Embed Size (px)
Citation preview
Renato Cutrera Dir. U.O.C. Broncopneumologie
Département de Médecine Pédiatrique Hôpital Bambino Gesù, IRCCS, Rome, Italie
R. Cutrera, 2015 -‐ [email protected] 1
NIV indications for children
with rare diseases

R. Cutrera, 2015 -‐ [email protected] 2
A disease or disorder is defined as rare in Europe when it affects fewer than 1 in 2000
PECULIARITA’ DELLE MALATTIE RARE
[email protected] R. Cutrera, 2015 - [email protected] 3
In the EU 30 million people affected over 6000 rare diseases existing.
[email protected] R. Cutrera, 2015 - [email protected] 4
80% of rare diseases have identified genetic origins others are the result of infections (bacterial or viral), allergies and environmental causes, or are degenerative and proliferative. 50% of rare diseases touch children.
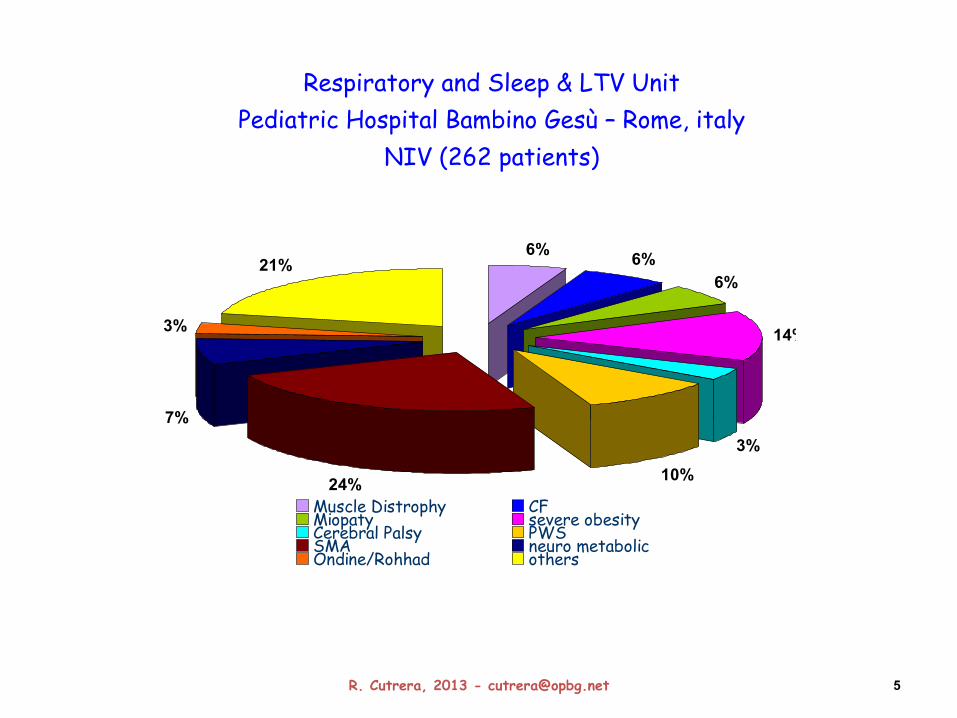
Respiratory and Sleep & LTV Unit Pediatric Hospital Bambino Gesù – Rome, italy
NIV (262 patients)
7%
3%
21%6% 6%
6%
14%
3%
10%24%Muscle Distrophy CFMiopaty severe obesityCerebral Palsy PWSSMA neuro metabolicOndine/Rohhad others
5 R. Cutrera, 2013 - [email protected]
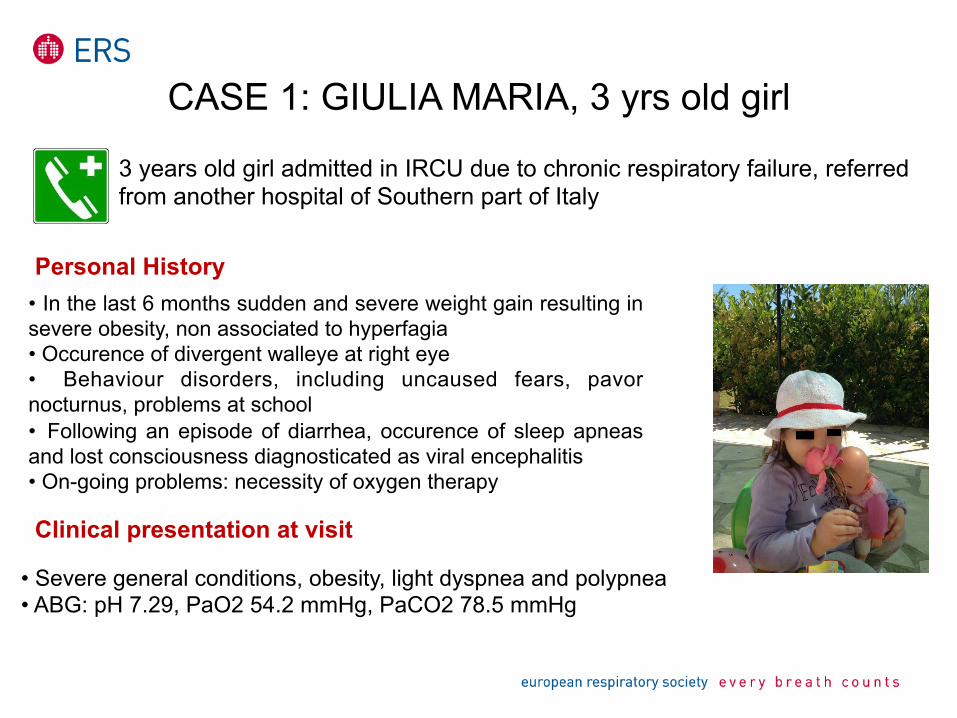
CASE 1: GIULIA MARIA, 3 yrs old girl
3 years old girl admitted in IRCU due to chronic respiratory failure, referred from another hospital of Southern part of Italy
Personal History • In the last 6 months sudden and severe weight gain resulting in severe obesity, non associated to hyperfagia • Occurence of divergent walleye at right eye • Behaviour disorders, including uncaused fears, pavor nocturnus, problems at school • Following an episode of diarrhea, occurence of sleep apneas and lost consciousness diagnosticated as viral encephalitis • On-going problems: necessity of oxygen therapy
Clinical presentation at visit
• Severe general conditions, obesity, light dyspnea and polypnea • ABG: pH 7.29, PaO2 54.2 mmHg, PaCO2 78.5 mmHg
ROHHAD SYNDROME
• Rapid-onset Obesity with Hypothalamic dysfunction, Hypoventilation and Autonomic Dysregulation (ROHHAD syndrome) is a very rare disease affecting approximately only 76 cases worldwide. Patients with ROHHAD have damage to the mechanism governing proper breathing. ROHHAD syndrome is a disease that is potentially lethal and incurable
• Differently from CCHS, a genetic mutation is not identified yet Main symptoms: - hyperphagia and obesity by age of 10 years - (median age 3 years) - respiratory problems (hypoventilation, hypercarbia, OSAS) - thermal or other hypothalamic dysregulations - neurobehavioral disorders - tumors of neural crest origin
Currently there are no official tests or treatments for ROHHAD. Many children are misdiagnosed or are never diagnosed until alveolar hypoventilation occurs.
