rehabilitation patients than either the St. Catharines General or Hôtel Dieu sites. As well, converting either of these two acute care facilities would result in higher capital costs than expanding the Shaver site to meet the projected needs of these clients. 5Hamilton-Wentworth Health Services Restructuring Report, May 1998.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
19
The HSRC supports option three, and concludes that the Shaver site is the best location in St. Catharines for complex continuing care and rehabilitation programs.
Representations were received by the HSRC requesting that five of the 17 regional rehabilitation beds allocated to Hamilton be located in Niagara Region at the Shaver/Niagara Rehabilitation site. The HSRC acknowledges and supports the role of Niagara Rehabilitation in joint replacement, joint revision, spinal cord rehabilitation and amputee programs. However, the HSRC has determined that five beds is an insufficient critical mass to provide quality programming for a specialized regional program. These programs must have sufficient critical mass to support specialized care providers who can care for clients with complex rehabilitation needs (e.g., major limb amputations). The HSRC confirms that the regional rehabilitation complement for Niagara will be located in Hamilton. In the HSRC’s October report, five transition-to-independent-living places were identified for the Niagara Region and sited in Hamilton. Representations made to the HSRC requested that these five places be located in Niagara. Upon further analysis, the HSRC has concluded that these places should be sited in Niagara.
The HSRC will direct that the five transition to independent living places allocated to Niagara be sited in Niagara.
Summary of Siting Decisions Development of the Hôtel Dieu Site as an Ambulatory Care Centre and Long-term Mental Health Pavillion In concluding that the acute inpatient services are best located at the St. Catharines General site the Hôtel Dieu site is left to become a major ambulatory care centre serving not just the residents of St. Catharines but the entire Niagara Region. As noted earlier, the HSRC has embraced the concept in other communities where this approach has been locally developed. The future orientation of hospital and health care is predominantly ambulatory in recognition of the technological advances that permit a different delivery mode and patient preferences for these types of service. As in Ottawa, Toronto and Kingston the advent of this approach to care will enhance patient and provider choice and access. The site will also offer a regional long-term mental health (LTMH) program. This program will be transferred from the Hamilton Psychiatric Hospital. The location of long-term mental health services closer to the patient population is consistent with the directions of mental health reform. The linkages between the St. Joseph’s Hospital and the McMaster University in Hamilton are fundamental to the successful introduction of this new level of service in the Niagara Re gion. Providers of acute mental health services will be linked to the referral centre at the Hôtel Dieu site. Mental health reform initiatives anticipate a much different clinical usage of the inpatient services with greater emphasis on delivering serv ices to patients in the community in order to avoid hospitalization until necessary. Therefore, linkages between the services at the Hotel Dieu C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
20
site and those in the community are fundamentally important to the successful implementation of mental health reform. A site role in both ambulatory care and Long Term Mental Health is similar to past decisions of the HSRC in both London and Ottawa. The HSRC concludes that the St. Catharines General site will offer a broad range of in -patient services, including 24-hour emergency and future cancer treatment services. The Hôtel Dieu site will be a major ambulatory care and urgent or prompt care centre for the Niagara Region. It will also offer a regional long-term mental health program which will be transferred from the Hamilton Psychiatric Hospital. The Shaver Hospital will provide complex continuing care and rehabilitation services. The five transition to independent living spaces for Niagara Region will be transferred from Hamilton to Niagara. Since the October 1998 report, the HSRC noted that it had included rural populations in siting sub-acute and complex continuing care services. This has been revised and the adjusted figures are reflected in the bed numbers for the Welland County and Greater Niagara sit es. The following table provides a summary of the bed configuration of all sites in Niagara.
Douglas Memorial Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 50 0 -- 0 -- 25 -- 75 1997-98 39 0 -- 0 -- 25 -- 64 Notices 39 0 0 0 0 --* --* 39
Directions 39 0 0 0 0 --* --* 39
Greater Niagara General Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 173 29 -- 0 -- 48 -- 250 1997-98 173 29 -- 0 -- 48 -- 250
Notices-2003 134 20 0 5 15 60 16 250 Directions 134 20 0 5 15 52 15 241
Hôtel Dieu Hospital St. Catharines Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 149 0 -- 0 -- 0 -- 149 1997-98 119 0 -- 0 -- 0 -- 119
Notices-2003 0 0 0 0 0 0 0 0 Directions 0 0 53 0 0 0 0 53
Maple Hurst Private Hospital Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 0 0 -- 0 0 20 -- 20 1997-98 0 0 -- 0 0 20 -- 20
Notices-2003 0 0 0 0 0 0 0 0 Directions 0 0 0 0 0 0 0 0
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
21
Niagara-on-the-Lake Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 18 0 -- 0 -- 20 -- 40 1997-98 9 0 -- 0 -- 11 -- 20
Notices-2003 9 0 0 0 0 --* --* 9 Directions 9 0 0 0 0 --* --* 9
Port Colborne General Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 50 0 -- 0 -- 30 -- 80 1997-98 36 0 -- 0 -- 24 -- 60
Notices-2003 36 0 0 0 0 --* --* 36 Directions 36 0 0 0 0 --* --* 36
St. Catharines General Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 223 26 -- 0 -- 36 -- 285 1997-98 201 26 -- 0 -- 36 -- 263
Notices-2003 303 35 0 11 0 0 36 385 Directions 303 35 0 11 0 0 36 385
Shaver Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 0 0 -- 22 -- 102 -- 124 1997-98 0 0 -- 22 -- 102 -- 124
Notices-2003 0 0 53 0 34 124 0 211 Directions 0 0 0 0 34 124 0 158
Welland County General Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 159 16 -- 0 -- 139 -- 314 1997-98 141 16 -- 0 -- 77 -- 234
Notices-2003 106 20 0 5 15 62 18 226 Directions 106 20 0 5 15 46 13 205
West Lincoln Memorial Acute Mental Health Local Rehabilitation CCC SAC TOTAL Acute Long-Term Short-Term Long-Term
1995-96 62 0 -- 0 -- 16 -- 78 1997-98 45 0 -- 0 -- 16 -- 61
Notices-2003 45 4** 0 0 0 --* --* 45 Directions 45 4** 0 0 0 --* --* 45
*The final distribution of 66 complex continuing care and 18 sub -acute care beds among the rural hospitals in Niagara will be determined in Stage 2 of the HSRC consideration of the rural and northern hospitals. ** To be located in Hamilton.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
22
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
23
SECTION III: GOVERNANCE OF NIAGARA REGION HOSPITALS Highlights of the Notices – October 1998 • Contractual relationship between the West Lincoln Memorial Hospital (Grimsby) and the Hamilton Health
Sciences Corporation endorsed. • St. Catharines General, Greater Niagara General, Niagara-on-the-Lake, Shaver, Niagara Rehabilitation Centre,
Welland County, Port Colborne General and Douglas Memorial to amalgamate into the Niagara Health Care System
• Standing committees to be established for the rural hospitals in Port Colborne, Niagara-on-the-Lake and Fort Erie, and the amalgamated Shaver/Niagara Rehabilitation Centre complex continuing care and rehabilitation programs.
• Contractual relationship to be established between the Niagara Health Care System and the Religious Hospitallers of St. Joseph of Hôtel Dieu, St. Catharines for long-term inpatient and outpatient mental health services.
• The creation of the Central West Mental Health Agency endorsed.
Principal Issues in the Representations The representations raised a number of governance issues. Port Colborne, Niagara-on-the-Lake, Fort Erie, and the Shaver hospitals supported autonomous governance rather than a standing committee structure within the Niagara Health Care System. Standing committees were only acceptable with changes to the terms of reference. Hôtel Dieu Hospital preferred to have a Joint Executive Committee (JEC) alliance instead of a management contract with the Niagara Health Care System Board, as was the HSRC’s intent. The contractual relationship between West Lincoln Memorial Hospital and the Hamilton Health Sciences Corporation was supported. Finally, a number of representations noted that there was insufficient recognition of the efforts to coordinate governance and management between hospitals and long-term care facilities. The HSRC’s Deliberations Background The direction of the HSRC in all governance decisions is clear: interdependence in hospital services is preferable to independence. The HSRC has attempted to establish governance structures that contribute to the successful implementation of restructuring, and the future coordination of service planning and delivery. The HSRC’s goal is to establish governance models that best serve the public interest. These models must facilitate the continuing integration of health services, while respecting the traditions and cultures of local hospitals. In its October 1998 report, the HSRC described three governance models to address issues associated with the desire of rural hospitals to preserve some local autonomy in governance decisions. Briefly these models were: • Joint Executive Committees strengthen cooperation between hospitals in a city or region by
horizontally integrating hospital services. Hospitals retain their separate governance but must work together in a number of ways. JECs build on the Ontario experience of joint liaison and planning committees, and alliance agreements. Local community care access centres and district health councils play important roles on JECs.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
24
• Subsidiary governance is more prevalent in the private sector, but is quite consistent with the
legal requirements of the Public Hospitals Act and other applicable Ontario legislation. A public hospital may carry on some of its activities through a subsidiary corporation, but its members owe their allegiance to the subsidiary rather than the parent corporation. Subsidiaries must have real activities to govern and meaningful decisions to make if they are to be successful.
• Standing committees of the board of directors is a third governance model. These
committees can ensure that particular interests have an effective voice at the board leve l by addressing particular service requirements, unique needs or other issues.
The HSRC’s Consideration of Governance Options The HSRC reconsidered its decisions on governance in light of the issues raised in the representations, and its final decisions on the siting of services. The following are addressed: • governance of West Lincoln Memorial Hospital; • governance of the Hôtel Dieu Hospital; and • governance of the other hospitals in Niagara Region. Governance of West Lincoln Memorial Hospital In its October 1998 report, the HSRC noted that West Lincoln Memorial Hospital has a contractual relationship with the Hamilton Health Sciences Corporation which oversees its management and day to day administration. The West Lincoln board retains its autonomy, its accountability for the hospital’s management and its veto over any dispute or disagreement relating to matters of its own policy. The relationship is consistent with the natural referral pattern noted by the HSRC in its determination of the rural and northern hospital networks.
The HSRC confirms its support of the West Lincoln Memorial Hospital and Hamilton Health Sciences Corporation governance and management arrangement .
Governance of the Hôtel Dieu Hospital In its October 1998 report, the HSRC determined that the Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines would retain independent governance and have a contract with the Niagara Health Care System to manage long-term mental health services. The HSRC noted that this would maintain the Catholic mission in health care and give the Religious Hospitallers a significant role in mental health services. In light of the fact that the HSRC will direct the Hôtel Dieu site to be retained as an ambulatory centre and long-term mental health facility, the HSRC concludes that the Hôtel Dieu should govern these services on its site. This governance should be separate but linked to the governance of other hospital services providers. This is in keeping with preserving the Catholic mission in health care, and the broader need to have joint decision making for these services.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
25
In its representation, Hôtel Dieu advocated a significant role in the provision of health care services in the region. It proposed to become a provider of many referral-based inpatient services. Local responses to the HSRC’s October report also supported maintaining Hôtel Dieu’s role in health care. The HSRC considered this input in its deliberations. It concluded that the range of services proposed for the current site owned by the Religious Hospitallers represents a significant regional and local role in the health service delivery system. The Hôtel Dieu retains independent governance and management of a significant range of services on its site. The HSRC is aware of the tradition of care and service embodied by Hôtel Dieu over the past 50 years. The HSRC considered this new role for Hôtel Dieu in providing ambulatory care in St. Catharines, in its deliberations on the best approach for separate governance within an integrated and coordinated health service system in Niagara Region. A linkage was considered for Hôtel Dieu as in the communities of Sarnia, Chatham and Sault Ste. Marie. These linkages have been voluntary with all services located on one site. In St. Catharines, since services will be offered at separate sites and a voluntary arrangement does not exist now, the HSRC concluded that Hôtel Dieu Hospital will govern and manage the ambulatory care centre and long-term mental health services on its existing site, and will establish a linkage with the other providers through a Joint Executive Committee. There will also be a single medical staff and Medical Advisory Committee (MAC) between Hôtel Dieu and the Niagara Health Care System. The JEC will support joint decision making for the full range of ambulatory care services that are intricately connected with the inpatient services to be provided on the General site. This arrangement will facilitate improved accessibility, quality and affordability of services while preserving the independent governance of the Hôtel Dieu.
