-
Safety and Antitumor Activity of AntiPD-1 Antibody,Nivolumab, in
Patients With Platinum-ResistantOvarian CancerJunzo Hamanishi,
Masaki Mandai, Takafumi Ikeda, Manabu Minami, Atsushi
Kawaguchi,Toshinori Murayama, Masashi Kanai, Yukiko Mori, Shigemi
Matsumoto, Shunsuke Chikuma,Noriomi Matsumura, Kaoru Abiko, Tsukasa
Baba, Ken Yamaguchi, Akihiko Ueda, Yuko Hosoe,Satoshi Morita,
Masayuki Yokode, Akira Shimizu, Tasuku Honjo, and Ikuo Konishi
Junzo Hamanishi, Masashi Kanai,Yukiko Mori, Shigemi
Matsumoto,Shunsuke Chikuma, NoriomiMatsumura, Kaoru Abiko,
TsukasaBaba, Ken Yamaguchi, Akihiko Ueda,Yuko Hosoe, Tasuku Honjo,
and IkuoKonishi, Kyoto University GraduateSchool of Medicine,
Kyoto, Japan;Masaki Mandai, Kinki University Facultyof Medicine,
Osaka, Japan; and Taka-fumi Ikeda, Manabu Minami, AtsushiKawaguchi,
Toshinori Murayama,Satoshi Morita, Masayuki Yokode, andAkira
Shimizu, Kyoto University Hospi-tal, Kyoto, Japan.
Published online ahead of print atwww.jco.org on September 8,
2015.
Supported by research funds fromHealth and Labour Sciences
ResearchGrant No. 11104959 (to J.H. and I.K.);by Translational
Research NetworkProgram of the Ministry of Education,Culture,
Sports, Science and Technol-ogy of Japan Grant No. 2013037 (toJ.H.
and I.K.); and by Kyoto Universitygrants.
Both J.H. and M.M. contributed nearlyequally to this work.
Terms in blue are defined in the glos-sary, found at the end of
this articleand online at www.jco.org.
Authors disclosures of potentialconflicts of interest are found
in thearticle online at www.jco.org. Authorcontributions are found
at the end ofthis article.
Corresponding author: Junzo Hamanishi,MD, PhD, Department of
Gynecology andObstetrics, Kyoto University GraduateSchool of
Medicine, 54 Kawahara-cho,Shogoin, Sakyo-ku, Kyoto, Kyoto
606-8507,Japan; e-mail: [email protected].
2015 by American Society of ClinicalOncology
0732-183X/15/3399-1/$20.00
DOI: 10.1200/JCO.2015.62.3397
A B S T R A C T
PurposeProgrammed death-1 (PD-1), a coinhibitory immune signal
receptor expressed in T cells, binds toPD-1 ligand and regulates
antitumor immunity. Nivolumab is an antiPD-1 antibody that
blocksPD-1 signaling. We assessed the safety and antitumor activity
of nivolumab in patients withplatinum-resistant ovarian cancer.
Patients and MethodsTwenty patients with platinum-resistant
ovarian cancer were treated with an intravenous infusionof
nivolumab every 2 weeks at a dose of 1 or 3 mg/kg (constituting two
10-patient cohorts) fromOctober 21, 2011. This phase II trial
defined the primary end point as the best overall response.Patients
received up to six cycles (four doses per cycle) of nivolumab
treatment or received dosesuntil disease progression occurred.
Twenty nivolumab-treated patients were evaluated at the endof the
trial on December 7, 2014.
ResultsGrade 3 or 4 treatment-related adverse events occurred in
eight (40%) of 20 patients. Twopatients had severe adverse events.
In the 20 patients in whom responses could beevaluated, the best
overall response was 15%, which included two patients who had a
durablecomplete response (in the 3-mg/kg cohort). The disease
control rate in all 20 patients was45%. The median progression-free
survival time was 3.5 months (95% CI, 1.7 to 3.9 months),and the
median overall survival time was 20.0 months (95% CI, 7.0 months to
not reached) atstudy termination.
ConclusionThis study, to our knowledge, is the first to explore
the effects of nivolumab against ovariancancer. The encouraging
safety and clinical efficacy of nivolumab in patients with
platinum-resistant ovarian cancer indicate the merit of additional
large-scale investigations (UMIN ClinicalTrials Registry
UMIN000005714).
J Clin Oncol 33. 2015 by American Society of Clinical
Oncology
INTRODUCTION
Ovarian cancer is the leading cause of death amongpatients with
gynecologic malignancies. Greaterthan 50% of patients with ovarian
cancer are di-agnosed at an advanced stage.1,2 Despite
cytore-ductive surgery and platinum- and
taxane-basedchemotherapies, greater than 70% of patientswith
advanced ovarian cancer who achieve remis-sion ultimately
experience relapse. Because thereare few effective treatments for
these patients,3 thedevelopment of new treatment strategies is
ur-gently required.3,4
Studies have demonstrated that ovarian can-cers express
cancer-specific antigens and elicitspontaneous antitumor immune
responses fromimmunotherapy.4-7 As we and others have shown,the
number of tumor-infiltrating lymphocytes is asignificant prognostic
factor,5-10 which suggeststhat host immunity plays a pivotal role
in theclinical course of ovarian cancer. However, it hasrecently
been shown that ovarian cancer cells ac-quire the potential to
escape from host immunityin the tumor microenvironment, and new
treat-ment strategies to overcome this phenomenonare
needed.3,11-13
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
2015 by American Society of Clinical Oncology 1
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2015.62.3397The
latest version is at Published Ahead of Print on September 8, 2015
as 10.1200/JCO.2015.62.3397
Copyright 2015 by American Society of Clinical Oncologyfrom
211.144.221.1
Information downloaded from jco.ascopubs.org and provided by at
HOFFMANN-LA ROCHE AG on September 15, 2015Copyright 2015 American
Society of Clinical Oncology. All rights reserved.
-
Programmed cell death-1 (PD-1), an immune checkpoint recep-tor
expressed by T cells, binds to two PD-1 ligands (PD-Ls),
PD-L1(B7-H1) and PD-L2 (B7-DC), and suppresses antigen-specific
cancerimmune reactions.14-16 Many types of human tumors, such as
mela-noma, renal cancer, and ovarian cancer, express PD-L1 and have
theability to escape from the host immune system via PD-1/PD-L1
sig-naling.7, 17-19 We previously reported that PD-L1 expression
was asso-ciated with poor prognosis in ovarian cancer5 and that
PD-L1promoted progression of ovarian cancer by inducing host
immuno-suppression of peripheral cytotoxic CD8T cell lymphocytes.20
Thesefindings suggest that PD-1/PD-L1 signaling might be a new
treatmenttarget for ovarian cancer.
Therefore, we conducted a phase II clinical trial in 20
patientswith platinum-resistant, recurrent, or advanced ovarian
cancer toevaluate the safety and antitumor efficacy of nivolumab, a
fullyhuman immunoglobulin G4 antiPD-1 receptor blocking mono-clonal
antibody.
PATIENTS AND METHODS
Study Design and PatientsThis single-center, open-label, phase
II trial was conducted in two co-
horts of patients with advanced or relapsed, platinum-resistant
ovarian cancer.Eligible patients were characterized by the
following: documented platinum-resistant (defined by a
platinum-free interval of 6 months from the mostrecent
platinum-based treatment regimen), recurrent or advanced
ovariancancer, peritoneal cancer, or tubal cancer; a treatment
history of at leasttwo chemotherapy regimens that included platinum
and taxane agents; agefrom 20 to 79 years; life expectancy of 3
months or greater; an EasternCooperative Oncology Group performance
status of 0 or 1; and lesionsevaluable by RECIST. Patients were
excluded if they had any of the follow-ing: complications of
autoimmune disease; previous systemic corticoste-roid therapy or
immune suppression; or a history of antiPD-1 antibodytherapy. The
study was approved by the institutional review board ofKyoto
University Hospital. Written informed consent for participation
inthe study was obtained from all participants.
