Embed Size (px)
Citation preview

Diets in functional bowel disorders: low FODMAP & beyond
NICOLE FAKHOURY-SAYEGH RD, MPH, PHD
Functional bowel disorders
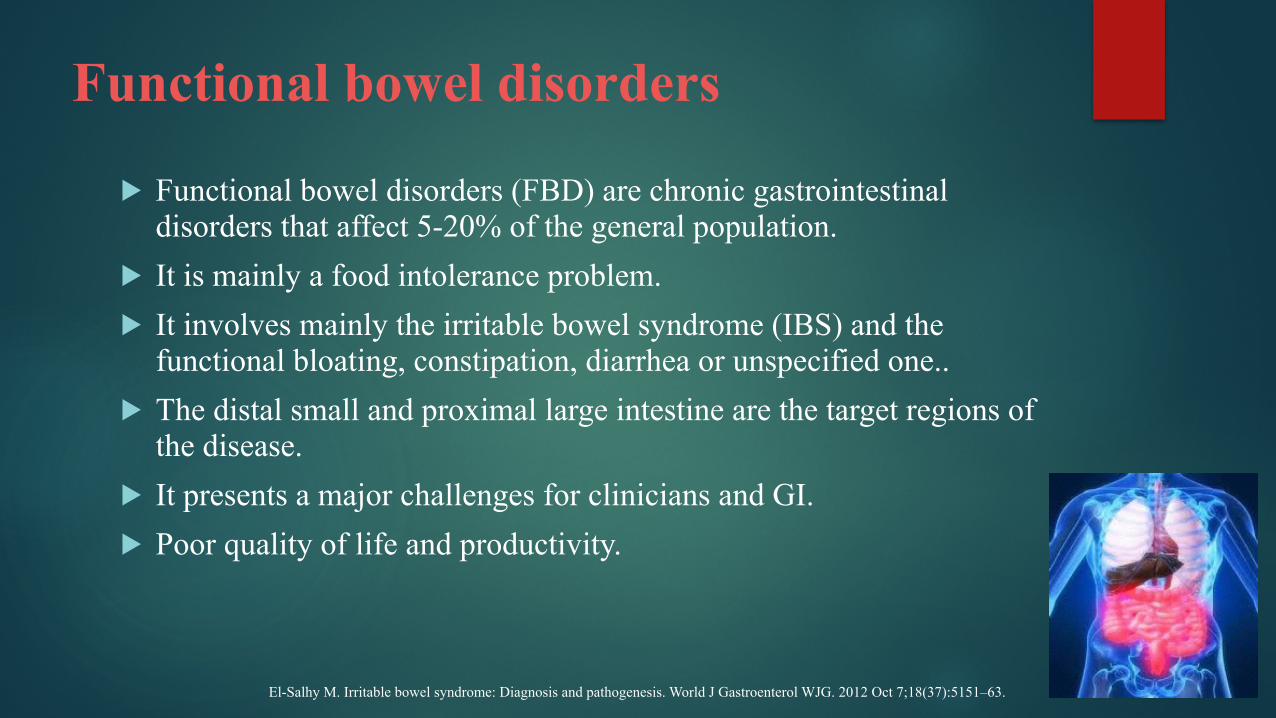
! Functional bowel disorders (FBD) are chronic gastrointestinal disorders that affect 5-20% of the general population.
! It is mainly a food intolerance problem. ! It involves mainly the irritable bowel syndrome (IBS) and the
functional bloating, constipation, diarrhea or unspecified one.. ! The distal small and proximal large intestine are the target regions of
the disease. ! It presents a major challenges for clinicians and GI. ! Poor quality of life and productivity.
El-Salhy M. Irritable bowel syndrome: Diagnosis and pathogenesis. World J Gastroenterol WJG. 2012 Oct 7;18(37):5151–63.
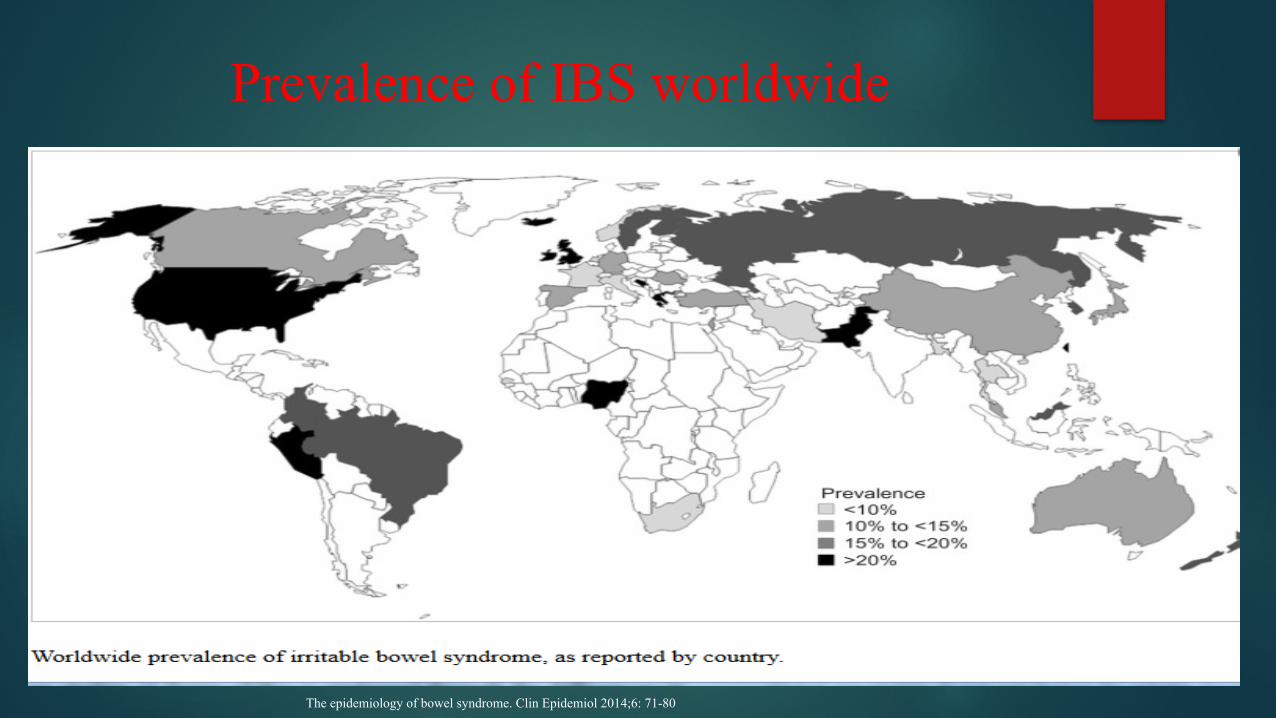
Prevalence of IBS worldwide
The epidemiology of bowel syndrome. Clin Epidemiol 2014;6: 71-80
Diagnosis of IBS
! According to the criteria of ROME III (2006)
! Recurrent abdominal pain(at least 6 months prior to diagnosis) associated with 2 or more of the following (3 days/month in the last 3 months).
! Abnormal stool frequency (more than 3 bowels movement/day or less than 3 bowels movements/week).
! Abnormal stool form (hard/loose/watery stool)
! Abnormal stool passage (straining, feeling of incomplete evacuation) ! Passage of mucous
! Bloating
! Improvement with defecation
El-Salhy M. Irritable bowel syndrome: Diagnosis and pathogenesis. World J Gastroenterol WJG. 2012 Oct 7;18(37):5151–63.
