Embed Size (px)
Citation preview
Nicole Bouchard MD FRCPC
Pulmonologist
April 29, 2011
Disclosure
I cannot identify any potential conflict of interest.
Objectives 1) Select the appropriate diagnostic tests to
accurately stage lung cancer
2) Understand the strengths and weaknesses of PET Scan for lung cancer staging
3) Propose a rational approach to optimally stage mediastinal lymph nodes
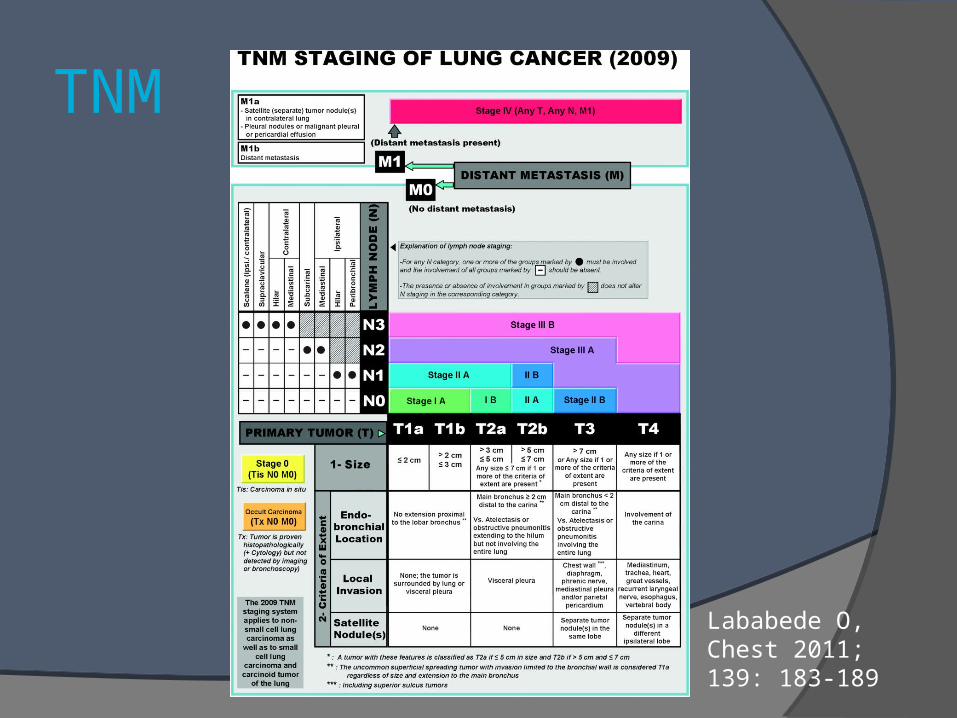
TNM
Lababede O, Chest 2011; 139: 183-189
Diagnostic tests
CT scan:chest and upper abdomen
PET-CT: if a radical treatment is considered
Pulmonary function testing Imaging of the head (MRI):
if symptomsfor small cell lung cancer maybe in stage 3 disease NSCLC
Lim E, Thorax 2010; 65 (Suppl III); iii1-iii27Alberts WM, Chest 2007; 132; 1S-19S
Diagnostic tests
Bone scintigraphy? PET is more sensitiveto avoid an unnecessary PET-CTPET: from base of skull to upper thighs
Diagnostic tests
Least invasive approach that provides both the diagnostic and the stagebronchoscopy, transthoracic CT guided needle
biopsy, radial probe EBUS
EBUS, EUS, mediastinoscopy, VATS
US guided needle aspiration: thoracentesis, cervical lymph node, liver
EUS: left adrenal metastasis
Diagnostic tests
→ Adequate sample
IASLC/ATS/ERS International Multidisciplinary Classification of Lung Adenocarcinoma
NSCLC are to be classified into adenocarcinoma or squamous cell carcinomagefitinib, pemetrexed, bevacizumab