ProcedureEligible patients were allocated sequentially to the
low-dose cohort (niv-
olumab 1 mg/kg; n 10) followed by the high-dose cohort
(nivolumab 3mg/kg; n 10) and received nivolumab intravenously every
2 weeks for up to1 year or until progressive disease (PD) or
disease progression occurred. Onecycle comprised four doses
administered 2 weeks apart (over a total of 8weeks). Patients
received a maximum of six cycles (24 doses over 48 weeks).Dose
modification was not permitted. The lesions of all patients were
evalu-ated by computed tomography every 2 months for up to 1 year
or until PD ordisease progression occurred. Response rate (RR) was
assessed by RECISTversion 1.1, and adverse events were evaluated by
the National Cancer InstituteCommon Terminology Criteria for
Adverse Events version 4.0. The trialscheme and flow diagram are
shown in Appendix Figures A1 and A2, respec-tively (online
only).
OutcomesThe primary end point was the best overall response for
each patient as
assessed by RECIST version 1.1. Antitumor response was
independently eval-uated by three central reviewers, including a
radiologist involved in this study.The secondary end points were
the following: drug safety, progression-freesurvival, overall
survival, disease control rate, and adverse events.
Statistical AnalysisThe sample size was based on the precision
of the estimate of the primary
end point (RR), because the main purpose of this trial was to
provide prelim-
inary evidence of drug efficacy before embarking on a larger
trial. For studysample sizes of 20, the corresponding upper limit
of the one-sided 97.5% CI(95% CI) that was calculated on the basis
of the binomial distribution if onepatient had a response of 24.9%
(21.6%). The next phase (a larger-scale,randomized, phase II or III
trial) would be considered worth undertaking ifgreater than one
patient had a response. Because this is the first time niv-olumab
has been studied for ovarian cancer, two dose cohorts were
imple-mented. Dose-specific evaluation and the dose-response
relationship wereonly secondary end points, for which statistical
accuracy has not been assuredin this study. Neither the precisions
of the estimates for each cohort nor acomparison between cohorts
was primarily evaluated in this trial, but theprecision for 10
patients would be considered guaranteed on the basis of theupper
limit values presented in the Appendix (online only). Thus, for
this trialwith two sequential cohorts, 10 patients were included
per cohort, for a totalsample size of 20.
Binary end points were used to estimate the best overall
response, with atwo-sided 95% CI that was based on the exact
binomial distribution. Time-to-event end points were used to
estimate median survival times with the Kaplan-Meier method. The
two-sided 95% CIs were calculated with the Brookmeyerand Crowley
method for the median survival time. These analyses were
imple-mented for the pooled cohort and for each cohort
individually.
Drug and Drug SupplyNivolumab is a fully human immunoglobulin G4
antiPD-1 monoclo-
nal antibody that binds PD-1, inhibits the engagement with PD-Ls
(PD-L1 orPD-L2), and can enhance antitumor activity of T cells.21
Nivolumab wasprovided by Ono Pharmaceutical (Osaka, Japan). All
trial drugs were packagedidentically in this study.
Immunohistochemical Analysis of PD-L1Immunohistochemical
analysis of PD-L1 was performed using
formalin-fixed, paraffin-embedded tumor specimens with murine
antihuman PD-L1 monoclonal antibody (clone 27A2; MBL, Nagoya,
Japan)5 byLSIMedience(Tokyo, Japan).Thestaining
forPD-L1wasevaluatedandscored ina third-party review (LSI Medience)
by two independent pathologists who wereunaware of the outcomes.
The methods are detailed in the Appendix.
RESULTS
Baseline Patient CharacteristicsA total of 20 patients with
advanced or relapsed, platinum-
resistant ovarian cancer were eligible for the protocol and were
treatedwith antiPD-1 antibody (nivolumab) from October 21, 2011,
toDecember 7, 2014 (trial completion date). The median patient age
was60 years (range, 47 to 79 years; standard deviation [SD], 9.0).
Histo-logic tumor subtypes were as follows: serous (n 15; 75%),
endo-metrioid (n 3; 15%), and clear cell (n 2; 10%; Table
1;International Federation of Gynecology and Obstetrics (FIGO)
stag-ing included as well). Eleven (55%) of the 20 patients were
previouslytreated with at least four regimens (Table 1). The median
follow-upperiod and the duration of treatment with nivolumab were
11.0months (range, 3 to 32 months; SD, 8.7) and 3.5 months (range,
1 to12 months; SD, 3.6), respectively (Appendix Table A1, online
only).
SafetyThe most common treatment-related adverse events (ie,
in
four patients [ 20%]) were increased serum AST,
hypothyroidism,lymphocytopenia, decreased serum albumin, fever,
increased serumALT, maculopapular rash, arthralgia, arrhythmia,
fatigue, and anemia(Table 2). Grade 3 or 4 treatment-related
adverse events occurred ineight of 20 patients (40%; 95% CI, 19.9%
to 64.0%; Table 2).
Hamanishi et al
2 2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
Treatment-related adverse events in this study included several
eventsthat were expected, including hypothyroidism and
lymphocytopeniawithout neutropenia. The frequency and severity of
treatment-relatedadverse events were not different between the 1-
and 3-mg/kg cohorts(Table 2). Treatment-related serious adverse
events were observed intwo patients (10%; 95% CI, 1.2% to 31.7%;
Appendix Table A2,online only). One patient in the 1-mg/kg cohort
had two grade 3events, disorientation and gait disorder, after
developing a feverthat lasted longer than 1 month. Another patient
in the 3-mg/kgcohort had grade 3 fever and deep vein thrombosis.
After treatmentfor these conditions, objective antitumor regression
was observed
in this patient. Nivolumab treatment was discontinued in
two(11%) of 18 patients as a result of treatment-related
thyroiditis(Appendix Table A1).
The most frequently observed adverse events were those relatedto
thyroid function: hypothyroidism (n8; Table 2), thyroiditis (n2),
hyperthyroidism (n 1), high thyroid-stimulating hormone (n1), and
low thyroid-stimulating hormone (n 1). Almost all eventswere grade
1 except for one occurrence of grade 2 thyroiditis. Niv-olumab 1
mg/kg treatment for this patient with nivolumab was ceasedafter one
dose in the first course because of thyroiditis-induced feverand
tachycardia, and subsequent tumor progression occurred. The
Table 1. Patient Characteristics
Enrolled Patient Data
No. (%) of Patients
Total (N 20) 1 mg/kg (n 10) 3 mg/kg (n 10)
Median (range) age, years 60.0 (47-79) 62.5 (49-79) 60.0
(47-76)Cancer type
Ovarian cancer 18 (90) 8 (80) 10 (100)Peritoneal cancer 2 (10) 2
(20) 0 (00)Tubal cancer 0 (0) 0 (0) 0 (0)
FIGO stage [subtype, No. of patients]I 2 (10) [Ic, 2] 0 (0) 2
(20) [Ic, 2]II 0 (0) 0 (0) 0 (0)III 14 (70) [IIIb, 1; IIIc, 13] 9
(90) [IIIb, 1; IIIc, 8] 5 (50) [IIIc, 5]IV 4 (20) 1 (10) 3 (30)
HistologySerous 15 (75) 8 (80) 7 (70)Endometrioid 3 (15) 2 (20)
1 (10)Clear cell 2 (10) 0 (0) 2 (20)
Prior chemotherapy regimens4 11 (55) 5 (50) 6 (60)4 9 (45) 5
(50) 4 (40)
ECOG performance status0 18 (90) 10 (100) 8 (80)1 2 (10) 0 (0) 2
(20)
NOTE. Summary of exposure to nivolumab, all treated patients: A
total of 20 patients with advanced or relapsed, platinum-resistant
ovarian cancer were treatedwith antiprogrammed death-1 (nivolumab).
International Federation of Gynecology and Obstetrics (FIGO)
staging of disease in all patients was performed at
initialdiagnosis postoperatively.Abbreviation: ECOG, Eastern
Cooperative Oncology Group.
