Embed Size (px)
Citation preview

NON-CORONARY ARTERIAL DISEASE
D P Mikhailidis BSc MSc MD FCPP FCP FFPM FRCP FRCPath
Dept. of Clinical Biochemistry Royal Free Hospital campus University College London

DECLARATION OF INTEREST
• Attended conferences and gave talks sponsored by MSD, Libytec and Astra Zeneca

DECLARATION OF INTEREST
Editor-in-Chief of: • Curr Med Res Opin• Expert Opin Pharmacother• Angiology• Curr Vasc Pharmacol • Open Cardiovasc Med J • Expert Rev Cardiovasc Ther• Clinical Lipidology• Journal of Drug Assessment

DECLARATION OF INTEREST
• Lead: Guidelines for Medical Management of Carotid Artery Stenosis (Eur Soc Vasc Surg)
• Chair: Expert Panel on Small Dense Low Density Lipoprotein• Co-chair: Expert Panel on Post-Prandial Hypertriglyceridaemia• Executive Board member: International Atherosclerosis Society
(IAS), 2016-18

CHD EQUIVALENTS
• *Diabetes• *Peripheral arterial disease• Symptomatic carotid disease• *Abdominal aortic aneurysm• *Chronic kidney disease (eGFR <60 ml/min/1.73m2
• Rheumatoid arthritis (?psoriasis + arthritis, SLE)

Common Types of Non-Cardiac Vascular Disease
• Abdominal Aortic Aneurysms (AAA)
• Peripheral Arterial Disease (PAD)
• Carotid Artery Disease
• Atherosclerotic Renal Artery Disease (ARAS)

NON-CARDIAC VASCULAR DISEASE
• PLATELETS • LIPIDS•HYPERTENSION • SMOKING•DIABETES

PERIPHERAL ARTERIAL DISEASE

PAD and the risk of vascular events, death and amputation
Ouriel K. Lancet 2001; 358: 1257-64
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
Time (years)
Patie
nts
(%)
Survival
Myocardial Infarction InterventionAmputation
Causes of death: • 55% coronary artery disease• 10% cerebrovascular disease• 25% non-vascular• < 10% other vascular

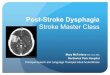
Risk of death in PAD
*Kaplan-Meier survival curves based on mortality from all causes. Large-vessel PAD
Normal subjects
Asymptomatic PAD†
Symptomatic PAD†
Severe symptomatic PAD†
100
75
50
25
00 2 4 6 8 10 12
Sur
viva
l (%
of p
atie
nts)
Year
Criqui MH et al. N Engl J Med 1992; 326: 381-86

PAD and high risk of MI and strokeIncreased risk of MI* Increased risk of stroke*
PAD
Post-MI
Post-stroke
4 ´greater risk4
(includes only fatal MI and other CHD death)
5-7 ´greater risk1
(includes death)
2-3 ´greater risk2
(includes anginaand sudden death†)
2-3 ´greater risk3
(includes TIA)
3-4 ´greater risk2
(includes TIA)
9 ´greater risk3
* Over 10 years vs the general population except for stroke following stroke which measures subsequent risk per year
† Sudden death defined as death documented within 1 h and attributed to CHD.
1. Adult Treatment Panel II. Circulation 1994; 89: 1333-14352. Kannel WB. J Cardiovasc Risk 1994; 1: 333-3393. Wilterdink JI, Easton JD. Arch Neurol 1992; 49: 857-8634. Criqui MH et al. N Engl J Med 1992; 326: 381-386

WHY BOTHER WITH LIPIDS IN PAD?
HIGH RISK PATIENTS (MI,CVA,ARAS)
• Improving symptoms• Decreasing the risk of events• Preventing PAD?

Heart Protection Study
Patient Population:20,536 patients
CHD(n=13,379)
Peripheral or
CerebrovascularDisease(n=10,036)
Diabetes Mellitus(n=5,963)
TreatedHypertension
(n=8,455)

SIMVASTATIN 40 mg: VASCULAR EVENT by PRIOR DISEASE
Risk ratio and 95% CISIMVASTATIN PLACEBOBaselinefeature (10269) (10267) STATIN better STATIN worse
STATIN worse
Previous MI 1007 1255
Other CHD (not MI) 452 597
No prior CHD
CVD 182 215
PVD 332 427Diabetes 279 369
ALL PATIENTS 2042 2606(19.9%) (25.4%)
24%SE 2.6reduction(2P<0.00001)
0.4 0.6 0.8 1.0 1.2 1.4

SIMVASTATIN 40 mg:STROKE by AETIOLOGY
Risk ratio and 95% CISTATIN PLACEBOStroke
aetiology (10269) (10267) STATIN better STATIN worse
Ischaemic 242 376Haemorrhagic 45 53Subarachnoid 12 10Unknown 69 100Unadjudicated 136 146
ALL STROKE 456 613(4.4%) (6.0%)
27% SE 5.3reduction(2P<0.00001)
0.4 0.6 0.8 1.0 1.2 1.4

Transient Ischaemic Attacks (TIA)
• 204 vs 250 (p = 0.02)
TIAs are ischaemic events that predict an increased risk of stroke.

Non-Coronary revascularization
450 vs 532 (p= 0.006)
• Carotid endarterectomy/angioplasty:
42 vs 82 (p= 0.0003)*
* included in non-coronary revasc.

