Embed Size (px)
Citation preview
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New Jersey Com-muni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Continued from/on page x
Caption is this
Subhead
PHOTO BY: ANWAR WALKER, PUBLIC HEALTH REPRESENTATIVE
Funding to Expand continued from page 1
The newly detectedavian influenzavirus (H7N9) and
the Middle EastRespiratory Syndromecoronavirus (MERS - CoV),which are currentlycausing illness inindividuals internationally,continue to be of concernto the New Jersey Department ofHealth (NJDOH). While it isimportant to note that there have notbeen any cases of illness associatedwith these viruses in New Jersey orthe United States, the NJDOHcontinues to closely monitor thesituations. Officials from theNJDOH are conducting respiratoryillness surveillance designed torapidly identify any individuals whomay become infected with theseviruses.
While these two viruses are notrelated, and are currently affectingpatients in different parts of theworld, each of them may cause severeacute respiratory illness (SARI).
MERS-CoVAs of July 29, 2013 WHO has beeninformed of a total of 91 laboratory-confirmed cases of infection withMERS-CoV, including 46 deaths
internationally. These cases have alloriginated in the following countries inthe Middle East Arabian Peninsula:Jordan, Qatar, Saudi Arabia, and theUnited Arab Emirates (UAE). France,Germany, Italy, Tunisia and the UnitedKingdom have also had cases that wereeither transferred there for care of thedisease, or returned from the MiddleEast, and subsequently became ill.International public health officials areworking with the Centers for DiseaseControl and Prevention (CDC) to learnmore about the virus, its source, andhow it is spread. Several clusters havebeen investigated indicating thatperson-to-person transmission hasoccurred but, to date, has not been
Summer 2013
Communicable DiseaseService Mission StatementOur mission is to prevent communicable disease amongall citizens of New Jersey, andto promote the knowledge anduse of healthy lifestyles to maximize the health and well-being of New Jerseyans.
We will accomplish our mission through our leadership,collaborative partnerships, andadvocacy for communicable disease surveillance, research,education, treatment, prevention and control.
Chris Christie, Governor
Kim Guadagno, Lt. Governor
Mary E. O’Dowd, MPHCommissioner
COMMUNICABLE DISEASE SERVICEChristina Tan, MD, MPHState Epidemiologist/Assistant Commissioner
Gary Ludwig, MS, Director
Suzanne Miro, MPH, MCHESEditor, Research Scientist
Continued on page 3
By: Lisa McHugh, Epidemiologist
C1950
NJDOH Monitoring for SevereAcute Respiratory Illness (SARI)in Returning Travelers
Coronaviruses are common worldwide. Theyusually cause colds. However, a novel coronaviruscalled “Middle East Respiratory SyndromeCoronavirus” (MERS-CoV) has caused severeillness and death in people from several countries.Learn more about MERS-CoV athttp://www.cdc.gov/Features/novelcoronavirus/.
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 2
Get more information athttp://nj.gov/health/cd/handwashing.shtml.
Vaccine preventable diseaseshave no age limits—they canstrike at any time in a
person’s lifespan. Far too manyadults become ill, are disabled, anddie each year from diseases thatcould easily have been prevented byvaccines. Throughout adulthood,immunizations help maintainprotection against certain diseases.
Influenza: All adults arerecommended to get a flu vaccineevery year. Every year in the U.S.,an average of 24,000 people diefrom the flu. Most of these deathsare among adults 65 years old andolder. Flu vaccination is especiallyimportant for adults 65 years of ageand older, people with chronichealth problems (such as diabetes,asthma, sickle cell, lung, heart, liver,or kidney diseases), people who livewith or care for people at high risk,people who live with or care forinfants and children, pregnantwomen, and health care workers.
Pertussis (Whooping Cough): Alladults need a one-time dose oftetanus, diphtheria, acellularpertussis (Tdap) vaccine. Adultsshould get Tdap in place of one oftheir regular tetanus boosters—thetetanus-diphtheria (Td) shot that isrecommended for adults every 10years. The dose of Tdap can begiven no matter when the last Tdshot was received.