Table 2. Treatment-Related Adverse Events of Special Interest
That Occurred in at Least 20% of All Treated Patients
Event
No. (%) of Patients With Adverse Event by Treatment Cohort and
Grade
Total (N 20) 1 mg/kg (n 10) 3 mg/kg (n 10)
All Grades Grade 3 or 4 All Grades Grade 3 or 4 All Grades Grade
3 or 4
Any adverse event 19 (95) 8 (40) 9 (90) 4 (40) 10 (100) 4
(40)AST increased 8 (40) 0 (0) 6 (60) 0 (0) 2 (20) 0
(0)Hypothyroidism 8 (40) 0 (0) 4 (40) 0 (0) 4 (40) 0
(0)Lymphocytopenia 7 (35) 3 (15) 4 (40) 3 (30) 3 (30) 0 (0)Albumin
decreased 6 (30) 2 (10) 2 (20) 1 (10) 4 (40) 1 (10)Fever 6 (30) 1
(5) 2 (20) 1 (10) 4 (40) 0 (0)ALT increased 5 (25) 1 (5) 4 (40) 1
(10) 1 (10) 0 (0)Maculopapular rash 5 (25) 1 (5) 3 (30) 0 (0) 2
(20) 1 (10)Arthralgia 5 (25) 0 (0) 5 (50) 0 (0) 0 (0) 0
(0)Arrhythmia 6 (30) 0 (0) 4 (40) 0 (0) 2 (20) 0 (0)Fatigue 4 (20)
0 (0) 2 (20) 0 (0) 2 (20) 0 (0)Anemia 4 (20) 3 (15) 3 (30) 2 (20) 1
(10) 1 (10)
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology 3
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
patient data, therefore, were classified as not evaluated. In
anotherpatient with thyroiditis, treatment with nivolumab 1 mg/kg
also endedduring the third course, although the patient experienced
a partialresponse (PR) for 5 months. The most common adverse events
aredescribed in Appendix Table A3 (online only).
Clinical ActivityThe best overall RR across the two cohorts,
confirmed by inde-
pendent central review, was 15% (three of 20 patients; 95% CI,
3.2% to
37.9%), and the disease control rate was 45% (nine of 20
patients; 95%CI, 23.1% to 68.5%; Table 3).
In the 1-mg/kg cohort, one patient experienced a PR and fourhad
stable disease. The objective RR was 10% (95% CI, 0.3% to44.5%),
and the disease control rate was 50% (95% CI, 18.7% to81.3%). The
partial responder experienced an antitumor response upto 5 months;
however, nivolumab treatment was stopped after threecourses because
of adverse events, and disease recurred 3 months afterwithdrawal
from the trial.
A
B
0shtnoM 4enilesaB
shtnoM 4enilesaB
CA-1
25 (U
/mL)
Time (days)
150
100
50
250
111
316
16 10 10 8 8 8
289 7 8 7 6 7
500
200 400
CA-1
25 (U
/mL)
Time (days)
300
200
100
0
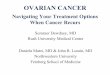
Fig 1. Activity of antiprogrammed death 1 (PD-1) antibody in two
patients with a complete response to recurrent ovarian cancer. (A)
Complete response ofplatinum-resistant and recurrent serous ovarian
cancer in a 59-year-old patient who received antiPD-1 antibody
(nivolumab) at a dose of 3.0 mg/kg. This patient hadpreviously
undergone primary surgery, and progressive disease had developed
after treatment with systemic chemotherapies (ie, cyclophosphamide,
adriamycin, andcisplatin; or docetaxel and carboplatin). Although
multiple pelvic lymph node metastases were observed on a baseline
computed tomographic image (left), these lesionswere no longer
apparent at 4 months after the start of nivolumab treatment
(middle). The white circles show regression of recurrent lymph node
metastases. Tumormarker cancer antigen 125 (CA-125) decreased to
normal range after one course of nivolumab (right). (B) Complete
response of platinum-resistant and recurrent ovarianclear cell
carcinoma in a 60-year-old patient who received nivolumab at a dose
of 3.0 mg/kg. This patient had previously undergone right
salpingo-oophorectomy, andprogressive disease had developed after
treatment with systemic chemotherapies (ie, mitomycin and
irinotecan; irinotecan and cisplatin; or paclitaxel and
carboplatin)and supracervical hysterectomy plus left
salpingo-oophorectomy. The circles show complete regression of
recurrent peritoneal dissemination (left, baseline; middle,4 months
after the start of nivolumab treatment). Tumor marker CA-125
decreased to normal range after one course of nivolumab (right).
The horizontal dashed linerepresents the cutoff level for CA-125
(35 U/mL).
Table 3. Clinical Effect of AntiPD-1 Antibody Treatment
Dose ofNivolumab
No. ofPatients
Response No. (%) of Patients [95% CI] Survival, Months (95%
CI)
CR PR SD PD NE RR DCR PFS OS
1 mg/kg 10 0 1 4 4 1 1 (10) [0.3 to 44.5] 5 (50) [18.7 to 81.3]
3.5 (0.7 to 3.9) 16.1 (2.6 to NR)3 mg/kg 10 2 0 2 6 0 2 (20) [2.5
to 55.6] 4 (40) [12.2 to 73.8] 3.0 (1.5 to 3.9) NR (2.9 to NR)Total
20 2 1 6 10 1 3/20 (15%) [3.2 to 37.9] 9/20 (45%) [23.1 to 68.5]
3.5 (1.7 to 3.9) 20.0 (7.0 to NR)
Abbreviations: CR, complete response; DCR, disease control rate
(ie, CR, PR, and SD); NE, not evaluated; NR, not reached; OS, point
estimate of overall survival;PD-1, programmed death-1; PFS, point
estimation of progression-free survival; PR, partial response; RR,
response rate (ie, CR and PR); SD, stable disease.No. of patients
of the total listed in the same row.
Hamanishi et al
4 2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
In the 3-mg/kg cohort, two patients had a complete response(CR),
and two had stable disease. The objective RR was 20% (95% CI,2.5%
to 55.6%), and the disease control rate was 40% (95% CI, 12.2%to
73.8%). One of the two patients who experienced a CR was
a59-year-old person with ovarian serous adenocarcinoma (Fig
1A).After two courses of nivolumab treatment, multiple pelvic
lymphnode metastatic lesions completely disappeared, and levels of
tumormarker cancer antigen 125 (CA-125) decreased to the normal
range.This patient survived without experiencing tumor relapse for
2months after completion of the 1-year trial of nivolumab. The
othercomplete responder was a 60-year-old patient who had clear
cellcarcinoma with recurrent disease and peritoneal dissemination
(Fig1B). After two courses of nivolumab treatment, these peritoneal
le-sions disappeared, and CA-125 decreased to the normal range.
Thispatient recently completed a 1-year trial of nivolumab and
continuesto experience a CR.
As shown in Figure 2A, in the four patients who had
antitumorresponses, the responses were durable and evident. Three
of fourpatients had an objective response according to RECIST
version 1.1(CR, n 2; PR, n 1), whereas one patient experienced
progressivedisease with a new recurrent lesion even though the
target lesion hadcompletely regressed (Figs 2A and 2B).
The median progression-free survival times were 3.5 months(95%
CI, 1.7 to 3.9 months) for the pooled cohort, 3.5 months (95%CI,
0.7 to 3.9 months) for the 1-mg/kg cohort, and 3.0 months (95%CI,
1.5 to 3.9 months) for the 3-mg/kg cohort (Table 3; Fig 3A).
Themedian overall survival times were 20.0 months (95% CI, 7.0
tomonths) for the pooled cohort and 16.1 months (95% CI, 2.6
tomonths) for the 1-mg/kg cohort; overall survival was not
evaluated forthe 3-mg/kg cohort, because data for greater than one
half of thepatients were censored (Table 3; Fig 3B). The upper
limits could not beevaluated for all 20 patients, because too few
events occurred after themedian overall survival times (Table 3;
Fig 3).
PD-L1 Expression on Tumor CellsOvarian cancer specimens from all
20 patients were analyzed for
PD-L1 expression in tumor cells by immunohistochemistry (Figs
4Ato 4D). Tumor specimens from 16 (80%) of 20 patients showed
highexpression of PD-L1 (n 15 patients with scores of2; n 1
patientwith a score of 3), whereas four (20%) of 20 patients showed
lowexpression of PD-L1 (n 4 patients with scores of1). An
objectiveresponse (ie, CR and PR) occurred in two of the 16
patients withtumors that showed high expression of PD-L1, whereas
nonresponseoccurred in two of the four patients with tumors that
expressed lowlevels of PD-L1. However, the expression of PD-L1 was
not signifi-cantly correlated with objective response (P .509; Fig
4E).