0 1 2 3 4 5 6
INTERMITTENT CLAUDICATION*
*A post-hoc analysis of 4SAdapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
New or Worsening Intermittent Claudication
38%risk reduction
P=0.008
4.54.03.53.02.52.01.51.00.5
0
%of
patie
nts
Simvastatin
Placebo
Years

MM McDermott et al. Circulation 2003;107:757
• Superior leg functioning after statin• Independent of cholesterol
lowering

LIMB SALVAGE• Patients were selected from 2007 - 2008 Medicare claims with claudication
(n = 8128), rest pain (n = 3056), ulceration/gangrene (n = 11,770), endovascular revascularization (n = 14,353) and open surgery (n = 8601).
• Half (n = 11,687) were statin users before revascularization. Statin users compared with non-users had lower amputation rates at 30 days (11.5 vs14.4%; p < 0.0001), 90 days (15.5 vs 19.3%; p < 0.0001) and 1 year (20.9 vs25.6%; p < 0.0001).
• Survival analysis: improved limb salvage during 1 year for statin users vsnon-users for the diagnosis of claudication (p = 0.003), a similar trend for rest pain (p = 0.061) and no improvement for ulceration/gangrene (p = 0.65).
Vogel TR, et al. Circ Cardiovasc Interv 2013; 6: 694 - 700

LIMB SALVAGE AND EVENTS
• After propensity weighting, statin therapy was associated with lower 1 year rates of MACCE (stroke, MI or death; HR: 0.53; 95% CI: 0.28 to 0.99), mortality (HR: 0.49, 95% CI: 0.24 to 0.97) and major amputation or death (HR: 0.53, 95% CI: 0.35 to 0.98).
• Statin use was also associated with improved lesion patency among patients undergoing infrapopliteal angioplasty.
• Patients with LDL-C >130 mg/dl (3.4. mmol/l) had increased HRs ofMACCE and mortality vs those with lower LDL-C levels.
Westin GG, et al. J Am Coll Cardiol 2014; 63: 682 - 90

LIMB SALVAGE AND EVENTS
• A total of 5861 patients with symptomatic PAD were included. • Statin use at baseline was 62.2%.
• Patients on statins had a significantly lower risk of the primary adverse limb outcome at 4 years vs those not taking statins [22.0 vs 26.2%; HR, 0.82; 95% CI, 0.72 - 0.92; p = 0.0013].
• The composite of CV death/MI/stroke was similarly reduced (HR, 0.83; 95% CI, 0.73 - 0.96; p = 0.01).
Kumbhani DJ, et al.; REACH Registry Investigators. Eur Heart J 2014; 35: 2864 - 72

LIMB SALVAGE AND EVENTS
• Vascular Study Group of New England registry: 2067 patients (71% male; mean age, 67 ± 11 years; 67% with critical limb ischemia [CLI]) who underwent infrainguinal bypass from 2003 to 2011.
• Of these, 1537 (74%) were on statins perioperatively and at 1 year follow-up 530 received no statin.
• Crude, adjusted, and propensity-matched rates of 5 year surviva1, 1 year amputation, graft occlusion and perioperative MI.
Suckow BD, et al; Vascular Study Group of New England. Statin therapy after infrainguinal bypass surgery for critical limb ischemia is associated with improved 5-year survival. J Vasc Surg 2015; 61: 126 - 33

LIMB SALVAGE AND EVENTS
• Patients taking statins at the time of surgery and at the 1 year follow-up were more likely to have CHD (38 vs 22%; p < .001), DM (51 vs 36%; p < .001), hypertension (89 vs 77%; p < .001) and prior revascularization (50 vs38%; p < .001).
• Despite higher comorbidity burdens, long-term survival was better for those taking statins: crude (RR 0.7; p < .001) and adjusted (HR 0.7; p = .001).
• Subgroup analysis: survival advantage was evident in patients on statins with CLI (5 year survival, 63 vs 54%; log-rank, p = .01) but not claudication (5 year survival, 84 vs 80%; log-rank, p = .59).
• Statin therapy was not associated with 1-year rates of major amputation (12 vs 11%; p = .84) or graft occlusion (20 vs 18%; p = .58) in CLI patients.
• Perioperative MI occurred more frequently in patients on a statin in crude analysis (RR, 2.2; p = .01) but not in the matched cohort (RR, 1.9; p = .17).
Suckow BD, et al; Vascular Study Group of New England. J Vasc Surg 2015; 61: 126 - 33

LIMB SALVAGE AND EVENTS
• 12 observational cohort studies and 2 randomised trials: 19,368 PAD patients. Meta-analysis.
• Statin therapy was associated with reduced all-cause mortality (OR 0.60, 95% CI 0.46 - 0.78) and incidence of stroke (OR 0.77, 95% CI 0.67 - 0.89).
• A trend towards improved CV mortality (OR 0.62, 95% CI 0.35 - 1.11), MI (OR 0.62, 95% CI 0.38 - 1.01) and the composite of death/MI/stroke (OR 0.91, 95% CI 0.81 - 1.03) was identified.
• Meta-analyses of studies performing adjustments showed decreased all-cause mortality in statin users (HR 0.77, 95% CI 0.68 - 0.86).
Antoniou GA, et al. Statin therapy in lower limb peripheral arterial disease: Systematic review and meta-analysis. Vascul Pharmacol 2014; 63: 79 - 87

STATINS, PAD AND EVENTS• In the Incremental Decrease in End Points Through Aggressive Lipid
Lowering (IDEAL) trial, 8888 MI patients were randomised to high-dose or usual-dose statin therapy (atorvastatin 80 vs simvastatin 20-40 mg/day).
• During a median follow-up of 4.8 years, 94 patients (2.2%) receiving atorvastatin and 135 patients (3.2%) receiving simvastatin developed PAD (HR = 0.70, 95% CI 0.53 - 0.91; p = 0.007).
• In PAD patients, major coronary events occurred in fewer patients in the atorvastatin group (14.4%) than in the simvastatin group (20.1%), but the difference did not reach significance (HR = 0.68, 95% CI 0.41 - 1.11; p = 0.13).
• Atorvastatin treatment significantly reduced overall CV (p = 0.046) and coronary events (p=0.004) and coronary revascularisation (p = 0.007) in these patients.
Stoekenbroek RM, et al.; Incremental Decrease in End Points Through Aggressive Lipid Lowering Study Group. High-dose atorvastatin is superior to moderate-dose simvastatin in preventing peripheral arterial disease. Heart2015; 101: 356 - 62

STATINS, PAD AND EVENTS• O'Donnell TFX, et al. J Vasc Surg 2017; 66: 572 - 8
• Use of the recommended intensity of statin therapy in compliance with 2013 American College of Cardiology/American Heart Association lipid management guidelines is associated with significantly improved survival and lower major adverse limb (1019 limbs from 931 patients with a median follow-up of 380 days) event (MALE) rate in patients undergoing revascularization for chronic limb-threatening ischemia.
• In multivariable analysis, discharge on any statin was associated with lower mortality (hazard ratio [HR], 0.71; 95% CI, 0.60-0.90; p < 0.01).
• Patients >75 years old and ≤75 years old accrued similar benefit.