The HSRC will direct Hôtel Dieu Hospital and the other hospital service providers in the region to establish a Joint Executive Committee, single medical staff and single Medical Advisory Committee.
Governance of the Other Hospitals in the Niagara Region The HSRC re-considered the governance arrangements of the other hospitals in Niagara Region. Although the rural and complex continuing care hospitals supported the need for regional governance of hospital services, they preferred separate governance arrangements supported with collaborative mechanisms (similar to the contractual arrangement in West Lincoln). Fundamentally, there is a fear that a larger governance structure would not be sympathetic to issues of importance to rural communities. Of primary concern to these hospitals, is that emergency services and inpatient beds would eventually be eliminated. The HSRC believes that these concerns can be addressed in the structure of a larger Niagara health care system which has representatives from each of the communities. It confirms its intent to direct the establishment of a Niagara Health Care System to govern and manage hospital services in the region (the Hôtel Dieu and West Lincoln Memorial hospitals will be governed and managed separately). Local input into decision making in the smaller communities would be assured through the creation of standing committees of the Board for Fort Erie, Port
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
26
Colborne and Niagara-on-the-Lake. These committees would address local clinical service management issues and linkages between the local hospital and other providers. There would also be a standing committee for complex continuing care and rehabilitation – to be provided at the Shaver/Niagara Rehabilitation Centre – that would maintain a focus on these important services and emphasize the need to coordinate with acute care.
The HSRC believes that this governance structure addresses quality of care and accessibility issues. From the perspective of quality of care, this governance structure will: • improve the provision of care and maximize the coordination of services in the Niagara
Region; • expedite the restructuring of acute care services in the region, and thereby maximize the
critical mass of services and support health care providers; • ensure that resources are allocated according to regional priorities; • ensure a profile for rehabilitation and complex continuing care, and the need to establish
links with acute care; • ensure a distinct voice for long-term mental health providers, an issue that was raised in both
the Steering Committee and the Niagara District Health Council reports; and • support a single medical staff. From the perspective of accessibility, this governance structure will: • help to attract and retain more physicians because of its integrated and coordinated approach
to care delivery; and • ensure accessibility to services by preserving a voice for smaller communities in decision
making about health care through the standing committees. From the perspective of affordability, the governance structure will: • support a unified management structure; and
Niagara Health Care System
Greater Niagara GeneralSt. Catharines General
Welland County GeneralDouglas Memorial
Port Colborne GeneralNiagara-on-the-Lake
ShaverNiagara Rehabilitation Centre
Complex ContinuingCare & Rehabilitation
Standing Committees of the Niagara Health Care System Board
Niagara-on-the-Lake
Port ColborneFort Erie
JECThe Religious
Hospitallers of St. Josephof the Hotel Dieu of St.
Catharines
CommonMedical StaffSingle CEO
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
27
• facilitate the consolidation of support services, thereby reducing overhead expenses. The Niagara Health Care System will be ultimately responsible for all matters relating to the operation of the hospital sites including: • the restructuring of hospital services, the allocation of services and the continuum of care
provided to patients; • the implementation of a plan that will address the impact of hospital restructuring; • the financial and operating plans for the hospitals; • the development of regional shared administrative and laboratory plans; and • the examination of opportunities for the appropriate integration of shared services to reduce
unnecessary duplication. The Standing Committees The HSRC reassessed the terms of reference of the standing committees, taking into account the concerns raised in the representations. These concerns centred on the need to understand issues of importance to rural communities. To ensure that the standing committees and the Niagara Health Care System is sensitive to these issues, the HSRC concluded that any decision to eliminate inpatient services or emergency services must be approved by the standing committee. Each standing committee will have at least one member from the Niagara Health Care System. In terms of Standing Committee decisions on the NHCS decisions regarding the elimination of emergency and/or inpatient services in any of the rural acute sites, the NHCS will work with the Standing Committees to establish appropriate decision criteria. The Standing Committees will be responsible for the following: • participating in the development of the mission and core values of the Nia gara Health Care
System; • participating in the development of the administrative and medical bylaws of the Niagara
Health Care System; • advising the Niagara Health Care System on matters pertaining to the nature, funding,
quality, accessibility and affordability of services delivered by the local hospital facility; • participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the Medical Advisory Committee of the Niagara
Health Care System; and • participating in the negotiation of partnership arrangements with other local health service
providers. • Any decisions to eliminate inpatient services or emergency department must be approved by
the Standing Committee • In approving decisions regarding the elim ination of emergency and/or inpatient services at
any of the rural acute sites the Standing Committee will not unreasonably withhold such approval.
• Each Standing Committee will have at least one member from the NHCS Board C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
28
Relationship Between Hospitals and Other Health Care Providers A number of representations indicated that hospitals have ongoing relationships with other health care providers. For example: • Port Colborne Hospital and Northland Manor have examined a joint venture arrangement
where the manor would be redeveloped on the hospital site. • At Douglas Memorial Hospital in Fort Erie, five community-based health organizations have
set up programs in the past 18 months using hospital space. The hospital is also exploring formal partnership opportunities with homes for the aged and nursing homes in the community.
• West Lincoln Memorial Hospital and Deer Park Villa have formal linkages with each other. For example they have shared board membership, a shared foundation and joint services in such areas as dietary, maintenance and finance.
Representations from organizations such as these, expressed concern that the HSRC’s proposed governance model will jeopardize current relationships. The HSRC supports the voluntary efforts of hospitals and long-term care facilities to engage in collaborative planning, shared governance and joint management. The synergies that result improve access to services for patients, and potentially lower costs related to administrative and support services.
The HSRC will advise to the Minister of Health to support the collaborative efforts of hospitals and long-term care facilities in governance and management.
Facilitation Assistance The HSRC confirms its intent to appoint a facilitator to assist the hospitals in creation of the Niagara Health Care System. The local hospitals have already started the process of selecting this individual. The HSRC will work with the hospitals to finalize the process. The process will lead to the development of the mission, vision, administrative and medical bylaws and a membership recruitment and nomination process for the amalgamated hospital, a hiring plan for the new Chief Executive Officer of the amalgamated hospital system, along with principles, framework and operational characteristics of the relationships among the parties. This work must be completed within 90 days. Priorities of the Health Care System Corporation There are a number of priorities arising from this report for the Niagara Health Care System, when it is formed. These address physician shortages, the activities of the ambulatory centre, work on rural and northern health care, and French language services.
The HSRC encourages the Niagara Health Care System, the local medical societies, McMaster University, the University of Western Ontario and the Ministry of Health to develop a task force to address the issue of physician shortages in Niagara Region.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
29
The HSRC will direct both Hôtel Dieu Hospital and the Niagara Health Care System Board to jointly develop a detailed functional program on the scope of ambulatory services provided at both HDH and SCGH sites.
Laboratory Services The Niagara hospitals are in one of two pilot sites for the new direction of laboratory services reform. In this region a request for proposals has been called by the Ministry of Health for the development of integrated laboratory systems by all providers in the Central South. The hospitals are directed to complete a plan for co-ordinated laboratory services to meet the needs of the hospitals in the Niagara region. The primary objective of this planning exercise is to provide laboratory services that better reflect the unique and individual needs of the region, while reinforcing an emphasis on patient requirements. This process represents an opportunity for the current providers to work collaboratively to deliver a viable responsive efficient laboratory services system. The capital funds for laboratory services are contingent upon receipt of a plan from the hospitals and will be based on the requirements identified in the plan and on the outcome of the Ministry’s request for proposal process, as appropriate. Therefore the capital reinvestment for laboratory services will be determined upon completion and approval of this plan.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
30
SECTION IV: OTHER ISSUES Coordination of Mental Health Services As noted in its October 1998 report, the HSRC continues to endorse structures for the planning, coordination and funding of mental health services. The restructuring of mental health services is an immediate issue that requires management by an independent and transitional body. The HSRC has been in the process of reviewing the role of regional agencies and expects to complete this work shortly. If the Ministry is to continue to discharge its responsibility for planning and funding mental health services, it is imperative that stronger, more effective coordinating mechanisms be put in place and that their effectiveness be demonstrated quickly. French Language Services Representations to the HSRC noted that Niagara Region has a significant francophone population. Within Niagara Region, Welland and Port Colborne have been designated under the French Language Services Act. A French language services plan was developed by the DHC in 1989 and is currently being updated for the Region. Welland, Niagara Falls and St. Catharines have the largest concentration of francophone residents. The Office of Francophone Affairs reports that 4.0% of the Niagara population is francophone (1996 census) .
The HSRC will direct the Niagara Health Care System, once formed, to seek appropriate designation under the French Language Services Act
Rural and Northern Health Care Framework The HSRC developed a two-stage approach to the Ministry of Health’s Rural and Northern Health Care Framework. This approach was presented in detail the October 1998 Niagara report. The rural hospitals in Niagara were excluded from stage 1 of this approach since these hospitals were already being considered in the deliberations on restructuring. At that time, the HSRC had not yet developed mechanisms to evaluate rural hospitals against the benchmarks for rural and northern hospitals. The HSRC released its reports on the 18 rural and northern networks on March 8, 1999 and has asked these networks to begin work on stage 2. 6 One task of the rural networks is to apply the rural and northern benchmarks to rural hospitals and configure the siting of non-acute services.
The HSRC will direct the Niagara Health Care System and the West Lincoln Memorial Hospital to apply the Rural and Northern Health: Parameters and Benchmarks to the rural hospitals in Niagara, allocate sub-acute and complex continuing care beds, where appropriate and to submit plans to the HSRC by September 20, 1999. The plans are
6 Health Services Restructuring Commission Rural and Northern Hospital Network Report, March 1999.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
31
expected to utilize the HSRC criteria of access, quality and affordability. The allocation process should also consider issues of critical mass and clinical coherence.
Current and Proposed Academic Activities in St. Catharines The academic physicians at Hôtel Dieu Hospital met with HSRC staff to discuss their current academic programs and future plans. There was concern that the HSRC’s siting and governance recommendations do not foster the developing academic program at Hôtel Dieu. Hôtel Dieu Hospital has a small teaching program associated with the University of Western Ontario (UWO). Two to four undergraduate students rotate through the 15-bed clinical teaching unit every four weeks. Eighteen core medical students have rotated through this program in the past 18 months. The program currently has three geographic full-time physicians. The hospital has financially supported the creation of the clinical teaching unit and the operation of a cardiovascular diseases research unit. UWO considers this teaching program to be a valuable enterprise that enriches both the medical culture of physicians in St. Catharines, and provides a setting for students to gain exposure to the broad range of patients seen in community hospitals and physicians’ offices. McMaster University has expressed an interest in having its medical students rotate through this teaching program as well. The HSRC acknowledges the interest and vision that the academic physicians and Hôtel Dieu have shown in attracting medical students to the St. Catharines community. The HSRC fully endorses the need to have the future generation of health sciences students placed in community hospital settings to enrich their exposure to basic medical care in community settings. The HSRC views the growing desire of both universities to train its students in St. Catharines as beneficial for attracting new physicians to the Niagara community. The HSRC believes this academic program should be fostered and enhanced. In Section 1 of this report the HSRC recommended to the Minister of Health the establishment of a Task Force to address physician shortages in Niagara Region. The HSRC further advises the Minister of Health that the above noted Task Force also consider the following tasks: • The scope of clinical teaching units at the St. Catharines General site, and ambulatory care
teaching largely to be provided at Hôtel Dieu Hospital; • A medical staff credentialling process that recognizes and fosters the need to have a cadre of
geographic full-time physicians (GFT) to improve overall quality of care and attract future physicians to work in the community; and
• Strategies to nurture a research environment in collaboration with both universities. The task force should submit a plan to the Ministry of Health by March 1, 2000. The HSRC has made allowance for teaching and research functions for the consolidated inpatient site in St. Catharines.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
32
SECTION V: SAVINGS AND REINVESTMENTS Highlights of the Notices – October 1998 • Capital reinvestments in Niagara Region to total $78.4 million. • St. Catharines General, Welland County General, Greater Niagara General and the Shaver hospitals to receive
capital reinvestments. • Capital needs of smaller hospitals to be determined at a later date.
