Embed Size (px)
Citation preview

Nicotine dependenceTerry Rustin, MD
Page 1
Nicotine and Tobacco Dependence
Terry A. Rustin, MD, FASAM
Review Course in Addiction Medicine September, 2012
ASAM Disclosure of Relevant Financial Relationships
Content of Activity: ASAM 2012 Review Course
Name Commercial Interests
Relevant Financial
Relationships: What Was Received
Relevant Financial
Relationships: For What
Role
No Relevant Financial
Relationships with Any
Commercial Interests
Terry Rustin Consultant Consultation fees
Developing smoking cessation programs
Physician Salary Assisting patients in quitting smoking
Author Book royalties Author of books on smoking cessation
3

Nicotine dependenceTerry Rustin, MD
Page 2
4
5
6Jean Nicot (1530 – 1600)

Nicotine dependenceTerry Rustin, MD
Page 3
8
All tobacco products have two things in common:
1. Nicotine
9
All tobacco products have two things in common:
2. They kill people

Nicotine dependenceTerry Rustin, MD
Page 4
10
Tobacco kills
• Over 400,000 Americans die every year from diseases caused by tobacco
11
Tobacco kills
• More Americans die from the effects of tobacco than from alcohol, cocaine, heroin, amphetamines, AIDS, suicides, murders, fires, drownings, airplane crashes, car crashes, and the death
penalty… combined
12
4,000 chemicalsin tobacco smoke
• hydrogen cyanide
• carbon monoxide
• formaldehyde
• acetaldehyde
• benzene
• nitrosamines
• pyrethrins
• cadmium
• lead
• arsenic
• radon
• polonium-210

Nicotine dependenceTerry Rustin, MD
Page 5
13
142009 NSDUH survey
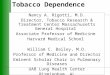
Cigarette use and mental health
• Co-occurring smoking and:• Schizophrenia: 85%
• Major depressive disorder: 60%
• Addictions: 75%
15

Nicotine dependenceTerry Rustin, MD
Page 6
162009 NSDUH survey
172009 NSDUH survey
182009 NSDUH survey

Nicotine dependenceTerry Rustin, MD
Page 7
192009 NSDUH survey
202009 NSDUH survey
.
Physicians: less than 3%
21
2002 2007 2009
Men 52.1 50.5 50.4
Women 38.4 33.6 33.0
All 45.3 41.8 41.6
Tobacco use in the past month,age 18‐25
2002, 2007, 2009 NSDUH survey

Nicotine dependenceTerry Rustin, MD
Page 8
22
Tobacco use and ethnicity, 2009
• American Indians, Alaska natives: 41.8%
• Whites: 29.6 %
• Blacks: 26.5 %
• Hispanics: 23.3 %
• Asians: 11.9 %
• “Mixed races”: 36.6 %
2009 NSDUH survey
Pharmacology of nicotine and smoking
24
Pharmacology of nicotine and smoking
• What’s so special about nicotine?
• What’s so special about smoking?

Nicotine dependenceTerry Rustin, MD
Page 9
At acid pH, most of the nicotine is ionized, and is not readily absorbed. Cigarette smoke is highly acidic.

Nicotine dependenceTerry Rustin, MD
Page 10
At physiologic pH, most of the nicotine is still ionized, and is not readily absorbed. Cigarette smoke entering the lungs must be buffered to physiologic pH before being absorbed.
When the pH of the smoke is raised to alkaline levels, most of the nicotine is no longer ionized, and is readily absorbed across biologic membranes.