Travis WD, Journal of Thoracic Oncology 2011; 6: 244-285
Diagnostic tests
Wait times and costs2852 patientsprovincial cancer registry: Manitoba≥ 25% of patients waited more than 55 days
Cheung WY, Lung Cancer 2010 Sep [ Epub ahead of print ]
Diagnostic tests
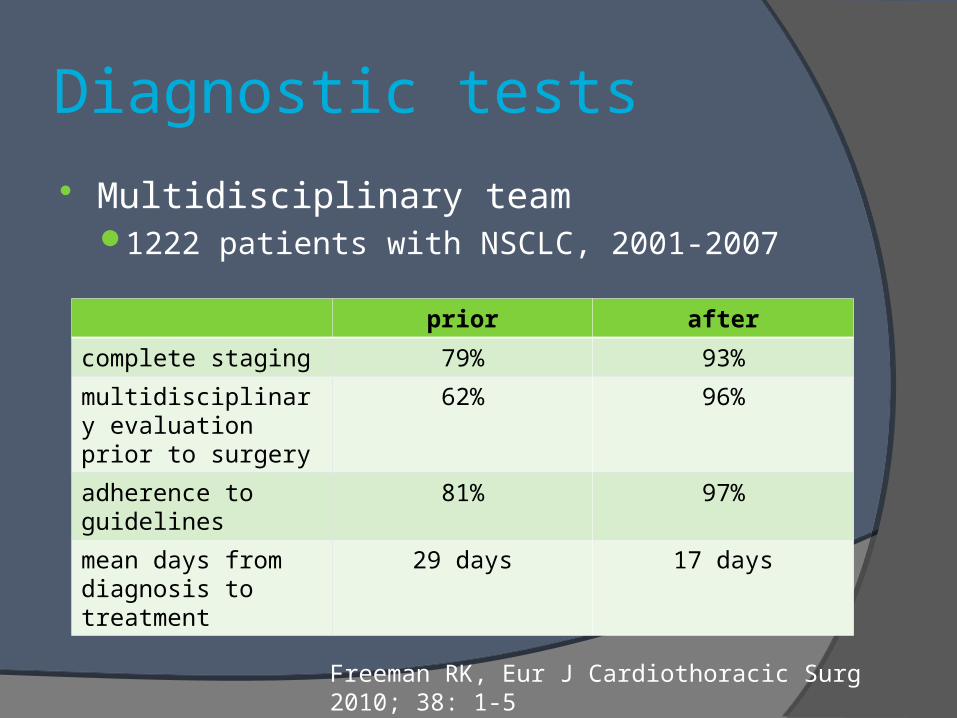
Multidisciplinary team1222 patients with NSCLC, 2001-2007
survival?
Freeman RK, Eur J Cardiothoracic Surg 2010; 38: 1-5
prior after
complete staging 79% 93%
multidisciplinary evaluation prior to surgery
62% 96%
adherence to guidelines
81% 97%
mean days from diagnosis to treatment
29 days 17 days
PET-CT Scan
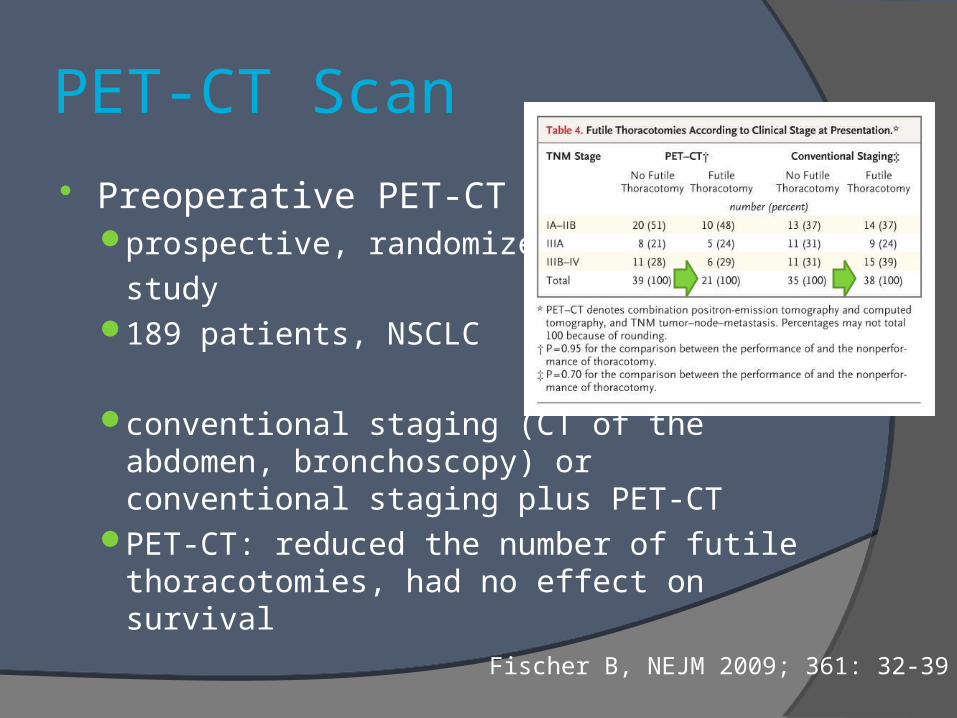
Preoperative PET-CTprospective, randomized
study189 patients, NSCLC
conventional staging (CT of the abdomen, bronchoscopy) or conventional staging plus PET-CT
PET-CT: reduced the number of futile thoracotomies, had no effect on survival
Fischer B, NEJM 2009; 361: 32-39
PET-CT Scan
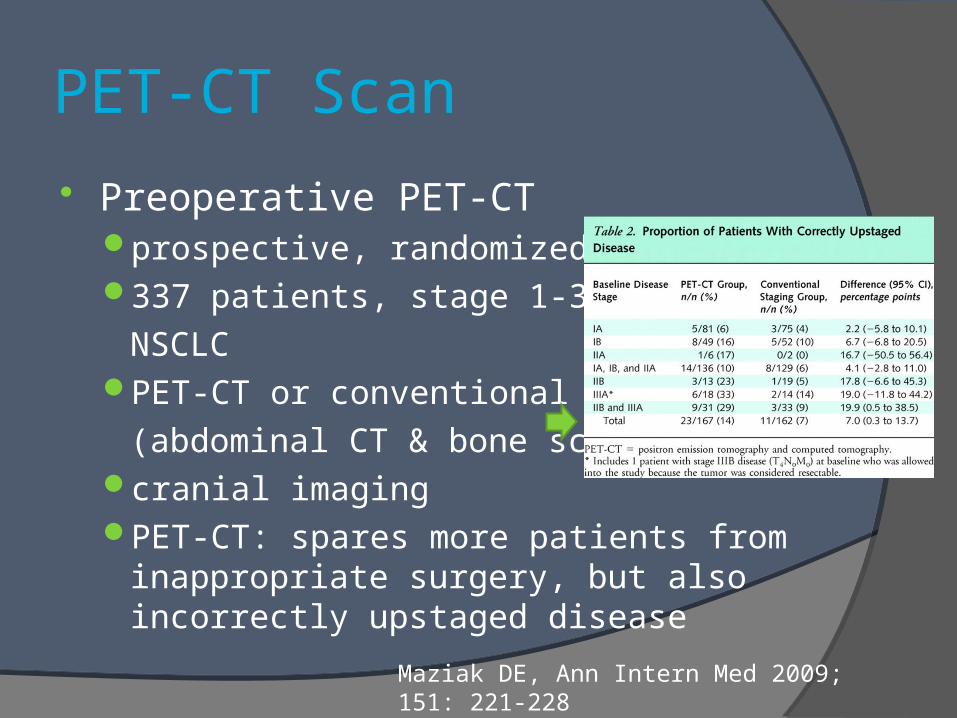
Preoperative PET-CTprospective, randomized trial337 patients, stage 1-3A
NSCLCPET-CT or conventional
(abdominal CT & bone scan)cranial imagingPET-CT: spares more patients from
inappropriate surgery, but also incorrectly upstaged disease
Maziak DE, Ann Intern Med 2009; 151: 221-228
PET-CT Scan
T stage (SUVmax 2,5)false positive: infectious and inflammatory