Principal Issues in the Representations Representations on capital reinvestments requested more funding. Greater Niagara General Hospital requested additional capital ($15.9 million rather than $8.2 million) to demolish an existing structure and construct a new buildin g for complex continuing care and rehabilitation. Welland County General Hospital requested more capital ($8.8 million rather than $3.7 million) to relocate existing operating rooms elsewhere and to expand emergency room space. Shaver Hospital requested an additional $1.8 million for an additional support services area. A number of representations expressed concern about the operational debt held by Greater Niagara General. The HSRC’s Deliberations Capital Reinvestment In its deliberations, the HSRC determined that additional capital funding is required to address service configurations at Greater Niagara General, for additional emergency space at Welland County, and for a support services area at the Shaver Hospital. The HSRC has adjusted its capital estimates accordingly. The HSRC acknowledges that certain costs are not addressed in the estimates process. Of particular note is restructuring capital, which is directed towards restructuring activities and not towards upgrade and replacement. Although some existing accommodations may be below current standards or improperly configured, these matters are not restructuring issues, but ones to be addressed either locally or by Ministry of Health cost-sharing arrangements.
The HSRC has reviewed its capital estimates and has made adjustments to its calculations. The HSRC confirms that these capital estimates adequately reflect the costs associated with hospital restructuring in Niagara Region.
Changes in capital estimates since the October 1998 repor t are the result of further analysis and the HSRC’s decisions on siting of services in Niagara Region (see Section II). Since the release of the first Niagara report, Cancer Care Ontario announced the placement of a three bunker cancer treatment units in St. Catharines. The capital requirements for this program is estimated at $20.8 million. The proposed configuration of services in St. Catharines have resulted in some reductions in the original capital estimates.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
33
As a result of changes since the October 1998 report, capital estimates have been reduced for the Shaver site. This reduction pertains primarily to the costs associated with the construction of a pavilion for long-term mental health services. The siting of this program at the Hôtel Dieu site substantially reduces the capital that would have been required at the St. Catharines General site for the expanded emergency department. There are no capital implications for maintaining the emergency at the Hôtel Dieu site. The revised capital estim ates, in millions, are noted below.
Niagara Capital Summary HSRC Directions March 1999
HSRC Notices October 1998
Shaver $5.8 $14.7 Welland $3.9 $3.7 Greater Niagara General $8.7 $8.2 St. Catharines General $35.6 $51.8 Hôtel Dieu $12.9 $0.0 SUB-TOTAL $66.9 $78.4 Cancer Treatment SCGH Site $20.8 -- TOTAL $87.7 $78.4
For a complete breakdown of capital estimates, please refer to Appendix A. Capital requirements have not been estimated for the four rural hospitals – Douglas Memorial, Port Colborne General, Niagara-on-the-Lake and West Lincoln Memorial. Capital requirements for these sites will be estimated once the Niagara Health Care System and West Lincoln Memorial have determined the service configuration at these locations, applied the Rural and Northern Health: Parameters and Benchmarks to these hospital sites and submitted their plans to the HSRC. Reinvestments in Other Services In order for hospital restructuring to be successful, reinvestment must occur in both hospital-based services, including acute care, sub-acute care, mental health, rehabilitation and complex continuing care as well as in other sectors of the health system, including long-term care and home care. Home Care Reinvestment The need for home care reinvestment was addressed in the HSRC research summarized in the July 1997 discussion paper7. The proposed reinvestment for home care services in Niagara Region is estimated at $6.0 million.
7 HSRC, Rebuilding Ontario’s Health System: Interim Planning Guidelines and Implementation Strategies.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
34
Long-Term Care Reinvestment The term ‘long-term care spaces’ includes long-term care beds in nursing homes and homes for the aged, supportive housing, long-term home care, attendant care and adult day care. In Niagara Region, based on the current funding system for long-term care beds, $28.6 million in additional annual funding would be required by 2003 to support the operating costs of 555 additional long-term care beds and 1,387 additional long-term care places. This reinvestment will have to be evaluated against the broader configuration of long-term care services. Sub-Acute Care Reinvestment The HSRC has developed a model16 to estimate the cost of this program. It has determined a cost of $211.07 per patient day, based on 90% occupancy rate (units greater than ten beds). Based on this approach, the additional annual investment required to provide 82 sub-acute beds would be no greater than $6.3 million. The HSRC intends to advise the Minister of Health to invest this amount in sub-acute care in Niagara Region by 2003. Mental Health Reinvestment The HSRC recognizes that additional investment may be required in community -based mental health services across the Niagara Region in addition to the investment for the additional mental health beds. The current policy of the Ministry of Health supports the protection of the exist ing envelope of funds allocated to mental health services in each community; any identified savings are to be reinvested in mental health care. While the HSRC has reflected this policy in its directions and recommendations, it notes that the current distribution of mental health funds may not be equitable across all regions of the province, and therefore some adjustments in the overall funding envelope may be required. In accordance with the new planning targets, Niagara Region’s residents will require 79 acute mental health beds and 53 long-term mental health beds. The investment associated with this is $7.7 million. Rehabilitation In accordance with the new planning targets, Niagara Region’s residents will require 85 local rehabilitation beds to be located in Niagara Region. The investment associated with this service is $6.3 million.
16 See Rebuilding Ontario’s Health System: Interim Planning Guidelines and Implementation Strategies. Health
Services Restructuring Commission, July 1997.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
35
The required 17 regional rehabilitation beds Niagara will be located in Hamilton, at the Hamilton Health Sciences Corporation. The five transition-to-independent living places for Niagara will be located in Niagara. Joint Replacement The HSRC has determined that reinvestment is required to achieve target rates of utilization for joint replacement procedures. The required reinvestment for Niagara Region for these services is between $0.7 and $0.9 million. Magnetic Resonance Imaging
The HSRC confirms the siting of MRI services at the General site in St. Catharines and recommends operating fund reinvestment of up to $1 million annually to cover the costs of its operation. Information Technology The need for improvements in information systems, information technology and enhanced telemedicine potential is strongly supported in Niagara Region. Such systems are essential for movement towards an integrated delivery of care to patients regardless of setting. The Ministry of Health is developing policy and process about these and some reinvestment will be required to achieve full development. Similarly, telemedicine enhancement can reduce patient transportation costs and improve diagnostic and treatment capabilities of hospitals and physicians in Niagara Region. Reinvestment in information technology will pay dividends in the longer term on both quality and efficiency aspects of care. Summary of Required Reinvestment The following table summarizes the estimated reinvestment requirements for the Niagara Region by 2003. Reinvestment Summary
Service Reinvestment Home Care $6.0 million Long-Term Care $28.6 million Sub-Acute Care $6.3 million Mental Health $7.7 million Rehabilitation $6.3 million Joint Replacement $0.7 – 0.9 million Magnetic Resonance Imaging Up to $1 million Information Technology TBD TOTAL $56.6 – 56.8 million
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
36
Estimated Operating Savings from Restructuring The following summary outlines the total expenses and savings associated with the restructuring recommendations after discounts for clinical efficiencies in non-rural hospitals.
Notices Directions 1995/96 Net Expenses* $255,153,037 $258,252,383** Clinical Efficiencies ($15,295,155) ($15,295,155) Program Transfers ($1,226,639) ($1,056,877) Transfer materials management $76,398 ($35,723) Support service efficiencies ($4,886,660) ($5,587,069) Administrative efficiencies ($7,141,034) ($5,587,215) Reallocation of other expenses $1,070,590 $1,070,590 Plant Closure ($1,439,985) $0 Change in selected expenses ($988,089) ($54,829) Complex Continuing Care Savings ($4,794,340) ($4,794,340) Total Savings ($30,226,920) ($29,693,213) Revised Expenses $224,926,117 $228,559,170 *Net Expenses from OCDM ** Corrected net expense figures since October 1998 Report The net expense budget for the Niagara Region hospitals has been calculated to be $255 million. Savings amount to $29.7 million or 11.5%. These savings include complex continuing care and are not in excess of reductions which have taken place after 1995/96. These savings also do not reflect any changes that may still need to occur in rural hospitals in the region. The revised net expenses for Niagara Region amount to $228.6 million. The HSRC continues to update its costing methodology and will now use Ontario Cost Distribution Methodology (OCDM) data. See Appendix E of the October 1998 report for a detailed description. To conduct its analysis of clinical and administrative efficiencies, and determine the operating savings estimates for each hospital, the HSRC has relied on the most recent data for the 1995/96 fiscal year. However, since 1995/96, due to financial pressures and changes in clinical practice, hospitals have made further adjustments to their operations. The Ministry of Health will need to consider the extent to which hospitals have already or will achieve the efficiencies and related operating savings in 1996/97 and 1997/98. Restructuring savings achieved by hospitals since 1995/96 should be applied against the HSRC’s operating saving estimates. Operating Debt In response to concerns expressed about current operating deficit levels at the Greater Niagara General hospital (GNGH): C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
37
The HSRC directs the GNGH to establish a Steering Committee to oversee the management of the debt. This Steering Committee will report to the Niagara Health Care System Board once established and will be responsible for ensuring the implementation of the recommendations of the operational review of the GNGH.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
38
SECTION VI: SUMMARY OF DIRECTIONS Siting Of Clinical Activity
Adult Acute Care The acute inpatient activity estimates for Niagara are based on the achievement of utilization improvements as well as upon the projected growth in population served. The HSRC has determined that these considerations result in an allocation of 543 acute care beds for Niagara’s non-rural acute care hospitals by 2003. Within St. Catharines, all acute in-patient and emergency care services will be consolidated at the St. Catharines General site. Ambulatory care services will be located at the Hôtel Dieu site in St. Catharines. Acute care beds at the other large hospital sites will be located at the Welland County General and Greater Niagara General sites. Operating rooms required to perform at the revised activity levels have been assessed, with a determination that 18 operating rooms and 13 procedure rooms are required in N iagara by 2003. The allocation of beds to the rural Niagara hospitals are to be determined by the NHCS Board and West Lincoln Memorial under Stage 2 of the of Rural and Northern Health Care Framework. Rural hospitals in Niagara currently have 129 beds. These bed numbers may change after the application of the rural and northern benchmarks, allocation of non-acute resources and additional beds for growth have been added. Adult Acute Mental Health Niagara will have 79 acute adult mental health beds, allocated among the larger acute care hospitals in the region. West Lincoln Memorial will access 4 adult acute mental health beds in Hamilton. Child and Adolescent Mental Health The eight child and adolescent mental health beds which have been determined to be required for Niagara to 2003 will be sited at the Hamilton Health Sciences Corporation. Long-Term Mental Health Niagara requires 53 long-term mental health beds to 2003, to repatriate this service into the region; these beds will be located at the Hôtel Dieu site, St. Catharines. This service will be managed by the Religious Hospitallers of St. Joseph of the Hôtel Dieu St. Catharines. Sub-Acute Care Niagara requires 82 sub-acute care beds. These beds will be distributed among each of the acute care sites in Niagara Region. The HSRC has sited 64 of these beds at the non-rural acute care