DISCUSSION
This study, to our knowledge, is the first
investigator-initiated, phase IIclinical trial to test the safety
and efficacy of nivolumab againstplatinum-resistant ovarian cancer.
The 3-mg/kg dose of nivolumabmay be more favorable than the 1-mg/kg
dose for ovarian cancer,because this dose showed better efficacy
without a significant increasein toxicity. A previous clinical
trial of nivolumab in other solid tumorsshowed the same finding.21
According to the National Comprehen-sive Cancer Network guidelines,
the current standard treatment forplatinum- and taxane-resistant
ovarian cancer is single-agent chemo-therapy with pegylated
liposomal doxorubicin, topotecan, or gemcit-abine; however, these
agents did not demonstrate a satisfactory clinicalantitumor
effect.22-24 In an early phase II trial in 44 patients
withplatinum-resistant ovarian cancer, monotherapy with
bevacizumab, avascular endothelial growth factor inhibitor, no
patients experienced aCR, and the RR was 15.9%. In this trial, the
median progression-freesurvival time was 4.4 months, and the median
overall survival timewas 10.7 months at study termination.25
In the context of these previous findings, the durable
antitumorresponse of the 3-mg/kg dose of nivolumab in our
exploratory studywas clinically significant enough to warrant
large-scale studies of niv-olumab in patients with
platinum-resistant ovarian cancer. Notably,in one of the two
patients who experienced a CR, the tumor washistologically
identified as clear cell carcinoma. Ovarian clear cellcarcinoma has
a worse prognosis than the more common serousadenocarcinoma.26
There are few effective chemotherapies for recur-rent clear cell
carcinoma; the overall RR for this malignancy wasreported to be
approximately 2% (ie, one of 51 patients).26 The geneexpression
profiles are similar between renal and ovarian clear
cellcarcinomas,27 so nivolumab may show potential benefit in
treatingclear cell carcinoma of the ovary.
SD SD SD SD NEPD* PD*
PRSD* CR*
CR
PD*
PD
PD PD PD PDSDPDPD
Chan
ge in
Tar
get L
esio
nsFr
om B
asel
ine
(%)
200
150
100
50
0
-50
-100
50 100 150 200 250 300 350 400
1 mg/kg (n = 10)3 mg/kg (n = 10)
1 mg/kg (n = 10)3 mg/kg (n = 10)
CR*
PR SD*
CRTime (days)
A
Chan
ge in
Tar
get L
esio
nsFr
om B
asel
ine
(%)
150
100
50
0
-50
-100
B
Fig 2. Best overall responses in all patients in two cohorts
with antiprogrammed death 1 (PD-1) antibody. The blue lines
represent the 1-mg/kgcohort, and the gold lines represent the
3-mg/kg cohort. (A) Duration of bestoverall responses and changes
in target lesions from baseline in 20 patients whoreceived antiPD-1
antibody at a dose of 1.0 or 3.0 mg/kg every 2 weeks. Twopatients
with a complete response (CR; [*] one patient with lymph
nodemetastasis evaluated as CR after antiPD-1 antibody treatment
[Fig 1A]; []another patient with peritoneal dissemination evaluated
[Fig 1B]) were stillreceiving treatment with antiPD-1 antibody. (B)
Changes in target lesions frombaseline in 20 patients. Although
four of 20 patients had data below the horizontaldashed lines,
three of these four patients were considered to have an
objectiveresponse (ie, two CRs and oen partial response [PR]). In
one patient withprogressive disease (PD) who had a new recurrent
lesion, best overall responsewas measured as stable disease (SD),
although the target lesion had completelyregressed after SD. In
three patients who had new recurrent lesions (indicated byPD*), PD
was determined, although the target lesions were measured as SD.The
two horizontal dashed lines mark the thresholds for objective
response(lower line, 30%) and PD (higher line, 20%), according to
RECIST (version 1.1).NE, not evaluable.
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology 5
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
In a previous phase I clinical trial of an antiPD-L1
antibody(BMS-936559) in 17 patients with ovarian cancers,28 one
patient ex-perienced a PR (RR, 5.9%), and three had stable disease,
which yieldeda disease control rate of 23.5%. These findings, as
well as those of thisstudy, indicate that a certain patient
population may demonstrate anantitumor effect in response to PD-1
signal blocking. Thus, targetingPD-1 signaling with antiPD-L1 or
antiPD-1 treatment is a potentialtreatment strategy in patients
with platinum-resistant ovarian cancer.
In this study, treatment-related adverse events of grade 3 or
4occurred in eight (40%) of 20 patients, although treatment could
becompleted in most (19 [95%] of 20) patients. The frequencies
ofarrhythmias and elevated AST were relatively higher in this study
thanin larger previous studies of nivolumab for other solid
tumors,21 butall of these events were grade 1 or 2 and were
controllable. Greater thanone half of the treatment-related adverse
events in this study, such asfever, maculopapular rash,
hypothyroidism, and lymphocytopenia
1 mg/kg
Prog
ress
ion-
Free
Surv
ival (
%)
Time (months)
No. at risk 10 9 2 2 2 2 0 0 0 0 0 0 0 0 0 0 0
100
50
A
0 10 20 30
Total
Prog
ress
ion-
Free
Surv
ival (
%)
Time (months)
No. at risk 20 15 5 5 5 5 2 1 0 0 0 0 0 0 0 0 0
100
50
C
0 10 20 30
3 mg/kg
1 mg/kg Total3 mg/kg
Prog
ress
ion-
Free
Surv
ival (
%)
Over
all S
urviv
al (%
)
Over
all S
urviv
al (%
)
Over
all S
urviv
al (%
)
Time (months)
No. at risk 10 6 3 3 3 3 3 1 0 0 0 0 0 0 0 0 0
100
50
B
0 10 20 30
Time (months)
No. at risk 10 10 9 8 7 6 6 5 5 5 5 2 1 1 1 1 0
100
50
D
0 10 20 30
Time (months)
No. at risk 20 19 17 15 12 11 8 6 5 5 5 2 1 1 1 1 0
100
50
F
0 10 20 30
Time (months)
No. at risk 10 9 8 7 5 5 2 1 0 0 0 0 0 0 0 0 0
100
50
E
0 10 20 30
Fig 3. Progression-free survival and overall survival.
Progression-free survival in the (A) 1-mg/kg cohort and (B) 3-mg/kg
cohort and (C) in all patients; bars indicatecensoring events.
Overall survival in the (D) 1-mg/kg cohort and (E) 3-mg/kg cohort
and (F) in all patients; bars indicate censoring events.
E
A B C D
P = .509
No.
of P
atie
nts
15
10
5
0PD-L1 high
(n = 16)
2 of 16
14 of 16
1 of 4
3 of 4
PD-L1 low(n = 4)
ResponderNonresponder
Fig 4. The relationship between pro-grammed death-1 ligand 1
(PD-L1) expressionon tumor cells and objective response to
antiprogrammed death-1 (PD-1) antibody treat-ment.
Immunohistochemical analysis offormalin-fixed paraffin-embedded
ovarian can-cer specimens before patients underwentantiPD-1
antibody treatment with antiPD-1monoclonal antibody. Representative
(A) high(3) and (B) low (1) staining patterns ofPD-L1 on ovarian
cancers are shown. (C)Positive-control staining of PD-L1 on
placenta(2) disappeared with the (D) absorption test.Scale bars,
100 m. (E) The correlation be-tween the expression of PD-L1 on
tumor cellsand the objective response to antiPD-1 anti-body in 20
patients with platinum-resistantovarian cancers. Expression of
PD-L1was notsignificantly correlated with objective re-sponse (P
.509).
Hamanishi et al
6 2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
without neutropenia, were reported in a previous clinical trial
ofnivolumab for other solid tumors.21 Neither pneumonitis nor
colitis,previously reported as severe immune-related adverse
events,21 wasobserved in this study.
Thyroiditis was observed in two patients in the 1-mg/kg
cohort.We revised the protocol to allow corticosteroid treatment
forimmune-related adverse events by referring to a previous phase
Itrial.21 After this protocol revision, one patient experienced
immune-related adverse events of eosinophilia and rash during the
third courseof treatment; after corticosteroid administration, the
patient was ableto tolerate the subsequent four courses of
nivolumab.