• Above-knee amputations (AKAs) and below-knee amputations (BKAs) are associated with high postoperative mortality rates. 811 patients underwent AKA (n = 325) or BKA (n = 486).
• In the year after amputation, medium-intensity statin (HR, 0.64; 95% CI, 0.47 - 0.87) and high-intensity statin (HR, 0.56; 95% CI, 0.33 - 0.95) conferred a mortality benefit. Low-intensity statins did not confer protection from mortality.
• At 1 year after amputation, only 44.7% of patients were receiving appropriate statin therapy.
DeCarlo C, et al. J Vasc Surg 2017; 66: 216 - 25

• Nationwide Taiwan DM database in from 2000 - 2011.
• 69,332 patients aged ≥20 years with DM and PAD.
• Only statin users were associated with the risk reduction of lower-extremities amputation (HR, 0.77; 95% CI, 0.61 - 0.97) and CV death (HR, 0.78; 95% CI, 0.68 - 0.89) when taking competing risk of death into consideration.
Hsu CY, et al. J Clin Endocrinol Metab 2017; 102: 2373 - 81

• Patients (n=3,642) had PAD (1,505 with no prior MI or stroke) in the FOURIER trial.
• Evolocumab significantly reduced the primary end point in patients with PAD (HR 0.79; 95% CI, 0.66 -0.94; p = 0.0098) and without PAD (HR 0.86; 95%CI, 0.80 - 0.93; p = 0.0003; Pinteraction = 0.40).
• Evolocumab reduced the risk of major adverse limb events in all patients (HR, 0.58; 95% CI, 0.38 - 0.88; p = 0.0093) with consistent effects in those with and without known PAD.
Bonaca MP, et al. Circulation 2018; 137: 338 - 50

Ezetimibe and evolocumabBonaca MP, et al. Polyvascular disease, type 2 diabetes, and long-term vascular risk: a secondary analysis of the IMPROVE-IT trial. Lancet Diabetes Endocrinol 2018; 6 :934-43Eze + simva better than simva monotherapyPAD or DM more risk than those without PAD or DM PAD + DM more risk (and more benefit) than either alone

Useful reviews and meta-analysis• Katsiki N, Giannoukas AD, Athyros VG, Mikhailidis DP. Lipid-lowering
treatment in peripheral artery disease. Curr Opin Pharmacol 2018; 39: 19 - 26
• Katsiki N, Triposkiadis F, Giannoukas AD, Mikhailidis DP. Statin loading in cardiovascular surgery: never too early to treat. Curr Opin Cardiol2018; 33: 436 – 43
• Arya S, et al. Association of Statin Dose With Amputation and Survival in Patients With Peripheral Artery Disease. Circulation 2018; 137: 1435 - 46
Statins, especially high-intensity formulations, are underused in PAD. High-intensity statin use at PAD diagnosis = a significant reduction in limb loss and mortality compared with low-to-moderate-intensity statin users, and patients treated only with antiplatelet medications but not with statins, as well.

CAROTID ARTERY DISEASE

CAROTID STENOSIS AND MORTALITY
• Asymptomatic carotid stenosis (ACS) > 50%
• 17 studies reporting 5-year all-cause mortality in 11,391 patients with ACS
• Of the 930 deaths, 589 (62.9%; 95% CI 58.81-66.89) were cardiac-related. Average cardiac-related mortality of 2.9% per year
• All-cause and cardiac mortality in ACS patients are very high
• Giannopoulos A et al. Eur J Vasc Endovasc Surg 2015 Aug 20. pii: S1078-5884(15)00545-6. [Epub ahead of print]

High-Dose Atorvastatin after Stroke or Transient Ischemic Attack
The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators
N Engl J Med 2006; 355: 549-59

Kaplan-Meier Curves for Stroke and TIA
SPARCL. N Engl J Med 2006;355:549-59

Kaplan-Meier Curves for Coronary and Cardiovascular Events
SPARCL. N Engl J Med 2006;355:549-59

RISK FACTOR ANALYSIS IN SPARCL
• Optimal control: LDL-C <70 mg/dl, HDL-C >50 mg/dl, TG <150 mg/dl and SBP/DBP <120/80 mmHg.
• Risk of stroke decreased as control increased (HR [95% CI] 0.98 [0.76 to 1.27], 0.78 [0.61 to 0.99], 0.62[0.46 to 0.84], and 0.35 [0.13 to 0.96]) for those achieving control of 1, 2, 3, or 4 factors as compared with none, respectively.
Amarenco P et al. Stroke 2009; 40: 2486 - 92

STATINS AND OPERATIVE CARDIAC MORTALITY
• Decreased operative mortality associated with general and vascular surgery
• Benefit evident even after short-term use of statins
Paraskevas KI, Liapis CD, Hamilton G, Mikhailidis DP. Eur J VascEndovasc Surg 2006;32:286 - 93 Paraskevas KI, Veith FJ, Liapis CD, Mikhailidis DP. Curr Vasc Pharmacol2013;11:112 - 20

STATINS AND OPERATIVE CARDIAC MORTALITY
• Pre-interventional use of statins has a protective effect against peri-interventional stroke, MI, or death in patients with internal carotid artery stenosis treated with stent-angioplasty (n = 344)
• Reiff T, et al. Eur J Vasc Endovasc Surg 2014;48:626 - 32
• Pre-interventional use of statins not only reduce cardiovascular events and mortality but may also have an important effect on the anatomic durability of CEA.
• Avgerinos ED, et al. Curr Vasc Pharmacol 2015;13:239 - 47

