Embed Size (px)
Citation preview

NoCVA HEN CAUTI Campaign Learning from Defects
Shelby Lassiter, BSN, RN, CPHQ, CIC
Kathy Steele, BSN, RN
October 11, 2012

Polling Question 1
I am experienced in doing defect analyses (root cause analyses) and am confident analyzing CAUTI events to learn from individual events as well as several events in aggregate. TRUE FALSE
Polling Question 2
I know what CUSP is and am experienced in applying CUSP principles in my unit. TRUE FALSE
Objectives
Participants will be able to: • Define CUSP and list the five steps • Define “defect.” • Describe at least one concept about why defects
occur. • Describe the first step in analyzing a CAUTI as a
defect. • Define “psychological safety” and describe why it is
important for a thorough defect analysis.
The Five Steps of CUSP
1. Educate on the Science of Safety 2. Identify defects (today) 3. Engage leadership (now and future) 4. Continue to learn from defects (today) 5. Teamwork and communication (now and future)

What is CUSP?
Comprehensive Unit-based Safety Program
Strategic framework for safety improvement that integrates communication, teamwork, and leadership to create and support a culture of patient safety that can prevent harms.
It features:
• evidence-based safety practices,
• staff training tools,
• standards for consistently measuring harms (infection rates such as CLABSI),
• engagement of leadership, and, tools to improve teamwork among health care team members.
New CUSP Toolkit and Location
« Now on AHRQ website
« Added tools, resources such as videos
http://www.ahrq.gov/cusptoolkit/
CUSP: Identifying and Learning from Defects
Tap into the website tools to enhance your LfD process.

What is a Defect ?
Defect: • Any clinical or operational event or situation that you
would not want to happen again. May include events that you believe actually caused harm or put patients at risk for significant harm.
Johns Hopkins’s “Learning from Defects” tool from CUSP Toolkit at http://www.ahrq.gov/cusptoolkit/identify.htm . Accessed Oct 8, 2012.

Definitions
Defect Analysis: -the process of analyzing a defect to determine its root cause.
Defect Prevention: -the process of addressing root causes of defects to prevent their future occurrence.
Lanier K. Experiences In Root Cause Analysis and Defect Prevention Methods. Presentation publically available at http://www.dtic.mil/ndia/2004cmmi/CMMIT5Tue/Root_CauseAnalysis.pdf
Accessed April 2010.

Basic steps in the “L-from-D” Process
1. What happened? 2. Why did it happen? 3. How will you reduce the likelihood of it
happening again? 4. How will you know the risk is reduced? 5. With whom should you share the
learning?

Why bother?
• Reimbursement systems are being reengineered to reward the best performers (no margin, no mission, no salary, no job…)
• Growing transparency of outcomes • Defects are expensive in many ways… • Excellence in care provided - learning from each defect is
the best way to prevent it from happening again • The Golden Rule-it’s what we’d want done for us or the
person we love most!

It’s All About Prevention
• Learning from defects reduces the likelihood of event occurring again and causing harm.
• Learning may occur in two areas: o System design o Human behavior
• Using a tool to aid learning provides structure and consistency • Learning from each CAUTI (or any type of harm) allows
learning from common cause variations. • Learning from defects that might contribute to CAUTIs (any
type of harm) allows prevention further “upstream” from the harm to make care even safer.

Background Concept #1
Normalized deviance: (Workarounds, short-cuts) Long-term phenomenon in which individuals or teams repeatedly accept a lower standard of performance until that lower standard becomes the “norm.”
I.e. what starts out as a deviation from SOP becomes routine practice and is “normalized.” It becomes acceptable and may no longer even be recognized as deviation. (Just Culture terms for this: behavioral drift, at-risk behavior)
• Allowed because we get away with it…most of the time…

A Famous Example: Challenger Tragedy
• NASA team accepted a lower standard of performance on solid rocket booster O-rings.
• Got comfortable with seeing occasional O-ring damage. • By the time Challenger launched, O-ring damage was
considered a marginal problem. • In 1986, O-ring damage had become an accepted normalized
deviance. • On 1/28/86, Challenger exploded soon after take-off, killing all
7 crew members.