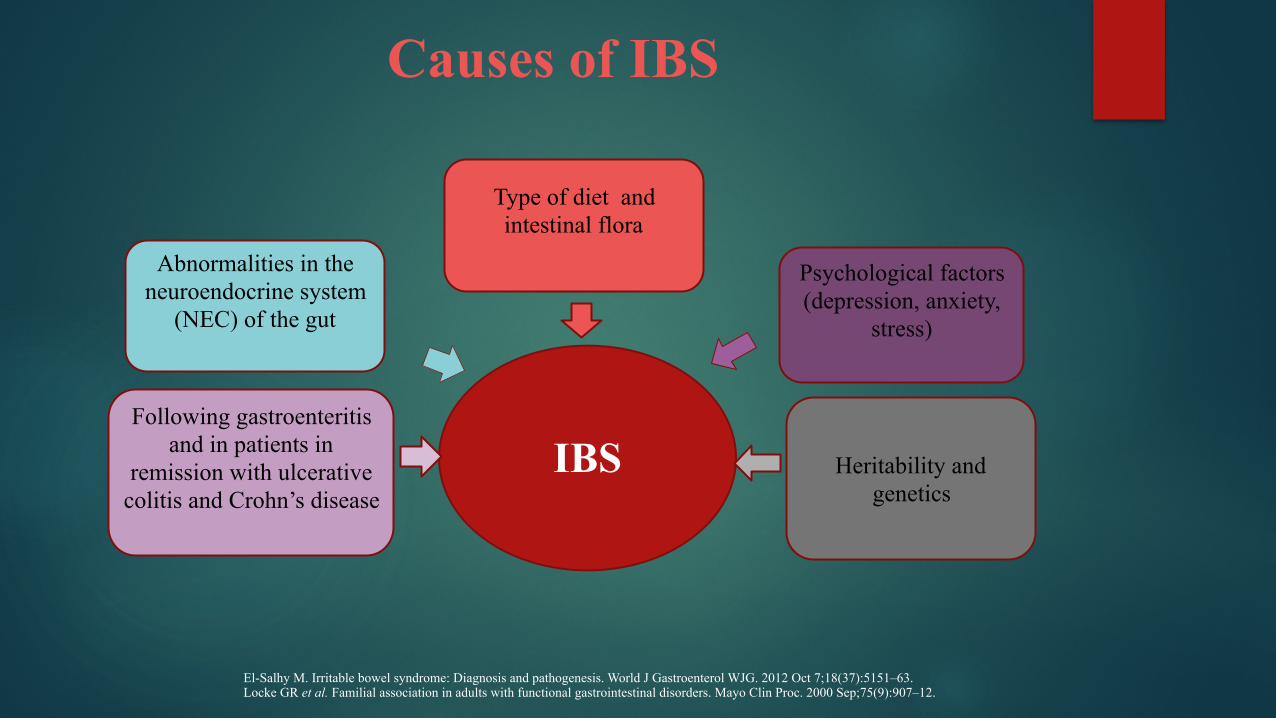
Causes of IBS
IBS Heritability and genetics
Psychological factors (depression, anxiety,
stress)
Type of diet and intestinal flora
Abnormalities in the neuroendocrine system
(NEC) of the gut
Following gastroenteritis and in patients in
remission with ulcerative colitis and Crohn’s disease
El-Salhy M. Irritable bowel syndrome: Diagnosis and pathogenesis. World J Gastroenterol WJG. 2012 Oct 7;18(37):5151–63. Locke GR et al. Familial association in adults with functional gastrointestinal disorders. Mayo Clin Proc. 2000 Sep;75(9):907–12.
Pathogenesis
! Alteration in bacterial mass ! Poor absorption in the proximal (large or small ?) intestine ! Presence of small molecules which are osmotically active. ! High fermentation by bacteria with high expansion of its
population. ! Increase in intestinal osmotic pressure and stimulation of
endocrine and peptidergic or serotonergic nerves of the enteric nervous system (ENS).
El-Salhy M. Irritable bowel syndrome: Diagnosis and pathogenesis. World J Gastroenterol WJG. 2012 Oct 7;18(37):5151–63. Locke GR, Zinsmeister AR, Talley NJ, Fett SL, Melton LJ. Familial association in adults with functional gastrointestinal disorders. Mayo Clin Proc. 2000 Sep;75(9):907–12.
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
FODMAPs
! Clinical studies had shown that a low FODMAP diet alleviates gastrointestinal symptoms in patients with IBS
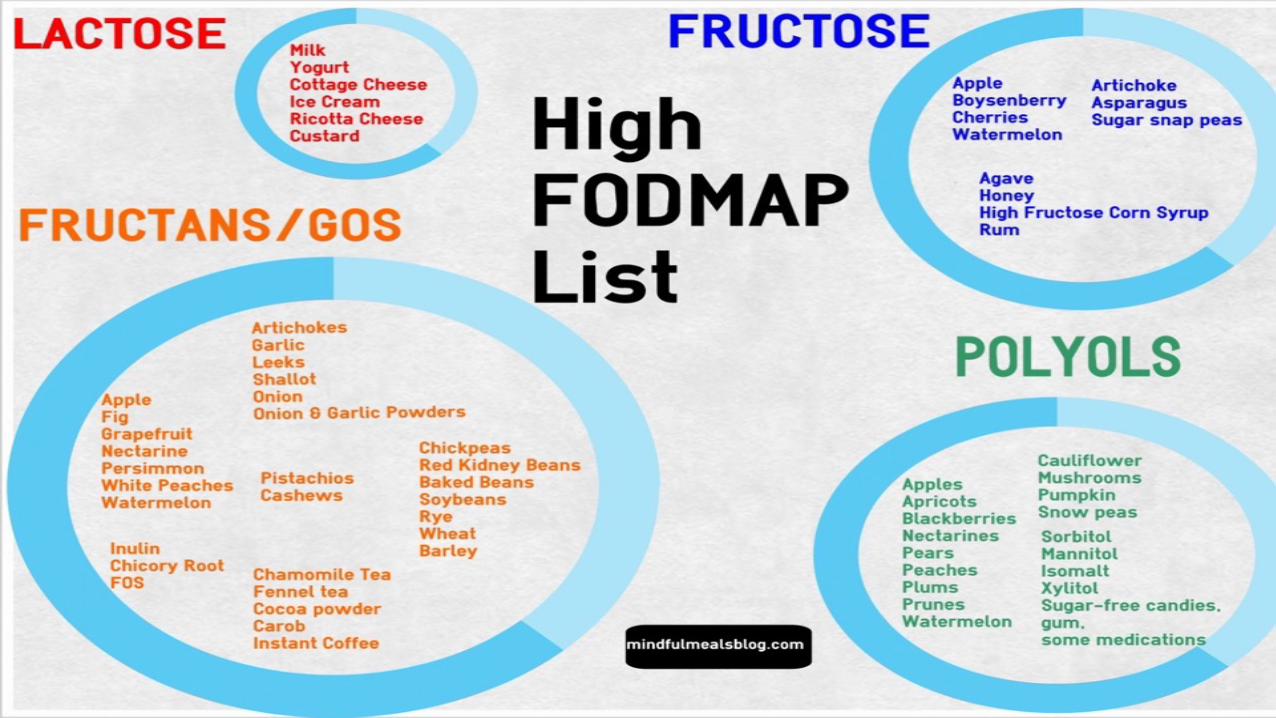
! FODMAP is an acronym for Fermentable Oligo-, Di, Mono-saccharides and Polyols.
! It comprises fructo-and galacto oligosaccharides (fructans and galactans), lactose , fructose and polyols.
! They are short-chain carbohydrates characterized by poor absorption and high fermentation rate.
! .