lesionsfalse negative: carcinoid, certain
adenocarcinomas, uncontrolled diabetes, cavity with necrotic center, lesion < 8 mm
Lim E, Thorax 2010; 65 (Suppl III); iii1-iii27
PET-CT Scan
Solitary pulmonary nodule (8 - 30 mm) and an initial SUVmax 2.6 retrospective study, CHUS, PET-CT20 / 65 (31%) patients: diagnosis of cancer;
mostly adenocarcinomasrisk factors for malignancy: higher 18F-FDG
uptake, spiculated noduleSUVmax 1: new threshold?
Houle MA, Can Respir J 2010; 17, suppl B: 6B
PET-CT Scan
N stageCT
> 10 mm in short axis diameter
sensitivity 57-61%, specificity 79-82%PET
sensitivity 84%, specificity 89%
false negative: small volume, low metabolic activity
false positive: inflammation → sampling
size of the lymph node is important
Alberts WM, Chest 2007; 132; 1S-19SLim E, Thorax 2010; 65 (Suppl III); iii1-iii27
PET-CT Scan
M stagesensitivity 93%, specificity 96%detect metastases:
15%, more with advanced stage
Lim E, Thorax 2010; 65 (Suppl III); iii1-iii27
PET-CT Scan
Sample of any isolated distant lesion350 patients21% had a solitary lesion: 46% had a benign
lesion or another cancer (second cancer or recurrence)
Lardinois D, J Clin Oncol 2005; 23: 6846-6853
Mediastinal lymph nodes (LN)
No lymph node sampling if uptake is within normal limits on PET-CT and < 1 cmfalse negative rate: 5-7% for a peripheral tumor
if central tumor, N1 enlargement? N2 or N3 ≥ 1 cm but PET negative?