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
39
hospital sites in Niagara and reserved the decision about siting the remaining 18 sub-acute care beds for Stage 2 of the HSRC’s approach to the rural and northern hospital networks. Complex Continuing Care A total of 288 complex continuing care beds are required in Niagara by 2003. Of these, 222 will be sited at Greater Niagara General, Shaver and Welland County General. The remainder will be considered as part of the Stage 2 process of the Rural and Northern Health Care Framework. Rehabilitation The 85 local rehabilitation beds (long-term and short-term) required for Niagara to 2003 will be located at Greater Niagara General, Welland County General, St. Catharines General and Shaver hospital sites. The required 17 regional rehabilitation beds Niagara will be located in Hamilton, at the Hamilton Health Sciences Corporation. The five transition-to-independent living places for Niagara will be located in Niagara
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
40
Summary of Clinical Service Changes The following table compares actual bed numbers in 1997/98 in Niagara to those required for 2003. Category of Care 1995-96 1997-98 Notices
2003 Directions
2003 Acute* 884 763 576 576 Projected Growth** -- -- 96 96 Adult Acute Mental Health 71 71 79 79 Child & Adolescent Mental Health*** -- -- 8 8 Long-Term Mental Health 0 0 53 53 Complex Continuing Care 416 345 288 288 Local Rehabilitation 22 22 85 85 Regional Rehabilitation*** -- -- 17 17 Transition-to-Independent Living -- -- ***5 5 Sub-Acute Care -- -- 82 82 Total 1,393 1,201 1,289 1,289 Long-Term Care Beds 2,986 2,986 3,304 3,541 Long-Term Care Places -- -- 1,387 1,387 ICUs (included in acute) 51 51 43 43 Operating Rooms 30 30 18 18 Procedure Rooms -- -- 13 13 * Estimate based on clinical efficiencies applied only to urban hospitals, rural hospitals maintained at 1997-98 bed numbers ** Estimate only for purposes of sizing physical plant (acute bed growth has only been applied to non-rural hospitals, rural efficiencies and growth will be applied in Stage 2) *** To be located in Hamilton
Costs and Savings Capital Costs Capital estimates for new construction, renovations, ancillary costs and site development amount to $66.84 million. In addition, the estimated capital requirements for the cancer treatment centre in St. Catharines, scheduled for 2005, totals $20.75 million. Operating Costs The net expense budget for the Niagara Region hospitals has been calculated to be $255 million. Savings amount to $29.7 million or 11.5%. These savings include complex continuing care and are not in excess of reductions which have taken place after 1995/96. These savings also do not reflect any changes that may still need to occur in rural hospitals in the region. The revised net expenses for Niagara Region amount to $228.6 million.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
41
Reinvestment The HSRC is recommending reinvestment in the necessary infrastructure and training to create a regional information system capable of linking all providers in hospitals, organized group practices, community agencies and laboratories along with individual practitioners. This reinvestment amount required is as yet to be determined. The total reinvestment estimated to be required for Niagara Region is $56.6 – $56.8 million, including $28.6 million for long-term care, $7.7 million for mental health, $6.3 million for rehabilitation, $6.3 million for sub-acute care, $6 million for home care and between $0.7 , $0.9 million for joint replacement and $1 million for the operating costs of the MRI. The following table shows the breakdown of reinvestment: Reinvestment Summary
Service Reinvestment Home Care $6.0 million Long-Term Care $28.6 million Sub-Acute Care $6.3 million Mental Health $7.7 million Rehabilitation $6.3 million Joint Replacement $0.7 – 0.9 million Magnetic Resonance Imaging Up to $1 million Information Technology TBD TOTAL $56.6 – 56.8 million
Governance and Management Since the release of the October 1998 report, the Minister of Health has accepted the advice of the HSRC and has announced the decision to close Maple Hurst Private hospital in Thorold. West Lincoln Memorial Hospital will continue to be linked to the Hamilton Health Sciences Corporation through its management contract. The Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines will maintain its governance and manage the long-term mental health services and ambulatory services located at the Hôtel Dieu site. The HSRC intends to direct St. Catharines General, Greater Niagara General, Niagara-on-the-Lake, Shaver, Niagara Rehabilitation, Welland County, Port Colborne General and Douglas Memorial hospital boards to amalgamate to become the Niagara Health Care System. This will include Standing Committees for the rural hospitals in Niagara-on-the-Lake, Port Colborne and Fort Erie and the amalgamated Shaver/Niagara Rehabilitation Centre site. The Niagara Health Care System and the Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines will be directed to form a Joint Executive Committee (JEC) with a single medical staff and Medical Advisory Committee (MAC). The JEC will permit joint decision -C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
42
making for the full range of ambulatory care services that are intricately connected with the inpatient services provided on the General site in St. Catharines. Human Resources Impact The restructuring of hospital services in Niagara Region will have a significant impact on care providers and workers within the health system. All hospitals in the Niagara Region in conjunction with employee representatives will need to develop a comprehensive labour adjustment plan. The purpose of the human resource plan is to provide a measure of security to those employees most likely to be affected by the hospital restructuring. The agreement deals with program transfers, job posting, dispute resolution process, job security measures, and a communication plan. The agreement will be in effect until 90 days following the last rationalization or consolidation or on April 30, 2000, whichever comes first. There is a provision for the parties to extend the agreement. The significance of this agreement should not be understated and clearly indicates the level of cooperation and commitment to restructuring by the Niagara Region. Summary of Niagara Region’s Hospitals’ Roles The following table summarized the roles and corporate status of each of the hospital sites in Niagara.
ACUTE CARE HOSPITALS Hospital
Site Status of Site
Health Services Restructuring Commission Decisions
Status of Corporate Entity /Governance
Douglas Memorial Hospital
Retain Will retain current acute and chronic beds emergency and ambulatory services Further decisions pending Stage 2 of HSRC’s consideration of the Rural and Northern Health Care Framework
Amalgamated under Niagara Health Care System Board (NHCS) Standing Committee of the NHCS Board
Greater Niagara General Hospital
Retain Will retain acute care, emergency and ambulatory care services Will acquire rehabilitation and sub-acute care beds Will continue to provide acute mental health and complex continuing care services
Amalgamated under Niagara Health Care System Board
Hôtel Dieu Hospital St. Catharines
Retain The Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines manage long-term mental health services and ambulatory services in St. Catharines at the Hôtel Dieu site.
Independent governance & management retained by Religious Hospitallers of St. Joseph of the Hôtel Dieu of St. Catharines; to form a Joint Executive Committee, single medical staff and single MAC with NHCS
Niagara-on-the-Lake Hospital
Retain Will retain current acute and chronic beds emergency and ambulatory services Further decisions pending Stage 2 of HSRC’s consideration of the Rural and Northern Health Care Framework
Amalgamated under Niagara Health Care System Board Standing Committee of the NHCS Board
Port Colborne Retain Will retain current acute and chr onic beds Amalgamated under Niagara Health
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
43
General Hospital
emergency and ambulatory services Further decisions pending Stage2 of HSRC’s consideration of the Rural and Northern Health Care Framework
Care System Board Standing Committee of the NHCS Board
St. Catharines General Hospital
Retain Single site for all acute care, emergency and cancer care services in St. Catharines
Amalgamated under Niagara Health Care System Board
Welland County General Hospital
Retain Will retain acute care, emergency and ambulatory care services Will acquire rehabilitation & sub-acute care beds Will continue to provide acute mental health and complex continuing care services
Amalgamated under Niagara Health Care System Board
West Lincoln Memorial Hospital
Retain Will retain current acute and chronic beds emergency and ambulatory services Further decisions pending Stage 2 of HSRC’s consideration of the Rural and Northern Health Care Framework
Maintain its management contract with the Hamilton Health Sciences Corporation
COMPLEX CONTINUING CARE AND REHABILITATION HOSPITALS Maple Hurst Private Hospital
Close No future role Ceases to exist.
Niagara Rehabilitation Centre
Retain Will continue to provide outpatient rehabilitation services
Amalgamated under NHCS Board Standing Committee of the NHCS Board for Complex Continuing Care & Rehabilitation Services
Shaver Hospital Retain
Will provide complex continuing care and rehabilitation services
Amalgamated under NHCS Board Standing Committee of the NHCS Board for Complex Continuing Care & Rehabilitation Services
Conclusion A great deal of local effort and energy has already gone into plans for restructuring in Niagara, especially on the part of the Niagara District Health Council and its Steering Committee on restructuring. The HSRC notes that there is a high level of awareness in the community as to the issues of fragmentation and lack of critical mass in existing health care services. The HSRC believes that its directions will facilitate progress toward the integrated, coordinated system of health care that Niagara needs to make the best use of its resources. One outcome of this restructuring will be to provide more stable professional resources in Niagara’s health services and this too will contribute to better quality health care services. The challenge that lies before Niagara Region and other communities across the province is not to be underestimated. Managing the process of change at the community level will require the collective involvement and commitment of everyone who values our health system. The HSRC believes that its final directions will facilitate positive change in the hospital system, both to maintain and improve patient care and to address future financial challenges. The directions also establish a solid foundation for the system-wide integration of hospital services, resulting in more efficient patient care for the residents of Niagara Region. C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Region Health Services Restructuring Report, March 1999
44
The task will not be an easy one. The HSRC’s expectation is that the community will work together and bring about the changes necessary to create workable solutions to health care reform.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
45
APPENDIX 1: CAPITAL ESTIMATES Assumptions: 1. For new acute care construction, where there is a balance (50:50) between space allocated to
high cost items (e.g., Emergency, NICU, Surgical Su ite, and Critical Care) and moderate/low cost items (e.g., Administrative, Materials Management, etc.) a blended rate of $187 per square foot will be applied.
2. For new acute care construction, where more than 50% of the space is high cost, a rate of $210/sf will be applied.
3. For new acute care construction, where more than 50% of the space is lower cost space, $160/sf will be used.
4. New construction for mental health will be applied at a rate of $140/sf (excluding medium secure forensic unit, which will be $170/sf).