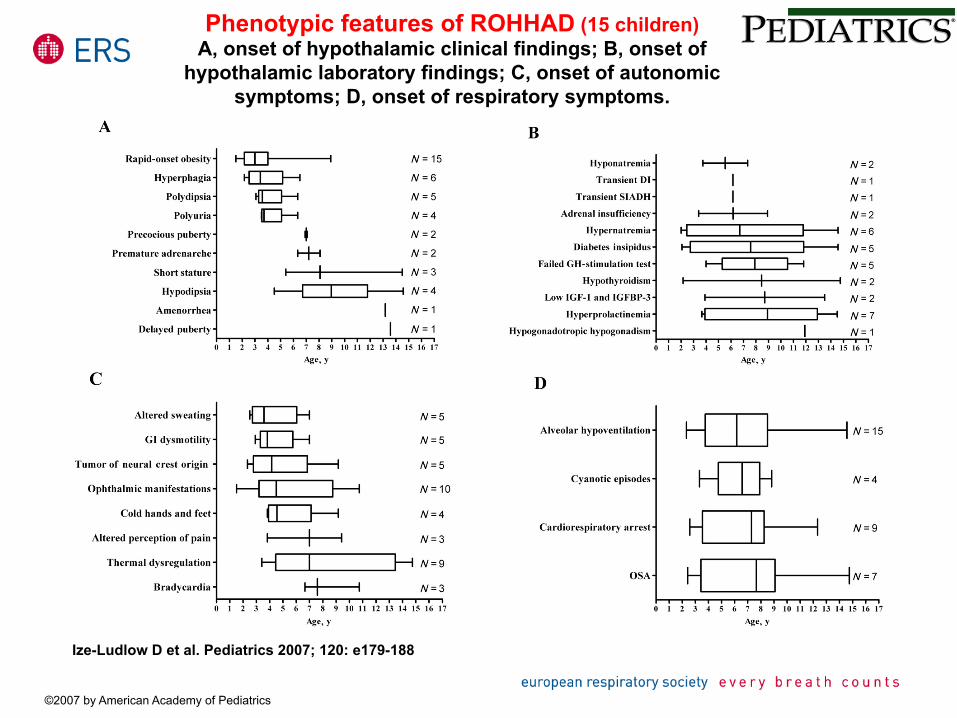
Phenotypic features of ROHHAD (15 children) A, onset of hypothalamic clinical findings; B, onset of
hypothalamic laboratory findings; C, onset of autonomic symptoms; D, onset of respiratory symptoms.
Ize-Ludlow D et al. Pediatrics 2007; 120: e179-188
©2007 by American Academy of Pediatrics
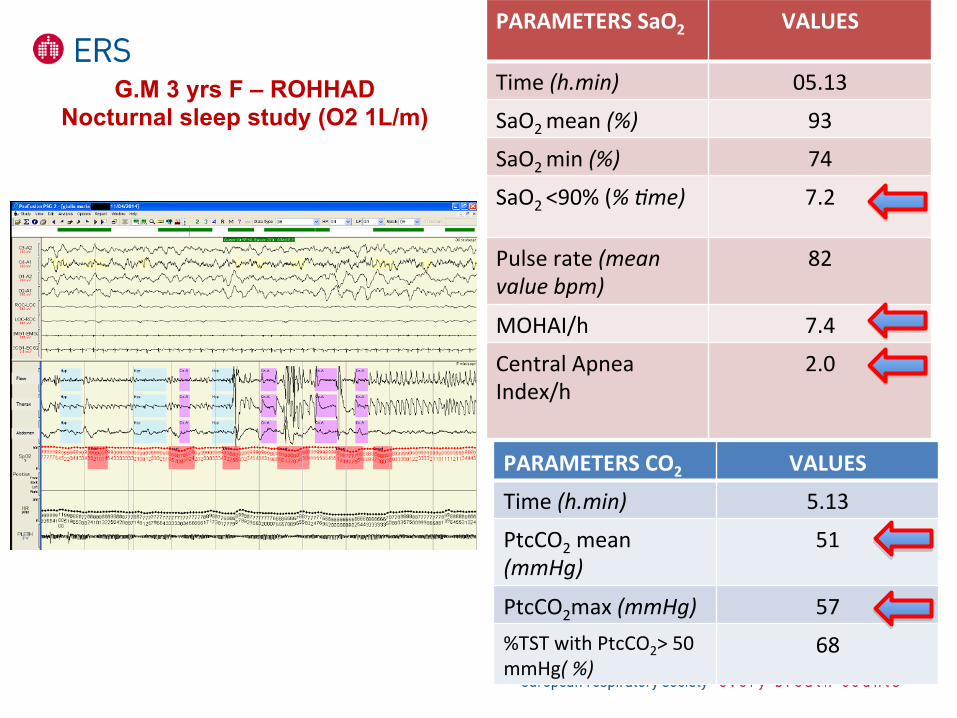
PARAMETERS CO2 VALUES
Time (h.min) 5.13
PtcCO2 mean (mmHg)
51
PtcCO2max (mmHg) 57 %TST with PtcCO2> 50 mmHg( %)
68
PARAMETERS SaO2 VALUES
Time (h.min) 05.13
SaO2 mean (%) 93
SaO2 min (%) 74
SaO2 <90% (% ,me) 7.2
Pulse rate (mean value bpm)
82
MOHAI/h 7.4
Central Apnea Index/h
2.0
G.M 3 yrs F – ROHHAD Nocturnal sleep study (O2 1L/m)
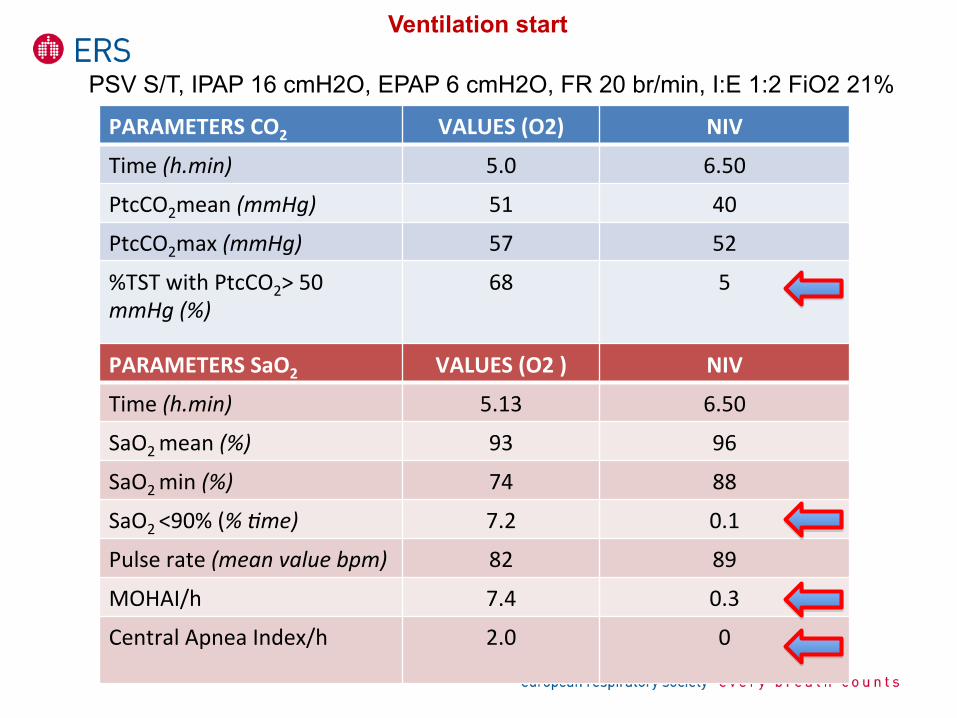
PARAMETERS CO2 VALUES (O2) NIV
Time (h.min) 5.0 6.50
PtcCO2mean (mmHg) 51 40
PtcCO2max (mmHg) 57 52
%TST with PtcCO2> 50 mmHg (%)
68 5
PARAMETERS SaO2 VALUES (O2 ) NIV
Time (h.min) 5.13 6.50
SaO2 mean (%) 93 96
SaO2 min (%) 74 88
SaO2 <90% (% ,me) 7.2 0.1
Pulse rate (mean value bpm) 82 89
MOHAI/h 7.4 0.3
Central Apnea Index/h
2.0 0
Ventilation start
PSV S/T, IPAP 16 cmH2O, EPAP 6 cmH2O, FR 20 br/min, I:E 1:2 FiO2 21%
CASE 2: ARIANNA, 12 months old, F, SMA1
12 months old infant with type 1 spinal muscular atrophy presenting with recurrent episodes of desaturation
Personal History
At the age of 2 months onset of progressive hypotonia, muscle weakness and delayed motor development At the age of 4 months diagnosis of Spinal Muscular Atrophy (SMA) confirmed with a DNA blood test. At the age of 5 months insertion of percutaneous endoscopic gastrostomy (PEG) under local anaesthesia (progressive difficulty in oral feeding - finishing a full meal, weight loss)
R. Cutrera, 2015 -‐ [email protected]
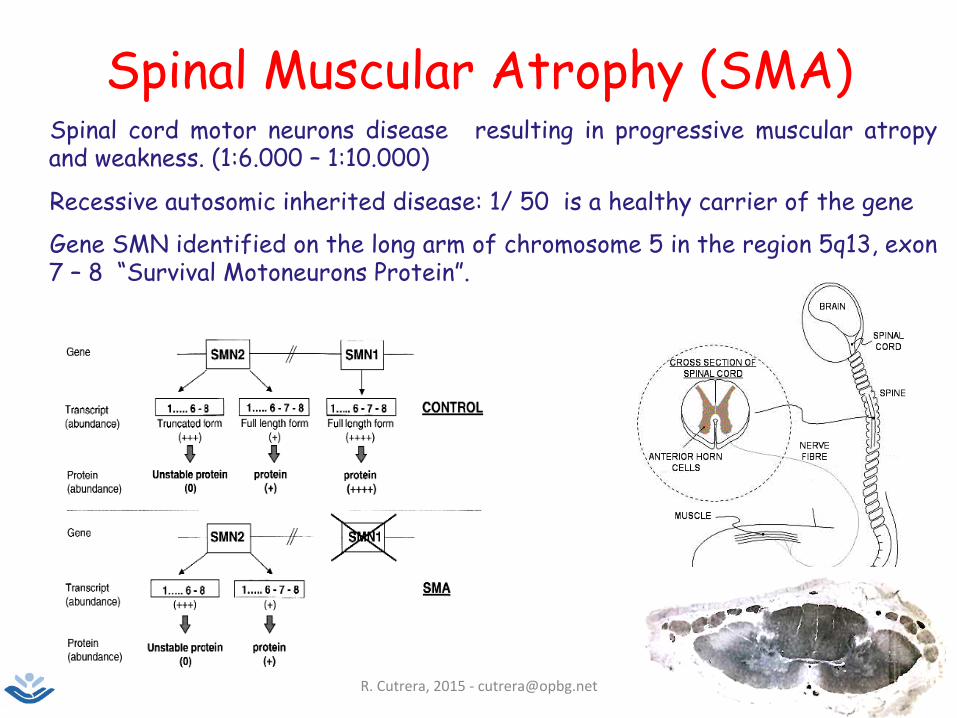