What are some common healthcare normalized deviances?
• Inconsistent hand hygiene practices. • Not disinfecting aspiration ports on Foleys when
obtaining specimens. • Using the same container to empty urine collection bags
in semi-private rooms. • Hanging the Foley bag on the walker or gait belt when
ambulating the patient or throwing it up on the stretcher during transport or hanging it from the side-rail.
• Diapering patients with diarrhea. • What else?

Excuses to Deviate
• “The rule(s) is stupid” –May not appear to have value • Rule or reason for it is unknown – Not valued • New technology • Complexity of work • Rule does not apply to this patient • “Rule(s) doesn’t apply to me” • “I know a better way” • Healthcare worker is not the one at risk in most situations. • Competing priorities:
o Cost and time, o Culture (politics, hierarchy, lack of communication openness, etc.)
• “It won’t hurt anything this one time…” –Assumed or minimal consequences.

Background Concept 2: Errors in Complex Systems
Active Failures
Active failures: errors that occur at the point of contact between a human and some aspect of a larger system (e.g., a human-machine interface). • They are generally readily apparent (e.g., pushing
an incorrect button, not securing a Foley) and almost always involve someone at the frontline or “sharp end”.

Latent Failures
• Latent Failures: less apparent failures of organization or design that contribute to the occurrence of errors or allowed them to cause harm to patients.
• Occurrences are at the “blunt end” but may result in active failures on the “sharp end.”
• AKA: “Accidents waiting to happen.”
Reason JT. Human Error. New York, NY: Cambridge University Press; 1990.

Swiss Cheese Model
Background Concept 3:
Analysis of a defect should occur as soon as possible after the defect is recognized.
The best light is often that from a burning bridge….
~Don Henley

A Review: The 5 Steps in the LfD Process
1. What happened? 2. Why did it happen? 3. How will you reduce the likelihood of it
happening again? 4. How will you know the risk is reduced? 5. With whom should you share the
learning?

Tips For HAI LfDs
• It is rare to find the exact source in a non-outbreak-related infection.
• HAIs are usually the culmination of many infection prevention breaches. (More than one hole lined up in the Swiss cheese…)
• Your job in a defect analysis is to search for the contributing factors that were most likely to have culminated in the infection in this particular patient.
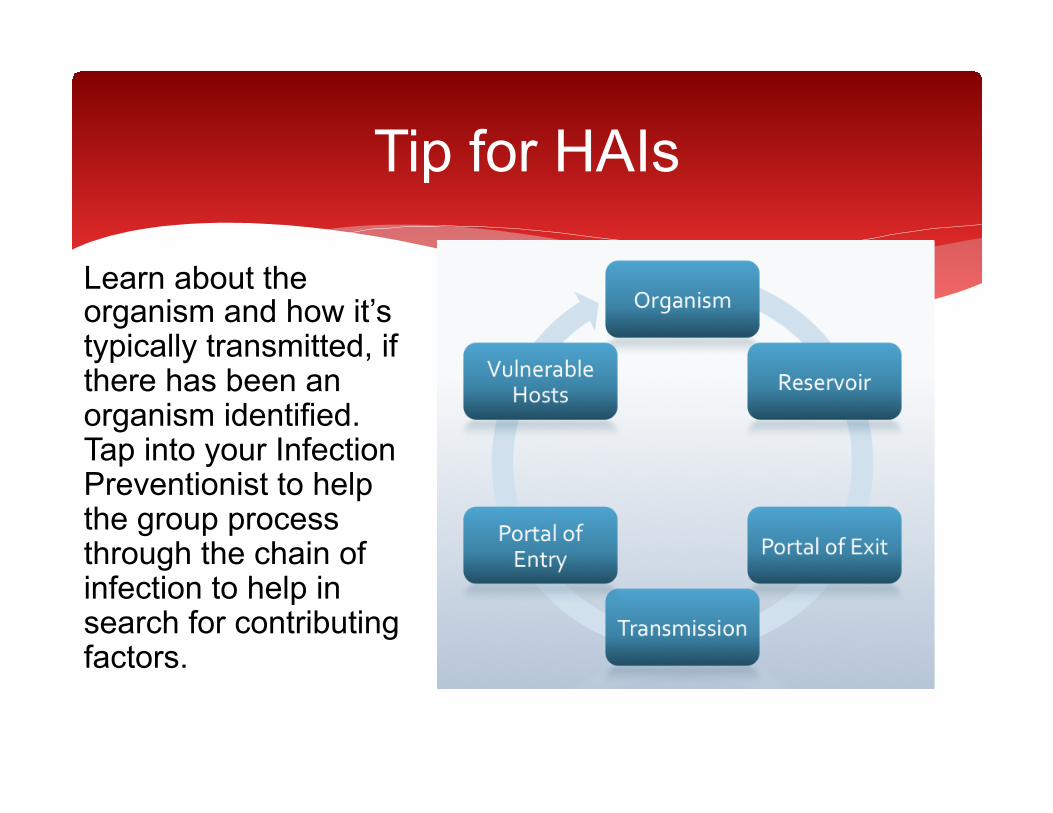
Tip for HAIs
Learn about the organism and how it’s typically transmitted, if there has been an organism identified. Tap into your Infection Preventionist to help the group process through the chain of infection to help in search for contributing factors.
Need to learn:
• What is organism? • Is this particular organism a MDRO? • Where is it commonly found in nature? • How is it transmitted? • How common is it in your organization? • How long can it live in the environment?