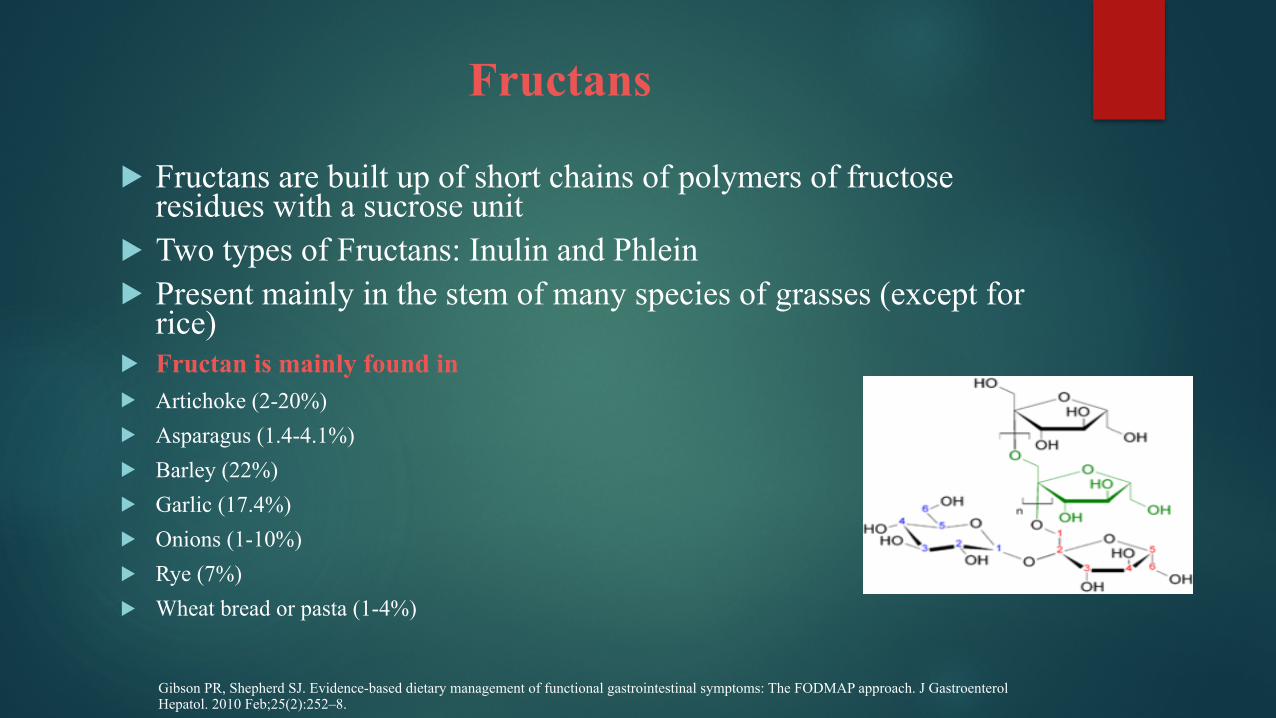
Fructans
! Fructans are built up of short chains of polymers of fructose residues with a sucrose unit
! Two types of Fructans: Inulin and Phlein ! Present mainly in the stem of many species of grasses (except for
rice)
! Fructan is mainly found in ! Artichoke (2-20%) ! Asparagus (1.4-4.1%) ! Barley (22%) ! Garlic (17.4%) ! Onions (1-10%) ! Rye (7%) ! Wheat bread or pasta (1-4%)
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
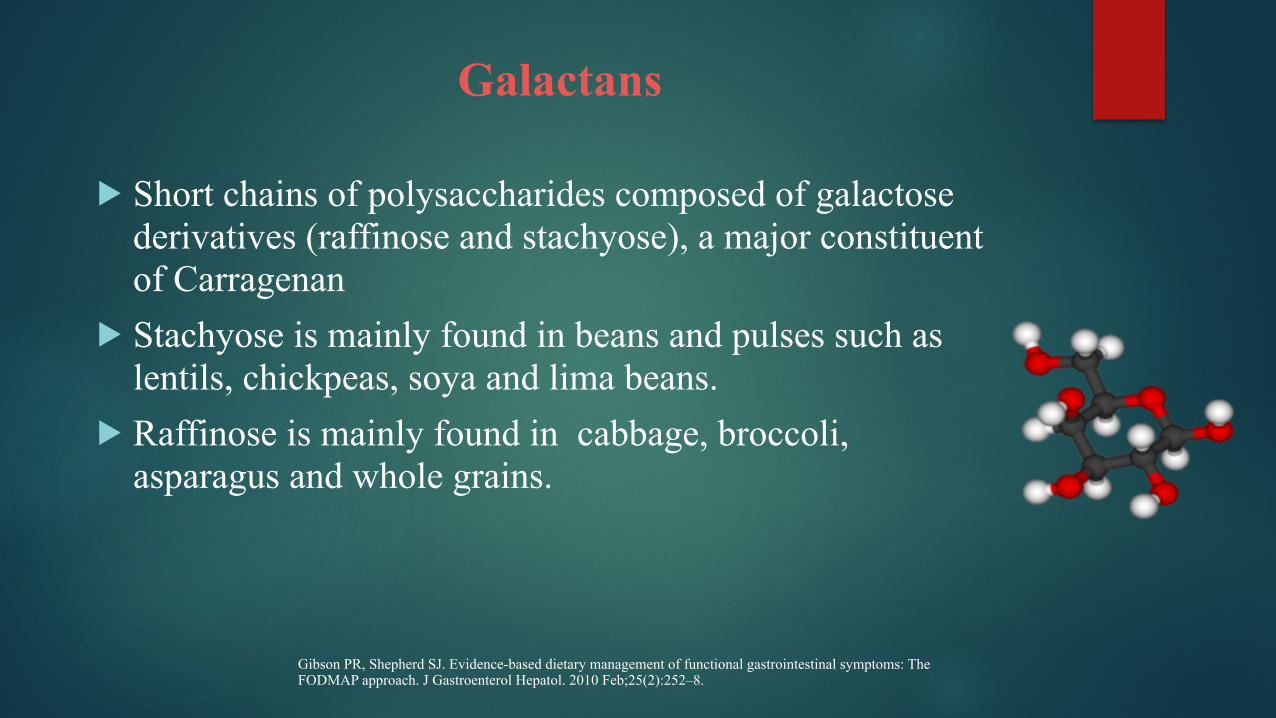
Galactans
! Short chains of polysaccharides composed of galactose derivatives (raffinose and stachyose), a major constituent of Carragenan
! Stachyose is mainly found in beans and pulses such as lentils, chickpeas, soya and lima beans.
! Raffinose is mainly found in cabbage, broccoli, asparagus and whole grains.