Spinal Muscular Atrophy (SMA) ➼ Spinal cord motor neurons disease resulting in progressive muscular atropy
and weakness. (1:6.000 – 1:10.000)
➼ Recessive autosomic inherited disease: 1/ 50 is a healthy carrier of the gene
➼ Gene SMN identified on the long arm of chromosome 5 in the region 5q13, exon 7 – 8 “Survival Motoneurons Protein”.
R. Cutrera, 2015 -‐ [email protected]
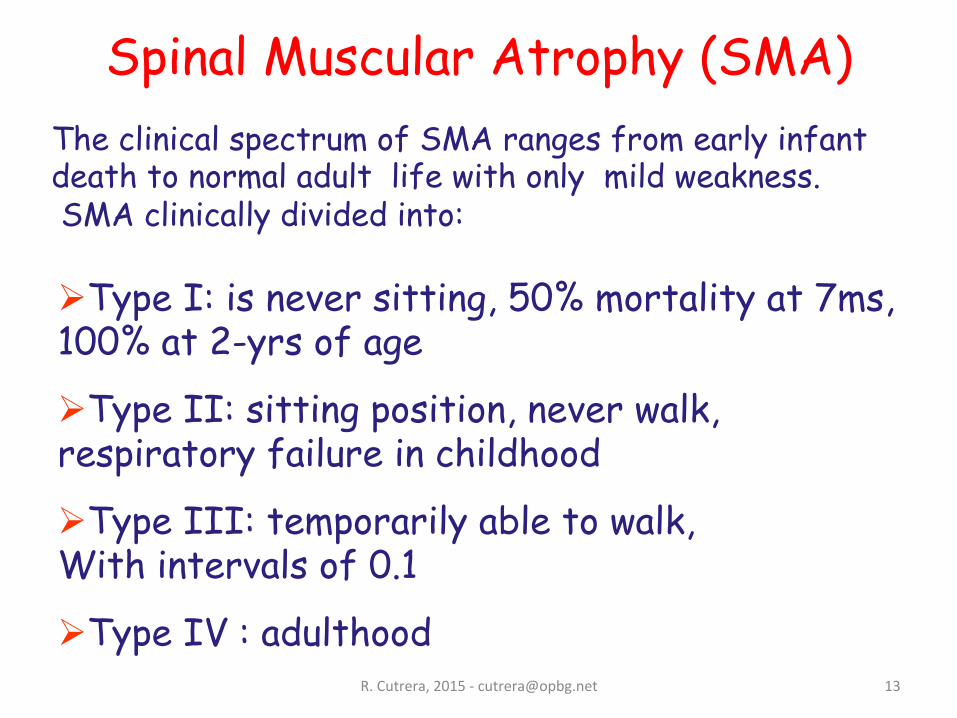
Ø Type I: is never sitting, 50% mortality at 7ms, 100% at 2-yrs of age
Ø Type II: sitting position, never walk, respiratory failure in childhood
Ø Type III: temporarily able to walk, With intervals of 0.1
Ø Type IV : adulthood
The clinical spectrum of SMA ranges from early infant death to normal adult life with only mild weakness. SMA clinically divided into:
Spinal Muscular Atrophy (SMA)
13
R. Cutrera, 2015 -‐ [email protected]
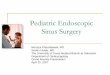
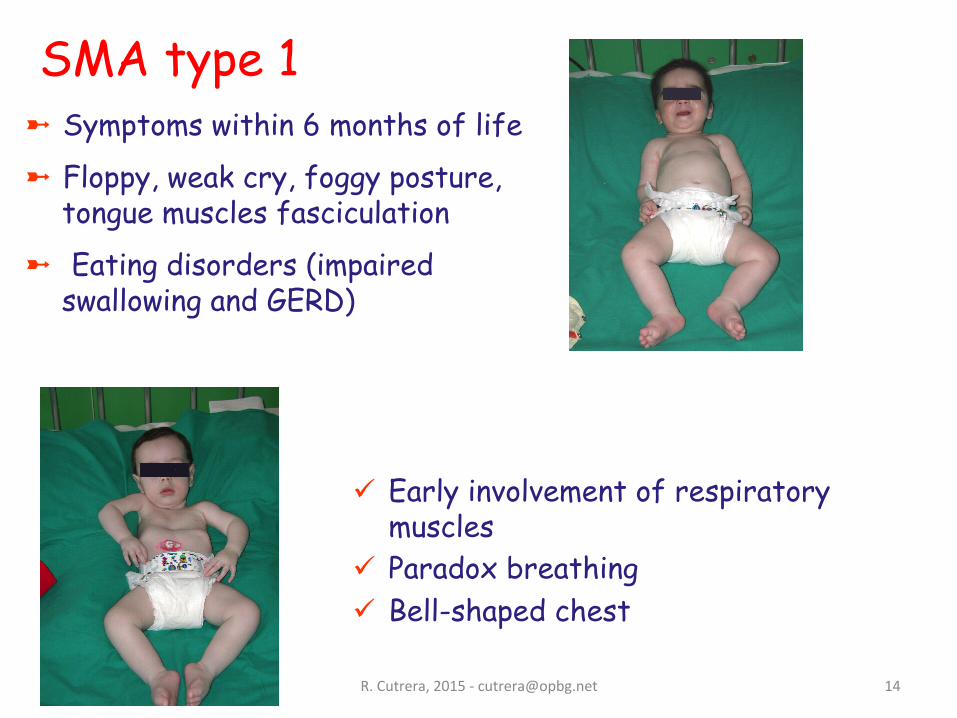
ü Early involvement of respiratory muscles
ü Paradox breathing ü Bell-shaped chest
➼ Symptoms within 6 months of life
➼ Floppy, weak cry, foggy posture, tongue muscles fasciculation
➼ Eating disorders (impaired swallowing and GERD)
SMA type 1
14
R. Cutrera, 2015 -‐ [email protected]
MUSCLE WEAKNESS EFFECTS
3. Lung under development
6. Hypoventilation (sleep awake) and Sleep Disordered Breathing
4. Impaired cough resulting in poor clearance of lower airway secretions
2. Chest wall deformity
5. Recurrent infections that exacerbate muscle weakness
1. Impaired swallowing and GERD
16
R. Cutrera, 2015 -‐ [email protected]
Impaired clearance of secretions
Impaired Cough (expiratory muscles weakness)
A. Simonds Neuromuscular Disorders 14 (2004)56-69
Stasis of thick secretions
Acute and chronic infectious complications
18
R. Cutrera, 2015 -‐ [email protected]