Statin pre-treatment
• TIA + carotid patients, nonprocedural 7-day stroke risk was 3.8% (CI, 1.2 - 9.7%) with statin treatment at TIA onset, compared with 13.2% (CI, 8.5 - 19.8%) in those not statin pre-treated (p = 0.01; 90-day risks 8.9 vs 20.8% [p = 0.01]).
• Statin pre-treatment was associated with reduced stroke risk in patients with carotid stenosis (OR for 90-day stroke, 0.37; CI, 0.17 - 0.82) but not non-stenosis patients (OR, 1.3; CI, 0.8 - 2.24; p for interaction, 0.008).
• Multivariable logistic regression: the association remained.
• Merwick A, et al. Stroke 2013; 44: 2814 - 20

Statin pre-treatment• 156 patients randomized to 600 mg (n = 78) or 300 mg (n = 78)
clopidogrel load 6 h before intervention and either atorvastatin reload (n = 76; 80 and 40 mg, 12 h and 2 h before the procedure, respectively) or no statin reload (n = 80).
• Primary endpoint: 30-day incidence of TIA/stroke or new ischemic lesions on cerebral diffusion-weighted MRI at 24 to 48 h.
• Patients were already on a statin at randomisation. • The primary outcome was significantly lower in the 600 mg
clopidogrel arm (18 vs 35.9% in the 300 mg group; p = 0.019) and in the atorvastatin reload arm (18.4 vs 35.0% in the no statin reload group; p = 0.031).
• High-dose clopidogrel also significantly reduced the TIA/stroke rate at 30 days (0 vs 9%, p = 0.02,) without increased bleeding risk.
Patti G et al. J Am Coll Cardiol 2013; 61: 1379 - 87•

INTENSIVE LDL-C LOWERING
• The combination of atorvastatin + ezetimibe canfurther decrease LDL-C and hsCRP levels and haveeffects on the progression of carotid atherosclerosisin elderly patients with hypercholesterolemiacompared with atorvastatin monotherapy
Luo P, et al. Genet Mol Res 2014;13:2377 - 84• Comment in• Genet Mol Res 2014;13:4805 - 7

LIPIDS AND CAROTID STENTING (CAS)
• 127 patients without preprocedural statin treatment and 53 patients with preprocedural statin treatment.
•• Preprocedural statin therapy appears to reduce the
incidence of stroke, myocardial infarction, and death within 30 days after CAS.
Groschel K, et al. Radiology 2006;240:145-51

Carotid Stenting and Statins
• Consecutive series of 397 symptomatic carotid artery stenosis (≥50% stenosis on angiography) treated with stenting.
•• Statin pretreatment divided into 3 categories according to
atorvastatin dose: none (n = 158; 39.8%), standard dose (<40 mg, n = 155; 39.0%) and high dose (≥40 mg; n = 84; 21.2%).
• Peri-procedural complication rates across the 3 categories of statin use were 12.0, 4.5 and 1.2%. After adjustment, p for trend = 0.01.
Hong JH, et al. Stroke 2017; 48: 1890 - 4

LIPIDS, CAROTID ENDARTERECTOMY AND ANATOMICAL DURABILITY
LIPID LOWERING DRUGS, protective for:
• Early restenosis: OR = 0.601 (p< 0.007)• Early and late anatomical failure: OR = 0.517
(p< 0.03) and 0.128 (p< 0.0003) • Progression of disease: OR = 0.202 (p<
0.0002)
LaMuraglia GM et al. J Vasc Surg 2005; 41: 762-8

LIPID LOWERING TREATMENT AND CAROTID PLAQUE COMPOSITION
• Less lipid content (p <0.05)• Less oxidized LDL immunoreactivity (p <0.001)• Fewer macrophages (p <0.05)• Fewer T cells (p <0.05)• Less matrix metalloproteinase 2 immunoreactivity (p
<0.05)• Greater tissue inhibitor of metalloproteinase 1(TIMP
1) immunoreactivity (p <0.05)• Higher collagen content (p <0.005)
M Crisby et al. Circulation 2001; 103: 926-33

STATINS AND CAROTID PLAQUE COMPOSITION
• 240 symptomatic plaques (previous 10 days) were divided into 3 groups: 80 in group A (atorvastatin 80 mg), 80 in group B (atorvastatin 40 mg) and 80 to group C (no atorvastatin)
• Gray-scale median (GSM) score increased significantly more (at 12 months) in group A than in group B (48.65 vs 39.46, p < .02) and group C (48.65 vs 19.3, p = .0002)
• An inverse association between reduction of LDL-C and the increase in the GSM score (r = -.456, p = .007) was observed
• The reduction in hsCRP correlated inversely with the increase in GSM (r = -.398, p = .021)
Marchione P et al. J Stroke Cerebrovasc Dis 2015;24:138-43

Study suggests statin therapy is associated with significant reductions in in lipid-rich-necrotic-core (LRNC) volumes at 1-year of statin therapy on serial carotid MRI.
However, no significant reduction in carotid wall volume was seen.
Brinjikji W, et al. J Neuroradiol 2017; 44: 234 - 40

Konishi T, et al. Stabilization of symptomatic carotidatherosclerotic plaques by statins: a clinico-pathological analysis.Heart Vessels 2018; 33: 1311 - 24
Plaques harvested from patients undergoing CEA suggests thatstatin therapy mitigates the plaque instability, which, in patientspresenting with strokes, might decrease cerebral infarct volume.

INTENSIVE LDL-C LOWERING
Intensive lipid-lowering therapy reduced progression of cIMT in high-risk Japanese patients.
Yokoi H et al. Int Heart J 2014;55:146 - 52

Bos S, Duvekot MH, Ten Kate GR, Verhoeven AJ, Mulder MT, Schinkel AF, Nieman K, Watts GF, Sijbrands EJ, Roeters van Lennep JE. Carotid artery plaques and intima medial thickness in familial hypercholesteraemic patients on long-term statin therapy: A case control study. Atherosclerosis 2017; 256: 62 - 6
Braamskamp MJAM, Langslet G, McCrindle BW, Cassiman D, Francis GA, Gagne C, Gaudet D, Morrison KM, Wiegman A, Turner T, Miller E, Kusters DM, Raichlen JS, Martin PD, Stein EA, Kastelein JJP, Hutten BA. Effect of Rosuvastatin on Carotid Intima-Media Thickness in Children With Heterozygous Familial Hypercholesterolemia: The CHARON Study (Hypercholesterolemia in Children and Adolescents Taking Rosuvastatin Open Label). Circulation 2017; 136: 359 - 66
Statin treatment in patients with FH reversed some carotid changes