Compared with a previous report about nivolumab,21 a late
an-titumor response pattern was not found in our series; rather, a
quickantitumor response was demonstrated (Figs 1 and 2).
Interestingly,few patients had stable disease or experienced a PR
in this study,whereas two patients experienced a CR. This discrete
difference in theeffectiveness of nivolumab was not observed in
other solid tumors21
and may be specific to patients with ovarian cancer. Thus, the
estab-lishment of a biomarker to predict the antitumor response of
niv-olumab in ovarian cancer is promising.
To identify predictive biomarkers for the antitumor effect
ofnivolumab, as done in previous reports,21,29 we evaluated the
expres-sion of PD-L1 in ovarian cancer tissues but did not find any
significantcorrelation between clinical response and PD-L1
expression (Fig 4).The discrepancy between this study and previous
reports might be aresult of the following two points: First,
ovarian cancers are classifiedinto several clusters on the basis of
the gene expression profile data,including data from the Cancer
Genome Atlas.30,31 One of these clus-ters, the immunoreactive
phenotype, contains several immune-related genes, but this
phenotype composes only approximately 20%of ovarian cancers.
Therefore, this classification might have contrib-uted to the low
RR in our study, even in the presence of high expres-sion of PD-L1
on tumor cells.
Second, our study may have had several problems related
tomaterials or methods, including the timing of tumor sampling.
Weacquired most tumor samples during primary operations of
patients,whereas most samples in previous reports were obtained via
biopsybefore nivolumab treatment for solid tumors.21,29 The
expressionof PD-L1 might be altered by the therapeutic process or
by inflam-
matory alterations at the tumor site.32 A recent trial of
combinationtherapy with antiPD-1 antibody and anti-CTLA4 (cytotoxic
T-lymphocyteassociated protein 4) antibody for advanced mela-noma
showed no significant correlation between objectiveresponse and
PD-L1 expression in tumor tissues.29 A methodo-logic problem may
have been the use of different antibody clonesor unstable staining
of formalin-fixed, paraffin-embeddedsamples.21,29,32 Therefore,
this study could not determine whetherthe expression of PD-L1 is a
true biomarker for the antitumoreffect against ovarian cancer, and
additional investigation will beneeded to resolve this issue.
In conclusion, nivolumab demonstrated encouraging clinical
ef-ficacy and tolerability in patients with platinum-resistant
ovarian can-cer. Therefore, this study indicates the merit of a
large-scaleinvestigation to evaluate the priority of nivolumab for
platinum-resistant ovarian cancer, and we plan to perform such a
trial with apharmaceutical company.
AUTHORS DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Disclosures provided by the authors are available with this
article atwww.jco.org.
AUTHOR CONTRIBUTIONS
Conception and design: Junzo Hamanishi, Masaki Mandai,
TakafumiIkeda, Manabu Minami, Toshinori Murayama, Satoshi Morita,
AkiraShimizuAdministrative support: Junzo Hamanishi, Takafumi
IkedaCollection and assembly of data: Junzo Hamanishi, Manabu
Minami,Toshinori Murayama, Masashi Kanai, Yukiko Mori,
ShigemiMatsumoto, Shunsuke Chikuma, Noriomi Matsumura, Kaoru
Abiko,Tsukasa Baba, Ken Yamaguchi, Akihiko Ueda, Yuko Hosoe,
MasayukiYokode, Tasuku Honjo, Ikuo KonishiData analysis and
interpretation: Junzo Hamanishi, Atsushi Kawaguchi,Satoshi Morita,
Akira ShimizuManuscript writing: All authorsFinal approval of
manuscript: All authors
REFERENCES
1. Hoskins P, Vergote I, Cervantes A, et al:Advanced ovarian
cancer: Phase III randomizedstudy of sequential cisplatin-topotecan
andcarboplatin-paclitaxel versus carboplatin-paclitaxel. JNatl
Cancer Inst 102:1547-1556, 2010
2. Jemal A, Siegel R, Ward E, et al: Cancerstatistics, 2009. CA
Cancer J Clin 59:225-249, 2009
3. Naumann RW, Coleman RL: Managementstrategies for recurrent
platinum-resistant ovariancancer. Drugs 71:1397-1412, 2011
4. Kandalaft LE, Powell DJ Jr, Singh N, CoukosG: Immunotherapy
for ovarian cancer: Whats next?J Clin Oncol 29:925-933, 2011
5. Zhang L, Conejo-Garcia JR, Katsaros D, et al:Intratumoral T
cells, recurrence, and survival in epi-thelial ovarian cancer. N
Engl J Med 348:203-213,2003
6. Ioannides CG, Freedman RS, Platsoucas CD,et al: Cytotoxic T
cell clones isolated from ovarian
tumor-infiltrating lymphocytes recognize multipleantigenic
epitopes on autologous tumor cells. JImmunol 146:1700-1707,
1991
7. Kooi S, Zhang HZ, Patenia R, et al: HLAclass I expression on
human ovarian carcinomacells correlates with T-cell infiltration in
vivo andT-cell expansion in vitro in low concentrations
ofrecombinant interleukin-2. Cell Immunol 174:116-128, 1996
8. Hamanishi J, Mandai M, Iwasaki M, et al:Programmed cell death
1 ligand 1 and tumor-infiltrating CD8 T lymphocytes are prognostic
fac-tors of human ovarian cancer. Proc Natl Acad SciUSA
104:3360-3365, 2007
9. Hamanishi J, Mandai M, Abiko K, et al: Thecomprehensive
assessment of local immune statusof ovarian cancer by the
clustering of multiple im-mune factors. Clin Immunol 141:338-347,
2011
10. Hwang WT, Adams SF, Tahirovic E, et al:Prognostic
significance of tumor-infiltrating T cells inovarian cancer: A
meta-analysis. Gynecol Oncol 124:192-198, 2012
11. Dunn GP, Bruce AT, Ikeda H, et al: Cancerimmunoediting: From
immunosurveillance to tumorescape. Nat Immunol 3:991-998, 2002
12. Schreiber RD, Old LJ, Smyth MJ: Cancerimmunoediting:
Integrating immunitys roles in can-cer suppression and promotion.
Science 331:1565-1570, 2011
13. Mellman I, Coukos G, Dranoff G: Cancer im-munotherapy comes
of age. Nature 480:480-489,2011
14. Keir ME, Butte MJ, Freeman GJ, et al: PD-1and its ligands in
tolerance and immunity. Annu RevImmunol 26:677-704, 2008
15. Iwai Y, Ishida M, Tanaka Y, et al: Involvementof PD-L1 on
tumor cells in the escape from hostimmune system and tumor
immunotherapy byPD-L1 blockade. Proc Natl Acad Sci USA
99:12293-12297, 2002
16. Zou W, Chen L: Inhibitory B7-family mole-cules in the tumor
microenvironment. Nat Rev Im-munol 8:467-477, 2008
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology 7
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
17. Okazaki T, Chikuma S, Iwai Y, et al: A rheostatfor immune
responses: The unique properties ofPD-1 and their advantages for
clinical application.Nat Immunol 14:1212-1218, 2013
18. Thompson RH, Gillett MD, Cheville JC, et al:Costimulatory
B7H1 in renal cell carcinomapatients: Indicator of tumor
aggressiveness andpotential therapeutic target. Proc Natl Acad Sci
USA101:17174-17179, 2004
19. Hino R, Kabashima K, Kato Y, et al: Tumor cellexpression of
programmed cell death-1 ligand 1 is aprognostic factor for
malignant melanoma. Cancer116:1757-1766, 2010
20. Abiko K, Mandai M, Hamanishi J, et al: PD-L1on tumor cells
is induced in ascites and promotesperitoneal dissemination of
ovarian cancer throughCTL dysfunction. Clin Cancer Res
19:1363-1374,2013
21. Topalian SL, Hodi FS, Brahmer JR, et al:Safety, activity,
and immune correlates of anti-PD-1antibody in cancer. N Engl J Med
366:2443-2454,2012
22. Morgan RJ Jr, Alvarez RD, Armstrong DK, etal: National
comprehensive cancer networks: Ovar-ian cancer, version 2.2013. J
Natl Compr Canc Netw11:1199-1209, 2013
23. Mutch DG, Orlando M, Goss T, et al: Random-ized phase III
trial of gemcitabine compared withpegylated liposomal doxorubicin
in patients withplatinum-resistant ovarian cancer. J Clin Oncol
25:2811-2818, 2007
24. Gordon AN, Fleagle JT, Guthrie D, et al:Recurrent epithelial
ovarian carcinoma: A random-ized phase III study of pegylated
liposomal doxoru-bicin versus topotecan. J Clin Oncol
19:3312-3322,2001
25. Cannistra SA, Matulonis UA, Penson RT, et al:Phase II study
of bevacizumab in patients withplatinum-resistant ovarian cancer or
peritoneal se-rous cancer. J Clin Oncol 25:5180-5186, 2007
26. Crotzer DR, Sun CC, Coleman RL, et al: Lackof effective
systemic therapy for recurrent clear cellcarcinoma of the ovary.