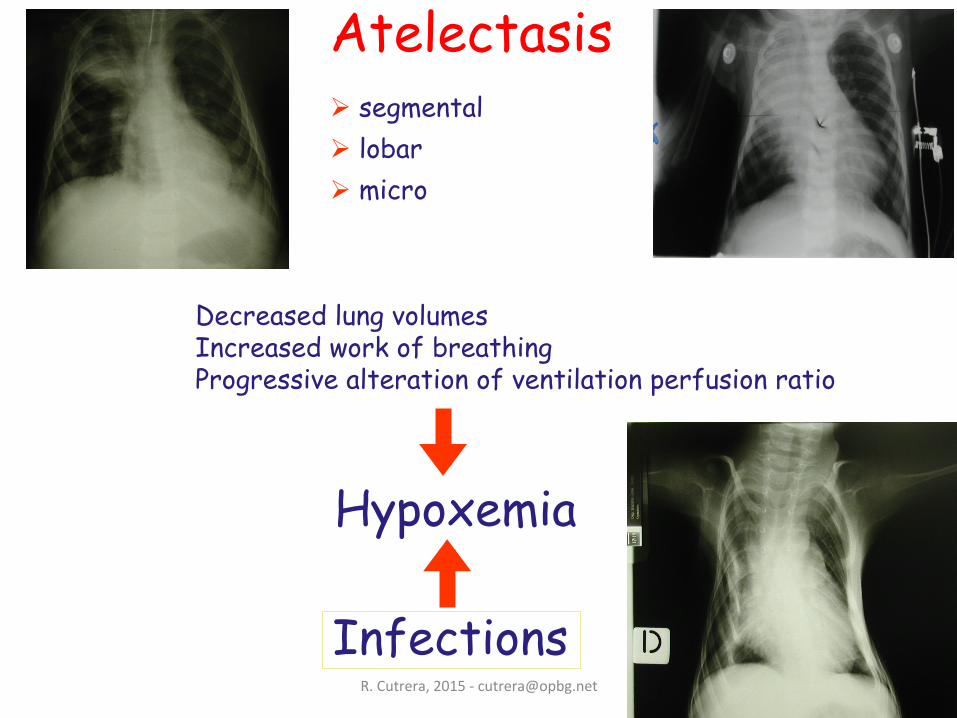
Ø segmental Ø lobar Ø micro
Atelectasis
Infections
Hypoxemia
Decreased lung volumes Increased work of breathing Progressive alteration of ventilation perfusion ratio
19
R. Cutrera, 2015 -‐ [email protected]
Mimics the physiological cough: gradually applying at the airways a positive pressure and immediately after a negative pressure. Removes deep lung secretions Reduces the recurrence of respiratory infections and pulmonary atelectasis
IN EX SUFFLATOR EMERSON
COUGH ASSIST Nippy B&D
Cough Assist Device
COUGH ASSIST (Mini) Pegaso DIMA
COUGH ASSIST Philips E70
20
R. Cutrera, 2015 -‐ [email protected]
Hypoventilation and SBD
Individuals tend to progress to daytime respiratory failure via a sequence of recurrent chest infections, nocturnal oxygen desaturation, nocturnal hypoventilation, and then daytime hypercarbia.
Baseline assessment and longitudinal monitoring can identify those at risk for sleep-disordered breathing and ineffective clearance of secretions.
Ventilatory support should be added at night if sleep-disordered breathing is present and cough assistance provided if cough efficiency is reduced.
21
R. Cutrera, 2015 -‐ [email protected]
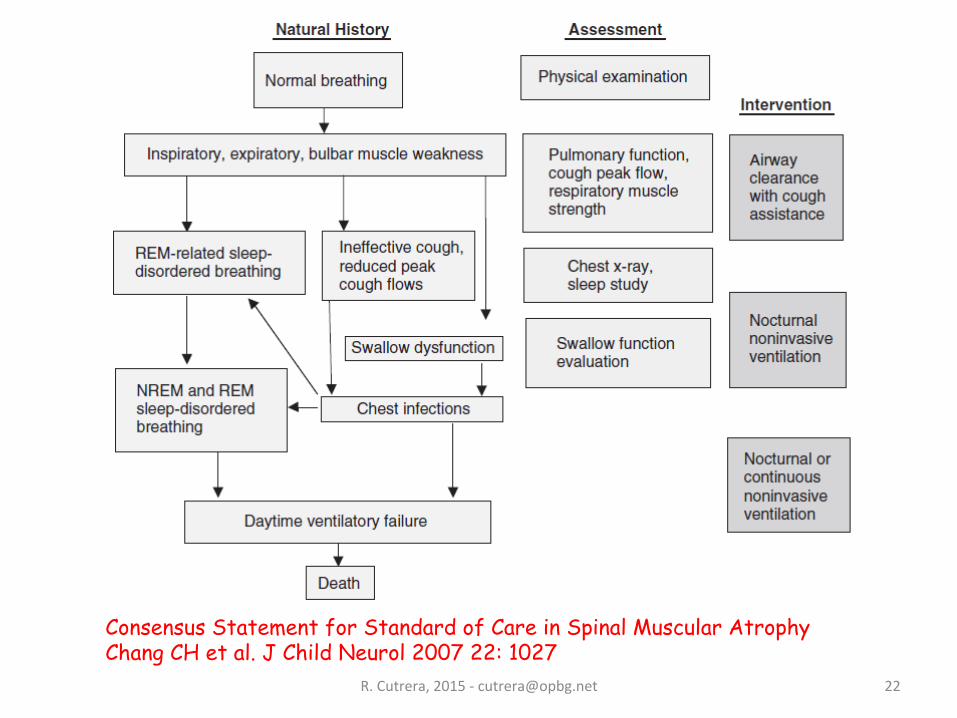
Consensus Statement for Standard of Care in Spinal Muscular Atrophy Chang CH et al. J Child Neurol 2007 22: 1027
22
R. Cutrera, 2015 -‐ [email protected]
Assisted ventilation is used in children with NMW for the following reasons: Ø To treat the symptoms of nocturnal hypoventilation. Ø To treat the symptoms of daytime hypoventilation. Ø To reduce the frequency of hospital admission for chest infections. Ø To prevent chest wall deformity in young children with the expectation of improved long-term outcome. Ø To prolong life.