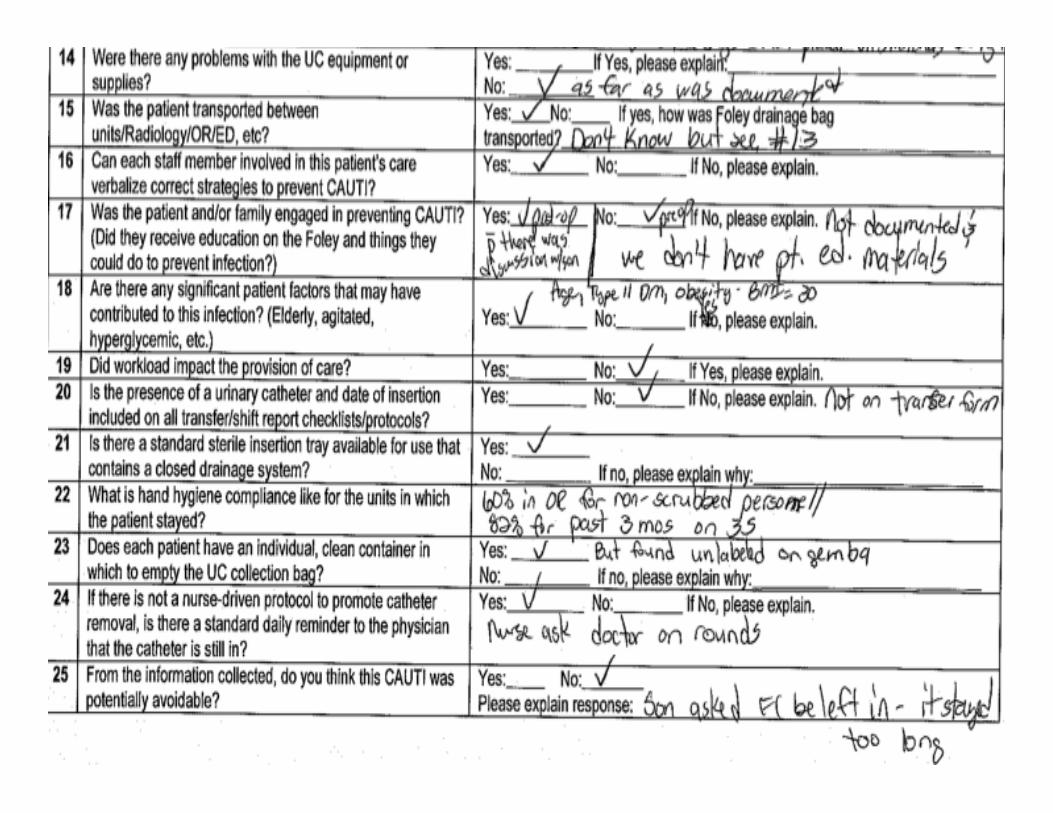
Step 1: What Happened?
• Use a standard event investigation format. • No perfect form so use what is familiar and accepted that
accomplishes the goal. • Must establish a chronological order of events and data
related to the event. • Usually requires some research and walking the process. • The same person should not do all the research/walking
the process. • Include assessment for active and latent failures.