Pertussis can be a serious, evendeadly, disease in babies. For thisreason, expectant mothers should
get one dose of Tdap during eachpregnancy, preferably at 27 through36 weeks. Receiving Tdap duringpregnancy helps to provide theinfant protection against pertussis inearly life, before the baby is eligibleto receive the childhood vaccine.
Chickenpox (Varicella): Chickenpoxcauses an itchy rash with blisters,tiredness, headache and fever.Chickenpox is usually mild, but itcan lead to severe skin infections,pneumonia, or even death. Adultswith chickenpox often have a higherfever, longer illness, and a worserash than children. They are seventimes more likely to suffer fromencephalitis (infection of the brain).
Two doses of varicella vaccine arerecommended for adults who havenot had chickenpox disease.
You Don’t Outgrow the Need forImmunizations By: Jennifer Smith, Health Educator
Continued on page 4
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 3
sustained. No casesof MERS – CoVhave been reportedin the UnitedStates.
H7N9An outbreak ofavian influenza A(H7N9) virus hasrecently affectedseveral provinces inChina, with 132human cases and 37deaths reported.
Most cases have had direct or indirectcontact with poultry. Noperson-to-person transmission has beendefinitively documented, though severalsmall clusters have occurred in whichperson-to-person transmission couldnot be ruled out. No cases of H7N9infection have been reported in theUnited States.
Advice for New Jersey ResidentsIf people get sick with fever, coughing,or shortness of breath within 10 days ofreturning from China, or within 14 daysof returning from countries in or nearthe Arabian Peninsula*, they shouldseek medical care and inform thehealth care provider about recent travel. The NJDOH will update its website asmore information becomes available.For more information, please visit:
MERS – CoVhttp://nj.gov/health/cd/mers/index.shtml
H7N9http://nj.gov/health/flu/surveillance.shtml
Additional information can also befound on the CDC website at:http://www.cdc.gov/coronavirus/index.html http://www.cdc.gov/flu/avianflu/h7n9-virus.htm
CDC travel websites:http://wwwnc.cdc.gov/travel/notices/watch/coronavirus-saudi-arabia-qatarhttp://wwwnc.cdc.gov/travel/notices/watch/avian-flu-h7n9-china
*Countries in and near the ArabianPeninsula: Bahrain, Iraq, Iran, Israel,Jordan, Kuwait, Lebanon, Oman,Palestinian territories, Qatar, Saudi Arabia,Syria, the United Arab Emirates (UAE),and Yemen.
MERS - CoV, continued from page 1
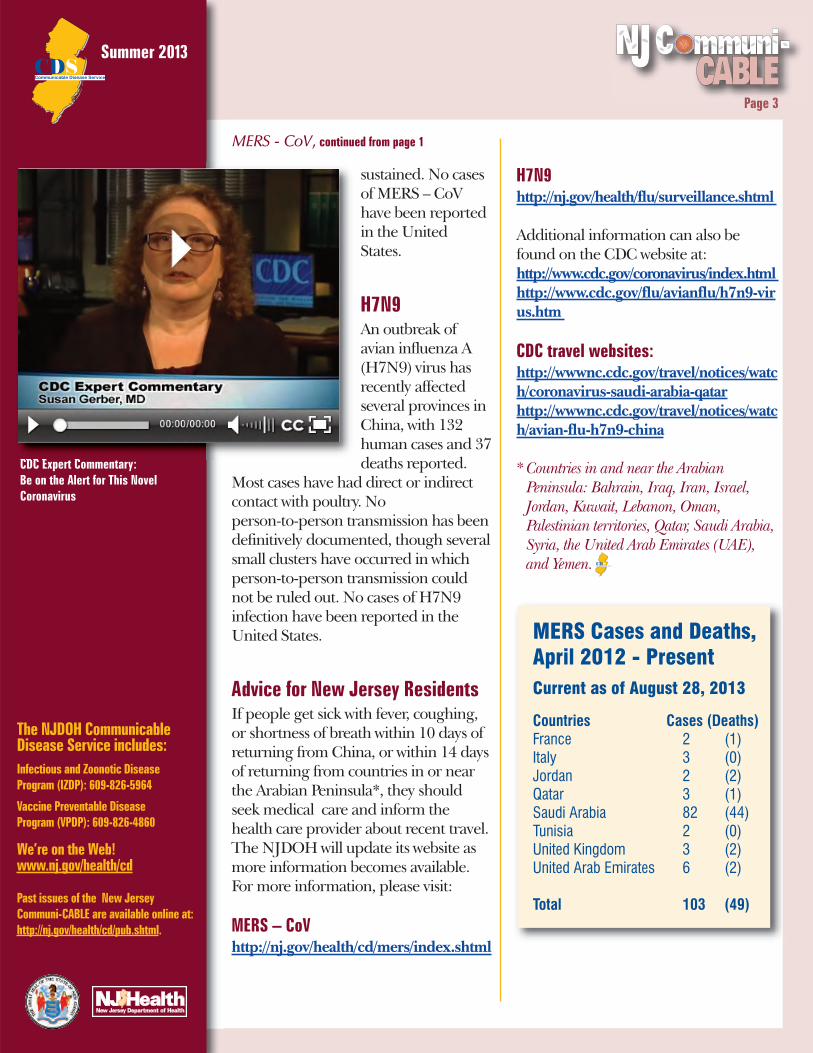
MERS Cases and Deaths,April 2012 - PresentCurrent as of August 28, 2013
