Embed Size (px)
Citation preview

Non-PCI Hospitals: STEMI Diagnosis -- Treatment
Decreasing Delays and Improving Outcomes
J. Lee Garvey, MD
Emergency Medicine
Carolinas Medical Center
Charlotte, NC

Disclosure Statement
Presenter:
J. Lee Garvey, MD
Title:
“Non-PCI Hospitals: STEMI Diagnosis -- Treatment
Decreasing Delays and Improving Outcomes”
No financial conflicts

STEMI Diagnosis
• ECG based diagnosis
– Need for SPEED � 10 minutes
• Prehospital ECG
• Triage ECG
• Once STEMI identified � trigger a response
• Goal is reperfusion

“10 minute” ECGs

PROBLEM:
A clinical history of ischemic-type chest discomfort (JAMA
2000;283:3223-29 )
• Primary symptoms (67%):
– Retrosternal chest pain (discomfort) with radiation to the neck, jaw, shoulders, or down the inside of either arm
• Secondary symptoms (33%):
– Shortness of breath, weakness, syncope, palpitations, diaphoresis, nausea, or vomiting

A clinical history of ischemic-type chest discomfort:
Lee Arch Int Med 1985:145;65-9
0
20
40
60
80
100
MI No MI
Chest Pain
Pt's (%
)
A t yp ical C P
T yp ical C P

Since 1/3 of AMI patients do not have “chest pain”,how do I screen for rapid ECG?!?

Triage of patients for a rapid (5-minute) electrocardiogram:
A rule based on presenting chief complaint.
Graff et al. Ann Emerg Med. Dec 2000;36;554-560.
• Symptoms derived from ED MI database – Tested retrospectively and prospectively
• Outcomes:
– STEMI -- Door to ECG decreased
• 10.0 --> 6.3 minutes
– STEMI -- Door to drug decreased• 36.9 --> 26.1 minutes
– 1% increase in ECGs performed
• 6.3% --> 7.3%
– 100% sensitive for patients with STEMI

RAPID EKG CRITERIA
Door to decision 10 minutes
≥≥≥≥ 30 YEARS OLD with suspicious CHEST PAIN(EXCLUDING OBVIOUS TRAUMA)
≥≥≥≥ 50 YEARS OLD with:
SyncopeWeakness
Rapid Heart Beat / PalpitationsDifficulty Breathing / Shortness of Breath
Reference: Graff L, Palmer AC, LaMonica P, Wolf S. Triage of patients for a rapid (5-minute) electrocardiogram:
a rule based on presenting chief complaints. Ann Emerg Med. December 2000;36:554-560.

ECG = STEMI

Attack Program for AMI
• Reperfusion strategy is institution
dependent
• Do not allow “confusion about reperfusion”
• PCI favored at interventional facilities
– 24/7? What about ‘off hours’
presentation
– Requires commitment of entire hospital
• Lytic drug if PCI not available within 90 minutes of first contact

Initial Reperfusion Therapy
• 3 Major Options:
• Pharmacological Reperfusion (Fibrinolytics)
• Primary Percutaneous Coronary Intervention
(PCI)
• Acute Surgical Reperfusion Antman et al. JACC 2004;44:680.
Primary Goal In STEMI:Achieve Coronary Patency
Class IAll patients should undergo rapid evaluation for reperfusion therapy & have a reperfusion strategy implemented promptly after contact with the medical system

Non-PCI Hospital STEMI Care
• Transfer for PCI
• Lytic and transfer
• Lytic and keep?

The system is as important
as the treatment

Optimizing the System
• Understand what the System is:
– Begins with the patient
– Prehospital environment
– Emergency Department
– Cardiology consultants
– Fibrinolytic drug administration, or catheterization laboratory for PCI

Optimizing the System
• Serial processing of individual steps:– Medic/ Hospital arrival
– ECG acquired– Data to decision maker
– Physician evaluation (EP, Primary care?)– Transfer call initiated
– Treatments administered
– Patient transported (transferred?)– Procedure initiated
– Reperfusion accomplished
Parallel

17
System Barriers to Reperfusion
• Lack of Standardized Protocols/ Standing Orders
• Ambiguity of Leadership and Responsibility– ED / EMS / Cardiology / Hospital / Government
• Inter Facility Transfer Issues– Majority of STEMI patients present to a facility w/o PCI capability
– EMTALA (Emergency Medical Transfer and Active Labor ACT)
Hospital liability for transferring “unstable” patients
– Locally funded and administered EMS
– Ability to transfer across single or multiple county lines may be restricted by coverage and/or guideline issues
– 50% of STEMI admissions come directly to local ED- EMS is not activated

Prehospital 12 lead ECG

19
AMI Guidelines 2004
JACC 2004;44:686.

20

21
Cardiac Destination Hospitals
• Should EMS ‘drive by’ one facility to deliver patient to a PCI center?
– This should be well coordinated within the EMS
community
• Distance/ time involved
• High risk STEMI patient
• Lytic ineligible patient