Case Study
• Jerri, a 72 yo female was admitted for THR on 3/10/11. • A #16 Fr. Foley was placed in OR just before surgery. • On 3/10 post-op, she experienced quite a bit of pain but was
otherwise stable. • Foley was due to come out on a.m. of 3/11, but her son
requested it be left in to avoid having her get up to go to the BR. The Foley remained in until 3/13 a.m.
• On 3/14, the patient spiked a fever to 101.40 F and was pan-cultured. UA was + for LE, nitrites, and 4+ bacteria in a cathed specimen. All cultures were negative except for urine, which grew out >100,000 CFU of Pseudomonas aeruginosa. CXR was negative.
Pseudomonas aeruginosa
• Gram negative rod. • Commonly found in soil and
water. • Is frequently found on surfaces
of plants and occasionally on animals.
• Favors moist environments and is often found in biofilm in faucets and sink drains.
• Opportunistic pathogen in humans: it exploits some type of break in host defenses to infect and rarely causes infection in healthy humans.
• It is primarily a nosocomial pathogen
• Reportedly colonizes more than 50% of humans.
• May be highly resistant to antibiotics.
• Transmitted by direct contact with a contaminated object, surface, solution, or hands.
• Studies have shown it can survive on inanimate objects for up to 16 months.
• In our organization, about 10% of our HAIs last year were with this organism.

Additional questions to consider, based on organism (examples)
A. What are potential sources of organism in this case? B. Based on answer to A., devise rest of questions, e.g.:
a. Given that P. aeruginosa is found in over 50% of humans normally and it’s an opportunistic pathogen, placing a Foley put Jerri at risk of getting infected as that compromised her host defenses. Did the need for the Foley outweigh the risk of catheter-related complications, such as this CAUTI? Why do we put Foleys in all THR patients?
b. Were there other sources of P. aeruginosa in Jerri’s environment we need to consider? Plants? Sink? How was bathing carried out? Are bath basins used? If so, how are they cleaned after/before use? Are sinks being used as a bath basin? How is room cleaning done? Any caregivers wearing long or artificial nails?
c. Could it have been transmitted from another patient via healthcare workers? From the patient in the room prior to Jerri’s being there?
C. Etc.

What have we learned?
• 72 yo Jerri experienced a symptomatic CAUTI 4 days after FC inserted from P. aeruginosa.
• FC inserted in the OR prior to surgery for THR per the circulating RN. • FC in for 3 days despite routine to remove it the day after surgery: kept in
per son’s request due to patient being in pain from surgery. • No alternatives to FC considered pre-op that are documented. • Assumed pt. met insertion criteria due to type of surgery. But why do we
put Foleys in all THR patients? What is the evidence to support that? • Securement device not placed in the OR. Found out it does not come in
Foley kits. • No documentation of RN competency for FC insertion. RN has nursed for
30+ years and has great experience placing urinary catheters in OR but how do we know she puts them in correctly?
What we’ve learned so far…continued
• Observed practice shows transporters are raising collection bag above level of bladder. Found they get no training in how to handle collection bags.
• Pt/family engagement about FC occurred only post-op when there was deviation. Found we do not have any patient-family education materials on pre-op topics for post-op review/reiteration.
• Transfer form includes only presence of FC, not date of insertion. • Hand hygiene compliance issues in OR and on unit. • Urine measurement containers are not labeled with patient name/
room #. • System for reminding MDs about FCs dependent on nurse being
present on rounds. • Pt. diabetic and BMI is 30.
Step 2: Why Did It Happen?
• Review events from event report with multidisciplinary team • Further research/lit review may be necessary to determine
why it happened and if there were any gaps with best practice. • Question all practices and compare to best practice defined in
the literature. Don’t be afraid to really challenge practice. • For each gap identified, ask “Why” five times or until the group
feels the root cause has been found. (Keep pushing to the 5 “Whys” to ensure root cause is determined and latent failures are recognized if present.)
• Identify and list all contributing factors. • Prioritize contributing factors.

The Five Whys – One Example
Gap: Foley remained in 2 days longer than protocol called for.
Why 1: Son requested: He felt it was too painful for her to get OOB Why 2: Son was not aware of pain management protocol nor need for pt. to be up and moving. Why 3: Son could not be w/his mother during pre-op visits and there is no patient education on this post-op. Why 4: No process in place to reinforce critical aspects of post-op care with patients and families. Why 5: We’ve assumed patients & families remember what they were taught pre-op.
Why 1: Surgeon agreed to keep Foley in. Why 2: Surgeon felt risk of developing pneumonia greater if pt. in pain and not coughing/deep breathing post-op compared to developing CAUTI. Why 3: Surgeon did not operate here often and was not familiar with our pain management protocols. Why 4: We don’t have processes to communicate new protocols effectively. Why 5: Such communication processes are not part of protocol development.