Countries Cases (Deaths)France 2 (1)Italy 3 (0)Jordan 2 (2)Qatar 3 (1)Saudi Arabia 82 (44)Tunisia 2 (0)United Kingdom 3 (2)United Arab Emirates 6 (2)
Total 103 (49)
CDC Expert Commentary:Be on the Alert for This NovelCoronavirus
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Shingles (Herpes Zoster): Shingles is adisease that causes a painful,blistering rash. One in five peoplewith shingles will have severe,long-term pain after the rash heals.Nearly one million Americans getshingles every year and about half ofthem are 60 years old and older.Anyone who has had chickenpox is atrisk of shingles. One dose of thisvaccine is recommended for adults 60years and older, whether or not theyhave had shingles.
Measles, Mumps, Rubella (MMR): Measles, mumps, and rubella areserious diseases. Before vaccines theywere very common, especially amongchildren. Adults born in 1957 orlater should have documentation ofone or more doses of MMR vaccine.
Pneumococcal disease: Pneumococcal disease can causeserious infection of the lungs(pneumonia), the bloodstream(bacteremia), and the covering of thebrain (meningitis).
Pneumococcal disease is one of themost common causes of vaccine-preventable death in the U.S. and isparticularly dangerous for older adults.All adults ages 65 and older need onedose of pneumococcal polysaccharidevaccine (PPSV23). Some adults mayneed additional doses of this vaccine ormay also need pneumococcal conjugatevaccine (PCV13).
The specific vaccines needed as anadult are determined by factors suchas age, lifestyle, risk conditions,locations of travel, and previous
Page 4
Immunizations, continued from page 2 vaccines. Some adults may alsoneed vaccines for humanpapillomavirus (HPV),meningococcal disease, hepatitis A,and hepatitis B. Health carepersonnel should have evidence ofimmunity to certain diseases toprotect themselves and theirpatients. Please see the followinglink for the Centers for DiseaseControl and Prevention (CDC)recommendations of immunizationsfor health care personnel,http://www.cdc.gov/mmwr/pdf/rr/rr6007.pdf
Adult vaccination coverage remainslow for most routinelyrecommended vaccines and wellbelow Healthy People 2020 targets.Many adults are not even aware thatthere are vaccines that can preventthese diseases and some adults aremisinformed about theireffectiveness and longevity ofprotection. Health care providerscan implement practices shown toimprove adult vaccination. Thesepractices include assessing patients’vaccination needs, routinelyrecommending and offering neededvaccines to adults, implementingreminder-recall systems, creatingstanding orders for vaccination, andreviewing practice-level vaccinationrates with feedback to staffmembers.