Nicotine dependenceTerry Rustin, MD
Page 11
33

Nicotine dependenceTerry Rustin, MD
Page 12
34
Addiction pharmacology
• Tolerance (neuroadaptation)
• Withdrawal
• Mind- and mood-altering effects
• Denial
• Compulsive use
35
36
Tolerance (neuroadaptation)
• Over time, more and more of the drug is required to produce the same effect
• Neuroadaptation to nicotine occurs faster than to most other drugs (10 min)
• Neuroadaptation to the various effects of nicotine occurs at different rates

Nicotine dependenceTerry Rustin, MD
Page 13
37
38
Withdrawal
• The set of signs and symptoms that occur when the drug is decreased or stopped, and which are alleviated when the drug is started again
• Specific to the drug, not the individual
• Nicotine: irritability, agitation, anxiety, difficulty concentrating, bradycardia, insomnia, hunger, labile mood
39

Nicotine dependenceTerry Rustin, MD
Page 14
40
41
Fagerström Testfor Nicotine Dependence
• How soon after you wake up do you smoke your first cigarette?
• <5 minutes = 3 points
• 5-30 minutes = 2 points
• 31-60 minutes = 1 point
• How many cigarettes do you smoke each day?
• >30 cigarettes = 3 points
• 21-30 cigarettes = 2 points
• 11-20 cigarettes = 1 point
Heatherton et al (1991). British Journal of Addictions 86:1119-1127
42
Fagerström Testfor Nicotine Dependence
• Is it hard to refrain from smoking in situation where you should not smoke? • Yes = 1 point No = 0 points
• Which cigarette do you value the most?• First one = 1 point Any other = 0 points
• Do you smoke more in AM?• Yes = 1 point No = 0 points
• Do you smoke if you are ill?• Yes = 1 point No = 0 points
Heatherton et al (1991). British Journal of Addictions 86:1119-1127

Nicotine dependenceTerry Rustin, MD
Page 15
43
Mind- and mood-altering
• Pharmacologically active alkaloid
• High potency (10 mg nicotine in the tobacco; 1-2 mg delivered per cigarette)
• Short half-life (100 minutes)
• Releases dopamine, growth hormone, epinephrine, cortisol
• Effects similar to cocaine, amphetamine
44
45
Denial
• The unconscious resistance to accepting the truth• The observation is true
• The conclusion is false

Nicotine dependenceTerry Rustin, MD
Page 16
46
Denial
• The behavior is perceived as risky or dangerous
• The individual engages in the behavior despite the risk
• A justification is given for engaging in the behavior
47
Perception of Great Risk from Substance Use among Persons Aged 12 to 17, by Gender and Age Group:
2007 and 2008
Risk Gender 12 or 13 14 or 15 16 or 17Smoking One or More Packs of Cigarettes Per Day
Male 67.3% 64.5% 64.5%
Smoking One or More Packs of Cigarettes Per Day
Female 72.1% 73.4% 74.3%
Having Five or More Drinks of Alcohol Once or Twice a Week
Male 40.7% 37.2% 32.3%
Having Five or More Drinks of Alcohol Once or Twice a Week
Female 45.9% 41.9% 42.7%
Source: 2007 and 2008 SAMHSA National Surveys on Drug Use and Health
48

Nicotine dependenceTerry Rustin, MD
Page 17
49
Compulsive use
• Craving: A drive state in which obtaining the chemical seems essential to survival
• Continued use despite consequences
• Inability to quit easily
50
51
Audrey Flack. Royal Flush

Nicotine dependenceTerry Rustin, MD
Page 18
52
53
Smoking cessation treatment
• “Quitting smoking” for individuals who do not have another addiction
• “Recovery from nicotine and tobacco dependence” for individuals who have another addiction

Nicotine dependenceTerry Rustin, MD
Page 19
Smoking cessation treatment
• “Quitting smoking” for individuals who do not have another addiction
NOT CONTROVERSIAL
• “Recovery from nicotine and tobacco dependence” for individuals who have another addiction
Smoking cessation treatment
• “Quitting smoking” for individuals who do not have another addiction
• “Recovery from nicotine and tobacco dependence” for individuals who have another addiction
HIGHLY CONTROVERSIAL
57
Smoking cessation treatment
• Now or later?
• Quit or switch brands?
• Quit or cut down?
• Medication or no medication?