ASSISTED VENTILATION
23
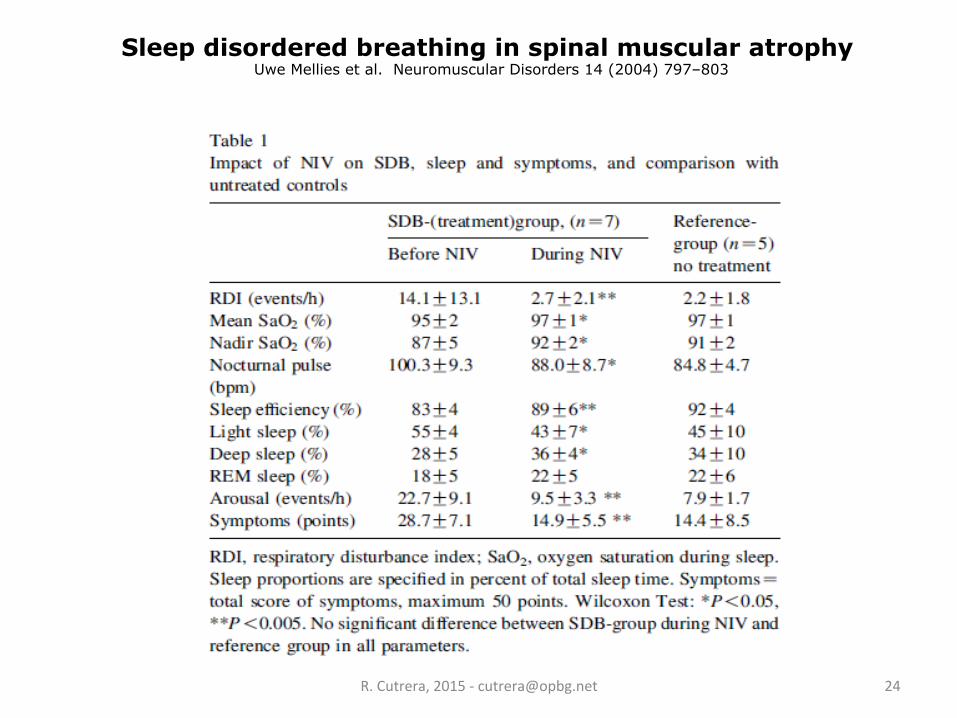
Sleep disordered breathing in spinal muscular atrophy Uwe Mellies et al. Neuromuscular Disorders 14 (2004) 797–803
R. Cutrera, 2015 -‐ [email protected] 24
R. Cutrera, 2015 -‐ [email protected]
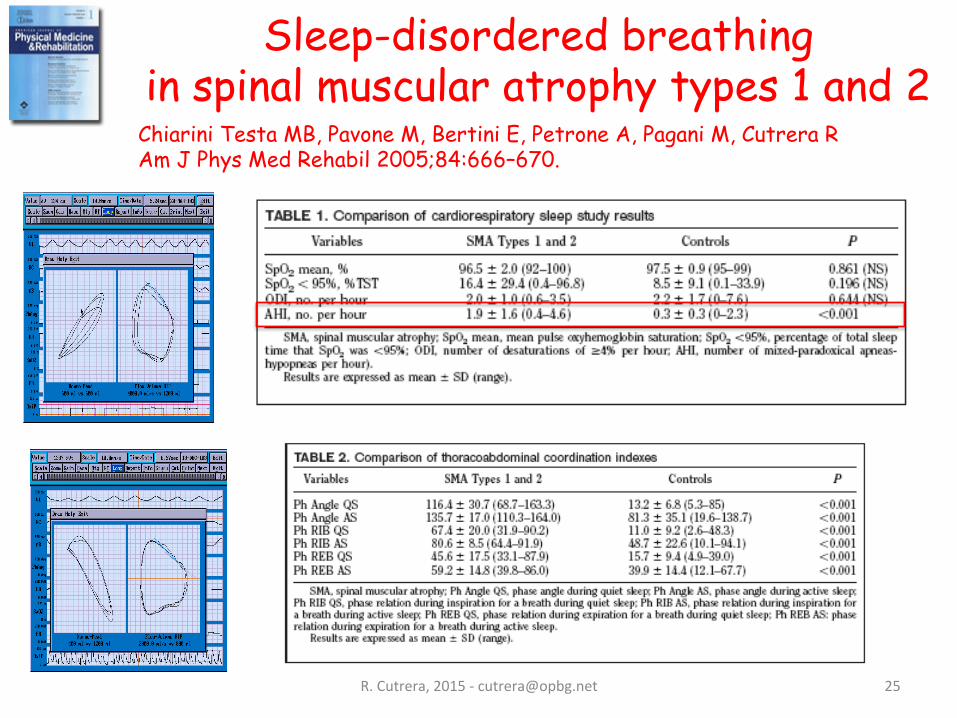
Chiarini Testa MB, Pavone M, Bertini E, Petrone A, Pagani M, Cutrera R Am J Phys Med Rehabil 2005;84:666–670.