ESVS GUIDELINES
Liapis CD, Bell PF, Mikhailidis DP, Sivenius J, Nicolaides A, Fernandes e Fernandes J, Biasi G, Norgren L; ESVS Guidelines Collaborators; European Society for Vascular Surgery. ESVS Guidelines: Section A--prevention in patients with carotid stenosis. Curr Vasc Pharmacol 2010;8:673-81
Liapis CD, Bell PF, Mikhailidis DP, Sivenius J, Nicolaides A, Fernandes e Fernandes J, Biasi G, Norgren L; ESVS Guidlines Collaborators; European Society for Vascular Surgery. ESVS Guidelines: Section B - diagnosis and investigation of patients with carotid stenosis. Curr Vasc Pharmacol 2010;8:682-91
Liapis CD, Bell PR, Mikhailidis D, Sivenius J, Nicolaides A, Fernandes e Fernandes J, Biasi G, Norgren L; ESVS Guidelines Collaborators. ESVS guidelines. Invasive treatment for carotid stenosis: indications, techniques. Eur J Vasc Endovasc Surg 2009;37(4 Suppl):1-19

CAROTID BRUITSAuscultation for carotid bruits in patients atrisk for heart disease could help select those who might benefit the most from an aggressive modification strategy for cardiovascular risk.
Paraskevas KI, et al. Neurol Res 2008;30:523-30Pickett CA et al. Lancet 2008; 371: 1587-94

STROKE PREDICTORS
• Age• BP• Peripheral Arterial Disease
Evidence that lipids also predict stroke

Colussi G, et al. Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study. J Clin Med 2018;7. pii: E286Survival analysis showed that statin use reduced risk of death (hazard ratio HR 0.36, 95%CI 0.23-0.58, p<0.0001).
Texakalidis P, et al. Preoperative Use of Statins in Carotid Artery Stenting: A Systematic Review and Meta-analysis. J Endovasc Ther 2018; 25: 624 - 31 Texakalidis P, et al. Outcome of Carotid Artery Endarterectomy in Statin Users versus Statin-Naïve Patients: A Systematic Review and Meta-Analysis. World Neurosurg 2018; 116: 444 - 50.e1. Ironside N, et al. Systematic review and meta-analysis of perioperative and long-term outcomes in patients receiving statin therapy before carotid endarterectomy. Acta Neurochir (Wien) 2018; 160: 1761 - 71. Statin therapy prior to CAS is associated with decreased risk of perioperative stroke and death without any effect on the rates of transient ischemic attack or myocardial infarction.

Rizwan M, et al. Statins reduce mortality and failure to rescue after carotid artery stenting. J Vasc Surg 2019; 69: 112 - 9. Statin use is associated with significant reduction in mortality and failure to rescue in patients who develop major complications (stroke/MI) after CAS.
Hussain MA, et al. Association Between Statin Use and Cardiovascular Events After Carotid Artery Revascularization. J Am Heart Assoc 2018; 7: e009745Continuous statin therapy was associated with a 25% lower risk of long-term adverse CV events in patients with significant carotid disease.

Good reviews
• Naylor AR. Medical treatment strategies to reduce perioperative morbidity and mortality after carotid surgery. Semin Vasc Surg 2017; 30: 17 - 24
• Cheng SF, Brown MM. Contemporary medical therapies of atherosclerotic carotid artery disease. Semin Vasc Surg 2017; 30: 8 - 16

ABDOMINAL AORTIC ANEURYSMS

STATINS AND AAA EXPANSION IN HUMANS
Second Manifestation of ARTerial disease (SMART) studyPatients using lipid-lowering drugs had a 1.2 mm/y (95% CI -2.34 to -0.060) lower AAAgrowth rate than nonusers.86 lipid lowering and 144 controls. Median follow up = 3.3 years.
Schlosser FJ, et al. J Vasc Surg 2008;47:1127-33

HOW COULD STATINS HELP PATIENTS WITH AAA?
• Less inflammationKajimoto K et al. Atherosclerosis 2009; 206: 505-11• Animal modelsAtorvastatin decreased AAA diameter (MMP-12, ICAM) independently of lipid levels. Early action (1 week)

SOCIETY FOR VASCULAR SURGERY
Statins may be considered to reduce the risk of AAA growth.
Level of recommendation: WeakQuality of evidence: Low
Chaikof EL, et al.; Society for Vascular Surgery. The care of patients with an abdominal aortic aneurysm: the Society for Vascular Surgery practice guidelines. J Vasc Surg 2009;50(4 Suppl):S2-49

The main determinants of survival following AAA repair are pre-existing risk factors.
Meta-analysis: 24 studies (53,118 patients) published between1989 and 2015, were included.
Statins improved survival following (≥ 1 year) open repair with a hazard ratio and 95% CI of 0.75 (0.70 - 0.80).
Khashram M, et al. Ann Vasc Surg 2017; 39: 301 - 11

• Single centre, retrospective cohort study; 640 patients with AAA treated by open surgery.
• Stratified analysis using the Mantel-Haenszel method on quintiles of the propensity score: adjusted odds ratio = 0.43 (95% CI: 0.18 - 0.96); 57% reduction of 30-day mortality for statin users.
• The adjusted rate ratio was 0.62 (95% CI: 0.45-0.83); a reduction of long-term mortality of 38% for statin users compared with non-users for a median follow-up of 3.93 years.
Mathisen SR, Abdelnoor M. Vasc Med 2017; 22: 406 - 10

Alshaikh HN, et al. Statin intensity and postoperative mortality following open repair of intact abdominal aortic aneurysm. BJS Open 2018; 2: 411 - 8 Statin use is associated with lower odds of death in hospital following open AAA repair.
Salata K, et al. Statins Reduce Abdominal Aortic Aneurysm Growth, Rupture, and Perioperative Mortality: A Systematic Review and Meta-Analysis. J Am Heart Assoc 2018; 7: e008657 Statin therapy may be associated with reduction in AAA progression, rupture, and lower rates of perioperative mortality following elective AAA repair.
Huang Q, et al. Effect of Statin Therapy on Survival After Abdominal Aortic Aneurysm Repair: A Systematic Review and Meta-analysis. World J Surg 2018; 42: 3443 - 50Statin therapy has beneficial effects on survival after AAA repair and statins should be recommended to patients who will receive open or endovascular AAA repair. However, these findings mainly relied on data from cohort studies, and the high-quality studies are needed.