Gynecol Oncol 105:404-408,2007
27. Zorn KK, Bonome T, Gangi L, et al: Geneexpression profiles
of serous, endometrioid, andclear cell subtypes of ovarian and
endometrial can-cer. Clin Cancer Res 11:6422-6430, 2005
28. Brahmer JR, Tykodi SS, Chow LQ, et al:Safety and activity of
antiPD-L1 antibody in patientswith advanced cancer. N Engl J Med
366:2455-2465, 2012
29. Wolchok JD, Kluger H, Callahan MK, et al:Nivolumab plus
ipilimumab in advanced melanoma.N Engl J Med 369:122-133, 2013
30. Tothill RW, Tinker AV, George J, et al: Novelmolecular
subtypes of serous and endometrioidovarian cancer linked to
clinical outcome. Clin Can-cer Res 14:5198-5208, 2008
31. Cancer Genome Atlas Research Network: In-tegrated genomic
analyses of ovarian carcinoma.Nature 474:609-615, 2011
32. Taube JM, Klein A, Brahmer JR, et al: Asso-ciation of PD-1,
PD-1 ligands, and other features ofthe tumor immune
microenvironment with re-sponse to anti-PD-1 therapy. Clin Cancer
Res 20:5064-5074, 2014
GLOSSARY TERMS
CA-125 (cancer antigen 125): a protein produced by thefallopian
tubes, the endometrium, and the lining of the abdomi-nal cavity
(peritoneum). CA-125 is a tumor marker present inhigher than normal
amounts in the blood and urine of patientswith certain cancers.
Typically, women with ovarian cancer havehigh levels of CA-125.
Other conditions associated with elevatedlevels of CA-125 include
endometriosis, pancreatitis, pregnancy,normal menstruation, and
pelvic inflammatory disease. CA-125levels may be used to help
diagnose ovarian cancer and to deter-mine whether these tumors are
responding to therapy. The nor-mal range for CA-125 is less than 35
U/mL and less than 20U/mL for women who have been treated for
ovarian cancer.Women with ovarian cancer may show values higher
than 65U/mL.
CD8 T cell: cytotoxic T cell that is the primary effector
cellsof the immune system. They are characterized by the presence
ofthe CD8 cell-surface marker.
Computed tomography (CT) scan: a series of picturescreated by a
computer linked to an x-ray machine taken of theinside of the body
from different angles.
FIGO staging: a tumor staging system established and revisedby
the International Federation of Gynecology and Obstetrics(FIGO)
that takes into account the postoperative histopathologicevaluation
of the specimen. The FIGO stage classification hasprognostic
value.
Immune checkpoint: immune inhibitory pathway that neg-atively
modulates the duration and amplitude of immune re-sponses. Examples
include the CTLA-4:B7.1/B7.2 pathway andthe PD-1:PD-L1/PD-L2
pathway.
Immunohistochemistry: the application of
antigen-antibodyinteractions to histochemical techniques.
Typically, a tissue section ismounted on a slide and incubated with
antibodies (polyclonal or mono-clonal) specific to the antigen
(primary reaction). The antigen-antibodysignal is then amplified
using a second antibody conjugated to a com-plex of
peroxidase-antiperoxidase, avidin-biotin-peroxidase, or
avidin-biotin alkaline phosphatase. In the presence of substrate
andchromogen, the enzyme forms a colored deposit at the sites of
antibody-antigen binding. Immunofluorescence is an alternate
approach to visu-alize antigens. In this technique, the primary
antigen-antibody signal isamplified using a second antibody
conjugated to a fluorochrome. Onultraviolet light absorption, the
fluorochrome emits its own light at alonger wavelength
(fluorescence), thus allowing localization ofantibody-antigen
complexes.
Immunotherapy: a therapeutic approach that uses cellular
and/orhumoral elements of the immune system to fight a disease.
PD-1: programmed cell death protein 1 (CD279), a receptor
expressedon the surface of activated T, B, and NK cells that
negatively regulatesimmune responses, including autoimmune and
antitumor responses.
PD-L1: programmed cell death 1 ligand 1 (CD274; also known as
B7-H1),the major binding partner (ligand) for the PD-1 inhibitory
immune receptor.PD-L1 is expressed on the surface of activated
antigen presenting cells, such asdendritic cells, and by many types
of cancer cells. Its expression is induced by theinflammatory
cytokine interferon-alfa
RECIST (Response Evaluation Criteria in Solid Tu-mors): a model
proposed by the Response Evaluation Criteria Groupby which a
combined assessment of all existing lesions, characterized bytarget
lesions (to be measured) and nontarget lesions, is used to
extrapo-late an overall response to treatment.
Hamanishi et al
8 2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
AUTHORS DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Safety and Antitumor Activity of AntiPD-1 Antibody, Nivolumab,
in PatientsWith Platinum-Resistant Ovarian Cancer
The following represents disclosure information provided by
authors of this manuscript. All relationships are considered
compensated. Relationships areself-held unless noted. I Immediate
Family Member, InstMy Institution. Relationships may not relate to
the subject matter of this manuscript. For moreinformation about
ASCOs conflict of interest policy, please refer to www.asco.org/rwc
or jco.ascopubs.org/site/ifc.
Junzo HamanishiNo relationship to disclose
Masaki MandaiNo relationship to disclose
Takafumi IkedaNo relationship to disclose
ManabuMinamiNo relationship to disclose
Atsushi KawaguchiNo relationship to disclose
Toshinori MurayamaHonoraria: Kowa Pharmaceuticals America
Masashi KanaiNo relationship to disclose
YukikoMoriSpeakers Bureau: BayerResearch Funding: Taiho
Pharmaceutical (Inst), Yakult Honsha (Inst)
ShigemiMatsumotoNo relationship to disclose
Shunsuke ChikumaNo relationship to disclose
NoriomiMatsumuraResearch Funding: Daiichi Sankyo (Inst)
Kaoru AbikoNo relationship to disclose
Tsukasa BabaNo relationship to disclose
Ken YamaguchiNo relationship to disclose
Akihiko UedaNo relationship to disclose
Yuko HosoeNo relationship to disclose
Satoshi MoritaHonoraria: Ono Pharmaceutical, Bristol-Myers
Squibb
Masayuki YokodeNo relationship to disclose
Akira ShimizuNo relationship to disclose
Tasuku HonjoResearch Funding: Ono Pharmaceutical
Ikuo KonishiNo relationship to disclose
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
AcknowledgmentWe thank Hiroyuki Yoshikawa, MD, Hiroshi Date, MD,
and Kaichiro Yamamoto, MD, for support on the Data and Safety
MonitoringBoard; Kazuhiko Ino, MD, Kimihiko Ito, MD, and Shigeaki
Umeoka, MD, for support as central reviewers; and Shingo Fujii, MD,
for
supervision.
Appendix
Appendix Materials and MethodsSample Size Estimation Details.