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
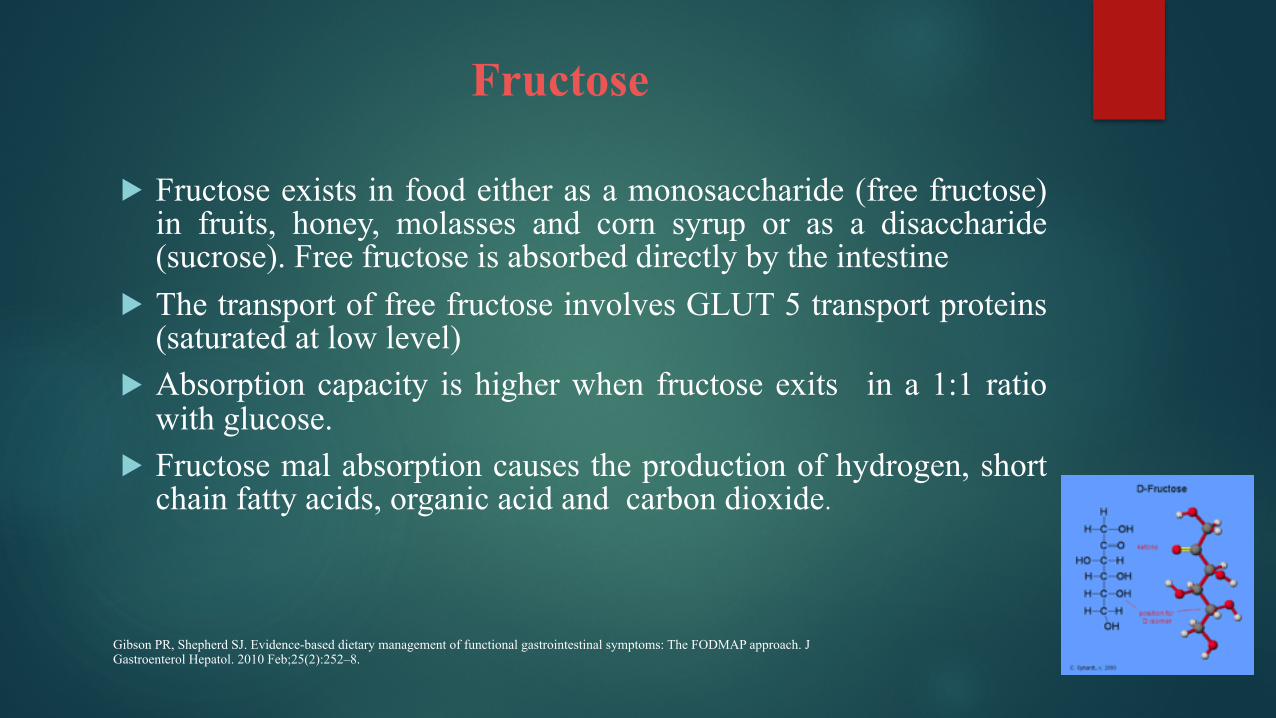
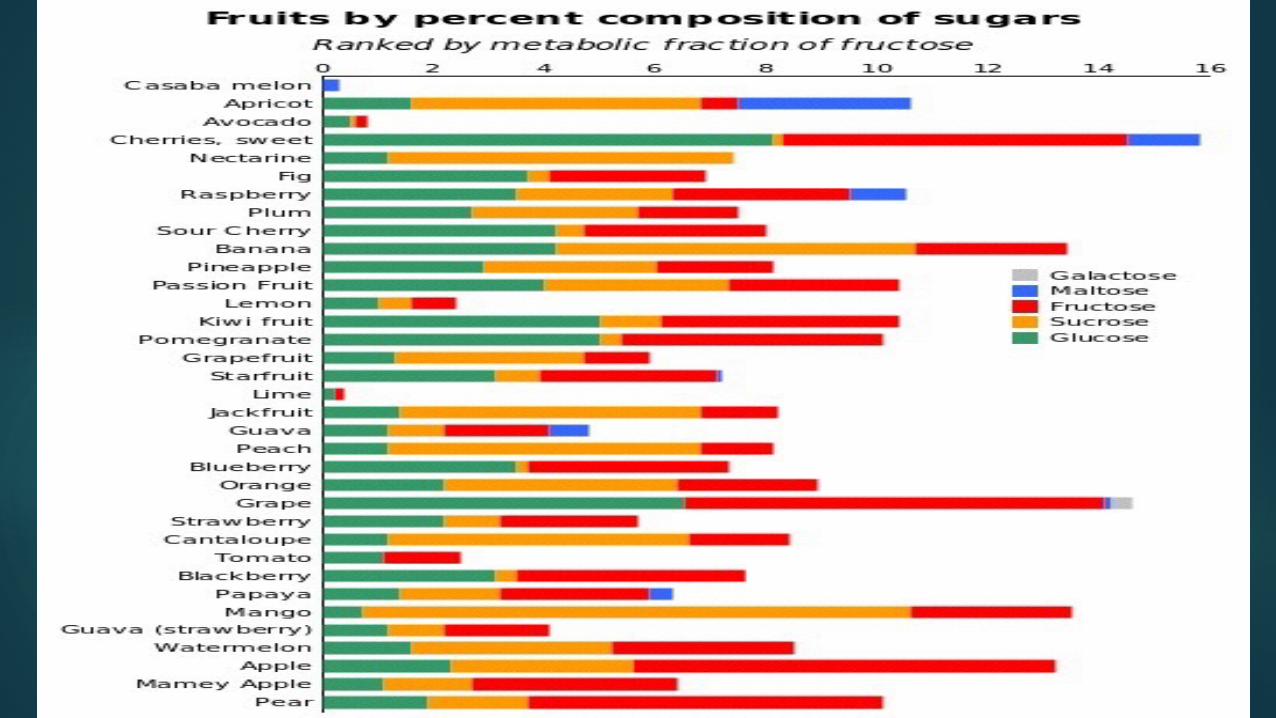
Fructose
! Fructose exists in food either as a monosaccharide (free fructose) in fruits, honey, molasses and corn syrup or as a disaccharide (sucrose). Free fructose is absorbed directly by the intestine
! The transport of free fructose involves GLUT 5 transport proteins (saturated at low level)
! Absorption capacity is higher when fructose exits in a 1:1 ratio with glucose.
! Fructose mal absorption causes the production of hydrogen, short chain fatty acids, organic acid and carbon dioxide.
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
Lactose
! Lactose is a disaccharide sugar made of galactose and glucose that is found in milk or dairy products. Lactose makes up around 2–8% of milk.
! Lactose intolerance is the inability of adults and children to digest lactose causing side effects.
! The principal symptom of lactose intolerance is an adverse reaction to products containing lactose (primarily milk), including abdominal bloating cramps, flatulence, diarrhea, nausea and vomiting.
! Health breath test is used to measure lactose mal absoption
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
Polyols
! Polyols, also called sugar alcohols (Sorbitol, Mannitol, xilitol..), are a group of versatile, reduced-calorie carbohydrates that provide the taste and texture of sugar with about half the calories.
! They are used as food ingredients to replace sugar in an increasing variety of sugar-free and reduced-calorie foods and beverages for their functional and health benefits
! These products include chewing gums, candies, ice cream, baked goods and fruit spreads.
! Polyols are only partially digested and absorbed in the small intestine, they are fermented by bacterias. This causes flatulance and a slight increase in the frequency of bowels movement.
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J
Gastroenterol Hepatol. 2010 Feb;25(2):252–8.
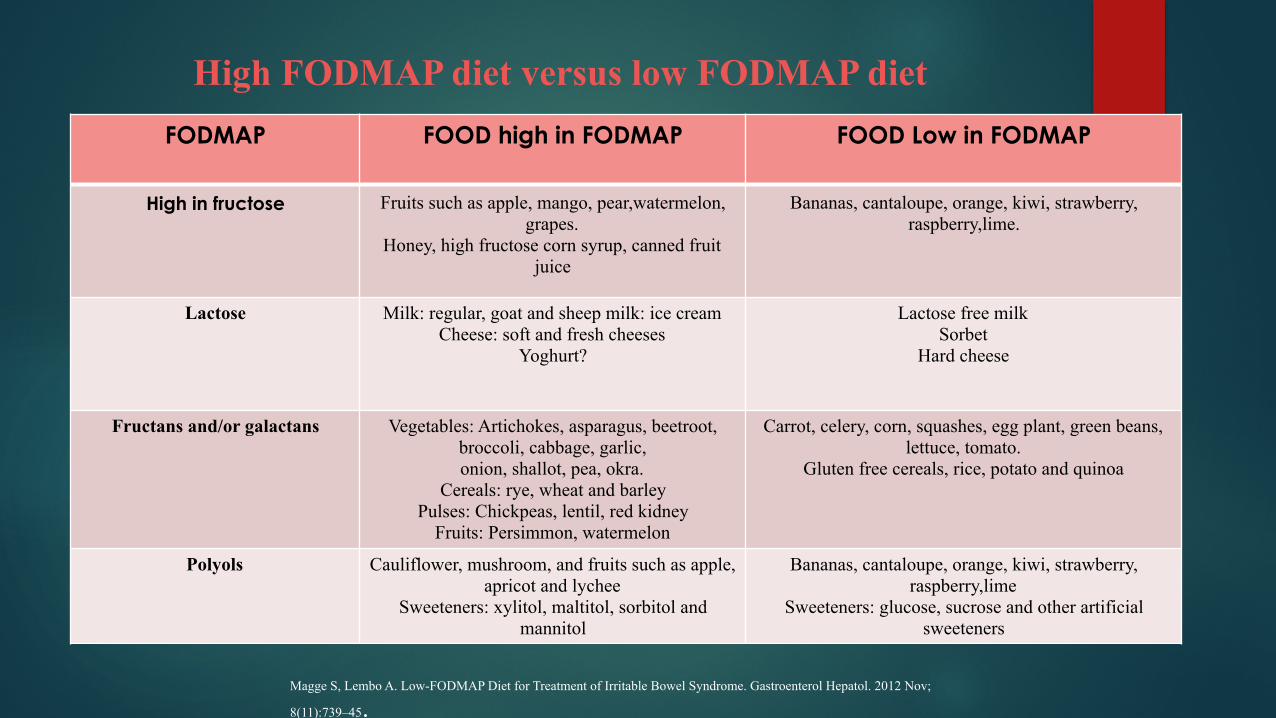
High FODMAP diet versus low FODMAP dietFODMAP FOOD high in FODMAP FOOD Low in FODMAP
High in fructose Fruits such as apple, mango, pear,watermelon, grapes.