Lymph node sampling if PET uptake is positive, to avoid false positive resultsEBUS/EUS; +/- mediastinoscopy if negative
Mediastinal lymph nodes (LN)
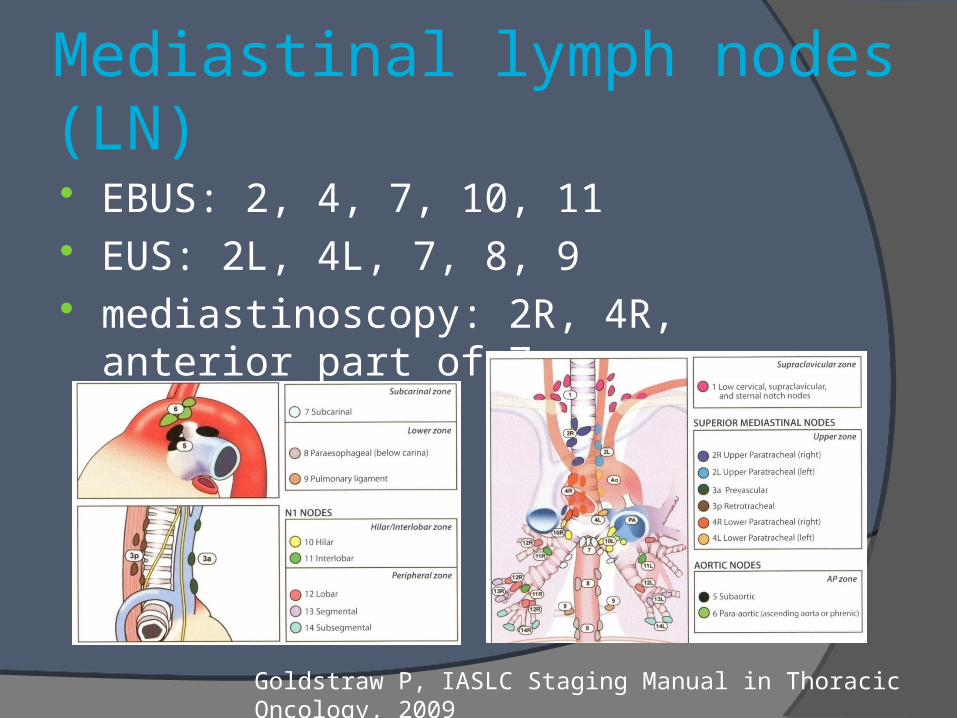
EBUS: 2, 4, 7, 10, 11 EUS: 2L, 4L, 7, 8, 9 mediastinoscopy: 2R, 4R, anterior part of 7
Goldstraw P, IASLC Staging Manual in Thoracic Oncology, 2009
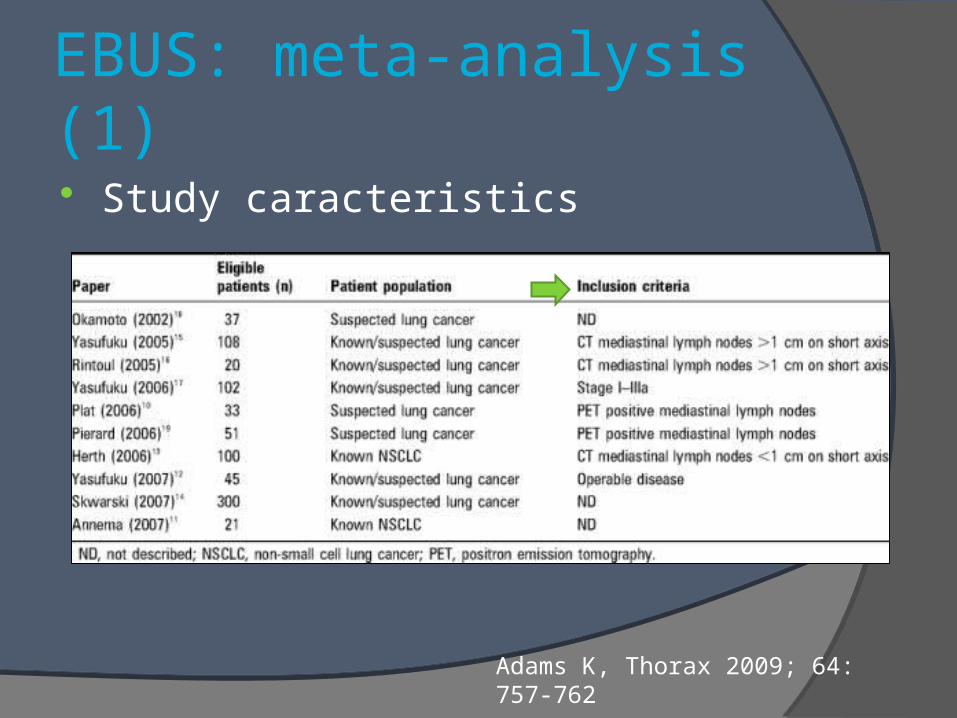
EBUS: meta-analysis (1)
Study caracteristics
Adams K, Thorax 2009; 64: 757-762
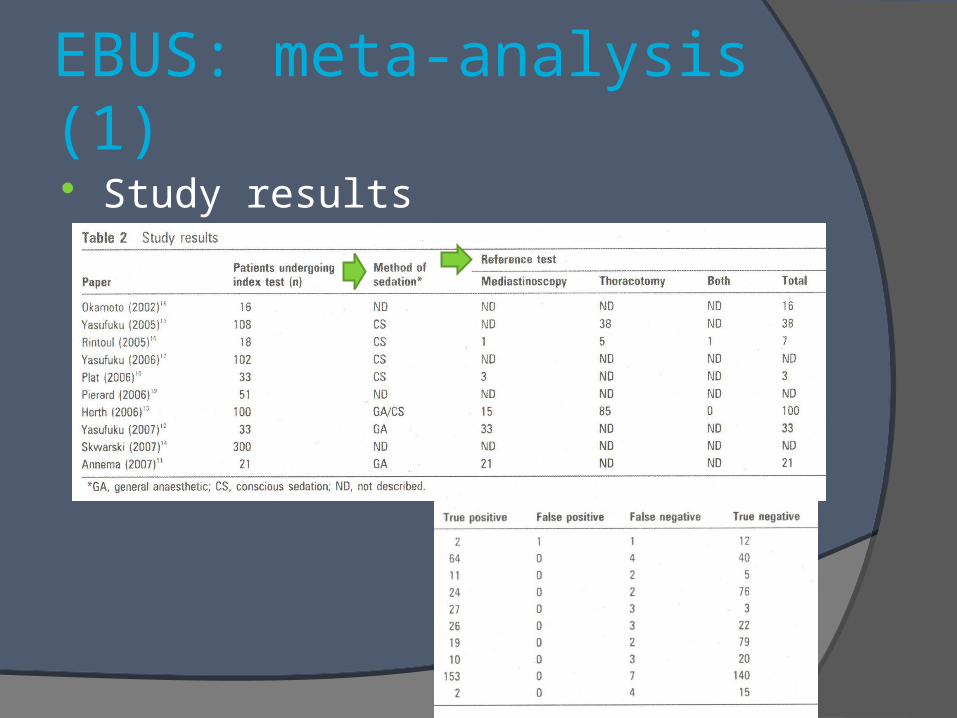
EBUS: meta-analysis (1)
Study results
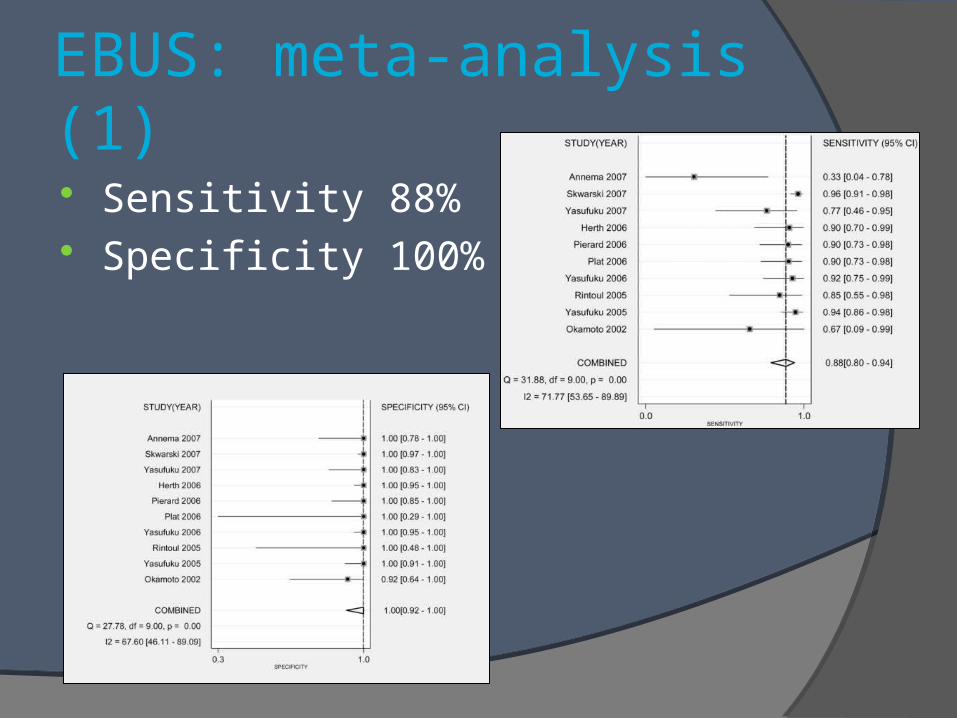
EBUS: meta-analysis (1)
Sensitivity 88% Specificity 100%
EBUS: meta-analysis (2)
Sensitivity 93% Specificity 100% Only 2 complications
2 / 1299 patients (0,15%)pneumothoraxpatient with COPD: hypoxemia during the
procedureGu P, European Journal of Cancer 2009; 45: 1389-1396
EBUS: false negative rate
False negative rates20-25%
External validityother studies have been published

EBUS: learning curve