DIABETES• Diabetes does not predict AAA risk!!• Diabetes may actually decrease the risk of
developing an AAA!!• Diabetes may actually decrease the rate of
AAA expansion!!

ATHEROSCLEROTIC RENAL ARTERY DISEASE
(ARAS)

ARAS• Features:BP difficult to control, PAD, flash pulmonary oedema, femoral bruits and low eGFR
• Risk (or associated) factors:Lipids, hypertension, CHD, PAD
• Treatment:Open surgery, endovascular (stenting) and best medical therapy

Renal Function and PAD
• ARAS• Renal atherosclerosis• Diabetes• Cholesterol emboli

PAD AND RENAL FUNCTION
Evidence for improvement of impaired renal function with statins in PAD.
Youssef F, Gupta P, Mikhailidis DP, Hamilton G. Angiology 2005;56: 279 - 87
Youssef F, Gupta P, Seifalian AM, Myint F, Mikhailidis DP, Hamilton G. Angiology 2004; 55: 53 - 62

CONCLUSIONS
• Patients presenting to vascular surgeons are less aggressively treated, in terms of prevention measures, than patients with CHD presenting to cardiology departments
• Aggressive risk factor management may improve prognosis as well as symptoms in this high risk population

Are statins useful in the elderly?
The answer is a definite maybe?
But why are we uncertain?
Toth PP. Treatment of Dyslipidemia in Elderly Patients With Coronary Heart Disease: There Are Miles to Go Before We Sleep. J Am Coll Cardiol 2015 27; 66: 1873 - 5

Are statins useful in the elderly? • The elderly die of many causes (high comorbidity) – so we need to separate causes
of death• Those who have subclinical problems may also have a low cholesterol• Vascular lesions may be too advanced to respond to statins• Heart failure is very common in the elderly and may not respond effectively to
statins• There are very few statin trials specifically focussed on the elderly• Is treatment “to target” or are prescribers using lower doses in the elderly?• Statin-associated new onset diabetes (NOD) may be more common and play a
bigger role in the elderly. Some loss of efficiency?• Adherence to treatment may be lower in the elderly (e.g. cognitive ability, cost and
polypharmacy)• Some evidence comes from heterogeneous populations (e.g. primary or secondary
prevention). • Menopause = increased risk• Who are the elderly? > 65, >70 or >75 years old? [PROSPER 70-82 years]

STROKE PREDICTORS
• Age (90% of strokes above the age of 65 years)
• BP• Peripheral Arterial Disease
Evidence that lipids also predict stroke

PROSPER• Pravastatin 40 mg vs placebo: weak and rarely
used statin• Age 70 - 82 years: common definition for
elderly is >65 years• Baseline cholesterol from 4.0 to 9.0 mmol/l:
heterogeneity• Follow-up = 3.2 years: short• Mixed population (n = 5804; vascular disease
+/-): heterogeneity
Shepherd J, et al. Lancet 2002; 360: 1623 - 30

PROSPER• CHD death or non-fatal MI or fatal or non-
fatal stroke HR 0.85 (p = 0.014): small effect• Fatal or non-fatal stroke: 131 vs 135: NS and
more with pravastatin!• Non vascular deaths greater by about 1% than
vascular deaths. Common problem with elderly populations
• Cancer 58 vs 65, p = 0.02: significantly more with pravastatin!
Shepherd J, et al. Lancet 2002; 360: 1623 - 30

OTHER TRIALS
• Mostly not randomised surveys, or subgroup/post hoc analyses of trials (e.g. CARDS, JUPITER, HPS, AFCAPS/TexCAPS, ASCOT-LLA, 4S).
Pedro-Botet J et al. Statins for primary cardiovascular prevention in the elderly. J Geriatr Cardiol 2015; 12: 431 - 8

2016 Joint European Society of Cardiology Guidelines
• No differences in the relative reduction between men and women and between younger and older age or between those with and without DM.
Piepoli MF et al. Euro Heart J doi:10.1093/eurheartj/ehw106
No differences in the relative reduction between younger and older age (n = 134,537)Cholesterol Treatment Trialists' (CTT) Collaborators. Lancet2012; 380: 581 - 90

• Aged 80 and older (mean 85.2) hospitalized from Jan 2006 to Dec 2010 with AMI, unstable angina pectoris, or chronic CAD and discharged alive (n = 1,262); n = 913 received and 349 did not receive a discharge prescription for a statin.
• Median follow-up: 3.1 years.
• After adjusting for baseline differences between groups and propensity for receiving statin therapy, the effect of statins on mortality was not significant (HR = 0.88, 95%CI = 0.74-1.05).
• Confounders: more effective vascular prevention treatment in statin group. Adherence? Co morbidity? Overall mortality.
Rothschild DP, et al. J Am Geriatr Soc 2016 Jun 13. doi: 10.1111/jgs.14207 •

• 68 094 ≥60 years from the general population
• Inverse association between all-cause mortality and LDL-C was seen in 16 cohorts (in 14 with statistical significance) representing 92% of the number of participants, where this association was recorded. In the rest, no association found
• In two cohorts, CV mortality was highest in the lowest LDL-C quartile and with statistical significance; in 7 cohorts, no association was found
• Heterogeneous studies• Association is not proof of causation
• Ravnskov U, et al. BMJ Open 2016;6:e010401