Honey, high fructose corn syrup, canned fruit juice
Bananas, cantaloupe, orange, kiwi, strawberry, raspberry,lime.
Lactose Milk: regular, goat and sheep milk: ice cream Cheese: soft and fresh cheeses
Yoghurt?
Lactose free milk Sorbet
Hard cheese
Fructans and/or galactans Vegetables: Artichokes, asparagus, beetroot, broccoli, cabbage, garlic, onion, shallot, pea, okra.
Cereals: rye, wheat and barley Pulses: Chickpeas, lentil, red kidney
Fruits: Persimmon, watermelon
Carrot, celery, corn, squashes, egg plant, green beans, lettuce, tomato.
Gluten free cereals, rice, potato and quinoa
Polyols Cauliflower, mushroom, and fruits such as apple, apricot and lychee
Sweeteners: xylitol, maltitol, sorbitol and mannitol
Bananas, cantaloupe, orange, kiwi, strawberry, raspberry,lime
Sweeteners: glucose, sucrose and other artificial sweeteners
Magge S, Lembo A. Low-FODMAP Diet for Treatment of Irritable Bowel Syndrome. Gastroenterol Hepatol. 2012 Nov;
8(11):739–45.
Barrett JS et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. 2010;31(8):874–82 De Roest RH et al. The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: a prospective study. Int J Clin Pract. 2013 Sep;67(9):895–903. Halmos EP et al. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut. 2015 Jan 1;6
Does Low FODMAP diet improve gastrointestinal symptoms in patients with IBS and decrease delivery of water and fermentable substrates to the proximal colon ?
! Dietary poorly absorbed short –chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon, 2010
! The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: a prospective study, 2013
! Diet that differ in their FODMAP content alter the colonic luminal microenvironment, 2015
16
Dietary poorly absorbed short –chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon
Objectives: To determine the effect of dietary FODMAPs on the content of water and fermentable substrates of ileal effluent.
Methods: Twelve ileostomates without evidence of small intestinal disease undertook two 4-days dietary period differing only in FODMAPs content in a randomised cross-over single-blinded intervention study. Day time ileal effluent was collected on day four for each diet. The volume and consistency were rated on a 10-cm visual analog scale.
Barrett JS et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. 2010;31(8):874–82.
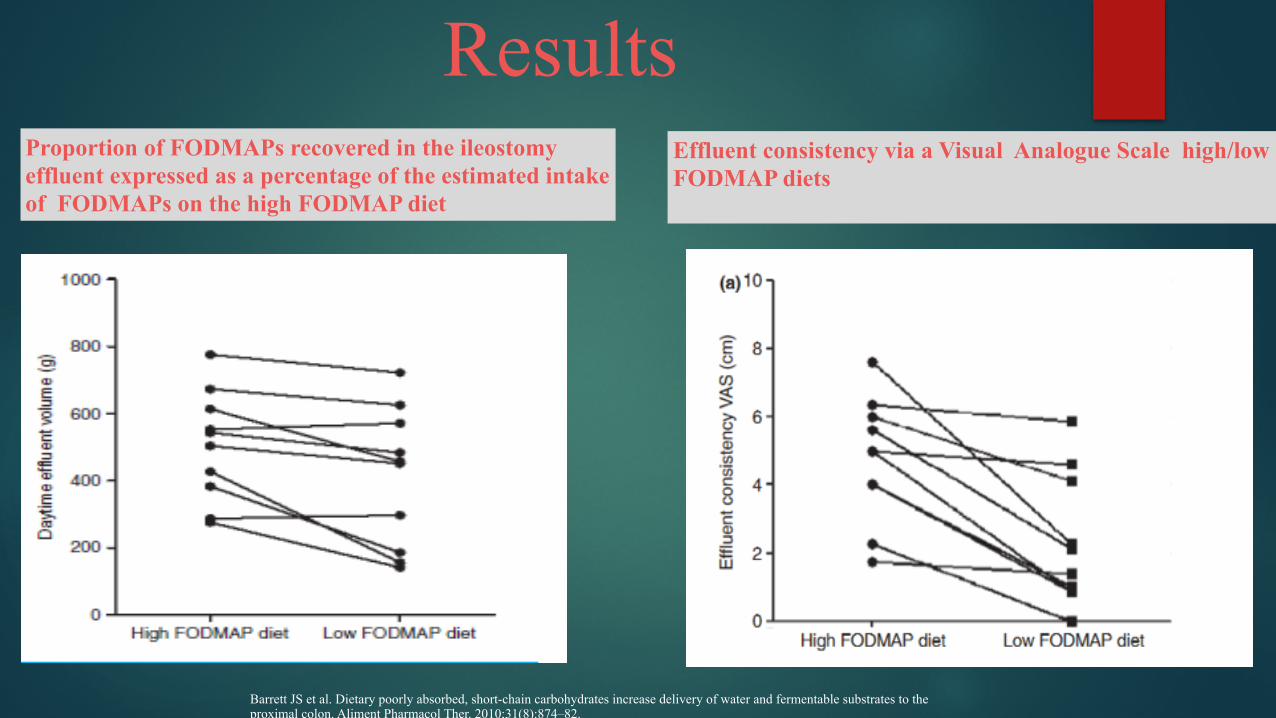
ResultsProportion of FODMAPs recovered in the ileostomy effluent expressed as a percentage of the estimated intake of FODMAPs on the high FODMAP diet
Effluent consistency via a Visual Analogue Scale high/low FODMAP diets
Barrett JS et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. 2010;31(8):874–82.
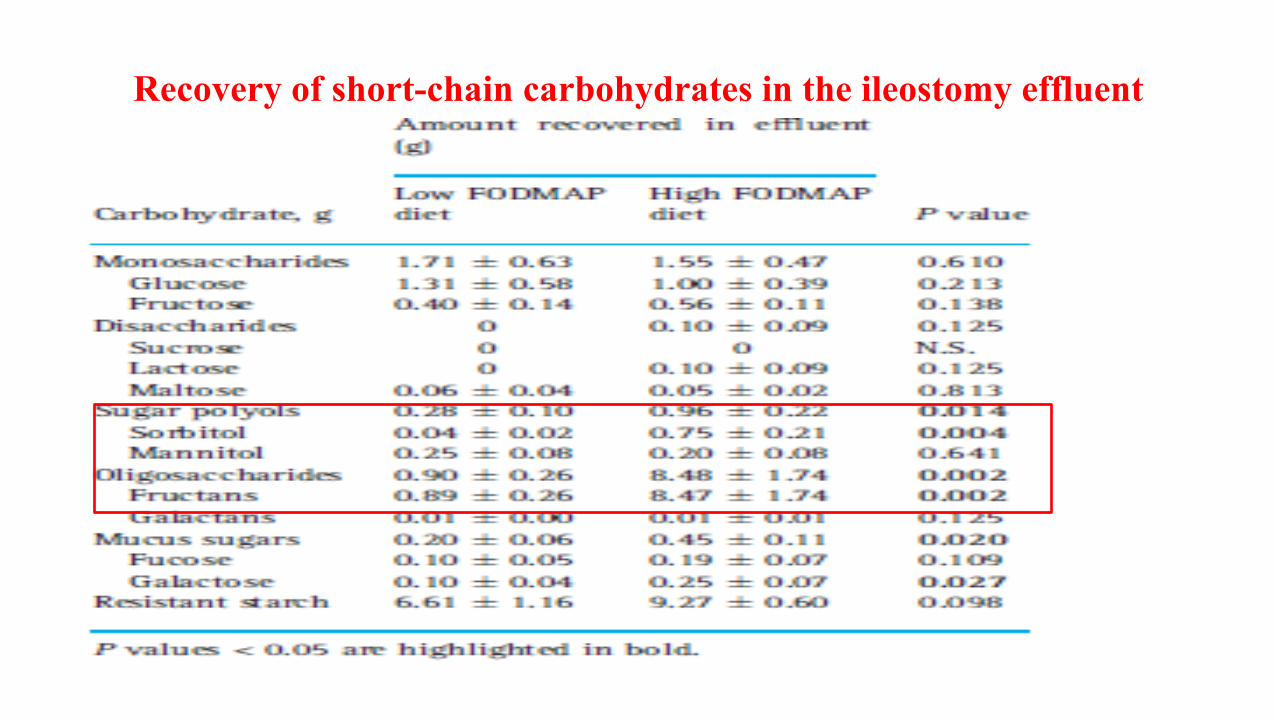
Recovery of short-chain carbohydrates in the ileostomy effluent
Conclusions
!FODMAPs might induce symptoms related to intestinal luminal distension via increasing delivery of water and rapidly fermentable substrates to the proximal colon.