Nicotine dependenceTerry Rustin, MD
Page 20
58
Smoking cessation treatment
• Now or later?
• Quit or switch brands?
• Quit or cut down?
• Medication or no medication?
59
Setting a Quit Day: The single most important contribution a clinician can make
• The patient must select the date, not the clinician
• Two weeks or more in the future
• Choose a date with significance
• Develop a plan to be successful on the Quit Day
60
.

Nicotine dependenceTerry Rustin, MD
Page 21
61
Smoking cessation treatment
• Now or later?
• Quit or switch brands?
• Quit or cut down?
• Medication or no medication?
62Neal Benowitz
63
Smoking cessation treatment
• Now or later?
• Quit or switch brands?
• Quit or cut down?
• Medication or no medication?

Nicotine dependenceTerry Rustin, MD
Page 22
64
Heavy smokers cut down using the nicotine inhaler. Carbon monoxide levels remained constant.
Hurt et al (2000) Nicotine and Tobacco Research
65
Heavy smokers cut down using the nicotine inhaler. Thio-cyanate levels (measure of carcinogenesis) stayed constant.
Hurt et al (2000) Nicotine and Tobacco Research
66
Smoking cessation treatment
• Now or later?
• Quit or switch brands?
• Quit or cut down?
• Medication or no medication?

Nicotine dependenceTerry Rustin, MD
Page 23
67
Medication for smoking cessation
• 85 percent of people who have successfully quit smoking did so without medication
• Use of appropriate medication doubles the success rate in smoking cessation
68
Medications for treating nicotine withdrawal
• Nicotine polacrilex
69

Nicotine dependenceTerry Rustin, MD
Page 24
70
Fortmann et al (1988)JAMA 260:1575-1580
Nicotine gum vs. placebo gum with no
counseling in a research setting
Point prevalence of abstinence at 6 mos
Placebo gum = 22 percent
Nicotine gum = 31 percent
71
Goldstein (1989)AmJPsychiatry, 146:56-60
Nicotine gum with and without counseling in a research setting
Point prevalence of abstinence at 6 mos
Education only = 17.5 percent
Education and counseling = 36.7 percent
72
Nicotine polacrilex (Nicorette®)• Reduces withdrawal
• Convenient
• OTC
• Improves quit rates when combined with counseling
• Pregnancy C
• Unpleasant taste
• Must keep saliva in mouth
• Must chew up to 25 pieces daily
• Must avoid acidic beverages, foods

Nicotine dependenceTerry Rustin, MD
Page 25
73
74
Medications for treating nicotine withdrawal
• Nicotine transdermal systems
75

Nicotine dependenceTerry Rustin, MD
Page 26
76
Hurt et al (1994)JAMA 271:595-600
Nicotine patch vs. placebo patch with
nurse counseling in a research setting
Point prevalence of abstinence at 1 year
Placebo patch = 14.2 percent
Nicotine patch = 27.5 percent
77
Richmond et al (1997)Addiction 92:27-31
Nicotine patch vs. placebo patch with
counseling in general practice (Australia)
Continuous abstinence for 12 months
Placebo patch = 9 percent
Nicotine patch = 19 percent
78
Stapleton et al (1995)Addiction, 90:31-42
Nicotine patch vs. placebo patch, no
counseling in general practice (England)
Continuous abstinence for 12 months
Placebo patch = 4.8 percent
Nicotine patch = 9.6 percent

Nicotine dependenceTerry Rustin, MD
Page 27
79
Nicotine transdermal system• Improves quit rates
• Reduces withdrawal
• Steady-state levels
• Unobtrusive
• 0TC
• Apply once daily
• Pregnancy C
• Skin irritation
• Limited dose range
• Smoking + patch may be a danger
• Start after Quit Date
• Nausea, bad dreams
80
Medications for treating nicotine withdrawal
• Nicotine nasal spray
81
Schneider et al (1995)Addiction, 90:1671-1682
Nicotine nasal spray vs. placebo in a
research setting
Continuous abstinence for 1 year
Placebo nasal spray = 8 percent
Nicotine nasal spray= 18 percent