Sleep-disordered breathing in spinal muscular atrophy types 1 and 2
25
R. Cutrera, 2015 -‐ [email protected] 26
R. Cutrera, 2015 -‐ [email protected] 27
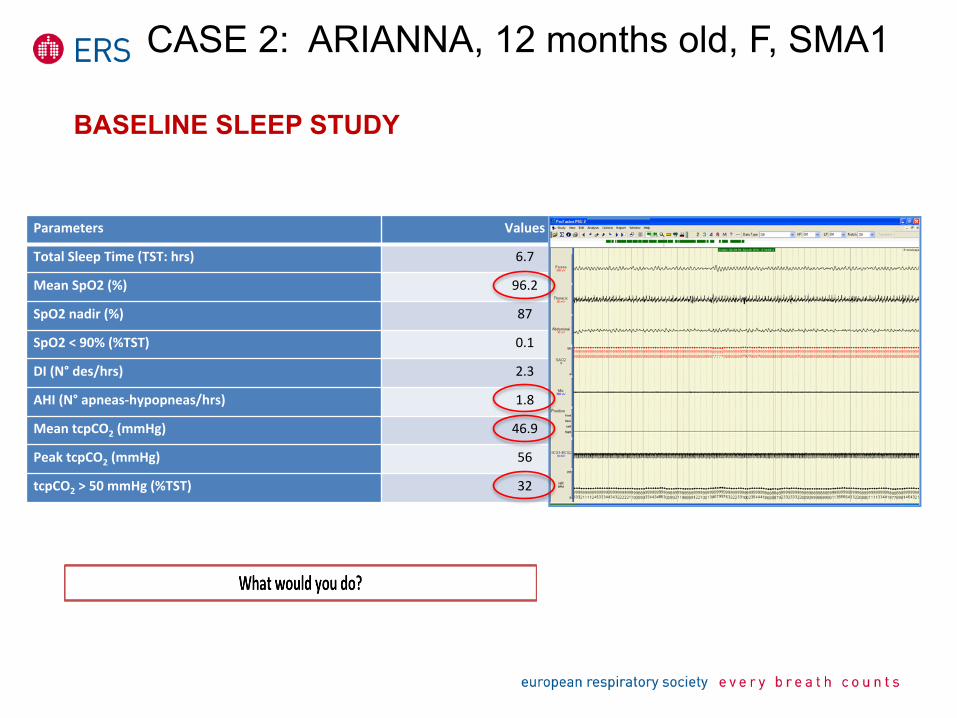
BASELINE SLEEP STUDY
Parameters Values
Total Sleep Time (TST: hrs) 6.7
Mean SpO2 (%) 96.2
SpO2 nadir (%) 87
SpO2 < 90% (%TST) 0.1
DI (N° des/hrs) 2.3
AHI (N° apneas-‐hypopneas/hrs) 1.8
Mean tcpCO2 (mmHg) 46.9
Peak tcpCO2 (mmHg) 56
tcpCO2 > 50 mmHg (%TST) 32
CASE 2: ARIANNA, 12 months old, F, SMA1
Treatment Options suggested to parents of children with SMA type 1
1. Let the Nature “take its course”: Home discharge without mechanical ventilation but with support for feeding and treatment for pain and dyspnoea and education to prevent and treat acute respiratory deterioration + MI-E
2. Home discharge with 1 + low span mechanical IPPV + MI-E
3. Home discharge with 1 +High span IPPV MI-E 4. Tracheal ventilation
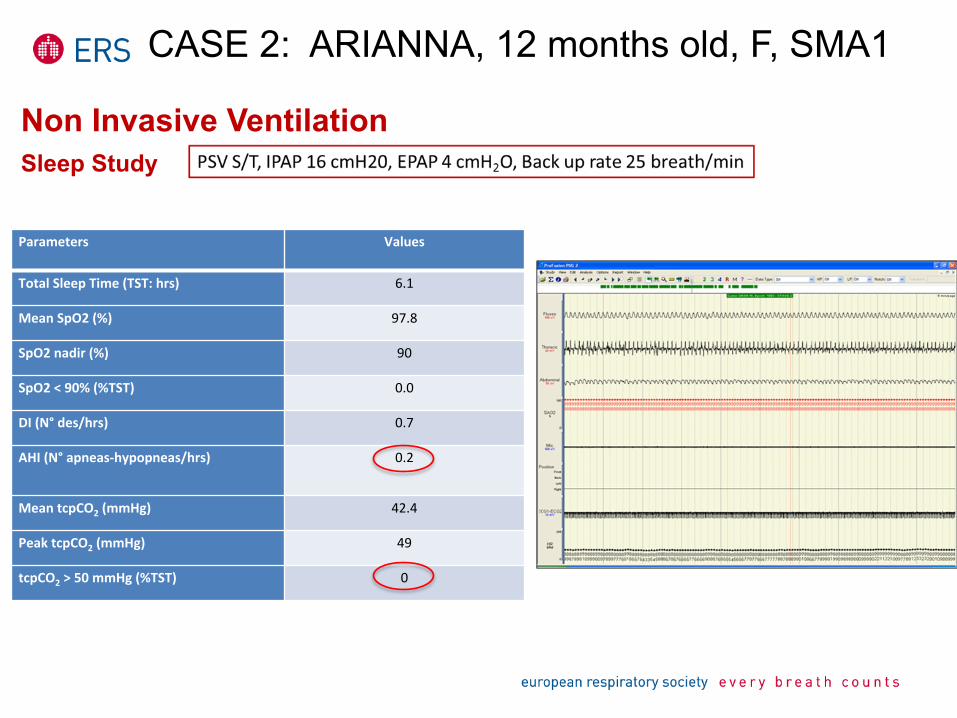
Non Invasive Ventilation
Parameters Values
Total Sleep Time (TST: hrs) 6.1
Mean SpO2 (%) 97.8
SpO2 nadir (%) 90
SpO2 < 90% (%TST) 0.0
DI (N° des/hrs) 0.7
AHI (N° apneas-‐hypopneas/hrs) 0.2
Mean tcpCO2 (mmHg) 42.4
Peak tcpCO2 (mmHg) 49
tcpCO2 > 50 mmHg (%TST) 0
Sleep Study
CASE 2: ARIANNA, 12 months old, F, SMA1
DISCHARGE PLANE
Mechanical assisted cough The use of a mechanical insufflator/exsufflator via a face mask increases peak cough flow and aids airway clearance Other techniques such as breath stacking with bag, mask and one-way valve and manually assisted coughs can be very useful in older children who are able to understand commands but are not applicable to infants with severe type 1 SMA
Oxygen - Home SpO2 monitoring Low-flow home oxygen should be considered for symptom relief in case of acute cyanotic attacks. However, practitioners should be aware that oxygen may mask worsening hypoventilation in the presence of hypercapnia by reducing respiratory drive.