The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: a prospective study
• Objectives: • To determine whether a low FODMAP diet leads to improved symptoms in IBS
patients and which factors are associated with positive outcome.
• Methods: • A prospective observational study of IBS patients • 192 recognized IBS patients referred in the last three years(2009-2011) with performed
breath testing for small intestinal bacterial overgrowth (SIBO), fructose and lactose mal absorption.
• Exclusion criteria: • Patients with Coeliac disease, inflammatory bowel resection or disease were excluded • All probiotics were ceased before the hydrogen breath testing
De Roest RH et al. The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: a prospective study. Int J Clin Pract. 2013 Sep;67(9):895–903
Methods
Questionnaire which contained 20 questions about bowel movement
The same questionnaire was asked at baseline and at follow up.
Retrospective assessment of symptoms improvement on a seven point Likert scale (bloating, abdominal pain/discomfort, etc..) Questions on adherence and satisfaction with the diet
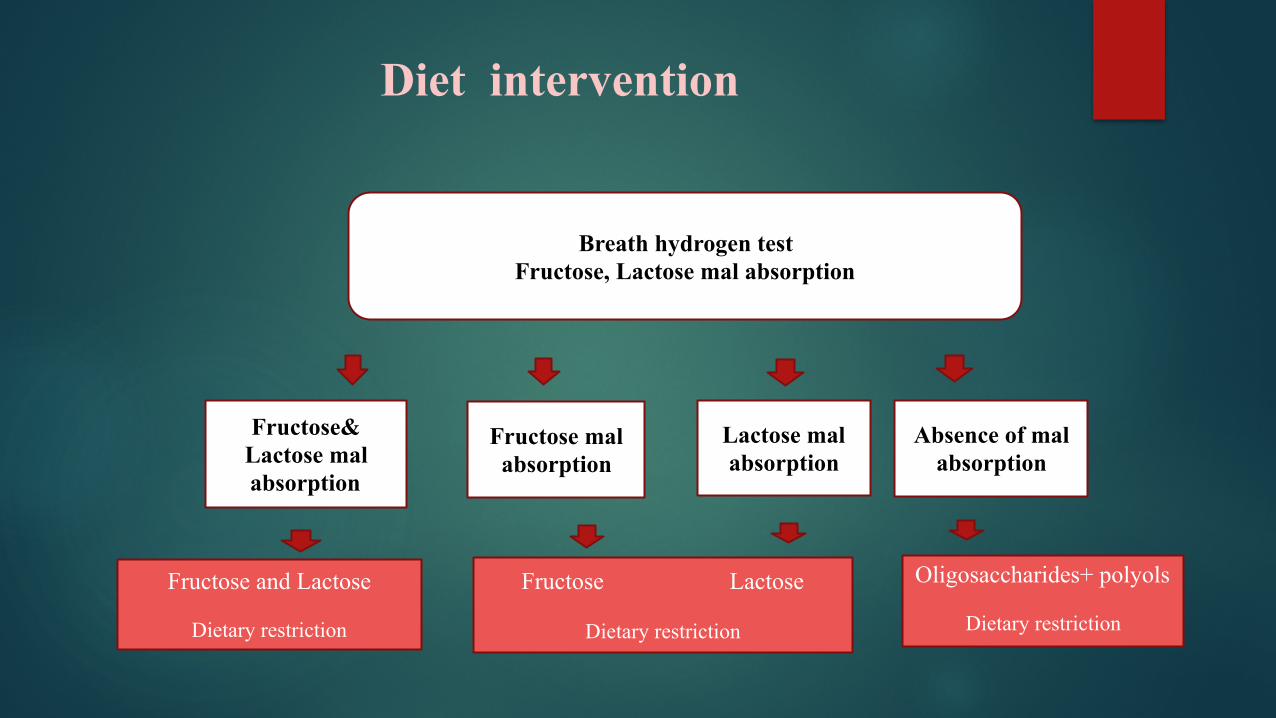
Diet intervention
Breath hydrogen test Fructose, Lactose mal absorption
Fructose& Lactose mal absorption
Fructose mal absorption
Lactose mal absorption
Absence of mal absorption
Fructose and Lactose
Dietary restriction
Fructose Lactose
Dietary restriction
Oligosaccharides+ polyols
Dietary restriction
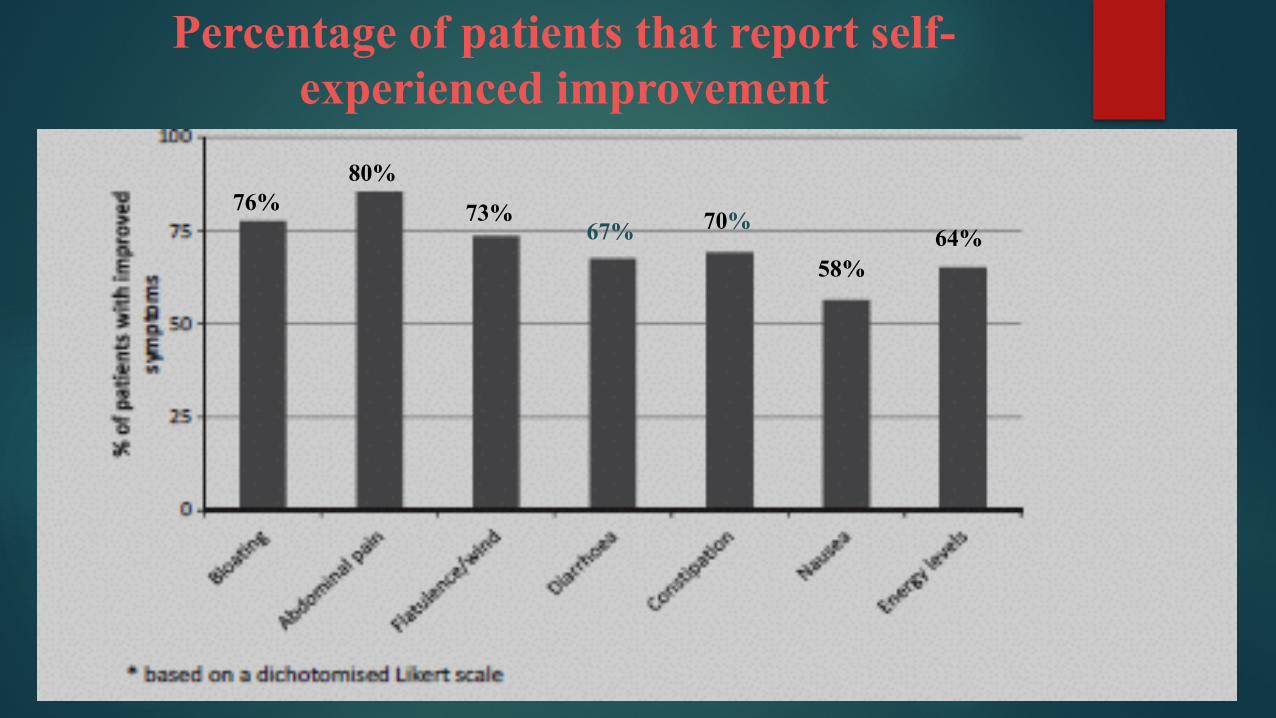
Percentage of patients that report self-experienced improvement
76%80%
73%67% 70%
58%64%
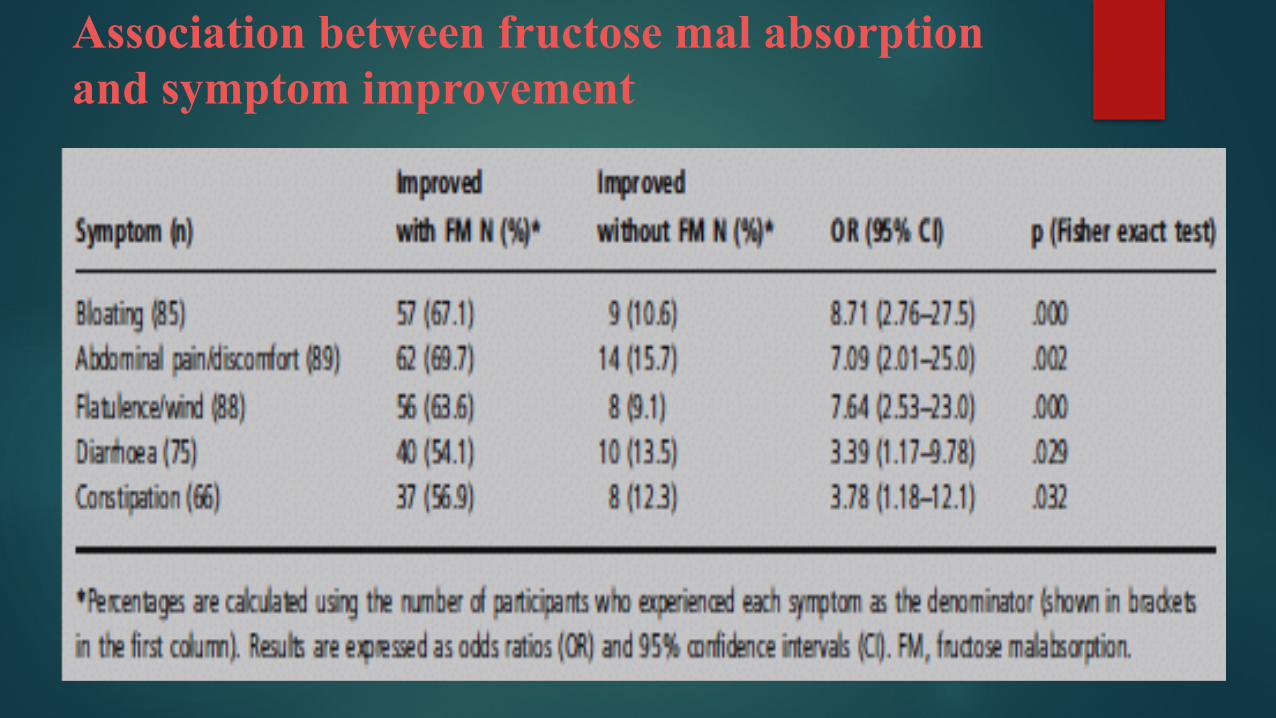
Association between fructose mal absorption and symptom improvement