Learning curves500 patients5 EBUS operatorsno learning from
prior experience
operators 3 & 5: still
in the learning phase
after 100 procedures
Kemp SV, Thorax 2010; 65: 534-538
EBUS: cost effectiveness
Cost effectivenesscost-beneficial in comparison with surgical
mediastinoscopy, for a prevalence as low as 30%
negative results confirmed by mediastinoscopy: cost-beneficial according to the prevalence of LN metastases (>79%)
Steinfort D, J Thorac Oncol 2010; 5: 1564-1570
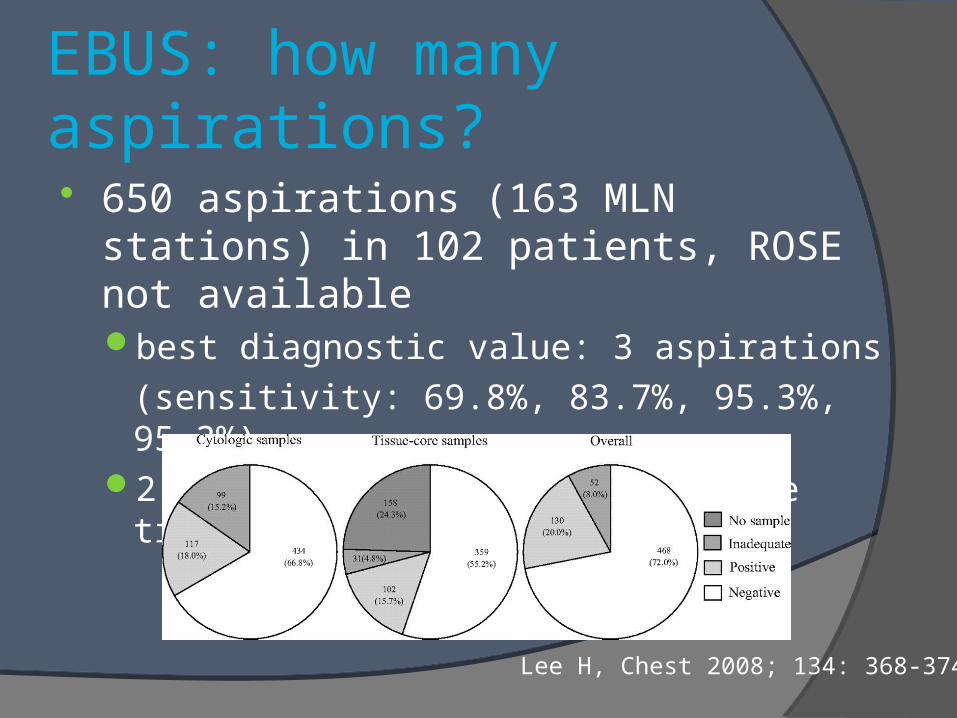
EBUS: how many aspirations?
650 aspirations (163 MLN stations) in 102 patients, ROSE not availablebest diagnostic value: 3 aspirations
(sensitivity: 69.8%, 83.7%, 95.3%, 95.3%) 2 aspirations: when at least one tissue core
Lee H, Chest 2008; 134: 368-374
EBUS: which needle?
21-gauge versus 22-gauge aspiration needle
45 lesionssame diagnostic yield21G: better histological preservation but
more blood contamination
Nakajima T, Respirology 2010 Sep [ Epub ahead of print ]