Nicotine dependenceTerry Rustin, MD
Page 28
82
Nicotine spray (Nicotrol NS®)
• Improves quit rates
• Rapid rise in nicotine levels
• Easy to use
• Pregnancy C
• Addictive potential
• Irritates nasal mucosa
83
Medications for treating nicotine withdrawal
• Nicotine oral inhaler
84
Schneider et al (1996)Addiction, 91:1293-1306
Nicotine oral inhaler vs. placebo oral inhaler, no counseling, research setting
Continuous abstinence for 1 year
Placebo oral inhaler = 8 percent
Nicotine oral inhaler = 13 percent

Nicotine dependenceTerry Rustin, MD
Page 29
85
Nicotine inhaler (Nicotrol®)
• Improves quit rates
• Moderately rapid rise in nicotine levels
• Easy to use
• Pregnancy C
• Addictive potential
• Looks and feels like a cigarette holder
• Kinetics similar to polacrilex
86
Ferry et al (1992)Circulation (abstract supp), 86:I-671
Bupropion 300 mg vs. placebo, treatment for 3 months in a research setting
Continuous abstinence for 6 months
Placebo = 0 percent
Bupropion = 50 percent
87
Hurt et al (1998)NEJM 337:1195-1205
Bupropion (Zyban) in a research setting
Point prevalence of abstinence at 12 months
Placebo = 12 percent
Zyban 100 mg QD = 20 percent
Zyban 150 mg QD = 23 percent
Zyban 150 mg BID = 23 percent

Nicotine dependenceTerry Rustin, MD
Page 30
88
Hurt et al (1998)NEJM 337:1195-1205
Bupropion (Zyban) in a research setting
Weight gain at six weeks
Placebo = 2.9 kg
Zyban 100 mg QD = 2.3 kg
Zyban 150 mg QD = 2.3 kg
Zyban 150 mg BID = 1.5 kg
89
Bupropion (Zyban®)• Improves quit rates
• Reduces withdrawal symptoms
• Reduces craving symptoms
• Reduces depressive symptoms
90
Bupropion (Zyban®)• Weight loss more
common than weight gain
• Well-tolerated by both depressed and nondepressed patients
• Pregnancy B

Nicotine dependenceTerry Rustin, MD
Page 31
91
Bupropion (Zyban®)• Insomnia, dry mouth
• Use caution when combining with antidepressants
• Contraindications: seizure disorders, anorexia/bulimia
92
Bupropion (Zyban®)
• Start with patients in Preparation stage
• For most patients: Set a Quit Date 1-2 weeks in the future
• Start Zyban 1-2 weeks before Quit Date
• Initial dose: 150 mg daily
• Maintenance dose: 150 mg BID
• Continue treatment at least 7 weeks
93
Jorenby et al (1999)NEJM 340:685-91
Bupropion (Zyban) + NTS in a research setting
Point prevalence of abstinence at 10 wks
Placebo = 27 percent
Nicotine patch 21 mg QD only = 33 percent
Zyban 150 mg BID only = 47 percent
Zyban 150 mg BID + patch 21 mg = 53 percent

Nicotine dependenceTerry Rustin, MD
Page 32
94
Bupropion (Zyban®) in combination with the patch
• No significant drug-drug interactions
• Higher quit rates than with either product alone
• Well tolerated in combination
• Increased cost
• Potential increase in side effects
95
Effective combinations
• Nicotine patch plus nicotine gum
• Nicotine patch plus nicotine nasal spray
• Bupropion plus nicotine gum
• Bupropion plus nicotine patch
• Bupropion plus nicotine nasal spray
96