Non-invasive ventilation (NIV) Non-invasive ventilation delivered via a mask attached with straps to the child's face “interface” as bi-level cycling between a higher and lower positive pressure to the follows setting ( PSV S/T, IPAP 16 cmH20, EPAP 4 cmH2O, Back up rate 25 breath/min) In this case the use of NIV can have a beneficial impact on chest shape, reducing the development of pectus excavatum
Enteral feeding
Nex visit, scheduled in one month .
CASE 2: ARIANNA, 12 months old, F, SMA1
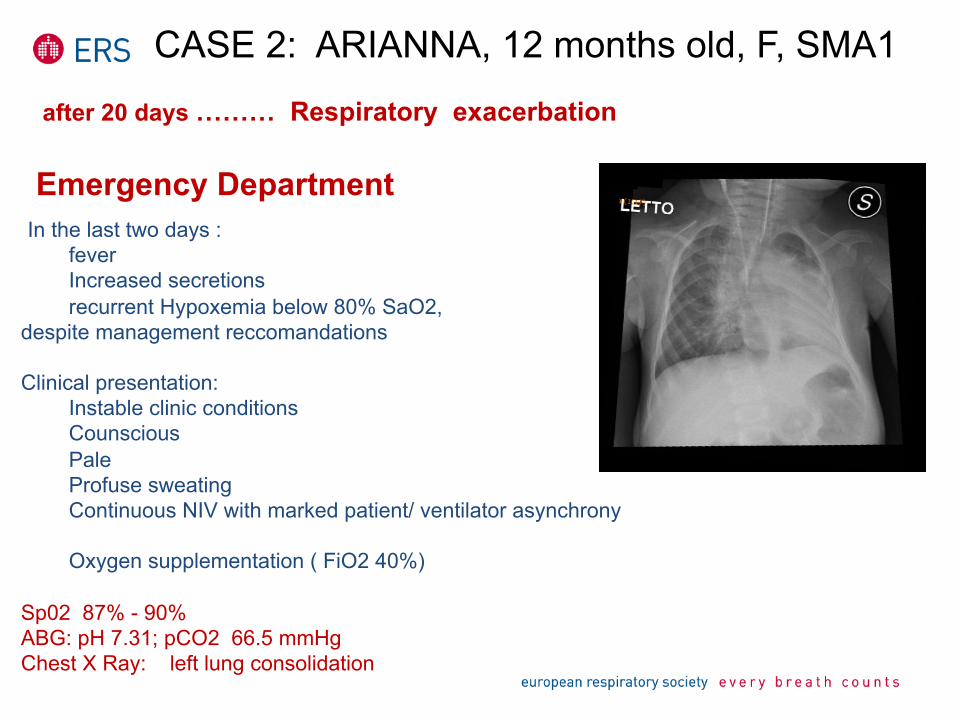
after 20 days ……… Respiratory exacerbation Emergency Department
In the last two days : fever Increased secretions recurrent Hypoxemia below 80% SaO2,
despite management reccomandations
Clinical presentation: Instable clinic conditions Counscious
Pale Profuse sweating Continuous NIV with marked patient/ ventilator asynchrony Oxygen supplementation ( FiO2 40%) Sp02 87% - 90% ABG: pH 7.31; pCO2 66.5 mmHg Chest X Ray: left lung consolidation
CASE 2: ARIANNA, 12 months old, F, SMA1
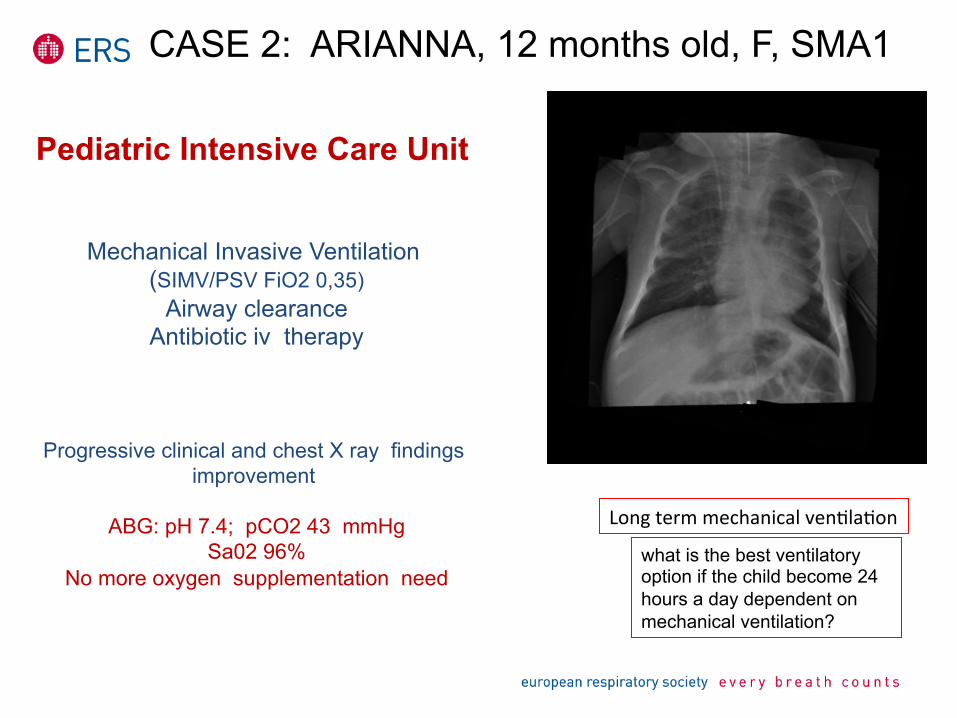
Pediatric Intensive Care Unit
Mechanical Invasive Ventilation (SIMV/PSV FiO2 0,35)
Airway clearance Antibiotic iv therapy
Progressive clinical and chest X ray findings improvement
ABG: pH 7.4; pCO2 43 mmHg
Sa02 96% No more oxygen supplementation need
what is the best ventilatory option if the child become 24 hours a day dependent on mechanical ventilation?
Long term mechanical venXlaXon
CASE 2: ARIANNA, 12 months old, F, SMA1
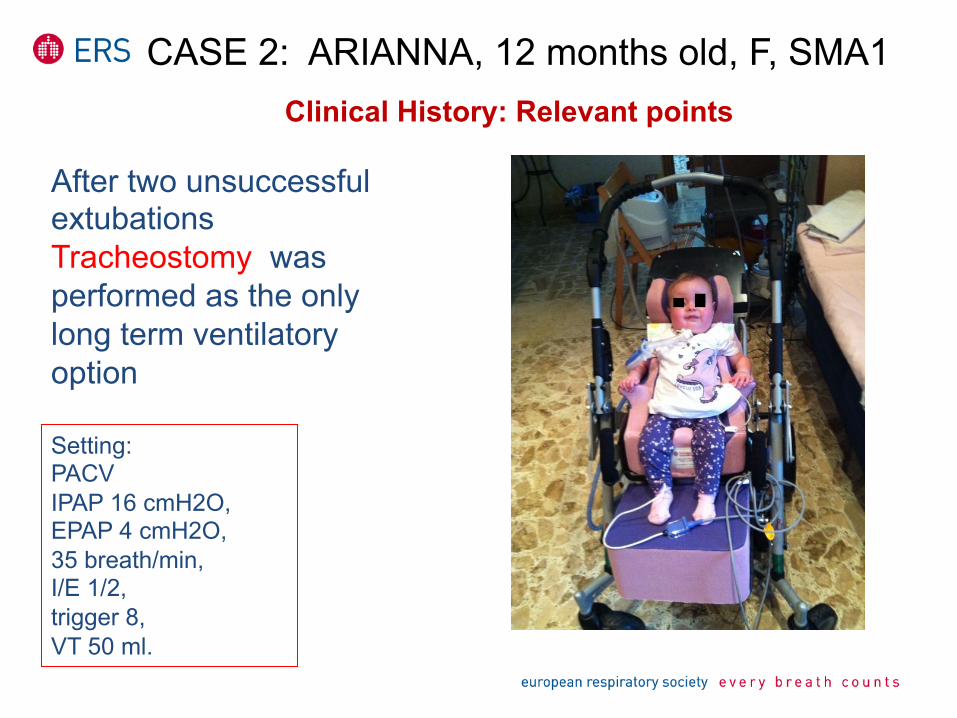
Clinical History: Relevant points
After two unsuccessful extubations Tracheostomy was performed as the only long term ventilatory option
Setting: PACV IPAP 16 cmH2O, EPAP 4 cmH2O, 35 breath/min, I/E 1/2, trigger 8, VT 50 ml.