EBUS: mutations and SCLC
Mutation analysisEGFR and KRAS mutations can be
performed in cytologic specimens (EUS/EBUS)
also EML4-ALK fusion gene
SCLC: high diagnostic yield
Schuurbiers OC, J Thorac Oncol 2010: 5: 1664-1667
Nakajima T, J Thorac Oncol 2011; 6: 203-206
Wada H, Ann Thorac Surg 2010; 90: 229-234
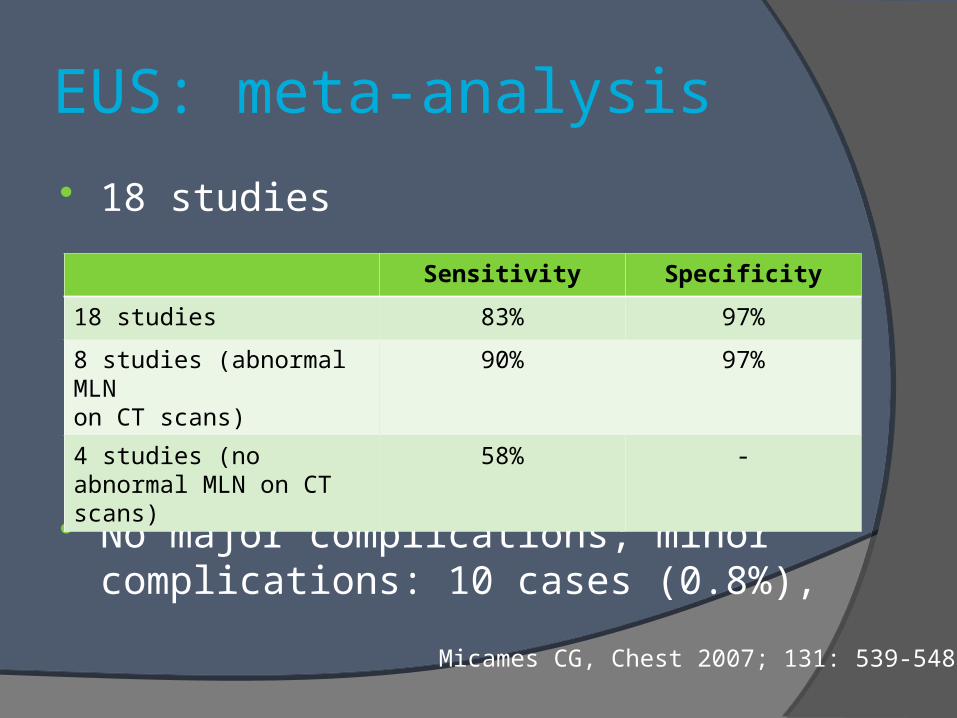
EUS: meta-analysis
18 studies
No major complications; minor complications: 10 cases (0.8%),
Micames CG, Chest 2007; 131: 539-548
Sensitivity Specificity
18 studies 83% 97%
8 studies (abnormal MLNon CT scans)
90% 97%
4 studies (no abnormal MLN on CT scans)
58% -
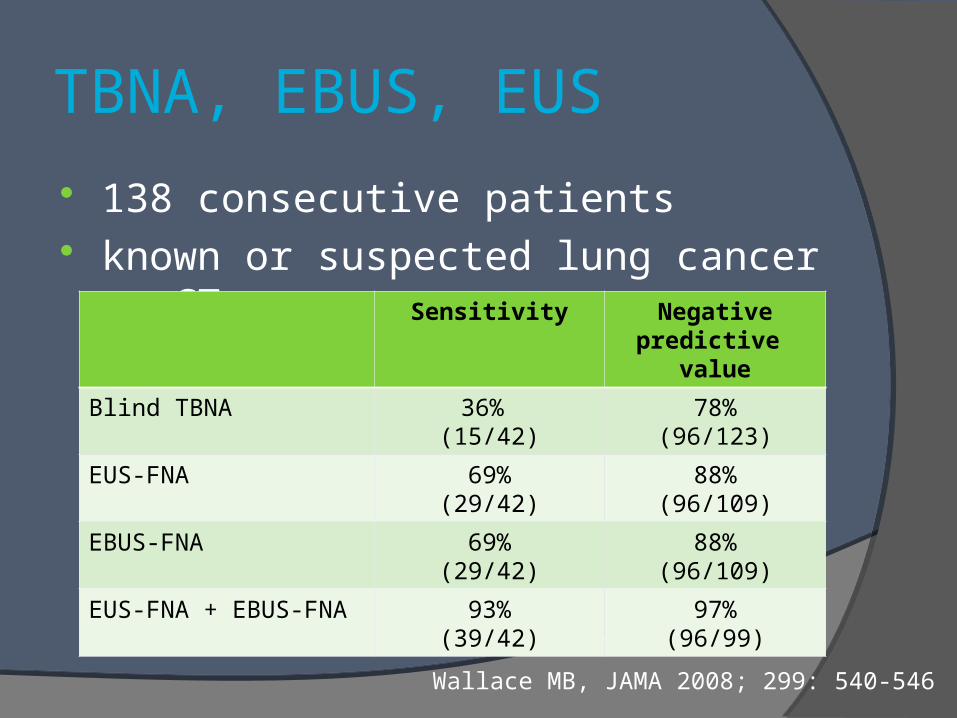
TBNA, EBUS, EUS
138 consecutive patients known or suspected lung cancer on CT
Wallace MB, JAMA 2008; 299: 540-546
Sensitivity Negative predictive
value
Blind TBNA 36% (15/42)
78%(96/123)
EUS-FNA 69%(29/42)
88%(96/109)
EBUS-FNA 69%(29/42)
88%(96/109)
EUS-FNA + EBUS-FNA 93%(39/42)
97%(96/99)
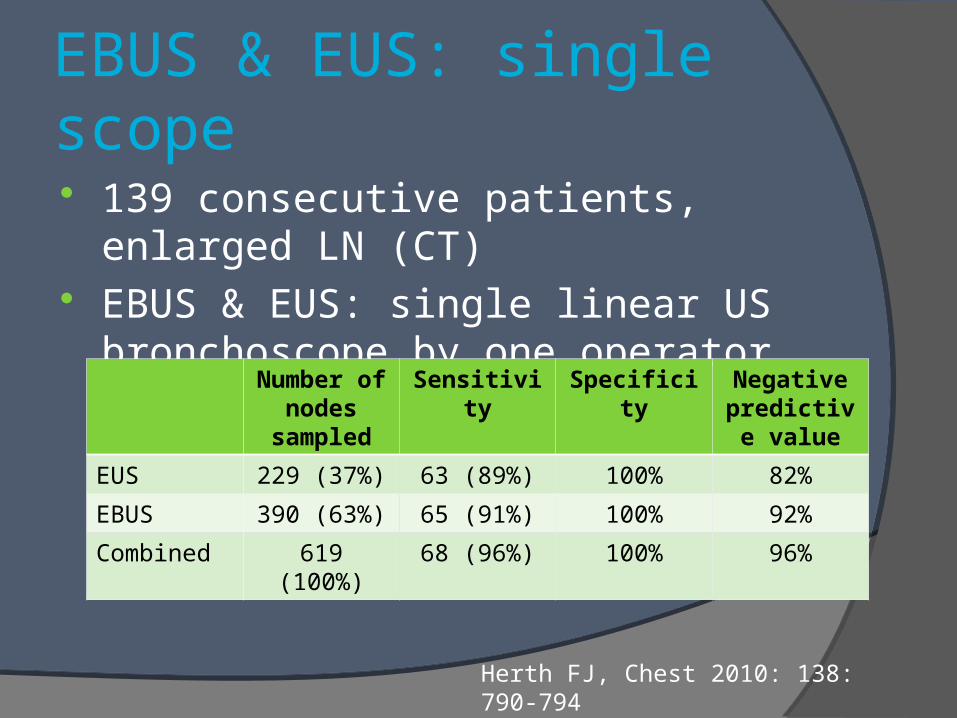
EBUS & EUS: single scope