5. New construction for rehabilitation beds will be applied at a rate of $160/sf.
6. New construction for complex continuing care beds will be applied at a rate of $160/sf.
7. Renovation costs will be calculated as follows:
moderate level of renovations moderate $100/sf significant level of renovations high $150/sf very high level of technologically complex
renovations very high $180/sf light renovations light $50/sf
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
46
City: Niagara Region Hospital: St Catherines General Option : Final Directions
Program Beds Area/Bed Area Required
Beds Available 357 Required 385Additional Needed 28
Target Area Acute 303 1,400 424,200 sf Mental Health 35 1,100 38,500 sf Continuing Complex Care - 1,000 - sf Rehabilitation 11 1,100 12,100 sf Sub-Acute Care 36 1,000 36,000 sfTotal 385 510,800 sfResearch - - sfAcademic Allocation - 10,000 sfGFT - - sfTOTAL 520,800 sf
Area Available Whole Hospital, excluding Residence (93,000 sf) 434,295 sfTotal 434,295 sf
Guideline Area Difference 76,505 sf
Focus of New Construction Capacity cgsf bgsf cost/bgsf Total New Space for activity displaced for Emerg expnsn 2,000 2,530 160 $404,800 Acute/Sub-Acute, beds (L3/4) 53 18,550 23,466 187 $4,388,095 Rehabilitation, beds (L3/4) 11 4,675 5,914 160 $946,220 Surgical Suite, expansion, OR's (L5) 2 4,000 5,060 210 $1,062,600 Expanded Surgical Suite Support (L5) 4,000 5,060 210 $1,062,600 Day Surgery, increment to serve 9 OR's 2,000 2,530 187 $473,110 Ambulatory programs, expansion (L1) 5,000 6,325 160 $1,012,000 Diagnostic Imaging exapansion (L1) 5,000 6,325 210 $1,328,250 Expanded clinical and general support (G) 10,000 12,650 187 $2,365,550 Space for transferred academic activity (L2) 10,000 12,650 160 $2,024,000 Other, temporary and permanent links 10,000 12,650 100 $1,265,000
Cancer Centre, 3 bunkers $15,547,175 --basic space 47,000 59,455 210 $12,485,550 --bunker area 4,500 5,693 450 $2,561,625 -- tunnel connection to hospital $500,000
Total 126,725 160,307 $31,879,400
Focus of Renovation Area (sf) Renovation (m,h,vh,l) Cost/sf Total Reno. Emergency, expansion for 60,000 visits 2,000 h $150 $300,000 Emergency, integration 2,000 h $150 $300,000 Other functions displaced from Leonard 10,000 m $100 $1,000,000 Surgical Suite integration 8,000 h $150 $1,200,000 Mental Health expansion, 17 beds 7,225 h $150 $1,083,750 Miscellaneous links to new construction 2,000 h $150 $300,000
Hospital support areas enhanced for Cancer Centre -- Higher cost areas, eg Diagnostic Imaging 2,000 h $150 $300,000 --Moderate cost areas, eg Pharmacy 3,000 m $100 $300,000Total 36,225 $4,783,750
Total Construction Cost $36,663,150Ancillary Costs @ 23.2% $8,505,851Demolition part Leonard, 20,000 sf $200,000Demolition School of Nursing and Residence, 93,550 sf $860,000Site Development Allowance $2,775,176Furnishings & Equipment Allowance (out of contract) $7,332,630TOTAL COST $56,336,807
Notes1) Hotel Dieu with LT Mental Health, Urgent Care (30,000 visits) and Ambulatory Care ( 87,500 visits).2) Assumes demolition of part Leonard but retention of cafeteria and kitchen.3) Emergency expanded by creation of "Fast track" which may not be adjacent to present department.4) Assumes two OR's reactivated as well as new additional OR's.5) Most existing acute beds back in service.6) Mental Health inpatients expanded in present space.7) No allowance for parking.8) Assumes HDH and non-hospital programs in houses (detox, DEC, Addiction Recovery etc) remain in place.9) Site Development Allowance includes component to increase site transformer capacity.10) Assumes removal of School of Nursing for Cancer Centre; Residence could be removed if needed.11) Equipment cost excludes radiotherapy and related equipment.12) No allowance for additional consolidation of Laboratory and Food Service.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
47
City: Niagara Region Hospital: Hotel Dieu Option : Final Directions
Program Beds Area/Bed Area Required
Beds Available 211 Required 53 Additional Needed 158-
Target Area Acute - 1,400 - sf Mental Health, Longer Term 53 1,100 58,300 sf Continuing Complex Care - 1,000 - sf Rehabilitation - 1,100 - sf Sub-Acute Care - 1,000 - sfTotal 53 58,300 sfResearch - - sfAcademic Allocation - - sfGFT - - sfTOTAL 58,300 sf
Area Available Building/Wing 206,448 sf
Total 206,448 sf
Guideline Area Difference 148,148- sf
Focus of New Construction Capacity cgsf bgsf cost/bgsf Total New- - $0- - $0
Other - - $0Total - - $0
Focus of Renovation Area (sf) Renovation (m,h,vh,l) Cost/sf Total Reno. Conversion, bed space for MH, 53 beds 22,525 m $100 $2,252,500 Conversion, MH program space 10,600 m $100 $1,060,000 Dialysis expansion 11,000 vh $180 $1,980,000 Dialysis, integration of existing 7,000 l $50 $350,000 Oncology expansion 3,000 h $150 $450,000 Oncology, integration of existing 7,000 l $50 $350,000 Ambulatory Care increment 17,000 h $150 $2,550,000Total 78,125 $8,992,500
Total Construction Cost $8,992,500Ancillary Costs @ 23.2% $2,086,260Site Development AllowanceFurnishings & Equipment Allowance (out of contract) $1,798,500TOTAL COST $12,877,260
Notes1) Hotel Dieu with LT Mental Health, Urgent Care (30,000 visits) and Ambulatory Care ( 87,500 visits).2) All surgery at SCGH.3) Available space excludes the Ambulance Facility, but includes outlying houses used for hospital purposes.4) Assumes Dialysis and Oncology stay at HDH but expanded for future growth.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
48
City: Niagara Region Hospital: Shaver Option : Final Directions
Program Beds Area/Bed Area Required
Beds Available 124 Required 158 Additional Needed 34
Target Area Acute - 1,400 - sf Longer Term Mental Health - 1,100 - sf Continuing Complex Care 124 1,000 124,000 sf Rehabilitation 34 1,100 37,400 sf Sub-Acute Care - 1,000 - sfTotal 158 161,400 sfResearch - - sfAcademic Allocation - - sfGFT - - sfTOTAL 161,400 sf
Area Available Main Hospital Building 88,657 sf ( Ancillary buildings, houses etc 36,864 )sfTotal 88,657 sf
Guideline Area Difference 72,743 sf
Focus of New Construction Capacity cgsf bgsf cost/bgsf Total New Expanded Complex Continuing Care, beds 22 9,350 11,828 160 $1,892,440 Rehabilitation, 34 bed total 12 5,100 6,452 160 $1,032,240 Expanded general support, eg Pharmacy 2,000 2,530 160 $404,800 Electrical Service upgrade, allowance $100,000 Other, links, displacements etc 2,000 2,530 140 $354,200Total 18,450 23,339 $3,783,680
Focus of Renovation Area (sf) Renovation (m,h,vh,l) Cost/sf Total Reno.$0
Links, integration 3,000 m $100 $300,000$0
Total 3,000 $300,000
Total Construction Cost $4,083,680Ancillary Costs @ 23.2% $947,414Site Development Allowance $189,184Furnishings & Equipment Allowance (out of contract) $567,552TOTAL COST $5,787,830
Notes1) Hotel Dieu with LT Mental Health, Urgent Care (30,000 visits) and Ambulatory Care ( 87,500 visits).
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
49
City: Niagara Region Hospital: GNGH Option : Final Directions
Program Beds Area/Bed Area Required
Beds Available 311 Required 241 Additional Needed 70-
Target Area Acute 134 1,400 187,600 sf Mental Health 20 1,100 22,000 sf Continuing Complex Care 52 1,000 52,000 sf Rehabilitation 20 1,100 22,000 sf Sub-Acute Care 15 1,000 15,000 sfTotal 241 298,600 sfResearch - - sfAcademic Allocation - - sfGFT - - sfTOTAL 298,600 sf
Area Available Main Hospital 251,600 sf
Total 251,600 sf
Guideline Area Difference 47,000 sf
Focus of New Construction Capacity cgsf bgsf cost/bgsf Total New Emergency, expansion, 63,728 total visits 6,800 8,602 210 $1,806,420 Complex Continuing Care, expansion, beds 12 5,100 6,452 160 $1,032,240 Rehabilitation Inpatient, beds 20 8,500 10,753 160 $1,720,400 Other - - $0Total 20,400 25,806 $4,559,060
Focus of Renovation Area (sf) Renovation (m,h,vh,l) Cost/sf Total Reno. Emergency, integration 5,000 h $150 $750,000 Emergency, integration 5,000 l $50 $250,000 Ambulatory Care increment 500 h $150 $75,000 Links to new construction 1,000 h $150 $150,000Total 11,500 $1,225,000
Total Construction Cost $5,784,060Ancillary Costs @ 23.2% $1,341,902Site Development Allowance $227,953Demolition, Simpson Wing/Health Unit, 20,000 sf $160,000Furnishings & Equipment Allowance (out of contract) $1,156,812TOTAL COST $8,670,727
Notes1) Hotel Dieu with LT Mental Health, Urgent Care (30,000 visits) and Ambulatory Care ( 87,500 visits).2) Assumes construction of a new 32-bed unit for Rhabilitation and increased Complex Continuing Care.3) Sub-acute to vacant/vacated acute beds.4) Assumes 5 operating rooms required in future.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Region Health Services Restructuring Report, March 1999
50
City: Niagara Region Hospital: Welland Option : Final Directions
Program Beds Area/Bed Area Required
Beds Available 361 Required 205 Additional Needed 156-
Target Area Acute 106 1,400 148,400 sf Mental Health 20 1,100 22,000 sf Continuing Complex Care 46 1,000 46,000 sf Rehabilitation 20 1,100 22,000 sf Sub-Acute Care 13 1,000 13,000 sfTotal 205 251,400 sfResearch - - sfAcademic Allocation - - sfGFT - - sfTOTAL 251,400 sf
Area Available Main Hospital Building 278,106 sf Maclean Residence 28,500 sfTotal 306,606 sf
Guideline Area Difference 55,206- sf
Focus of New Construction Capacity cgsf bgsf cost/bgsf Total New Emergency, expanded for 37,221 total visits 4,200 5,313 210 $1,115,730 Ambulatory Care expansion, expanded visits 2,140 535 677 187 $126,557Total 4,735 5,990 $1,242,287
Focus of Renovation Area (sf) Renovation (m,h,vh,l) Cost/sf Total Reno. Emergency integration 5,000 h $150 $750,000 Expansion of Mental Health, 4 beds 1,700 h $150 $255,000 Displaced Mental Health outpatient space 1,700 m $100 $170,000 Displacements to recover CCC beds 2,000 m $100 $200,000Total 10,400 $1,375,000
Total Construction Cost $2,617,287Ancillary Costs @ 23.2% $607,211Site Development Allowance $124,229Furnishings & Equipment Allowance (out of contract) $523,457TOTAL COST $3,872,184
Notes1) Hotel Dieu with LT Mental Health, Urgent Care (30,000 visits) and Ambulatory Care ( 87,500 visits).2) "Area Available" excludes Extended Care Unit of 34,650 sq feet.3) Assumes rehabilitation beds to recovered Chronic/Complex Care.4) Assumes sub-acute care to vacant Acute Care beds.5) Assumes expansion of Mental Health will displace MH outpatient program.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
ST. CATHARINES GENERAL HOSPITAL THE HEALTH SERVCIES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the St. Catharines General Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System”8. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
8 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Serv ices Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

St. Catharines General Hospita l
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 9 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
9 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission. The Health Services Restructuring Commission further directs the St. Catharines General to take all proceedings, corporate and otherwise, to implement such directions.
The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Report dated March 1999 that has been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: St. Catharines General Hospital 142 Queenston St. St. Catharines, ON L2R 7C6
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH CONCERNING ST. CATHARINES GENERAL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and
administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $59,686,362 Transfer of expenses to amalgamated hospital $59,686,362 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the St. Catharines General Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Catharines General Hospita l
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999.
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
GREATER NIAGARA GENERAL HOSPITAL
THE HEALTH SERVCIES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED TH E REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Greater Niagara General Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the St. Catharines Genera l Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System” 10. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
10 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
2
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following: • approving any decisions to eliminate inpatient or emergency services at any of
the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commiss ion and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
3
2. Pending the amalgamation and with all Niagara region hospitals, and with representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 11 and the majority
11 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
4
of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
6. In conjunction with all of the Niagara region hospitals develop and begin
implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
9. By April 30, 1999 Establish a Steering Committee to oversee the management of the debt. This Steering Committee will report to the Niagara Health Care System Board once established and will be responsible for ensuring the implementation of the recommendations of the operational review of the GNGH.