How to prioritize contributing factors – an example
Contributing Factors Importance to current event, 1 (low) to 5 (high)
Importance to future events 1 (low) to 5 (high)
Ease of Resolution 3 =easy, 2 = fairly easy 1=hard
Total Score
No process to reinforce pre-op education post-op with patients and families
5 5 2 12
Communication of new/revised protocols to MDs is not a formal step of protocol development/review.
5 5 1 11
Foley insertion criteria are not used with THR patients as community practice is to place a Foley in all of these patients, but w/o scientific evidence.
2 5 1 8
Daily review of Foley necessity is dependent upon nurses rounding with surgeons to remind them.
5 5 3 13
No process in place to assess RN competency for Foley insertion upon hire or periodically thereafter.
2 4 2 8
Step 3: How can we reduce the chances of it happening again?
1. Develop interventions (countermeasures) to defend against the most important contributing factors.
2. Then, rate each countermeasure on its ability to mitigate the root cause and on the team’s belief that the countermeasure will be executed.
3. Make an action plan for 2-5 of the highest scoring countermeasure.
• Must have many different perspectives. • Must engage leadership.

Countermeasures
• Consider safe design principles: • Standardize – eliminate steps when possible • Create independent checklists • Learn when things go wrong (analyze defects)
• Safe designs apply to technical and team work. • Brainstorm strategies and consider:
1. Ability to mitigate error. 2. Strength of countermeasures to prevent error. 3. Ease of implementation. (Resources and will necessary
to implement.)
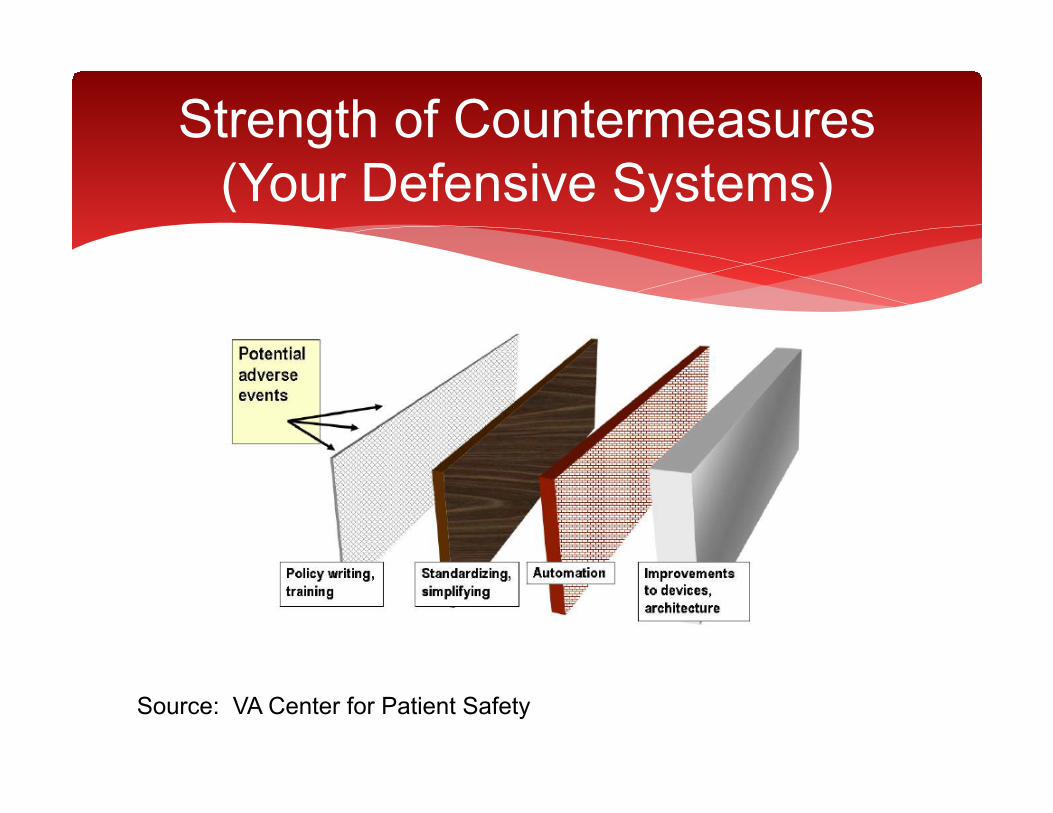