139 consecutive patients, enlarged LN (CT) EBUS & EUS: single linear US bronchoscope
by one operator
Herth FJ, Chest 2010: 138: 790-794
Number of nodes
sampled
Sensitivity Specificity Negative predictive
value
EUS 229 (37%) 63 (89%) 100% 82%
EBUS 390 (63%) 65 (91%) 100% 92%
Combined 619 (100%) 68 (96%) 100% 96%
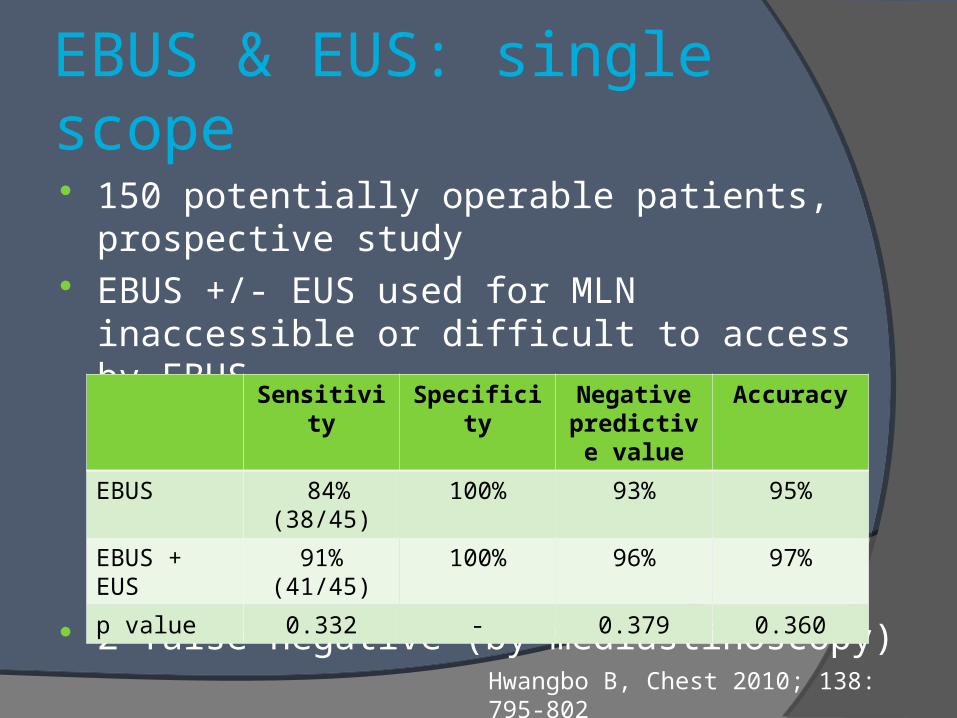
EBUS & EUS: single scope
150 potentially operable patients, prospective study
EBUS +/- EUS used for MLN inaccessible or difficult to access by EBUS
2 false negative (by mediastinoscopy)Hwangbo B, Chest 2010; 138: 795-802
Sensitivity Specificity Negative predictive
value
Accuracy
EBUS 84% (38/45) 100% 93% 95%
EBUS + EUS
91% (41/45) 100% 96% 97%
p value 0.332 - 0.379 0.360
EBUS versus mediastinoscopy
66 patients, prospective crossover trial Prevalence of malignancy: 89% Diagnostic yield
EBUS: 91% versus mediastinoscopy: 78% (p=0.007)
disagreement: subcarinal lymph nodes (24%; p=0.011)
no difference: true pathologic N stage (per patient)
Ernst A, Journal of Thoracic Oncology 2008; 3; 577-582
ASTER study
Randomized controlled multicenter trial 241 patients Lung or mediastinal abnormality on CT,
no extrathoracic metastases
EUS & EBUS (systematic sampling) and surgical staging if negative or surgical staging (mediastinoscopy): N2 & N3
Annema JT, JAMA 2010; 304: 2245-2252
ASTER study
Nodal metastases62 patients by combined staging (p=0.02)41 patients by surgical stagingmediastinoscopy: 11 patients to identify 1
with nodal metastasis
Thoracotomy unnecessary21patients in the mediastinoscopy group9 patients in the combined group (p = 0.02)
No increase rate of complications
Conclusion PET-CT: before surgery and radiotherapy
When N2 or N3 is suspected on PET: EBUS; mediastinoscopy if negative
Complete mediastinal staging: EBUS +/- EUS; role of mediastinoscopy?
Further studies are ongoingpreoperative EBUS, EBUS vs mediastinoscopy,
surgical staging vs endosonography





