• Randomized trials comparing statins vs placebo in subjects (age ≥ 65 years) without established CVD
• 8 trials enrolling 24,674 subjects (mean age: 73.0 ± 2.9 years; mean follow up 3.5 ± 1.5 years)
• Significantly reduced risk of MI by 39.4% (RR: 0.61 [95% CI: 0.43 to 0.85]; p = 0.003) and risk of stroke by 23.8% (RR: 0.76 [95% CI: 0.63 to 0.93]; p = 0.006). In contrast, the risk of all-cause death (RR: 0.94 [95% CI: 0.86 to 1.03]; p = 0.21) and of CV death (RR: 0.91 [95% CI: 0.69 to 1.20]; p = 0.493) were not significantly reduced. New cancer onset did not differ between statin- and placebo-treated subjects (RR: 0.99 [95% CI: 0.85 to 1.15]; p = 0.89)
Savarese G, et al. J Am Coll Cardiol 2013; 62: 2090 - 9

• Primary care electronic medical records from the UK Clinical Practice Research Datalink. Compared older (60+) statin users and 1:1 propensity-score-matched controls (total n = 12,156; ≈38% > 80 years old). Follow-up: 10 years
• Mean age 76.5 ± 9.2 years. Statins associated with near significant reduction in MI recurrence (subhazard ratio = 0.84, 0.69 - 1.02, p = .073), with protective effect in the 60-79 age group (0.73, 0.57 - 0.94) but a nonsignificant result in the 80+ group (1.06, 0.78 - 1.44; age interaction p = .094). No significant associations were found for stroke or dementia. Data suggest an increased risk of falls (1.36, 1.17 - 1.60) and fractures (1.33, 1.04 - 1.69) in the first 2 years of treatment, particularly in the 80+ group.
• Ble A, et al. J Gerontol A Biol Sci Med Sci 2016 May 4. pii: glw082. [Epub ahead of print]

• Treatment was associated with lower all-cause mortality. (HR = 0.62, 0.57 - 0.68, p < .001). Increasing age (60-79: 0.62, 0.55 -0.72, p < .001; 80+: 0.77, 0.67 - 0.89, p < .001; p for interaction = .010), but not burden of disease, affected the association between statins and all-cause mortality
• Statin use was associated with health care cost savings in the 60 - 79 group but higher costs in the 80+ group
Ble A, et al. J Gerontol A Biol Sci Med Sci 2016 May 4. pii: glw082. [Epub ahead of print]

• 5152 men and women from the Age, Gene/Environment Susceptibility-Reykjavik Study. Mean age 77 years (range: 66 - 96 years)
• Prevalence of type 2 DM was 12.4% of which 35% used statins. Statin use was associated with a 50% (95% CI 8 to 72%) lower CV mortality and 53% (29 to 68%) lower all-cause mortality in persons with DM. For those without DM, statin use was associated with a 16% (-24 to 43%) lower CV and 30% (11 to 46%) lower all-cause mortality
• Persons with DM on statins had a comparable risk of CV and all-cause mortality asthe general population without DM
• The effect was independent of glycaemic controlOlafsdottir E, et al.. BMJ Open 2011;1(1):e000132

• Inclusion criteria: randomized allocation to statin or placebo, documented CHD, ≥ 50 elderly patients (defined as age ≥ 65 years) and ≥ 6 months of follow-up
• 9 trials, 19,569 patients (age range: 65 - 82). Pooled rates of all-cause mortality were 15.6% with statins and 18.7% with placebo. RR 0.78; 95% credible interval [CI] 0.65 - 0.89 over 5 years. Furthermore, statins reduced CHD mortality by 30% (RR 0.70; 95% CI 0.53 - 0.83), nonfatal MI by 26% (RR 0.74; 95% CI 0.60 - 0.89), need for revascularization by 30% (RR 0.70; 95% CI 0.53 - 0.83), and stroke by 25% (RR 0.75; 95% CI 0.56 - 0.94)
Afilalo J, et al. J Am Coll Cardiol 2008; 51: 37 - 45

• Randomized controlled trials comparing any statins with placebo or usual care for primary prevention of CVD in subjects aged ≥65 years
• Eight studies (n = 25,952) were included in the meta-analysis
• Statins significantly reduced the risks of composite major adverse CV events (RR 0.82, 95% CI 0.74-0.92), nonfatal MI (0.75, 0.59-0.94) and total MI (0.74, 0.61-0.90)
• Treatment effects of statins were insignificant in fatal MI (0.43, 0.09-2.01), stroke (fatal: 0.76, 0.24-2.45; nonfatal: 0.76, 0.53-1.11; total: 0.85, 0.68-1.06) and all-cause mortality (0.96, 0.88-1.04)
Teng M, et al. Drugs Aging 2015; 32: 649 - 61

• Significant differences were not observed in myalgia (0.88, 0.69-1.13), elevation of hepatic transaminases (0.98, 0.71-1.34), new-onset diabetes (1.07, 0.77-1.48), serious adverse events (1.00, 0.97-1.04) and discontinuation due to adverse events (1.10, 0.85-1.42).
• Myopathy, rhabdomyolysis and cognitive impairment was largely unreported in the included trials.
Teng M, et al. Drugs Aging 2015; 32: 649 - 61

CONCLUSIONS
Adherence to statins in the elderly
Depriving treatment in the face of guidelines?
Common sense (e.g. terminal cases or potential problem with “first do no harm”)
Clearly more evidence required

How to address discontinuation
Pharmacists, nurses, auto-reminders, refill remindersKnowledge of guidelines. Confusion – too many guidelines
Side effects real or imagined; Prescriber’s role: “take your time”Patient participation; know your level and why you need to achieve it
Alternative medication optins (e.g. ezetimibe, PCSK9 inhibitors); drug spacingDealing with risk factors for side effects: thyroid, vit D? CoQ10?
Monitor: new ACC guidelines; wireless-enabled pill bottles or even pillsPolypharmacy; polypill;
Special cases: discontinuation on admission for ACSCost to patient or prescriber’s budget
Patient characteristics: other drugs, age, exercise, genetics, dementia, motivation, effect of the press on patients
Defining statin intolerance

Stroes ES, et al.; European Atherosclerosis Society Consensus Panel. Statin-associated muscle symptoms: impact on statin therapy-EuropeanAtherosclerosis Society Consensus Panel Statement on Assessment, Aetiologyand Management. Eur Heart J 2015; 36:1012 - 22
Banach M, et al. Statin intolerance - an attempt at a unified definition.Position paper from an International Lipid Expert Panel. Arch Med Sci 2015;11: 1 - 23
Statin-associated muscle symptoms = SAMS
The second panel statement considers SAMS as well as other side effectsassociated with statin use (e.g. liver)