Strength of Countermeasures (Your Defensive Systems)
Source: VA Center for Patient Safety
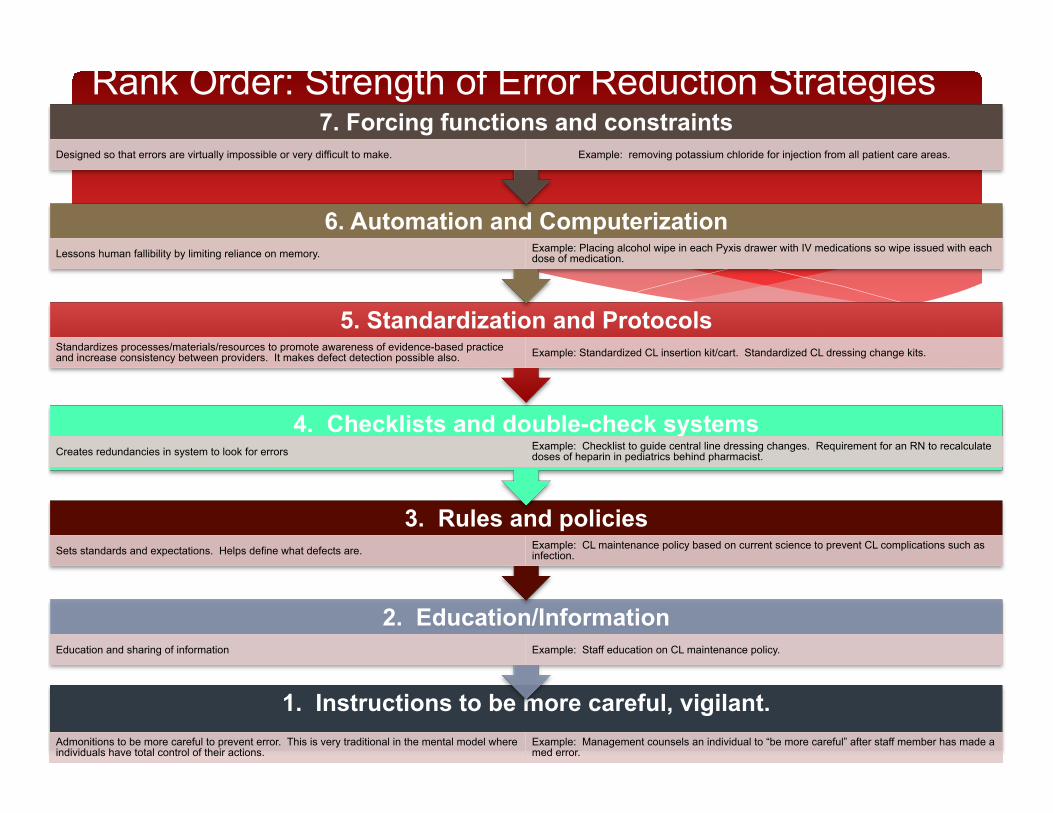
Rank Order: Strength of Error Reduction Strategies
1. Instructions to be more careful, vigilant. Admonitions to be more careful to prevent error. This is very traditional in the mental model where individuals have total control of their actions.
Example: Management counsels an individual to “be more careful” after staff member has made a med error.
2. Education/Information Education and sharing of information Example: Staff education on CL maintenance policy.
3. Rules and policies Sets standards and expectations. Helps define what defects are. Example: CL maintenance policy based on current science to prevent CL complications such as
infection.
4. Checklists and double-check systems Creates redundancies in system to look for errors Example: Checklist to guide central line dressing changes. Requirement for an RN to recalculate
doses of heparin in pediatrics behind pharmacist.
5. Standardization and Protocols Standardizes processes/materials/resources to promote awareness of evidence-based practice and increase consistency between providers. It makes defect detection possible also. Example: Standardized CL insertion kit/cart. Standardized CL dressing change kits.
6. Automation and Computerization Lessons human fallibility by limiting reliance on memory. Example: Placing alcohol wipe in each Pyxis drawer with IV medications so wipe issued with each
dose of medication.
7. Forcing functions and constraints Designed so that errors are virtually impossible or very difficult to make. Example: removing potassium chloride for injection from all patient care areas.