Nicotine dependenceTerry Rustin, MD
Page 33
97
Nicotine
Varenicline
98
Varenicline
• Approved May 11, 2006 by FDA (Pfizer)
• Partial agonist at the acetylcholine-N (nicotine) receptor
• High affinity for the α4β2 subtype
• Trade name: Chantix, Champix
• Derived from natural chemical cytisine, found in the plant “false tobacco”
Foulds (2006) The neurobiological basis for partial agonist treatment of nicotine dependence: varenicline. J Clin Pract 60: 571–576
99
Varenicline
• Excretion is primarily in unchanged form (81 percent)
• Remainder glucuronidated
• Minimal metabolism
• T ½ excretion = 17 ± 3 hours
Orbach et al (2006) Metabolism and disposition of varenicline, a selective alph4-beta2 acetylcholine receptor partial agonist, in vivo and in vitro.. Drug Metabolism and Distribution http://dmd.aspetjournals.org/cgi/content/abstract/34/1/121

Nicotine dependenceTerry Rustin, MD
Page 34
100Orbach et al (2006) Drug Metabolism and Distribution http://dmd.aspetjournals.org/cgi/content/abstract/34/1/121
101
Powledge TM (2004) Nicotine as therapy.PLoS Biol 2(11): e404.
Nicotine receptor
102
http://www.sdsc.edu/
Nicotine receptor (electron micrograph)

Nicotine dependenceTerry Rustin, MD
Page 35
103Foulds (2006) J Clin Pract 60: 571–576
104Foulds (2006) J Clin Pract 60: 571–576
105
N
N = Nicotine

Nicotine dependenceTerry Rustin, MD
Page 36
106
N
107
N
Na+
108
N V
V = VareniclineN = Nicotine

Nicotine dependenceTerry Rustin, MD
Page 37
109
NV
V = VareniclineN = Nicotine
110
N
V
111
N
V

Nicotine dependenceTerry Rustin, MD
Page 38
112
N
V
113
N
V
114
N
V

Nicotine dependenceTerry Rustin, MD
Page 39
115
N
V
116
N
V
Na+
117
Varenicline
• Partial agonist at the acetylcholine-Nurse site—targets the α4β2 receptor
• Reduced craving and withdrawal symptoms
• The most common adverse effects included nausea, headache, trouble sleeping, and abnormal dreams
Pfizer: data on file

Nicotine dependenceTerry Rustin, MD
Page 40
118
Varenicline
• Abstinence at 12 weeks of treatment
Varenicline 44 %
Bupropion 30 %
Placebo 17.7 %
Pfizer: data on file
119
Varenicline
• Abstinence at 12 months of treatment
Varenicline 22.1%
Bupropion 16.4%
Placebo 8.4%
Pfizer: data on file
120

Nicotine dependenceTerry Rustin, MD
Page 41
121
Varenicline
• November 22, 2007: Early communication on suicidal ideation
• July 1, 2009: Black Box Warning
• Risk of psychiatric symptoms, including depression and suicidal ideation
122
WARNING:Serious neuropsychiatric events, including, but not limited to depression, suicidal ideation, suicide attempt and completed suicide have been reported in patients taking CHANTIX. Some reported cases may have been complicated by the symptoms of nicotine withdrawal in patients who stopped smoking. Depressed mood may be a symptom of nicotine withdrawal. Depression, rarely including suicidal ideation, has been reported in smokers undergoing a smoking cessation attempt without medication. However, some of these symptoms have occurred in patients taking CHANTIX who continued to smoke. All patients being treated with CHANTIX should be observed for neuropsychiatric symptoms including changes in behavior, hostility, agitation, depressed mood, and suicide-related events, including ideation, behavior, and attempted suicide. These symptoms, as well as worsening of pre-existing psychiatric illness and completed suicide have been reported in some patients attempting to quit smoking while taking CHANTIX in the post-marketing experience. When symptoms were reported, most were during CHANTIX treatment, but some were following discontinuation of CHANTIX therapy. These events have occurred in patients with and without pre-existing psychiatric disease. Patients with serious psychiatric illness such as schizophrenia, bipolar disorder, and major depressive disorder did not participate in the pre-marketing studies of CHANTIX and the safety and efficacy of CHANTIX in such patients has not been established. Advise patients and caregivers that the patient should stop taking CHANTIX and contact a healthcare provider immediately if agitation, hostility, depressed mood, or changes in behavior or thinking that are not typical for the patient are observed, or if the patient develops suicidal ideation or suicidal behavior. In many post-marketing cases, resolution of symptoms after discontinuation of CHANTIX was reported, although in some cases the symptoms persisted; therefore, ongoing monitoring and supportive care should be provided until symptoms resolve. The risks of CHANTIX should be weighed against the benefits of its use. CHANTIX has been demonstrated to increase the likelihood of abstinence from smoking for as long as one year compared to treatment with placebo. The health benefits of quitting smoking are immediate and substantial. (See WARNINGS/Neuropsychiatric Symptoms and Suicidality, PRECAUTIONS/Information for Patients, and ADVERSE REACTIONS/Post-Marketing Experience)
123