OTHER SPECIFIC GROUPS
• GENDER:As shown in the ESC 2016 guideline slide there is no difference between men and women in terms of benefit from statin treatment. However,
- Pre-menopausal vs post-menopausal- HRT- Representation in trials

OTHER SPECIFIC GROUPS
• HIV:Complex situation:• Drug interactions• Other factors: inflammation, lipodystrophy, insulin
resistance and new onset diabetes

OTHER TRIALS
• CARDS: Diabetes type 2; atorvastatin 10 mg vs placebo
• HPS: high risk patients; simvastatin 40 mg vs placebo
• TNT: stable CHD; atorvastatin 10 mg vs atorvastatin 80 mg


Risk ratio (95% CI)PlaceboEze/simv
Eze/simv better
Placebo better
(n=4620)(n=4650)
Non-dialysis (n = 6247) 296 (9.5%) 373 (11.9%) Dialysis (n = 3023) 230 (15.0%) 246 (16.5%)
Major atherosclerotic event 526 (11.3%) 619 (13.4%) 16.5% SE 5.4 reduction (p=0.0022)
0.6 0.8 1.0 1.2 1.4
SHARP: Major Atherosclerotic Eventsby renal status at randomization
No significant heterogeneity between non-dialysis and dialysis patients (p = 0.25)

SHARP: Cause-specific mortality Risk ratio & 95% CIEvent PlaceboEze/simv
Eze/simvbetter
Placebobetter
(n = 4620)(n = 4650)
Coronary 91 (2.0%) 90 (1.9%) Other cardiac 162 (3.5%) 182 (3.9%) Subtotal: Any cardiac 253 (5.4%) 272 (5.9%) 7.4% SE 8.4
reduction (p=0.38) Stroke 68 (1.5%) 78 (1.7%)
Other vascular 40 (0.9%) 38 (0.8%) Subtotal: Any vascular 361 (7.8%) 388 (8.4%) 7.3% SE 7.0
reduction (p=0.30)
Cancer 150 (3.2%) 128 (2.8%) Renal 164 (3.5%) 173 (3.7%) Other non-vascular
Subtotal: Any non-vascular 668 (14.4%) 612 (13.2%) 8.6% SE 5.8 increase (p=0.14)
Unknown cause 113 (2.4%) 115 (2.5%)
Total: Any death 1142 (24.6%) 1115 (24.1%) 1.9% SE 4.2 increase (p=0.65)
0.6 0.8 1.0 1.2 1.4
354 (7.6%) 311 (6.7%)

Risk ratio & 95% CIEvent PlaceboEze/simv
Eze/simvbetter
Placebobetter
(n = 3130)(n = 3117)
Main renal outcomeEnd-stage renal disease (ESRD) 1057 (33.9%) 1084 (34.6%) 0.97 (0.89-1.05)
Tertiary renal outcomesESRD or death 1477 (47.4%) 1513 (48.3%) 0.97 (0.90-1.04)
ESRD or 2 x creatinine 1190 (38.2%) 1257 (40.2%) 0.94 (0.86-1.01)
0.6 0.8 1.0 1.2 1.4
SHARP: Renal outcomes

Prop
ortio
nal r
educ
tion
inat
hero
scle
rotic
eve
nt ra
te (9
5% C
I)
0%
5%
10%
15%
20%
25%
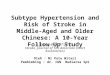
30% Statin vs control(21 trials)
Mean LDL cholesterol differencebetween treatment groups (mg/dL)
More vs Less(5 trials)
SHARP32 mg/dL
0 20 4010 30
SHARP17% risk reduction
CTT: Effects on Major Atherosclerotic Events

LIPIDS AND STATINS IN CKD
• “Normal” renal function:Statins improve eGFR and reduce vascular events (GREACE, HPS, TNT, CARDS)
• Pre-dialysis:Ezetimibe + simvastatin reduces events but no change in renal function (SHARP)
• On-dialysis:Statins no improvement in events or renal function (4D, AURORA). Ezetimibe + simvastatin reduces events (SHARP)

Why was SHARP successful?n DM Duration HD
AURORA: 2,776 20% 3.8 yrs ALL
4D: 1,255 ALL 4 yrs ALL
SHARP: 9,270 23% 4.9 yrs 1/3** No heterogeneity

OTHER SPECIFIC GROUPS
• CKD:Kidney dysfunction = CHD equivalent

Change in serum creatinine (%) in the structured and the usual care groups
Athyros VG et al. J Clin Pathol 2004; 57: 728 - 34
-15
-10
-5
0
5
0 6 w 6 m 12 m 18 m 24 m 30 m 36 m 42 m 48 m
Usual Care no hypolipidemics n=687 Usual Care hypolipidemics n=113Structured Care no atorvastatin n=17 Structured Care atorvastatin n=783
-9.6%
-4%
3%2%

Special conditions
• Pre-operative statins and CKD
• Post-transplant
• Contrast Induced Nephropathy (CIN)

CONCLUSIONS
• Dialysis: probably no statin benefit• Early CKD: statin benefit• CKD prevention: statin benefit
Proteinuria/microalbuminuria

OTHER SPECIFIC GROUPS
• ONCOLOGY:Radiation to the heartCytotoxic drugs and the heartDisease effects

OTHER SPECIFIC GROUPS
• AUTOIMMUNE DISEASES:
SLE, RA, Psoriasis
• Effect on disease progression (symptoms, complications)
• Effect on inflammatory markers
• Effect on CV risk

OTHER SPECIFIC GROUPS
• TRANSPLANTATION:
Lovastatin, atorvastatin, simvastatin CAUTION in patients on immunosuppressants(i.e. cyclosporine, sirolimus, tacrolimus)
• CYP3A4

Garshick M, Underberg JA. The Use of Primary Prevention Statin Therapy in Those Predisposed to Atherosclerosis. Curr Atheroscler Rep 2017; 19: 48

A professor is someone who talks in someone else’s sleep
WH Auden 1907 – 1973 English poet
I hope that I kept you awake!