Countermeasures (interventions to reduce the risk of the defect) “Daily review of Foley necessity is dependent upon nurses rounding with surgeons to remind them.”
Ability to mitigate the contributing factor, 1 (low) to 5 (high)
Team believes the countermeasure will be implemented and executed, 1 (low) to 5 (high)
Strength of Strategy, 1 (low) to 7 (high)
Total Score
Develop medical protocol giving nursing the ability to remove the Foley when certain criteria are met. (Nurse-driven protocol for Foley removal)
4 2 5 11
Include patient and family in daily assessment for need.
3 5 4 12
Place a reminder sticker on front of patient’s chart
3 1 4 8
For all patients with a Foley in, create a pop-up reminder on MD’s CPOE screen.
3 1 6 10

Step 4: How will we know the risk is reduced?
• Assess outcome and process data (CAUTI rates, compliance to catheter maintenance protocols, monitoring of specific process changes, etc.)
• Talk to staff to get their perspectives. • Talk to patients/families to get their perspectives. • Do gemba walks for direct observation. • Feedback from patient safety rounds.

Step 5: How do we communicate our findings and to whom?
Internal communications • Other units • Quality committee • Risk Manager • Staff and physicians
External communications
• PSO • Collaboratives, CAUTI Campaign
Common Pitfalls in LfD
• A systematic, scientific approach is not used. • Only one person does the investigation. • The medical record is the only source of information of what happened
or may have happened. • Direct care providers that cared for the specific patient are not
involved. • Active errors are identified but no work to push “upstream” and find the
latent errors contributing to them. • Physicians and patients/families are often left out. • Team or individuals get caught in “analysis paralysis”. • Primary countermeasures stop at “re-educate” and admonishments to
providers to “Be more careful.” • Learning stops at the individual defect. • Information goes no further than the team involved.
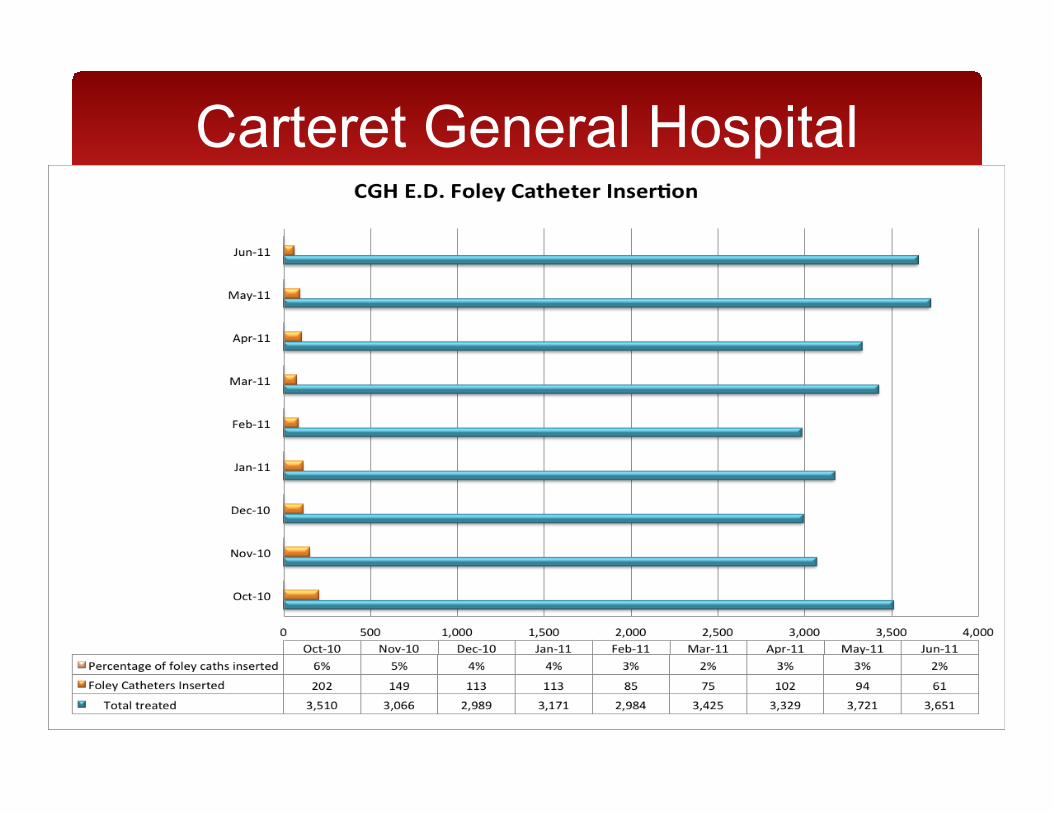
Carteret General Hospital