For more information about adultimmunization, please visit theCDC’s new adult vaccinationwebsite:http://www.cdc.gov/vaccines/adults/index.html
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 5
When the word ‘research’ ismentioned, what words cometo mind that are associated
with it? Data might be one of the firstones spoken. When the word‘epidemiology’ is mentioned, what wordscome to mind that are associated with it?Once again, data might be the first onespoken. Hence, the unique link betweenresearch and epidemiology. For thisreason, we chose to review a timely articleon fungal infections associated withcontaminated methylprednisoloneinjections from a single compoundingpharmacy in New England. BarbaraCarothers, LPN, a public health staffperson at the NJ Department of Health(NJDOH), and LPN Forum boardmember, participated in data collectionrelated to this issue, and shared herknowledge and experience as part of thisemergency public health response, as acoauthor in an article published in theNew England Journal of Medicine (Seereference below). In the followingdiscussion, Dr. Susan Fowler, New JerseyNurseResearch Corner editor, andBarbara Carothers share the details ofthis critical event.
The trigger for this emergency publichealth response is referred to as anindex patient, a 56 year old patient withaspergillus meningitis who had receivedan epidural glucocorticoid injection forlower back pain at an ambulatorysurgical center 46 days earlier.Additional patients were identified inTennessee, four of whom sufferedposterior circulation strokes. All
patients had received medication froma single compounding pharmacy inNew England. After being notified, thepharmacy voluntarily recalled three lotsof medications, but more states beganto report additional cases of fungalmeningitis and stroke.
The NJDOH started a promptinvestigation surrounding the facilitieswho received the products and the localhealth departments (LHDs) wherethese facilities were located. Regionalepidemiologists covering thejurisdictions of facilities receivingimplicated lots were initially notifiedand asked to assist facilities withidentifying patients exposed to thethree implicated lots. Regionalepidemiologists were asked to makecontact with these facilities and assistwith assembling lists of patientsexposed to these lots because of theamount of data collection necessary.The facilities (with help from theregional epidemiologist in some cases)were responsible to contact patients.
Patients who may have received theimplicated medication were contactedby phone calls and door-to-door visits.They were instructed not to leave avoice message, but to speak with thepatient or caregiver personally. TheCenters for Disease Control andPrevention (CDC) requested all patientnotification completed by 5 pm onMonday, October 8, 2012.
Staff at the NJDOH coordinated patientoutreach and data collection for the
Fungal Infections Associated with ContaminatedMethylprednisolone Injections: Review andInsights* By: Susan B. Fowler, PhD, RN, CNRN, FAHA and Barbara Carothers, LPN
* Reprinted with permission from NJ Nurse Continued on page 6

Summer 2013
The NJDOHCommunicable DiseaseService includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are availableonline at:http://nj.gov/health/cd/pub.shtml.
Page 6
osteomyelitis, or worseninginflammatory arthritis of a joint after aninjection, without a known cause.
Physicians were asked to have a lowthreshold for lumbar puncture andmagnetic resonance imaging (MRI) atthe site of injection. Clinical records werereviewed and symptomatic patientsclassified using CDC case definitions.The current New Jersey case count as ofJanuary 28, 2013, was 48 with 41meningitis cases, (six also have anabscess/osteomyelitis), six patients withabscess/osteomyelitis, and one individualsuffering from a joint infection.
Initially, facilities were asked to follow-upwith patients for three months after theirlast injection. As the investigationevolved and the incubation periodbecame longer, follow-up has increasedto six months following the lastinjection. The NJDOH has providedguidance, including an algorithm, toassist facilities with follow up.