The Health Services Restructuring Commission further directs the Greater Niagara General Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Greater Niagara General Hospital 5546 Portage Road P. O. Box 1018 Niagara Falls, ON L2E 6X2
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING THE GREATER NIAGARA GENERAL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and progr am transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $49,510,376 Transfer of expenses to amalgamated hospital $49,510,376 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Greater Niagara General Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

The Greater Niagara General Hospital
2
Accompanying this Advice is: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO
THE WELLAND COUNTY GENERAL HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the St. Catharines General Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, St.Catharines General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System”12. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
12 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contribut ions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater N iagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with
representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Welland County General Hospital
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 13 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
13 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Welland County General Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directio ns are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that has been prepared by the Health Services Restructuring Commiss ion. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Welland County General Hospital 63 Third Street Welland, ON L3B 4W6
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE
MINISTER OF HEALTH CONCERNING WELLAND COUNTY GENER AL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and
administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $45,476,832 Transfer of expenses to amalgamated hospital $45,476,832 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Welland County General Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Welland County General Hospital
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
PORT COLBORNE GENERAL HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Port Colborne General Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, St. Catharines General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System” 14. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
14 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether
to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with
representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Port Colborne General Hospital
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 15 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
15 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above direct ions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Port Colborne General Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Port Colborne General Hospital 260 Sugarloaf Street Port Colborne, ON L3K 2N7
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING PORT COLBORNE GENERAL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $11,551,874 Transfer of expenses to amalgamated hospital $11,551,874 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Port Colborne General Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Port Colborne General Hospital
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
NOTICE OF INTENTION TO ISSUE DIRECTIONS TO THE NIAGARA-ON-THE-LAKE HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Niagara-on-the-Lake Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, St. Catharines General Hospital, Port Colborne General Hospital, Douglas Memorial Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System” 16. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision
of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
16 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and prior ities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with
representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara-on-the-Lake Hospital
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or
cluster of hospitals; ⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals
develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 17 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
17 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Niagara-on-the-Lake Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; 3. A copy of the Niagara Region Health Services Restructuring Report, March1999
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Niagara-on-the-Lake Hospital Box 1270
176 Wellington Street Niagara-on-the-Lake, ON L0S 1J0
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING NIAGARA-ON-THE-LAKE HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $3,565,330 Transfer of expenses to amalgamated hospital $3,565,330 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Niagara-on-the-Lake Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara-on-the-Lake Hospital
2
Accompanying this Notice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
DOUGLAS MEMORIAL HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Douglas Memorial Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, St. Catharines General Hospital, Niagara-on-the-Lake Hospital, Port Colborne General Hospital, Shaver Hospital and the Niagara Rehabilitation Centre to amalgamate into one corporation the “Niagara Health Care System”18. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision
of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, miss ion and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
18 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emerge ncy services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with
representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Douglas Memorial Hospital
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or
cluster of hospitals; ⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals
develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 19 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
19 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Douglas Memorial Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Douglas Memorial Hospital 230 Bertie Street Fort Erie, ON L2A 1Z2
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING DOUGLAS MEMORIAL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $10,307,393 Transfer of expenses to amalgamated hospital $10,307,393 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Douglas Memorial Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Douglas Memorial Hospital
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

West Lincoln Memorial Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE WEST LINCOLN MEMORIAL HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the West Lincoln Memorial Hospital to:
1. Review the contract between West Lincoln Memorial Hospital and the Hamilton
Health Science Centre in the context of the HSRC’s approach to the Rural and Northern Health Care Framework to ensure that this contract meets the principles of this framework.
Any revisions to the current contract must be submitted to the Health Services Restructuring Commission and Minister of Health by May 31, 1999.
2. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
3. In conjunction with the Hamilton Health Science Centre develop and begin
implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

West Lincoln Memorial Hospital
2
provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. In conjunction with all of the Niagara region hospitals and the Hamilton Health
Sciences Centre develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
5. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
The Health Services Restructuring Commission further directs the West Lincoln Memorial Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

West Lincoln Memorial Hospital
3
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: West Lincoln Memorial Hospital 169 Main St. E. Grimsby, ON L3M 1P3
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

West Lincoln Memorial Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING WEST LINCOLN MEMORIAL HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
West Lincoln Memorial HospitalTotal Budget 1995/96 Net Expense $12,815,636Less Selected Expenses -$1,936,975Total Program Transfers $0Total Clinical Efficiencies $0Total Support Service Efficiencies $0Re-allocation of Other Expenses $276,840Site Closures $0Total Administrative Efficiencies $0Add Selected Expenses $1,936,975Sub-Total for West Lincoln Memorial Hospital $13,092,476
Revised Total Operating Expense $13,092,476Change in Operating Net Expense $276,840Percent Change in Net Expenses 2.2%
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

West Lincoln Memorial Hospital
2
Accompanying this Advice are: 1. Copies of the Notice(s) of the Intention to Issue Directions to the hospitals in Niagara
region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
NIAGARA REHABILITATION CENTRE
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Niagara Rehabilitation Centre to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, St. Catharines General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Port Colborne General Hospital to amalgamate into one corporation the “Niagara Health Care System” 20. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision
of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Nia gara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
20 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
2
• approving any decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community served;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital bo ards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System.
The plan must be submitted to the Health Services Restructuring Commission and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with
representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Rehabilitation Centre
3
Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or
cluster of hospitals; ⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals
develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 21 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
21 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
4
6. In conjunction with all of the Niagara region hospitals develop and begin implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Niagara Rehabilitation Centre to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Niagara Rehabilitation Centre 547 Glenridge Avenue St. Catharines, ON L2T 4C2
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING NIAGARA REHABILITATION CENTRE
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $4,456,405 Transfer of expenses to amalgamated hospital $4,456,405 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Niagara Rehabilitation Centre should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Rehabilitation Centre
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO
THE SHAVER HOSPITAL
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Shaver Hospital to: 1. Develop a plan, led by a facilitator appointed by the Health Services Restructuring
Commission, in conjunction with the Greater Niagara General Hospital, Welland County General Hospital, St. Catharines General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and the Port Colborne General Hospital to amalgamate into one corporation the “Niagara Health Care System” 22. The plan will:
a) provide for the creation of a new corporate structure that will govern the provision
of hospital-based inpatient and outpatient services currently provided at the St. Catharines General, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre;
b) include a statement of vision, mission and core values for the new corporate structure;
c) create four Standing Committees of the Board for the communities of Fort Erie, Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
22 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
2
• approving any decisions to eliminate inpatient or emerge ncy services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advising the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility; • appointing a local advisory committee to the medical advisory committee of
the Niagara Health Care System; and • participating in the negotiation of partnership arrangements with other local
health service providers.
d) Develop the criteria to be applied by the standing committees in deciding whether to approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
e) outline the structure, composition and membership of the new corporate structure taking into consideration the demographic, cultural, linguistic, religious, economic, geographic, ethnic and social characteristics of the community ser ved;
f) ensure that members of the new corporate structure have experience and expertise in governing health services for the communities which they serve;
g) take into account the contributions of the existing hospital boards as an important foundation in the creation of the new corporate structure;
h) include guidelines for the selection of the initial and subsequent board of directors;
i) consistent with the mission, vision, values and priorities of the new corporate structure, include principles to guide the appointment of administrative and medical leadership;
j) propose the relationship of the new corporate structure to charitable foundations related to St. Catharines General Hospital, Greater Niagara General Hospital, Welland County General Hospital, Port Colborne General Hospital, Niagara-on-the-Lake Hospital, Douglas Memorial Hospital, Shaver Hospital and Niagara Rehabilitation Centre; and,
k) confirm a name for the Niagara Health Care System. The plan must be submitted to the Health Services Restructuring Commissio n and Minister of Health by June 30, 1999. The amalgamation of the hospitals shall occur no later than September 30, 1999.
2. Pending the amalgamation and with all Niagara region hospitals, and with representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services Restructuring Commission’s directions on the hospitals’ employees. The plan must
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
3
include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
3. Pending the amalgamation and in conjunction with all Niagara region hospitals
develop and begin implementation by August 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
4. Develop a plan by September 20, 1999, for Stage II of the HSRC’s approach to Rural
and Northern Health Care Framework. The terms of reference for the network plan should address:
a) Sizing and siting of acute and non-acute services; b) To identify linkages with regional referral centres and ensure access to
tertiary/quaternary services; c) Development of stronger partnerships with other health providers and
organizations in the network to provide a better continuum of care (i.e. patient centered approach.)
5. Develop by December 31, 1999, with the Hotel Dieu Hospital St. Catharines, a plan
for consolidation of all inpatient acute care and emergency care in St. Catharines at the St. Catharines General site of the Niagara Health Care System 23 and the majority of ambulatory services, including day surgery and urgent or prompt care services, at the Hotel Dieu Hospital by March 31, 2001.
6. In conjunction with all of the Niagara region hospitals develop and begin
implementation by no later than June 30, 1999 of a plan for the provision of
23 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
4
laboratory services that is consistent with the directions of the Ministry of Health’s Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
8. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets out of the ordinary course of business to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Shaver Hospital to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Report dated October, 1998 and March, 1999 that has been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
5
DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Shaver Hospital 541 Glenridge Avenue St. Catharines, ON L2T 4C2
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING SHAVER HOSPITAL
1. The funding allocation to the hospital be adjusted to reflect the clinical and administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
1995/96 net expenses $11,029,280 Transfer of expenses to amalgamated hospital $11,029,280 Savings derived from these expenses will be realized in the Niagara Health Care System.
2. Effective October 1, 1999 funding to the Shaver Hospital should be transferred to the Niagara Health Care System.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Shaver Hospital
2
Accompanying this Advice are: 1. Copies of the Directions to the hospitals in Niagara region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission. DATED at Toronto this 9th day of March, 1999
__________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DIRECTIONS TO THE
HOTEL DIEU HOSPITAL ST. CATHARINES
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the Hotel Dieu Hospital St. Catharines to: 1. Pass a by-law to appoint by September 30, 1999 the executive committee of the
hospital’s board of directors to the joint executive committee and delegate to the executive committee the powers to make decisions on behalf of the hospital to implement the HSRC directions.
2. Led by a facilitator appointed by the Commission develop a plan with the Niagara
Health Care System, once formed, to create a Joint Executive Committee between the Hotel Dieu Hospital and the Niagara Health Care System by December 31, 1999. The JEC will:
a) Develop and implement a plan for a common medical staff between the St.
Catharines General site of the Niagara Health Care System and the Hotel Dieu Hospital.
b) Coordinate the plannin g and delivery of services between the Hotel Dieu Hospital and the Niagara Health Care System.
c) Implement the plan to transfer services between the St. Catharines General site of the Niagara Health Care System and the Hotel Dieu Hospital in accordance with the roles assigned by the Commission.
d) Jointly develop a task force with the Niagara Health Care System directed at strengthening academic programs in the Region’s hospitals. The task force will include representation from both University of Western Ontario and McMaster University and will be responsible for:
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
2
• developing a plan to enhance the scope of clinical teaching in the Niagara Region and the role of Niagara Health Care System and hotel Dieu hospital
• developing a medical credentialling process that reco gnizes and fosters the need to have a cadre of geographic full-time physicians (GFT) to improve overall quality of care;
• developing strategies to nurture a research environment in both hospitals 3. In conjunction with the Niagara Health Care System, develop a plan by December 31,
1999 to transfer all inpatient services to the St. Catharines General site of the Niagara Health Care System24 and receive the majority of ambulatory care services from St. Catharines General site by March 31, 2001.