Conclusions
! Almost all GI symptoms improved significantly with low FODMAP diet.
! Fructose mal absorption was associated with improvement with restricted fructose diet .
Diets that differ in their FODMAP content alter the colonic luminal microenvironment
Objective: To compare the effect of a Low FODMAP diet with a typical Australian diet on biomarkers of colonic health in a single-blinded, randomized, cross-over trial.
Methods: Twenty seven IBS and six healthy subjects were randomly allocated one of two 21-day provided diets low FODMAP diet versus Australian diet and then crossed over to a habitual diet (washout period =21 days). Feces were pooled in both interventional diets (5 days each). PH, short chain fatty acids concentration and bacterial abundance and diversity were assessed.
Halmos EP et al. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut. 2015 Jan 1;6
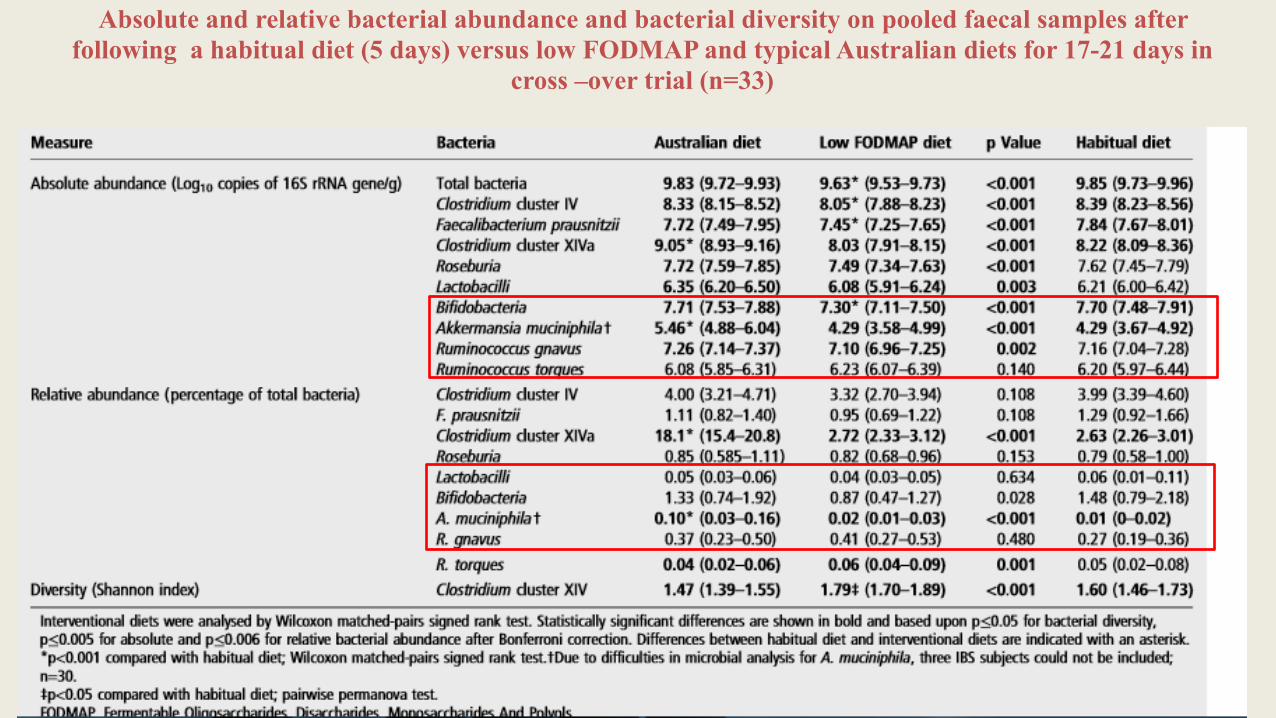
Absolute and relative bacterial abundance and bacterial diversity on pooled faecal samples after following a habitual diet (5 days) versus low FODMAP and typical Australian diets for 17-21 days in
cross –over trial (n=33)
Conclusion
The interventional diets were associated with several differences in faecal microbiota
! The low FODMAP diet was associated with lower absolute abundance of total bacteria, butyrate-producing bacteria and prebiotic bacteria
! Decrease in specific bacterias such as Clostridium cluster XIVa and A. muciniphila
Limitations of FODMAP diet
! Problem in prebiotic intake that can alter the gut microbiota (decrease in Bifidobacteria and butyrate producing Clostridial groups)..