Over 13,000 persons were identifiednationally as having the potential forbeing exposed to medication from atleast one of the three lots with mostexposed through epidural, spinal, andparaspinal injections. By mid- December,590 cases had been identified in 19 stateswith 37 patients having died.Thirty-three cases (9%) had sufferedstrokes and when the location was known,24 (96%) involved the posteriorcirculation. Therefore, a relatively smallproportion of exposed individualsdeveloped disease as result of exposure.Unfortunately, these numbers may beunderestimates since there still has notbeen sufficient time for symptoms to bemanifested clinically.
facilities in New Jersey. A script wasprovided and disseminated by theNJDOH to the facilities. NJDOH alsoprovided them with talking points (whichwere updated throughout the outbreak),on-line lists, and questionnaires for useduring communication with patients orcaregivers.
The process of identifying cases beganwith a chart review to compile a list ofpatients potentially exposed to thecontaminated product. Symptomaticpatients were advised to seek medicalevaluation immediately andasymptomatic patients were advised toseek medical evaluation should theybecome symptomatic. New Jersey’sCommunicable Disease Reporting andSurveillance System (CDRSS) was utilizedto keep track of patients who presentedfor evaluation and/or became cases.
Staff at the NJDOH learned, throughspeaking with the providers’ officepersonnel, that some patients were veryconcerned and sought medicalevaluation immediately, even thoughthey were not symptomatic. Some wereconcerned about the financial aspect ofdiagnosis and treatment, and werereluctant to have testing done.
The definition of a case changed alongthe course of this outbreak, but an earlydefinition included one of the following:1) meningitis of unknown cause thatdeveloped after an epidural orparaspinal injection; 2) posteriorcirculation stroke due to presumedmeningitis after an injection; 3) cliniciandiagnosed osteomyelitis, abscess, orother infection of unknown cause inspinal or paraspinal structures or nearinjection site; and, 4) clinician diagnosed
Fungal Infections, continued from page 5
Continued on page 8
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 7
Our dear friend andco-worker, Kim Bernini,passed away on Monday,June 10, 2013. Kim wasan important part of theCommunicable Diseasesupport staff, havingworked for theDepartment of Health forover 10 years. She was afriendly face in theworkplace as well as ahelpful voice on thephone, providing variouscallers with requestedinformation.
Faye Sorhage retired from the NJDepartment of Health (DOH) onAugust 1st, after 28 years of service. Sheis looking forward to reading mysteries,gardening, going to museums,traveling, volunteering, and doing lotsof walking and exercise. She also plans
to do part-timeconsulting on rabies,zoonotic diseases andanimal facility/welfareissues. She can bereached [email protected].
CDS Says Farewell, but Not Goodbye toColleagues
Faye Sorhage, State Public Health Veterinarian
Without being selected to be a part ofthe Public Health Associate Program(PHAP) fellowship, I would not havehad the exceptional opportunity to jointhe NJDOH. When asked about myfellowship experience, I say that “It wastime well spent.” I could not imagine abetter entry-level experience into theincredible field of public health. Thewealth of knowledge, and the beautifulpersonalities, amongst individuals inthe program is extraordinary. Everyonecontributed in making the new workenvironment, long commutes andstressful work days joyous. I gainedexposure in many interesting areas ofpublic health, which all were very
intriguing, and thefellowship providedan opportunity todevelop various skillsthat will betransferable to mysecond-yearassignment andthroughout my professional career. InJuly, I transitioned into the second yearof the fellowship, working at the CDCDepartment of Global Migration andQuarantine station, located at theNewark Liberty Airport. I’m certain thatthe professional relationships that wereformed, will continue to grow for years tocome.
A Personal Note from Fernando McLean
Farewell

Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
In New Jersey, 40 cases were identifiedfrom 639 persons potentially exposed.This number equates to an attack rate of6.3 (number of cases/100 personspotentially exposed). This number haschanged to 705 potentially exposed.