Nicotine dependenceTerry Rustin, MD
Page 42
124
125
Suicidal ideation
• Current smoking is reliably associated with suicide both in case-control and cohort studies. Hypotheses:• Smokers have pre-existing conditions that increase
their risk for suicide• Smoking causes painful and debilitating conditions
that might lead to suicide• Smoking decreases serotonin and monoamine
oxidase levels• Stopping smoking leads to depression in some
smokers; thus, it could induce suicide• Smoking cessation has not been associated with
suicide in the few studies available
Hughes. (2008) Smoking and Suicide: A Brief Overview. Drug Alcohol Depend 98(3): 169–178.
Recovery from nicotine dependence
• Smokers with stable, long-term recovery
• Smokers new in recovery
• Smokers in primary treatment settings

Nicotine dependenceTerry Rustin, MD
Page 43
Recovery from nicotine dependence
• Smokers with stable, long-term recovery
• Smokers new in recovery
• Smokers in primary treatment settings
Baca (2009) J Subst Abuse Treatment 36:205-219
Recovery from nicotine dependence
• Consensus among nicotine dependence experts• Quitting smoking and recovery from nicotine
dependence while in primary addiction treatment is possible, does not interfere with primary addiction recovery, and may be beneficial to recovery
• Addiction treatment episodes are ideal opportunities to address nicotine dependence.
• Becoming a smoke-free treatment environment is necessary but not sufficient to adequately address nicotine dependence during addiction treatment
• The staff will be a bigger problem than the patients

Nicotine dependenceTerry Rustin, MD
Page 44
130
Nicotine as a therapeutic agent
• Use of nicotine ligand for treatment of schizophrenia
• Nicotine protects against lesions in the striatum in rats (possible protective effect from Parkinson’s disease)
• A nicotine ligand suppresses amphetamine-seeking behavior in rats
• Nicotine reduces Alzheimer’s type degeneration
131
132
Nicotine and sensory gating
• The p50 auditory evoked potential (AEP) attenuates with repeated stimuli in normal humans
• Persons diagnosed with schizophrenia do not attenuate the p50 AEP
• After one cigarette, the AEP in patients with schizophrenia normalizes
• The AEP does not normalize with use of the nicotine patch
Adler (1998) Schizophrenia Bulletin, 24(2): 189-202.

Nicotine dependenceTerry Rustin, MD
Page 45
133
Environmental tobacco smoke
• Annoying, messy, insensitive
• Acute respiratory illnesses
• Arteriosclerotic heart disease
• Carcinoma
135

Nicotine dependenceTerry Rustin, MD
Page 46
136Source: Gallup poll
Public health measures
• Increasing the cost of tobacco products• Smokefree buildings and grounds• Decreased availability of cigarettes• Programs to decrease smoking initiation
by children and adolescents• Limiting advertising of cigarettes• Public awareness programs• Information on health risks of smoking

Nicotine dependenceTerry Rustin, MD
Page 47
Percentage of smokers quitting each year
Zhu (2012) Tobacco Control 21:110-118
Quit attempts, quit success, use of cessation aidsZhu (2012) Tobacco Control 21:110-118
Thank you for your participation in the Review Course