! Problem of nutritional adequacy (Deficiency in calcium) ! The diet is too difficult for most patients to be followed. ! Most food do not list their FODMAP content. The cut off
levels for FODMAP content are not clearly defined
Halmos EP, Power VA, Shepherd SJ, et al. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome.
Gastroenterology 2014;146:67–75
Limitations of FODMAP diet
! Presence of other food related proteins (soy, milk) such as β casein (milk), proteins from spinach (rubisco) or glycoproteins from wheat (lectin) which can activate different aspects of the immune system and causes IBS symptoms.
! Presence of bioactive food chemicals such as salicylates, glutamates, amines, preservatives and coloring agents which can exacerbate the enteric nerves and induce IBS or FBD.
Halmos EP, Power VA, Shepherd SJ, et al. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome.
Gastroenterology 2014;146:67–75.
Conclusion
! The low FODMAP DIET should not be recommended for asymptomatic populations or for people having a functional diarrhea or constipation for a long term use.
! FODMAP restriction should be stopped at the time of controlling symptom.
! Breath test is primordial in order to avoid unnecessary restricted diet.
Other dietary treatments for FBD or IBS
! Use of resistant starch(long chains carbohydrates) such as oat, potatoes, corn or banana. Psyllium (soluble fiber) had been recognized as a supplement to treat IBS.
! Increase the intake of fluid, mainly water up to 1.5 liters/day. Carbonated beverages should be limited.
! Probiotics supplements. ! Decrease large meals and avoid eating quickly ! Decrease fatty meals. Lipids are well recognized to enhance intestinal
motility and visceral sensitivity. ! Elimination diets followed by open rechallenge to identify suspected food.
Chouinard LE. The role of psyllium fibre supplementation in treating irritable bowel syndrome. Can J Diet Pract Res Publ Dietit Can Rev Can Prat Rech En Diététique Une Publ Diététistes Can. 2011;72(1):e107–14
Thank you
References
! Bellentani S, Saccoccio G, Masutti F, Croce LS, Brandi G, Sasso F, et al. Prevalence of and risk factors for hepatic steatosis in Northern Italy. Ann Intern Med 2000; 132:112–7.
! Bernsmeier Christine, Markus H Heim. Stéatose hépatique non alcoolique et Steatohepatitis non alcoolique: manifestation hépatique du syndrome métabolique. forum Med Suisse 2011; 11(4): 53-57.
! Charles S Lieber et al. Model of nonalcoholic steatohepatitis. The American journal of clinical nutrition 2011; 79- 502-9.
! Caroline Romestaing et al. Long term highly saturated fat diet does not induce NASH in Wistar rats. Nutrition and metabolism 2007; 4:4.
! Zheng-Jie Xu et al. Characterization of High-Fat, Diet-Induced, Non-alcoholic Steatohepatitis with Fibrosis in Rats. Springer Science 2010; 55: 931-940.
! Yoneda M, Mawatari H, Fujita K, et al. Current status and agenda in the diagnosis of nonalcoholic steatohepatitis in Japan. World J. Hematology 2010; 2(10): 374-383
! Westwater JO, Fainer D. Liver impairment in the obese. Gastroenterology 1958; 34(4): 686-93.
! P Paschos and K Paletas. Non-alcoholic fatty liver disease and the metabolic syndrome. Hippokratia 2009; 13: 9-19.
! Yamauchi T, Kamon J, Ito Y, et al. Cloning of adiponectin receptors that mediate antidiabetic metabolic effects. Nature 2003; 423(6941): 762-9.
! Kamada Y, Tamura S, Kiso S, et al. Enhanced carbon tetrachloride-induced liver fibrosis in mice lacking adiponectin. Gastroenterology 2003; 125(6): 1796- 807.
! Musso G, Gambino R, Durazzo M, et al. Adipokines in NASH: postprandial lipid metabolism as a link between adiponectin and liver disease. Hepatology 2005; 42: 1175-83.
! Gonzalez FJ. Role of cytochromes P450 in chemical toxicity and oxidative stress: studies with CYP2E1. 2005; 569:101-10.
! Zangar RC, Novak RF. Effects of fatty acids and ketone bodies on cytochromes P450 2B, 4A, and 2E1 expression in primary cultured rat hepatocytes. Arch Biochemical Biophysics 1997; 337: 217-24.
! Chalasani N, Gorski JC, Asghar MS, et al. Hepatic cytochrome P450 2E1 activity in no diabetic patients with nonalcoholic steatohepatitis. Hepatology 2003; 37: 544-50.
! Yamauchi T, Kamon J, Ito Y, et al. Cloning of adiponectin receptors that mediate antidiabetic metabolic effects. Nature 2003; 423(6941): 762-9.
! Kamada Y, Tamura S, Kiso S, et al. Enhanced carbon tetrachloride-induced liver fibrosis in mice lacking adiponectin. Gastroenterology 2003; 125(6): 1796- 807.
! Musso G, Gambino R, Durazzo M, et al. Adipokines in NASH: postprandial lipid metabolism as a link between adiponectin and liver disease. Hepatology 2005; 42: 1175-83.
! Gonzalez FJ. Role of cytochromes P450 in chemical toxicity and oxidative stress: studies with CYP2E1. 2005; 569:101-10.
! Zangar RC, Novak RF. Effects of fatty acids and ketone bodies on cytochromes P450 2B, 4A, and 2E1 expression in primary cultured rat hepatocytes. Arch Biochemical Biophysics 1997; 337: 217-24.
! Chalasani N, Gorski JC, Asghar MS, et al. Hepatic cytochrome P450 2E1 activity in no diabetic patients with nonalcoholic steatohepatitis. Hepatology 2003; 37: 544-50.
! Lieber CS, Leo MA, Mak KM, et al. Model of nonalcoholic steatohepatitis. American J Clinical Nutrition 2004; 79: 502-9.
! Weltman MD, Farrell GC, Liddle C. Increased hepatocyte CYP2E1 expression in a rat nutritional model of hepatic steatosis with inflammation. Gastroenterology 1996; 111:1645-53.
! Caro AA, Cederbaum Al. Oxidative stress, toxicology, and pharmacology of CYP2E1. Annual Revue Pharmacology Toxicology 2004; 44: 27-42.
! Hasegawa T, Yoneda M, Nakamura K, et al. Plasma transforming growth factor- beta1 level and efficacy of alpha-tocopherol in patients with non-alcoholic steatohepatitis: a pilot study. Aliment Pharmacology 2001; 15(10): 1667-72.
! Schuppan D, Afdhal NH. Pathological features of NASH. Front Bioscopy 2005; 10:1475-1484.
! Metin basaranoglu. Understanding mechanisms of the pathogenesis of nonalcoholic fatty liver disease. World journal of gastroenterology 2010; 16(18): 2223-2226.
! Sunil K. Panchal and Lindsay Brown. Rodent Models for Metabolic Syndrome Research. Journal of Biomedicine and Biotechnology 2011.
! Michal Carmiel-Haggai et al. A high-fat diet leads to the progression of non-alcoholic fatty liver disease in obese rats. The FASEB journal 2010.
! Sandra K Erickson. Nonalcoholic fatty liver disease. Journal of lipid research 2011; 50: 412-416.



![Huet & Sayegh Model [memo] · 2. Huet & Sayegh (H&S) Model 2.1 The variable dashpot 2.2 The general H&S model 3. Application of the H&S Model (Examples) 3.1 Porous Asphalt (ZOAB;](https://img.pdfslide.net/doc/110x75/5f031d777e708231d4079c54/huet-sayegh-model-memo-2-huet-sayegh-hs-model-21-the-variable.jpg)