When a symptomatic patient presentsfor evaluation, specimens obtained fromlumbar puncture, joint aspiration, andsurgical intervention, for example, aretested at the facility (or commercial lab).Specimens from case patients and casesunder investigation are sent from thefacility to the CDC for further testing.This process is coordinated by the statehealth department and public healthlaboratory. Any case or case underinvestigation is issued a NJ case numberby the CDC. This number is used fortracking specimens and results.
Authors highlight the fact that thisinvestigation was part of an emergencypublic health response. The experiencedefinitely felt like an emergency,according to staff at the NJDOH. Acrossthe country case counts and deaths wereincreasing and details were changingdaily. It was of utmost importance toidentify and notify patients potentiallyexposed to the implicated products.The NJDOH formed an outbreakinvestigation team consisting of expertsin clinical care, surveillance,communications, and logistics. TheNJDOH provided written guidance tothe facilities, hosted conference calls forthe affected facilities, clinicians, andregional epidemiologists. Various LocalInformation Network System (LINCS)messages to healthcare and publichealth groups were disseminated toprovide an overview of the investigation,clarify clinical issues, offer guidance, and
provide updates on the situation.Information, Frequently AskedQuestions, and talking points wereposted on the NJDOH website andupdated as the outbreak evolved.
Treatment was critical for suppressingor preventing fungal infection. Over50% of case patients receivedvoriconazole alone, 42% received bothvoriconazole and amphotericin B, andless than 1% amphotericin B alone.The overall attack rate was 4.4 cases per100 exposed persons.
Authors presented substantial datareflecting epidemiological andlaboratory answers and trends. Tablesand figures can succinctly explain thedata, often more than written words.Columns in tables addressed all cases,those with meningitis only, spinal andparaspinal injections only, andperipheral joint infections only. Thefirst column held the most datafollowed by the meningitis onlycolumn. The article included a figurefrom date of initial symptom onset witha steady increase from Sept. 7, 2012 toOctober 5, 2012 (almost one month).Readers can visit the CDC website foradditional information (www.cdc.gov).
Note: Carothers comments that “Myprimary role in this investigation was toassist with case finding and datacollection by reviewing medical recordsincluding results of diagnostic studies. Icontinue today to sift throughemergency room (ER) records, cliniccharts, progress notes and MRIs to helpidentify and classify new cases. I alsoassist with patient follow-up andprovide facility guidance.”
Rachel M. Smith, M.D., M.P.H., Melissa
Page 8
Fungal Infections, continued from page 6
Continued on page 9
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 9
K. Schaefer, M.D., Marion A. Kainer,M.B., B.S., M.P.H., Matthew Wise,Ph.D., Jennie Finks, D.V.M., M.V.P.H.,Joan Duwve, M.D., M.P.H.,Elizabeth Fontaine, M.S.P.H., AlvinaChu, M.H.S., Barbara Carothers,L.P.N., Amy Reilly, R.N., Jay Fiedler,M.S., Andrew D. Wiese, M.P.H.,Christine Feaster, R.M., Lex Gibson,B.S., Stephanie Griese, M.D., AnnePurfield, Ph.D., Angela A. Cleveland,M.P.H., Kaitlin Benedict, M.P.H., Julie
R. Harris, Ph.D., M.P.H., Mary E.Brandt, Ph.D., Dianna Blau, D.V.M.,Ph.D., John Jernigan, M.D., J. ToddWeber, M.D., and Benjamin J. Park,M.D., for the Multistate FungalInfection Outbreak Response Team.(Dec. 19, 2012). Fungal InfectionsAssociated with ContaminatedMethylprednisolone Injections—Preliminary Report. New EnglandJournal of Medicine.DOI:10.1056/NEJMoa1213978
Fungal Infections, continued from page 8
Abig thank you to the “SafeInjection Ambassadors,” avaluable group of 25 health
care professionals who volunteeredto help the New Jersey Departmentof Health educate healthprofessionals about safe injectionpractices. Ambassadors attended aday-long training, receivedmaterials to teach about NJ’s safeinjection program, agreed to
present at leasttwo presentationswithin one yearof being trainedand passed aqualifying exam! Sincebeing trained in 2012, theAmbassadors have conducted 61presentations to nearly 800individuals!