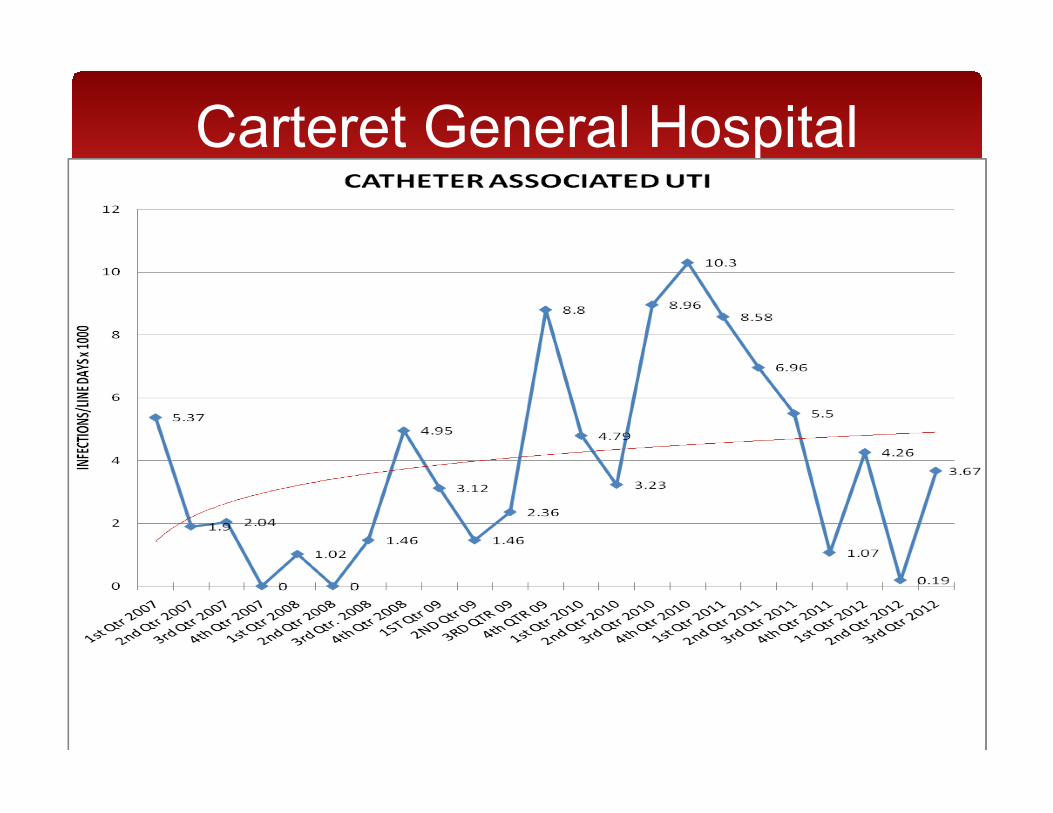
Carteret General Hospital
Carteret General Hospital
Your Charge
• Within the next two months, use the Event Investigation tool (or your own tool) to investigate a CAUTI or a defect that may lead to a CAUTI.
• Go through each of the five steps of defect analysis.
• Call Shelby or Jan if you have any questions, need to talk through anything, etc.
Resources
• http://www.ahrq.gov/cusptoolkit/ • http://www.ncqualitycenter.org/nocva/
campaigncauti.lasso • http://www.ncqualitycenter.org/resources.lasso
(CLABSI toolkit - Chapter 6 – Hygiene) • NC Participants: Shelby Lassiter –
[email protected] • VA Participants: Jan Mangun – [email protected]