The sample size was based on the precision of the estimate of the
primary end point (the response
rate), because the main purpose of this trial was to provide
preliminary evidence of drug efficacy before embarking on a larger
trial. Forstudy sample sizes of 3, 6, 10, 15, and 20, the
corresponding upper limits of the one-sided 97.5% (95%) CI
calculated on the basis of thebinomial distribution if no patient
had a response were 70.7% (63.2%), 45.9% (39.3%), 30.9% (25.9%),
21.8% (18.1%), and 16.8%(13.9%), respectively; if one patient had a
response, the respective values were 90.6% (86.5%), 64.1% (58.2%),
44.5% (39.4%), 32.0%(27.9%), and 24.9% (21.6%). The next phase
would be considered worth undertaking if more than one patient had
a response.Conversely, if none of the sample of 20 patients was to
demonstrate a response, the response rate would have an upper
one-sided 97.5%confidence limit of 16.8%; 16.8% or lower would be
unacceptable, and the treatment would not be promising in the
target population.Neither the precisions of the estimates for each
cohort nor a comparison between cohorts was evaluated in this
trial, but the precision for10 patients would be considered
guaranteed on the basis of the upper-limit values presented above.
Thus, for this trial with two cohorts,10 patients were included per
cohort, for a total sample size of 20.
Definition of Disease Control Rate, Progression-Free Survival,
and Overall SurvivalThe disease control rate was the proportion of
patients whose best overall response was either complete response
or partial response.
Progression-free survival (PFS) was defined as the period from
the day of registration to recurrence, progression, or death as a
result of anycause, whichever came first. For patients who did not
experience recurrence or progression, PFS was censored on the last
known date freeof recurrence or progression on the basis of
radiologic criteria. For reference and exploratory comparisons, PFS
was censored on the lastknown date free of recurrence or
progression on the basis of clinical evaluation (radiologic
confirmation not necessary). PFS was notcensored at the start of
follow-up therapy. The occurrence of heterochronous multiple
cancers was not regarded as a PFS event. Therefore,PFS was not
censored at the discovery of heterochronous multiple cancers. The
study site (not the central evaluation committee) evaluatedclinical
progression. Overall survival (OS) was defined as the period from
the date of registration to the date of death as a result of any
cause.For patients who remained alive, OS was censored at the time
the patient was last known to be alive. For patients whose data
were lost tofollow-up, OS was censored on the date that the
patients were last known to be alive before they became
unreachable.
Efficacy End PointsTumor response was the primary end point of
this study. By using the exact binomial test, we estimated the
tumor response rate and
its two-sided 95% CI (equivalent to the one-sided 97.5% CI) for
the full analysis set (FAS; ie, the two dose cohorts combined). In
addition,we repeated the procedure separately for each cohort.
The disease control rate was a secondary end point of this
study. By using the exact binomial test, we estimated the disease
control rateand its two-sided 95% CI for the FAS. In addition, we
repeated the procedure separately for each cohort. PFS was an
additional secondaryend point of this study. We used the
Kaplan-Meier method to estimate the median PFS and the N-year PFS
rates (N1, 2, etc) for the FAS.We used the Brookmeyer and Crowley
method to estimate the two-sided 95% CI for the median PFS, and we
employed Greenwoodsformula to determine the two-sided 95% CI for
the N-year PFS rates. In addition, we repeated the procedure
separately for each cohort.OS was the final secondary end point of
this study. We used the Kaplan-Meier method to estimate the median
OS and the N-year OS rates(N 1, 2, etc) for the FAS. We used the
Brookmeyer and Crowley method to estimate the two-sided 95% CI for
median OS, and weemployed Greenwoods formula to determine the
two-sided 95% CI for the N-year OS rates. In addition, we repeated
the procedureseparately for each cohort.
Immunohistochemical Analysis of Programmed Death-1 Ligand
1Immunohistochemical analysis of programmed death-1 ligand 1
(PD-L1) was performed with formalin-fixed, paraffin-embedded
tumor specimens and with murine antihuman PD-L1 monoclonal
antibody by LSI Medience (Tokyo, Japan). Briefly, LSI
Medienceconducted immunohistochemistry of PD-L1 as follows:
Heat the sections for 1 hour at 60C. Deparaffinize the sections
with xylene three times for 5 minutes each. Wash the slides with
ethanol for 5 minutes. Wash the slides with 90% ethanol and 80%
ethanol for 30 seconds each. Then,
wash the slides with 70% ethanol for 5 minutes. Wash the slides
with flowing water for 5 minutes, and wash the slides with purified
water. Place the slides on a staining basket in a 500-mL beaker
with 500 mL of 10 mmol/L citrate buffer (pH 6.0). Cover the
beaker
with plastic wrap; then process the slides in the autoclave for
10 minutes at 120C.
Hamanishi et al
2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
Let the slides cool down in the beaker at room temperature for
approximately 1 hour. Remove the slides from the citrate buffer and
wash the slides with phosphate-buffered saline (PBS) T (0.3%
Tween-20 in
PBS) two times for 5 minutes each with a magnetic stirrer. Cover
each section with 0.3% H2O2 in MeOH for 15 minutes at room
temperature to block endogenous peroxidase activity.
Wash two times in PBS-T for 5 minutes each with a magnetic
stirrer. Remove the slides from PBS-T, wipe gently around each
section, and cover tissues with blocking solution II (blue
bottle,
Histofine SAB-PO (M) kit; Nichirei, Tokyo, Japan) for 30 minutes
to block nonspecific staining. Do not wash. Tip off the blocking
buffer, wipe gently around each section, and cover tissues with
anti human CD274/PD-L1 antibody
(27A2) diluted with PBS that contains 1% bovine serum albumin at
10 g/mL. Incubate the sections for 1 hour at roomtemperature.
Wash the slides twice in PBS-T for 5 minutes each with a
magnetic stirrer. Wipe gently around each section, and cover
tissues with biotinylated anti-mouse antibody (yellow bottle,
Histofine SAB-PO
kit; Nichirei). Incubate for 30 minutes at room temperature.
Wash the slides twice in PBS-T (0.3% Tween-20 in PBS) for 5minutes
each time with a magnetic stirrer.
Wipe gently around each section, and cover tissues with
streptavidin-peroxidase (pink bottle, Histofine SAB-PO
kit;Nichirei). Incubate for 30 minutes at room temperature. Wash
the slides two times in PBS-T (0.3% Tween-20 in PBS) for5 minutes
each with a magnetic stirrer.
Visualize by reacting for 3 minutes with DAB solution. Wash the
slides with flowing water for 5 minutes, and wash the slide with
purified water. Counterstain with hematoxylin for 3 to 30 seconds,
wash the slides with flowing water for 5 minutes, and wash the
slide with
purified water. Dehydrate by immersing in 70% ethanol and 95%
ethanol for 3 minutes and in ethanol three times for 3 minutes
each
followed by immersion in xylene three times for 3 minutes each.
Ready for mounting.
LSI Medience used an isotype control antibody (mouse
immunoglobulin G2b) as a negative control and conducted an
antibodyabsorption test with recombinant human B7-H1/PD-L1 Fc
chimera (R&D Systems; Minneapolis, MN). Normal placenta
(Super-BioChips, Seoul, South Korea, and US BioMax, Rockville, MD)
was used as a positive control. The expression of PD-L1 was
evaluatedaccording to the intensity of the staining and was scored
as follows: 0, negative; 1, very weak expression; 2, moderate
expression but weakerthan placenta; and 3, equivalent to or
stronger expression than placenta. Occurrences with scores of 0 or
1 were defined as thelow-expression group (low), and occurrences
with scores of 2 or 3 were the high-expression group (high;
Appendix Fig A2). Validation,assessment, and scoring of PD-L1
expression were performed in a third-party review (LSI Medience) by
two independent pathologistswho were unaware of the outcomes.
Validation Study of PD-L1 StainingTo validate PD-L1 expression,
four primary antibodies and three detection agents were tested to
determine the optimal conditions for
immunohistochemistry labeling for the detection of PD-L1.The
primary antibodies were antihuman CD274/PD-L1 antibody (27A2; MBL,
Nagoya, Japan), purified antihuman CD274
(B7-H1, PD-L1) antibody (BioLegend, San Diego, CA), PDL-1
antibody (ProSci, Poway, CA), and antiB7-H1/PD-L1/CD274
antibody(LifeSpan, Seattle, WA). Two kinds of ovarian cancer tissue
microarrays were evaluated to confirm the reproducibility of
staining forPD-L1. Consequently, of the four primary antibodies,
27A2 was the best in terms of staining of PD-L1 compared with human
normalplacenta. Furthermore, the specific staining of PD-L1 was
acquired by incubation with 50L/mL of primary antibody (27A2) for 1
hourat room temperature after heat-induced epitope retrieval at pH
9. The antigen absorption test was performed with recombinant
PD-L1.There was no positive reaction of PD-L1 at placental
epithelial cells. Thus, these results confirmed the specificity of
27A2 antibodies.