Injection Safety
In May, staff from theCommunicable Disease Service andthe Division of HIV/AIDS, TB and
STD Services presented a day-longtraining called “Birds of a Feather:Integrating Hepatitis into STD andHIV Prevention Services” to 25 HIVand Risk Reduction Counselors atRutgers University. This is a newtraining designed to integrate hepatitisprevention into existing STD and HIVprevention services. The trainingcoincided with May as NationalHepatitis Awareness Month.
Bridging Hepatitis and STD Prevention
Amelia Hamarman, Health Educator in theDivision of HIV/AIDS, TB and STD Services, leadsthe group in a learning activity.
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
April 17, 2013 Edward J. Septimus, MD, ClinicalProfessor of Internal Medicine atTexas A&M Health SciencesCenter, a proponent ofantimicrobial stewardship, recentlystated during an interview for theAgency for Healthcare Researchand Quality that antibioticresistance continues to be a seriousthreat to public health. This is aglobal phenomenon with theWorld Health Organization reporting that 440,000 newcases of multidrug-resistant tuberculosis occur annually.Extensively drug-resistant tuberculosis has been reportedin 64 countries to date. Dr. Septimus promotes the Centersfor Disease Control and Prevention’s campaign “Get SmartAbout Antibiotics” as a way to educate health care providersto reduce the inappropriate use of antibiotics. Thecampaign provides resources for the public and for healthcare professionals.http://innovations.ahrq.gov/content.aspx?id=3762
May 22, 2013 The U.S. Department of Healthand Human Services (HHS) hasformed a strategic alliance todevelop new antibiotics. Thedrugs will be developed under apublic-private partnershipagreement between the HHS’Biomedical Advanced Research and DevelopmentAuthority and GlaxoSmithKline. This initiative will take aportfolio approach to developing multiple products in aneffort to develop a robust pipeline of novel antibioticsrather than individual products. Ultimately, is it is hopedthat this will enhance the ability to provide medicalcountermeasures for biodefense.http://www.phe.gov/Preparedness/news/Pages/strategic-alliance-130522.aspx
Page 10
Antibiotic Resistance
NEWS.......................................In The
Summer 2013
The NJDOH CommunicableDisease Service includes:Infectious and Zoonotic Disease Program (IZDP): 609-826-5964
Vaccine Preventable Disease Program (VPDP): 609-826-4860
We’re on the Web!www.nj.gov/health/cd
Past issues of the New JerseyCommuni-CABLE are available online at:http://nj.gov/health/cd/pub.shtml.
Page 11
Suzanne Miro, Health Educatorwith the Communicable DiseaseService, was invited to speak at
the 64th Annual Meeting of the Societyfor Public Health Education, April 19,2013. An unlikely gathering of threehealth educators, with very differentbackgrounds, provided for aninteresting and lively panelpresentation of how health education has evolved overthe years and has been shaped by three significantpublic health issues (polio, bioterrorism, and war).
Suzanne’s role in the 2001 anthrax emergency wasone that has provided unique insight regarding healtheducation during a bioterrorism response effort. “Ithas been quite a while since I have given a talk aboutthe anthrax response so it was an opportunity Iwelcomed.” Titled “Eleven Years Later: HealthEducation After Anthrax” the presentation providedan overview of the anthrax response and howbioterrorism changed the way health educators withinpublic health departments do their jobs. Waxing andwaning federal funding has also had a great impact onthe role of health educators in emergencypreparedness. “Even though funding for public healthpreparedness continues to shrink, I hope I was able toconvey the fact that the skills of a health educator areextremely valuable during an emergency and that ourskills are not easily replaced,” stated Suzanne.
CDS Health Educator Talks History at National ConferenceH