CASE 2: ARIANNA, 12 months old, F, SMA1
R. Cutrera, 2015 -‐ [email protected] 35
R. Cutrera, 2015 -‐ [email protected]
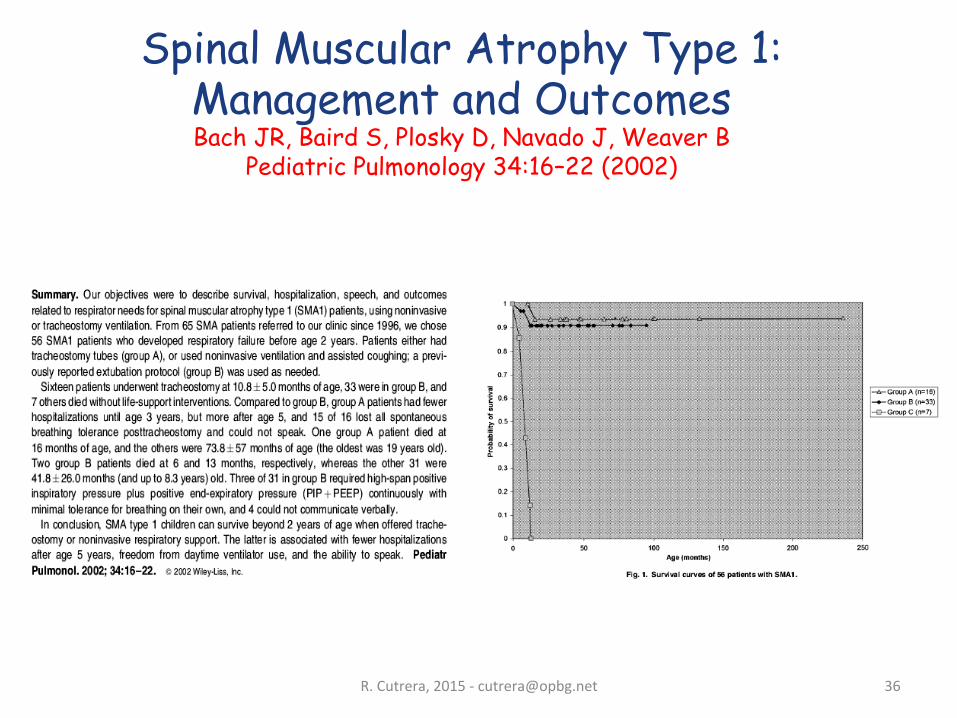
Spinal Muscular Atrophy Type 1: Management and Outcomes Bach JR, Baird S, Plosky D, Navado J, Weaver B
Pediatric Pulmonology 34:16–22 (2002)
36
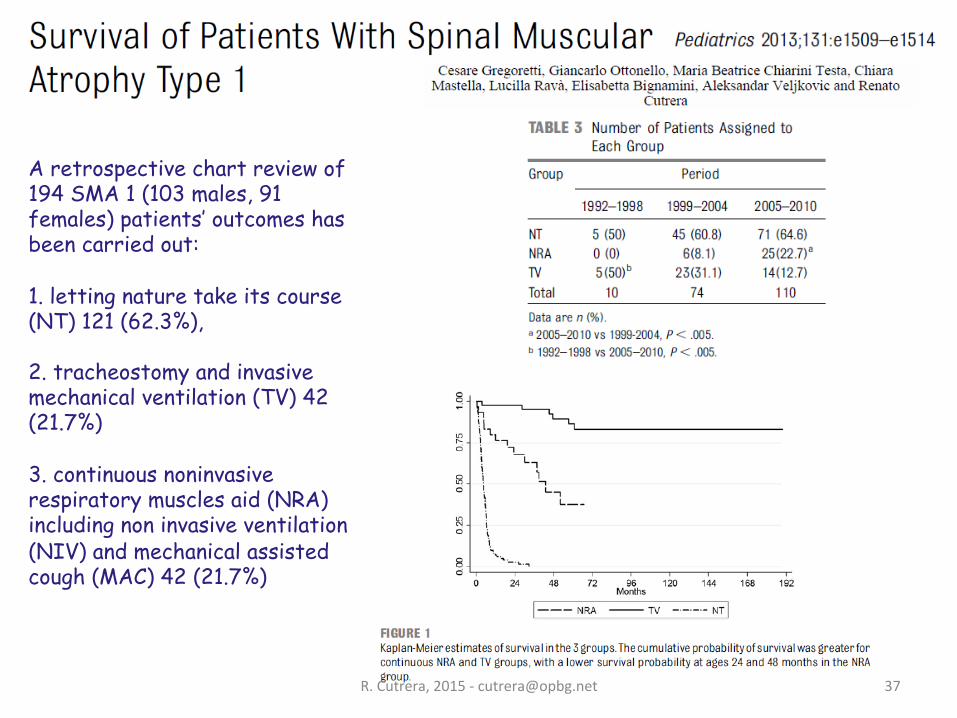
A retrospective chart review of 194 SMA 1 (103 males, 91 females) patients’ outcomes has been carried out: 1. letting nature take its course (NT) 121 (62.3%), 2. tracheostomy and invasive mechanical ventilation (TV) 42 (21.7%) 3. continuous noninvasive respiratory muscles aid (NRA) including non invasive ventilation (NIV) and mechanical assisted cough (MAC) 42 (21.7%)
R. Cutrera, 2015 -‐ [email protected] 37
R. Cutrera, 2015 -‐ [email protected] 38
R. Cutrera, 2015 -‐ [email protected]
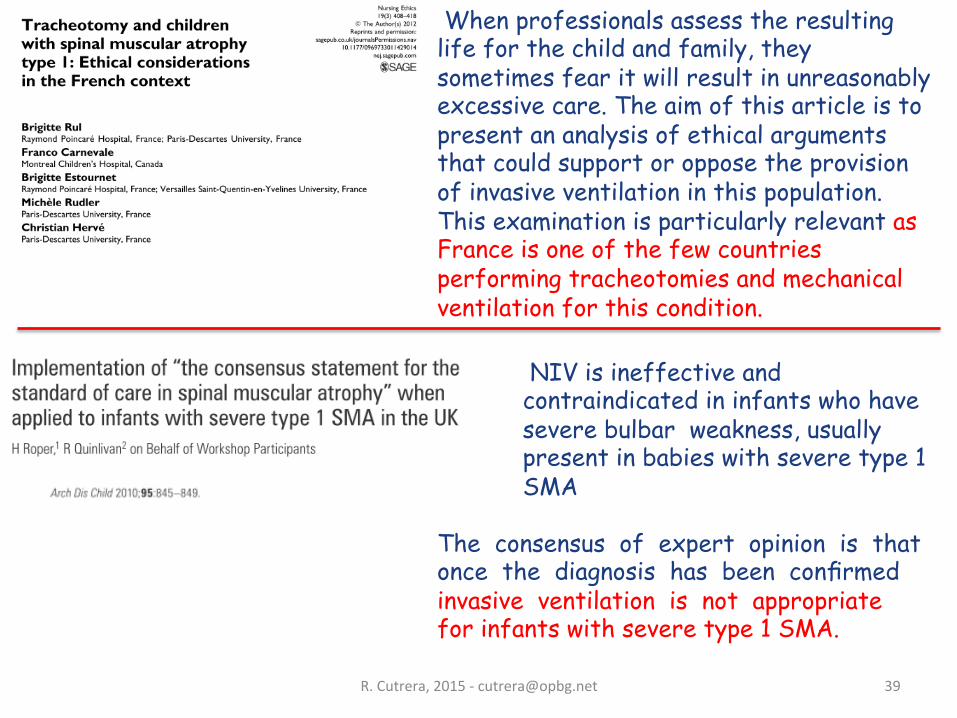
NIV is ineffective and contraindicated in infants who have severe bulbar weakness, usually present in babies with severe type 1 SMA
The consensus of expert opinion is that once the diagnosis has been confirmed invasive ventilation is not appropriate for infants with severe type 1 SMA.
When professionals assess the resulting life for the child and family, they sometimes fear it will result in unreasonably excessive care. The aim of this article is to present an analysis of ethical arguments that could support or oppose the provision of invasive ventilation in this population. This examination is particularly relevant as France is one of the few countries performing tracheotomies and mechanical ventilation for this condition.
39
R. Cutrera, 2015 -‐ [email protected] 40
SMA1 - 69 pts (2002-2014)
-
- 69 pts (31 M ; 38 F) - 53 dead (some of theme palliative NIV) - 16 alive: - 12 invasive ventilation (tracheo) - 3 in therapeutic NIV: 1. VC, F, 2ys and 5 ms, diagnosis at 10 ms, NIV at18 ms. 2. RG, M, 23 ms, diagnosis and NIV at 4 ms 3. QR, M, 31 ms, diagnosi and NIV at 5 ms - 1 new diagnosis at 6 ms in palliative NIV
Average age at diagnosis 4 months Average age at death 11.5 months Average age at tracheotomy 11.6 months
R. Cutrera, 2015 -‐ [email protected] 41
SMA2 - 55 pts (2002-2014)
- 55 pts (29 M ; 26 F) - 49 alive: 36 in therapeutic NIV 1 invasive ventilation (tracheo) 12 spontaneous breathing - 2 dead: case1 NIV at 24 mts, death at 42 mts; case2 NIV at 5yrs, death at 20 yrs - 4 lost at follow up
Average age at diagnosis 17 months Average age at NIV 5 yrs
R. Cutrera, 2015 -‐ [email protected] 42

R. Cutrera, 2015 -‐ [email protected] 43

R. Cutrera, 2015 -‐ [email protected] 44