Reperfusion Checklist




Primary PCI or LyticsThe Importance of TimePrimary PCI or Lytics
The Importance of Time
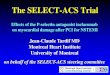
PCI-Related Time Delay (DTB - DTN)PCI-Related Time Delay (DTB - DTN)
Circle sizes = sample size of the individual study.
Solid line = weighted meta-regression.
Circle sizes = sample size of the individual study.
Solid line = weighted meta-regression.
Nallamothu BK et al., Am J Cardiol. 2003Nallamothu BK et al., Am J Cardiol. 2003
Favors PCIFavors PCI
Favors LysisFavors Lysis
Every 10 min delay to PCI: 1% increase in mortality differenceEvery 10 min delay to PCI: 1% increase in mortality difference
P = 0.006P = 0.006
62 min62 min
Ab
so
lute
Ris
k D
iffe
ren
ce i
n D
eath
(%
)A
bso
lute
Ris
k D
iffe
ren
ce i
n D
eath
(%
)
1515
1010
55
00
-5-500 2020 4040 6060 8080 100100

Develop a reperfusion strategy
for your institution
• Have a well thought-out strategy that fits the patients’ needs to the resources of your institution
• Communicate strategy to all care givers
• Minimize branch points/ decision points
• Empower decision makers: EMS, EP
• Anticipate needs (registration, lab, Rx)

Code STEMI Protocol
• Prehospital (or ED) activation of STEMI Team– EPs, ED RNs, Techs,
?Cardiology, Nursing Supervisor
• Short stay in ED for evaluation, medicines (ASA, heparin, ?lytic).
• Labs, XR, etc only if time permits
• No infusions– Goal is to leave ED within
30 min of arrival

Transfer for PCI
• PCI Center selection
– How to chose, if several available
– Patient request
– Ease and timeliness of transfer
• Single call to arrange transfer
• Hotline
– Accepting site should activate their plan on your call

Transfer for PCI
• Transportation issues
– Air vs. ground
• Weather and availability
– Your EMS
• Backfill issues
• Limitation of local resources

Circulation 2005;111:761-767Circulation 2005;111:761Circulation 2005;111:761--767767
1st Door to Balloon11stst Door to BalloonDoor to Balloon Door to DoorDoor to DoorDoor to Door
95.8% of patients treated after 90 minutes95.8% of patients treated after 90 minutes95.8% of patients treated after 90 minutes

NRMI-5: North CarolinaJuly 2003-June 2004
NC Nation Guidelines
N 2,738 79,927
% eligible treated 81% 80%
Door-balloon 101 min 100 min <90 min
11PM to 7AM 107 min
Weekend 105 min
Transfer
1st door – balloon 191 min 165 min <90 min
1st d-b <90 min 0.8% 5.5% 100%
NC Nation Guidelines
N 2,738 79,927
% eligible treated 81% 80%
Door-balloon 101 min 100 min <90 min
11PM to 7AM 107 min
Weekend 105 min
Transfer
1st door – balloon 191 min 165 min <90 min
1st d-b <90 min 0.8% 5.5% 100%




RACE
� Need for improvement in timeliness of
STEMI reperfusion
� To do so the SYSTEM is as important
as the SPECIFIC TREATMENT

RACE
� Key results:� All hospitals showed improved processes
� Median reperfusion times improved� D2B PCI: 85 min � 74 min
� % Pts PCI within 90 min (non transfer): 56% � 72%
� D2Needle: 35 min � 29 min
� Door1In to Door1 Out: 120 min � 71 min� % Pts PCI within 90 min (transfer): 4% � 13%
� Median D12B : 165 min � 128 min
� No change in hospital mortality
� Did not measure morbidity

Top Ten List
10. Use local ambulance to transport pts within 50 miles
9. Keep patient on local ambulance stretcher
8. Give heparin bolus (70 U/kg) and no IV infusion
7. Establish protocol for lytics vs. PCI for each ED
6. Establish single call number to PCI centers that "automatically" activates cath lab
5. Apply Process Improvement techniques to STEMI care/ referrals
4. Provide standardized feedback reports to each ED
3. Prehospital ECG’s for all CP patients
2. Train all Paramedics to read ST elevation on ECG’s, call from ambulance to activate cath lab
1. Create EMS, ED, cardiology team with committed leadership

Accreditation – Cycle II 2006 - 2008
www.scpcp.org

Chest Pain Center
• A Chest Pain Center is not a section of the hospital that treats STEMIs
• Nor is it an area dedicated to evaluation of ‘low risk’ chest pain patients
• A Chest Pain Center, like a Trauma Center, is a facility wide process based system that starts from the time a patient activates EMS until that patient is discharged from the hospital.

1.1. ED Integration with EMSED Integration with EMS
2.2. Emergency Assessment Emergency Assessment
-- Diagnosis and Treatment of ACSDiagnosis and Treatment of ACS
3.3. Evaluation of Low Risk Patients Evaluation of Low Risk Patients
4.4. Functional Facility DesignFunctional Facility Design
5.5. Personnel, Competencies, Training Personnel, Competencies, Training
6.6. Organizational StructureOrganizational Structure
7.7. Process Improvement Orientation Process Improvement Orientation
8.8. Community OutreachCommunity Outreach
8 Key Elements of a Chest Pain Center

Process Improvement –Case review and feedback
• Questions to ponder in each case review:– Meet regularly
– Post timeline of reperfusion intervals for each case
– Let the staff know what the outcomes were
– Identify areas that were done well by EMS, ED, Cardiology
– Identify areas that need improvement by EMS, ED, Cardiology
– Decision makers can modify institution’s process