4. Pending the amalgamation and with all Niagara region hospitals, and with representatives of affected employees develop and begin implementation by July 1, 1999 of a human resources plan that will address the impact of the Health Services Restructuring Commission’s directions on the hospitals’ employees. The plan must include, at a minimum, the following components:
⇒ the process for dealing with human resources issues common to all hospitals or cluster of hospitals;
⇒ a dispute resolution mechanism; ⇒ the establishment of a jobs registry; ⇒ the governance structure of the jobs registry and the participation of employee
representatives in the governance structure; ⇒ the mandatory participation of the hospitals in the jobs registry and any other jobs
registry and processes agreed to by the hospitals and employee representatives; and
⇒ the funding plan for the registry.
The plan is to be submitted to both the Minister of Health and the Health Services Restructuring Commission.
5. Develop and begin implementation by July 1, 1999, of a plan to maximize the efficiency of the delivery of administrative services, support services and diagnostic services. The plan must address alternative service delivery systems, including services that can be provided by the private sector. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission by June 30, 1999.
6. In conjunction with all of the Niagara region hospitals develop and begin
implementation by no later than June 30, 1999 of a plan for the provision of laboratory services that is consistent with the directions of the Ministry of Health’s
24 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Corporation.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
3
Laboratory Reform Strategy. Submit a copy of the plan to both the Minister of Health and the Health Services Restructuring Commission.
7. Develop a plan to receive 53 long term mental health beds and associated outpatient
services transferred from the St. Joseph’s Hospital (which will receive the Hamilton Psychiatric Hospital’s programs) by March 31, 2001. The plan must be developed by December 31, 1999 and submitted to the Ministry of Health.
8. Prepare and submit to the Minister of Health a plan that outlines will renovations to
the inpatient areas to accommodate 53 long-term mental health beds and expansion of ambulatory care areas by December 31, 1999. The total budget for the construction project including equipment and furnishings should be set at a maximum of $12.9 million.
9. Establish a task force made up of the Niagara Health Care System, the Hotel Dieu
Hospital, local medical societies, McMaster University and Univ ersity of Western Ontario to develop a plan to recruit and retain family physicians and designated specialty physicians to the region.
10. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program transfer plan. The first report is to be received at the latest July 31, 1999 for the period ending June 30, 1999.
11. By April 30, 1999 pass a resolution that would prohibit the transfer of any hospital
funds and assets outside of the regular business of the hospital to any related hospital foundation or any other person without a further direction from the Health Services Restructuring Commission.
The Health Services Restructuring Commission further directs the Hotel Dieu Hospital St. Catharines to take all proceedings, corporate and otherwise, to implement such directions. The Health Services Restructuring Commission’s reasons for these Directions are based on the Commission’s review of health services in the Niagara region as outlined in the Niagara Region Health Services Restructuring Reports dated October, 1998 and March, 1999 that have been prepared by the Health Services Restructuring Commission. Accompanying these Directions are: 1. Copies of the Directions to the other hospitals in the Niagara region; 2. Copies of the advice that the Health Services Restructuring Commission has provided
to the Minister of Health of Ontario; and 3. A copy of the Niagara Region Health Services Restructuring Report (March, 1999)
prepared by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
4
DATED at Toronto this 9th day of March, 1999
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: Hotel Dieu Hospital 155 Ontario Street St.Catharines, ON L2R 5K3
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH
CONCERNING HOTEL DIEU HOSPITAL ST. CATHARINES 1. The funding allocation to the hospital be adjusted to reflect the clinical and
administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
Hôtel DieuTotal Budget 1995/96 Net Expense $49,586,715Less Selected Expenses -$1,750,185Total Program Transfers $613,509
Transfer of inpatient activity from Hôtel Dieu to SCGH -$17,482,204Transfer of day surgery, emergency and ambulatory care from SCGH to Hôtel Dieu $10,939,777Mental Health Restructuring Allocation $7,464,200Transfer of Materiels Management -$308,263
Total Clinical Efficiencies $0Total Support Service Efficiencies -$783,792
Net Clinical Lab Efficiencies -$320,477Net Food Services Efficiencies -$273,414Discount for Clinical Eff. $47,266Net Materials Mgmt Efficiencies -$237,167
Re-allocation of Other Expenses $0Total Administrative Efficiencies -$536,715Add Selected Expenses $2,022,596Sub-Total for Hôtel Dieu $49,152,129
Revised Total Operating Expense $49,152,129Change in Operating Net Expense -$434,586Percent Change in Net Expenses -0.9%
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Hotel Dieu Hospital, St. Catharines
2
Accompanying these Directions are: 1. Copies of the Directions to the hospitals in the Niagara Region and; 2. A copy of the Niagara Region Health Services Restructuring Report dated March,
1999 prepared by the Health Services Restructuring Commission . DATED at Toronto this 9th day of March, 1999
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Advice to Minister of Health
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MINISTER OF HEALTH CONCERNING REINVESTMENT AND OTHER RESTRUCTURING ISSUES IN
THE NIAGARA REGION HEALTH CARE SYSTEM Captial 1. The Niagara Health Care System should be given approval to plan for a capital
construction project including: construction of a 3-bunker regional cancer centre, consolidation of all acute beds at the St. Catharines General site, and renovations to the Shave, Welland General and Greater Niagara General sites. The total budget for the construction should be set at a maximum of $74.8 million including ancillary, site development, and new furnishings and equipment. The cost of the construction project and equipment and furnishings should be funded by the Ministry of Health and the hospital according to prevailing Ministry of Health policy.
2. The Hotel Dieu Hospital should be given approval to plan for a capital construction
project including: renovations to acute care space to develop a 53-bed long-term mental health program and expansion of ambulatory care programs up to a maximum of $12.9 million in total capital costs including ancillary, site development, and new furnishings and equipment. The cost of the construction project and equipment and furnishings should be funded by the Ministry of Health and the hospital according to prevailing Ministry of Health policy.
Reinvestment
1. The Ministry of Health reinvest the following operating funds to mitigate the effects of restructuring of hospital services and address the current gaps in service:
C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Advice to Minister of Health
2
Reinvestment Summary Service Reinvestment
Home Care $6.0 million Long-Term Care $28.6 million Sub-Acute Care $6.3 million Mental Health $7.7 million Rehabilitation $6.3 million Joint Replacement $0.7 – 0.9 million MRI (St. Catharines site) up to $1.0million Information Technology tbd TOTAL $56.6 – 56.8 million
Labour Adjustment 1. Accept a plan for labour adjustment from the Niagara Region by September 30, 1999
and respond to the plan by October 31, 1999.
Mental Health
1. Establish a transitional mental health agency/committee for the central west region to
manage restructuring of mental health services on an interim basis. The agency should include representatives of all services sites, including community service providers.
2. Receive a plan from Hotel Dieu Hospital in cooperation with the St. Joseph’s Hospital Hamilton, a plan to transfer 53 long-term mental health beds and associated outreach activities and funds from the Hamilton Psychiatric Hospital to the Hotel Dieu Hospital no later than by March 31, 2001.
Recruitment of Physicians to the Niagara Region 1. To ensure the Ministry of Health is represented on a task force made up of the
Niagara Health Care System, the Hotel Dieu Hospital, local medical societies, McMaster University and University of Western Ontario to develop a plan to recruit and retain family physicians and designated specialty physicians to the region.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Advice to Minister of Health
3
DATED at Toronto this 9th day of March, 1999.
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block 80 Grosvenor Street Toronto, ON M7A 2C4
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DRAFT
NOTICE OF INTENTION TO ISSUE DIRECTIONS TO THE NIAGARA HEALTH CARE SYSTEM 25
TAKE NOTICE THAT the Health Services Restructuring Commission intends, not earlier than thirty (30) days following the date of service of this Notice, to issue the following Directions to the Board of Directors of the Niagara Health Care System. THE HEALTH SERVICES RESTRUCTURING COMMISSION DIRECTS the Board of Directors of the Niagara Health Care System to: 1a) Create four Standing Committees of the Board for the communities of Fort Erie,
Niagara-on-the-Lake, Port Colborne, and for complex continuing care and rehabilitation which will be responsible for the following:
• approving any decisions to eliminate inpatient or emergency services at any of the
acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake) which approval shall not be unreasonably withheld
• participating in the development of the mission and core values of the Niagara Health Care System;
• participating in the development of the administrative and medical bylaws of the Niagara Health Care System;
• advis ing the Niagara Health Care System on matters pertaining to the nature, funding, quality, accessibility and affordability of services delivered by the local hospital facility;
• participating in the selection of the site administrator for the hospital facility;
25 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
2
• appointing a local advisory committee to the medical advisory committee of the Niagara Health Care System; and
• participating in the negotiation of partnership arrangements with other local health service providers.
1b) Appoint one member of the Board to each Standing Committee established.
1c) Develop the criteria to be applied by the standing committees in deciding whether to
approve decisions to eliminate inpatient or emergency services at any of the acute sites (Port Colborne, Fort Erie, Niagara-on-the-Lake)
2. Develop and submit to the Ministry of Health and the Health Services Restructuring
Commission by December 31, 1999 a plan for the configuration of services on all eight sites (St. Catharines General, Welland County General, Greater Niagara General, Port Colborne General, Niagara-on-the-Lake, Douglas Memorial, Shaver and Niagara Rehabilitation Centre) that, at minimum, meets the following requirements:
⇒ provides access to emergency/urgent care services and related inpatient services
on all sites;
3. Implement a plan to operate a maximum number of 627 acute beds by March 31, 2001, 75 acute mental health beds for adult patients by 2003, 85 rehabilitation beds by 2003, 70 subacute beds by 2003 and 246 complex continuing care beds by 2003.
4. Prepare and submit to the Minister of Health a plan that outlines a capital construction project for the following:
⇒ St. Catharines General site which will consist of new construction for the cancer
centre, expansion of acute care beds, emergency services, rehabilitation, acute mental health and sub-acute beds. The total budget for the construction project should be set at a maximum of $56.4 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $7.3 million.
⇒ Greater Niagara General site which will consist of new construction for the expansion of emergency services, mental health and complex continuing care beds. The total budget for the construction project should be set at a maximum of $8.7 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $1.1 million.
⇒ Welland County General site which will consist of new construction for the expansion of emergency services and mental health beds. The total budget for the construction project should be set at a maximum of $3.9 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $0.5 million.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
3
⇒ Shaver site, which will consist of development of rehabilitation, beds. The total budget for the construction project should be set at a maximum of $5.8 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $0.5 million.
The master plan and related information shou ld be provided to the Ministry of Health by December 31, 1999.
5. Pass a by-law to appoint by September 30, 1999 the executive committee of the
hospital’s board of directors to the joint executive committee and delegate to the executive committee the powers to make decisions on behalf of the hospital that will implement the HSRC directions.
6. Led by a facilitator appointed by the Commission develop a plan with the Niagara
Health Care System, once formed, to create a Joint Executive Committee between the Hotel Dieu Hospital and the Niagara Health Care System by December 31, 1999. The JEC will:
• Develop and implement a plan for a common medical staff between the St.
Catharines General site of the Niagara Health Care System and the Hotel Dieu Hospital.
• Coordinate the planning and delivery of services between the Hotel Dieu Hospital and the Niagara Health Care System.
• Implement the plan to transfer services between the St. Catharines General site of the Niagara Health Care System and the Hotel Dieu Hospital in accordance with the roles assigned by the Commission.
• Jointly develop a task force with the Niagara Health Care System directed at strengthening academic programs in the Region’s hospitals. The task force will include representation from both University of Western Ontario and McMaster University and will be responsible for: • developing a plan to enhance the scope of clinical teaching in the Niagara
Region and the role of Niagara Health Care System and hotel Dieu hospital • developing a medical credentialling process that recognizes and fosters the
need to have a cadre of geographic full-time physicians (GFT) to improve overall quality of care;
• developing strategies to nurture a research environment in both hospitals 7. Establish a task force made up of the Niagara Health Care System, the Hotel Dieu
Hospital, local medical societies, McMaster University and University of Western Ontario to develop a plan to recruit and retain family physicians and designated specialty physicians to the region.