Of the 108 ovarian cancer tissues, 83.3% (n 45 , SBC; n 45, UBM)
demonstrated specific staining of PD-L1 (score,1 to3) intwo kinds
of tissue microarrays, whereas 11.1% (n 10, SBC; n 2, UBM) were
negative (score, 0). Finally, 4.6% (n 4, SBC; n 1,UBM) were not
evaluated.
Trial Steering Committee and Data Monitoring Committee
Monitoring CommitteeThe Trial Steering Committee and Data
Monitoring Committee were located at the Department of Data Science
and Clinical
Innovative Medicine, Kyoto University Graduate School of
Medicine, Kyoto, Japan. Every month, the management team monitored
thetrial progress.
Ethical Considerations and RegistrationThe study protocol
complied with the Declaration of Helsinki and the Ethics Guidelines
for Clinical Research published by the
Ministry of Health, Labor, and Welfare of Japan. We obtained
approval for this study from the institutional review board of
KyotoUniversity Hospital on June 23, 2011. The protocol and
informed consent forms were approved by the ethics committee.
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
Table A1. Summary of Exposure to Nivolumab in All Treated
Patients
Factor
No. (%) of Patients by Nivolumab Dose
Total 1 mg/kg 3 mg/kg
Study treatment statusOn study 2 (10) 0 (0) 2 (20)Off study 18
(90) 10 (100) 8 (80)
Follow-up period, monthsMedian 8.0 12.5 5.0SD (range) 5.80
(2-22) 5.83 (3-22) 3.96 (2-15)
Duration of treatment, monthsMedian 4.0 3.5 4.0SD (range) 3.7
(1-12) 3.1 (1-12) 4.2 (1-12)
Key reason for study discontinuation
PD 16 (89) 8 (80) 8 (100)Adverse effect (treatment-related) 2
(11) 2 (20) 0 (0)
Abbreviations: PD, progressive disease; SD, standard
deviation.Total number of patients was 18 (10 patients at 1 mg/kg;
eight patients at 3 mg/kg). The other two patients continued to
receive nivolumab (3 mg/kg) in key reasonfor study discontinuation,
each at the trial end date.Key reason for study discontinuation of
the two patients was thyroiditis.
Table A2. Treatment-Related Serious Adverse Events
Dose No. of Patients Event
1 mg/kg 1 Grade 3 disorientationGrade 3 gait disorderGrade 3
fever
3 mg/kg 1 Grade 3 feverGrade 3 deep vein thrombosis
Table A3. All Adverse Events Regardless of Causality That
Occurred in at Least 20% of All Treated Patients
Event
Total No. (%) of Patients WithEvent by Grade (N 20)
No. (%) of Patients With Events by Grade and Treatment
Cohort
1 mg/kg (n 10) 3 mg/kg (n 10)
All Grades Grade 3 or 4 All Grades Grade 3 or 4 All Grades Grade
3 or 4
Any adverse event 20 (100) 13 (65) 10 (100) 6 (60) 10 (100) 7
(70)AST increased 8 (40) 0 (0) 6 (60) 0 (0) 2 (20) 0
(0)Hypothyroidism 8 (40) 0 (0) 4 (40) 0 (0) 4 (40) 0
(0)Lymphocytopenia 8 (40) 3 (15) 5 (50) 3 (30) 3 (30) 0 (0)Albumin
decreased 8 (40) 3 (15) 2 (20) 1 (10) 6 (60) 2 (20)Fever 6 (30) 1
(5) 2 (20) 1 (10) 4 (40) 0 (0)Arrhythmia 6 (30) 0 (0) 4 (40) 0 (0)
2 (20) 0 (0)ALT increased 5 (25) 1 (5) 4 (40) 1 (10) 1 (10) 0
(0)Cough 5 (25) 0 (0) 3 (30) 0 (0) 2 (20) 0 (0)Maculopapular rash 5
(25) 1 (5) 3 (30) 0 (0) 2 (20) 1 (10)Arthralgia 5 (25) 0 (0) 5 (50)
0 (0) 0 (0) 0 (0)Itching 4 (20) 0 (0) 4 (40) 0 (0) 0 (0) 0 (0)Sore
throat 4 (20) 0 (0) 0 (0) 0 (0) 4 (40) 0 (0)Fatigue 4 (20) 0 (0) 2
(20) 0 (0) 2 (20) 0 (0)Anemia 4 (20) 3 (15) 3 (30) 2 (20) 1 (10) 1
(10)CRP increased 4 (20) 0 (0) 1 (10) 0 (0) 3 (30) 0 (0)
Abbreviation: CRP, C-reactive protein.
Hamanishi et al
2015 by American Society of Clinical Oncology JOURNAL OF
CLINICAL ONCOLOGY
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
-
Baseline
CT CT
0 2 w 4 w
1 cycle Approx. 6 cycles
6 w
PD orprogression
CT
Nivolumab1 mg/kg, n = 103 mg/kg, n = 10
w 84w 8
CR, PR, SD Follow-up
Off study
Fig A1. The trial scheme. Eligible patients were allocated
sequentially to the nivolumab low-dose (1 mg/kg; n 10) or high-dose
(3 mg/kg; n 10) cohort. The phaseII efficacy trial defined a
primary end point of response rate and a composite secondary end
point of safety. Patients received nivolumab intravenously every 2
weeks,and their lesions were evaluated by computed tomography (CT)
every 2 months for up to 1 year or until progressive disease (PD;
assessment of treatment effect onthe basis of RECIST version 1.1)
or clinical disease progression (progression), defined as
symptomatic deterioration. Adverse effects were assessed on basis
of theCommon Terminology Criteria for Adverse Events version 4.0.
CR, complete response; PR, partial response; SD, stable
disease.
Assessed for eligibility(N = 135)
Registration(n = 21)
Cohort transition
Excluded Did not meet inclusion criteria Refused to
participate
(n = 114)(n = 114)
(n = 0)
1 mg/kg cohort Received allocated intervention Did not receive
allocated intervention (disease progression after registration)
(n = 11)(n = 10)(n = 1)
3 mg/kg cohort Received allocated intervention Did not receive
allocated intervention
(n = 10)(n = 10)(n = 0)
Lost to follow-upDiscontinued intervention Progressive disease
Adverse effect (treatment related)
(n = 0)
(n = 8)(n = 2)
Lost to follow-upDiscontinued intervention Progressive disease
Adverse effect (treatment related)
(n = 0)
(n = 8)(n = 0)
Analyzed Excluded from analysis
(n = 10)(n = 0)
Analyzed Excluded from analysis
(n = 10)(n = 0)
Fig A2. Flow diagram of patient progress through the steps of
this trial.
AntiPD-1 Antibody for Ovarian Cancer
www.jco.org 2015 by American Society of Clinical Oncology
from 211.144.221.1Information downloaded from jco.ascopubs.org
and provided by at HOFFMANN-LA ROCHE AG on September 15, 2015
Copyright 2015 American Society of Clinical Oncology. All rights
reserved.
Safety and Antitumor Activity of AntiPD-1 Antibody, Nivolumab,
in Patients With Platinum ...INTRODUCTIONPATIENTS AND METHODSStudy
Design and PatientsProcedureOutcomesStatistical AnalysisDrug and
Drug SupplyImmunohistochemical Analysis of PD-L1
RESULTSBaseline Patient CharacteristicsSafetyClinical
ActivityPD-L1 Expression on Tumor Cells
DISCUSSIONREFERENCESAcknowledgmentAppendix










![PARP inhibitors: clinical development, emerging ...€¦ · ARIEL2, Part 1 NCT01891344 (2017)[21] 2 Recurrent, platinum-sensitive high-grade ovarian cancer, received at least 1 platinum-based](https://img.pdfslide.net/doc/110x75/5f01af2a7e708231d4008c8d/parp-inhibitors-clinical-development-emerging-ariel2-part-1-nct01891344-201721.jpg)
