8. Submit to the Health Services Restructuring Commission quarterly progress reports
on the status and implementation of the above directions, including a progress report on the implementation of the human resources adjustment plan, and the program C
opy
for a
rchi
ve p
urpo
ses.
Ple
ase
cons
ult o
rigin
al p
ublis
her f
or c
urre
nt v
ersi
on.
Cop
ie à
des
fins
d’a
rchi
vage
. V
euill
ez c
onsu
lter l
’édi
teur
orig
inal
pou
r la
vers
ion
actu
elle
.

Niagara Health Care System
4
transfer plan. The first report is to be received at the latest January 31, 2000 for the period ending December 31, 1999.
The Health Services Restructuring Commission further directs the Niagara Health Care System to take all proceedings, corporate and otherwise, to implement such direct ions.
The Health Services Restructuring Commission’s reasons for these Directions are included in the Niagara Region Restructuring Report dated October 1998 that has been prepared by the Health Services Restructuring Commission.
Accompanying this Notice are:
1. Copies of the Directions to the other hospitals in the Niagara Region; 2. Copies of the Advice that the Health Services Restructuring Commission has
provided to the Minister of Health of Ontario; 3. Guidelines issued by the Health Services Restructuring Commission for making
representations to the Health Services Restructuring Commission; and 4. A copy of the Niagara region Health Services Restructuring Report dated March
1999 prepared by the Health Services Restructuring Commission. IF YOU WISH TO MAKE REPRESENTATIONS to the Health Services Restructuring Commission with relation to the intended directions, such representations must be received by the Commission
NOT LATER THAN THE CLOSE OF BUSINESS AT 5:00 IN THE AFTERNOON
ON THE THIRTIETH (30th) DAY next following the date that this Notice is served, complying in form to the Guidelines of the Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
5
DATED at Toronto this 9th of March, 1999.
_______________ Chair
Health Services Restructuring Commission 56 Wellesley Street West, 12th Floor Toronto, Ontario M5S 2S3 Tel: (416) 327-5919 Fax: (416) 327-5689 To: Niagara Health Care System
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
DRAFT
NOTICE OF ADVICE TO THE MINISTER OF HEALTH CONCERNING NIAGARA HEALTH CARE SYSTEM26
1. The funding allocation to the hospital be adjusted to reflect the clinical and
administrative efficiencies that will be achieved by the hospital and program transfers. Based on the latest available clinical and service data for 1995/96 the estimated adjustments in the costs of operation are:
26 The name “Niagara Health Care System” is a working title only and should not be taken to be a new name designated by the Health Services Restructuring Commission.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
2
Niagara Health Care SystemTotal Budget 1995/96 Net Expense $180,098,167
St. Catharines General Hospital 1995/96 Net Expense $59,686,362Welland County General 1995/96 Net Expense $45,476,832Greater Niagara General 1995/96 Net Expense $49,510,376Port Colborne General Hospital 1995/96 Net Expense $11,551,874Niagara-on-the-Lake Hospital 1995/96 Net Expense $3,565,330Douglas Memorial Hospital 1995/96 Net Expense $10,307,393
Less Selected Expenses -$10,459,495Total Program Transfers $6,033,484
Transfer of inpatient activity from Hôtel Dieu to SCGH $16,463,141Transfer of day surgery, emergency and ambulatory care from SCGH to Hôtel Dieu -$10,977,592Mental Health Restructuring Allocation $275,394Transfer of Materiels Management $272,541
Total Clinical Efficiencies -$15,295,155Alternative Level of Care -$3,612,925Avoidable Admissions (CMG 851, 910, MNRH) -$238,959Conversion to Day Surgery -$861,764Length of Stay Reduction -$10,581,507
Total Support Service Efficiencies -$3,156,018
Net Clinical Lab Efficiencies -$1,364,714Net Food Services Efficiencies -$1,114,196Discount for Clinical Eff. $197,290Net Materials Mgmt Efficiencies -$874,398
Re-allocation of Other Expenses $793,750Total Administrative Efficiencies -$5,050,355Add Selected Expenses $10,132,255Sub-Total for Niagara Health Care System $163,096,633
Net Inpatient and Outpatient Rehabiliation Expense $7,141,038Less Selected Expenses -$84,611Program Reductions/Enhancements $5,502,507Total Administrative Efficiencies $826,465Add Selected Expenses $84,611Revised Net Inpatient and Outpatient Rehabilitation Expense $13,470,011Change in Rehabiliation Expense $6,328,973
Net Chronic Care & Palliative Expense (including outpatient expenses) $29,566,718Less Selected Expenses -$982,724Program Reductions/Enhancements -$8,134,196Resource Intensity Adjustment $2,173,370Total Administrative Efficiencies -$1,857,341Add Selected Expenses $812,572Revised Net Complex Continuing Care Expense $21,578,401Change in Complex Continuing Care Expense -$7,988,318
Sub-acute Care $4,930,595
Revised Total Operating Expense $182,119,748Change in Operating Net Expense -$13,730,284Percent Change in Net Expenses -7.6%
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
3
3. The estimated reductions in operating costs should be applied against any Ministry of health reductions in operating funds in 1996/97, 1997/98 and 1998/99.
4. Consider adjustments to the amounts noted here to take into account non-Ministry of Health revenue and inflationary pressures that Niagara Health Care System may experience and advise the Health Services Restructuring Commission of these considerations.
5. The Niagara Health Care System should be given approval to plan for a capital construction project for the following:
⇒ St. Catharines General site which will consist of new construction for the cancer
centre, expansion of acute care beds, emergency services, rehabilitation, acute mental health and subacute beds. The total budget for the construction project should be set at a maximum of $56.4 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $7.3 million.
⇒ Greater Niagara General site which will consist of new construction for the expansion of emergency services, mental health and complex continuing care beds. The total budget for the construction project should be set at a maximum of $8.7 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $1.1 million.
⇒ Welland County Memorial site which will consist of expansion of emergency services and mental health beds. The total budget for the construction project should be set at a maximum of $3.9 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $0.5 million.
⇒ Shaver site which will consist of new construction for the development of
rehabilitation beds. The total budget for the construction project should be set at a maximum of $5.8 million. The total budget for equipment and furnishings, included in this total should be set at a maximum of $0.5 million.
The cost of the construction project and furnishings should be funded by the Ministry of Health and the hospital according to prevailing Ministry of Health policy.
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

Niagara Health Care System
4
Accompanying this Advice are: 1. Copies of Directions to the hospitals in Niagara Region; and 2. A copy of the Niagara Region Health Services Restructuring Reports dated October
1998 and March 11, 1999 prepared by the Health Services Restructuring Commission.
DATED at Toronto this 9th day of March, 1999.
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
To: The Honourable Elizabeth Witmer Minister of Health 10th Floor, Hepburn Block Toronto, ON M7A
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

McMaster University
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MAT TER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE MCMASTER UNIVERSITY CONCERNING ACADEMIC PROGRAMS AND PHYSICIAN RECRUITMENT
IN THE NIAGARA REGION Recruitment of Physicians to the Niagara Region 1. To participate on a task force made up of the Niagara Health Care System, the Hotel
Dieu Hospital, local medical societies, University of Western Ontario and the Ministry of Health to develop a plan to recruit and retain family physicians and designated specialty physicians to the region.
2. To Join a task force with the Niagara Health Care System and Hotel Dieu Hospital to
strengthen academic programs in the Region’s hospitals. The task force will include representation from both University of Western Ontario and McMaster Univ ersity and will be responsible for:
• developing a plan to enhance the scope of clinical teaching in the Niagara Region
and the role of Niagara Health Care System and hotel Dieu hospital • developing a medical credentialling process that recognizes and fosters the need
to have a cadre of geographic full-time physicians (GFT) to improve overall quality of care;
• developing strategies to nurture a research environment in both hospitals
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

McMaster University
2
Accompanying this Advice are: 1. Copies of Directions to the hospitals in Nia gara Region; and 2. A copy of the Niagara Region Health Services Restructuring Reports dated October
1998 and March 11, 1999 prepared by the Health Services Restructuring Commission.
DATED at Toronto this 9th day of March, 1999.
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Joseph’Hospital
1
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
ADVICE TO THE UNIVERSITY OF WESTERN ONTARIO CONCERNING ACADEMIC PROGRAMS AND PHYSICIAN RECRUITMENT
IN THE NIAGARA REGION Recruitment of Physicians to the Niagara Region 1. To participate on a task force made up of the Niagara Health Care System, the Hotel
Dieu Hospital, local medical societies, McMaster University and the Ministry of Health to develop a plan to recruit and retain family physicians and designated specialty physicians to the region.
2. To Join a task force with the Niagara Health Care System and Hotel Dieu Hospital to
strengthen academic programs in the Region’s hospitals. The task force will include representation from both University of Western Ontario and McMaster University and will be responsible for:
• developing a plan to enhance the scope of clinical teaching in the Niagara Region
and the role of Niagara Health Care System and hotel Dieu hospital • developing a medical credentialling process that recognizes and fosters the need
to have a cadre of geographic full-time physicians (GFT) to improve overall quality of care;
• developing strategies to nurture a research environment in both hospitals
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Joseph’Hospital
2
Accompanying this Advice are: 1. Copies of Directions to the hospitals in Niagara Region; and 2. A copy of the Niagara Region Health Services Restructuring Reports dated October
1998 and March 11, 1999 prepared by the Health Services Restructuring Commission.
DATED at Toronto this 9th day of March, 1999.
________________________ Chair Health Services Restructuring Commission 12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Joseph’Hospital
3
Health Services Restructuring Commission
IN THE MATTER OF the Public Hospitals Act RSO 1990, c.P.40, as amended
AND IN THE MATTER OF Ontario Regulation 87/96
made under the Public Hospitals Act
AND IN THE MATTER OF The Ministry of Health Act RSO 1990, c.M.26, as amended
AND IN THE MATTER OF Ontario Regulation 88/96
made under the Ministry of Health Act
NOTICE OF SUPPLEMENTARY DIRECTIONS TO THE
ST. JOSEPH’S HOSPITAL, HAMILTON
THE HEALTH SERVICES RESTRUCTURING COMMISSION HAVING ISSUED THE NOTICES OF INTENTION TO ISSUE DIRECTIONS TO THE NIAGARA HOSPITALS ON OCTOBER 27, 1998, AND HAVING CONSIDERED THE REPRESENTATIONS RECEIVED IN RESPONSE DIRECTS the Board of Directors of the St. Joseph’s Hospital, Hamilton to: 1. Work with Hotel Dieu Hospital in St. Catharines to develop a plan to transfer 53 long
term mental health beds and associated outpatient services from the St. Joseph’s Hospital (which will receive the Hamilton Psychiatric Hospital’s programs) by March 31, 2001. The plan must be developed by December 31, 1999 and submitted to the Ministry of Health.
Accompanying this Direction are: 3. Copies of Directions to the hospitals in Niagara Region; and 4. A copy of the Niagara Region Health Services Restructuring Reports dated October
1998 and March 11, 1999 prepared by the Health Services Restructuring Commission.
DATED at Toronto this 10th day of March, 1999.
________________________ Chair Health Services Restructuring Commission
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.

St. Joseph’Hospital
4
12th Floor 56 Wellesley Street West Toronto, Ontario M5S 2S3 Tel: (416) 316-5919 FAX: (416) 316-5689
Cop
y fo
r arc
hive
pur
pose
s. P
leas
e co
nsul
t orig
inal
pub
lishe
r for
cur
rent
ver
sion
. C
opie
à d
es fi
ns d
’arc
hiva
ge.
Veu
illez
con
sulte
r l’é
dite
ur o
rigin
al p
our l
a ve
rsio
n ac
tuel
le.