Embed Size (px)
Citation preview

1 Int roduct ion
WE HAVE developed a wearable artificial endocrine pancreas with a needle-type glucose biosensor and have established physiological glycaemic regulations in ambulatory diabetic patients (Sn]cmRi et aL, 1982; 1984).
However, the major obstacle to extending the term of glycaemic control has been the lack of success in developing an implantable glucose sensor with high precision in tissue or blood glucose determination. Conventional methods, either chemical or electrochemical, for the determination of blood glucose are not suitable for application in vivo on a long-term basisl Therefore, it is necessary to seek other methods to measure blood or tissue glucose concentrations noninvasively. Currently, the most promising method for
Reprints are available from Dr K. Kajiwara
First received 9th January and in final form 29th June 1992
�9 IFMBE: 1993
the noninvasive determination of blood glucose appears to be infra-red spectroscopy.
In 1978, KAISER (1978; 1979) made the interesting suggestion of measuring the physiological concentrations of glucose noninvasively, in very thin layers, by using Fourier transform infra-red (FTIR) spectroscopy with an attenuated total reflection (ATR) prism. We have also evaluated the feasibility of FTIR spectroscopy with an ATR prism in glucose measurement and have reported that glucose molecules had characteristic absorptions at the wave numbers of 1033 and 1080cm -1 and that the difference absorbance spectra were useful in eliminating the interference derived from constituents in the blood with glucose specific absorbances (KAJIWARA et al., 1989a; 1989b; 1990; 1991).
In this study, we have examined whether FTIR spectroscopy with an ATR prism could be applied for noninvasive glucose measurement through oral mucous membranes.
MBEC Kyoto World Congress supplement July 1993 S17

2 Mater ia ls and methods
2.1 Equipment
In this experiment, infra-red absorption spectra were recorded on a Fourier transform infra-red spectrometer (model FT/IR-5M, Nihon Bunko Co. Ltd., Tokyo, Japan) equipped with a zinc-selenate attenuated total reflection prism (flat-type) at 40 ~ angle of incidence. The absorption spectra were obtained at wave numbers from 4300 to 400 cm ~ under the conditions of 25-27~ room tempera- ture. Each sample was scanned 500 times for glucose aqueous solution and blood, and 100 times for oral mucosa. The time taken to complete 100 scans was 100 s. The light from the nichrome emitter was divided into two beams by a beam splitter, introduced into a sample cell with an unknown sample and a reference cell with distilled water, reflected repeatedly by an ATR prism, and finally detected by a nitrogen-cooled mercury-cadmium-tellerium (MCT) detector.
The absorption coefficients of the samples (glucose solution, blood sample or oral mucosa) and of distilled water were determined in a sample and a reference cell, respectively. By calculating the difference between them, the absorption of the molecules contained in the samples was obtained. In all experiments, the absorbance spectra at 1033 cm ~ showing the greatest sensitivity to glucose were used for the quantification of glucose concentrations.
2.2 Exper iments
2.2.1 Evaluation in the glucose aqueous solutions: Aqueous solutions with glucose concentrations of 10-1000mg (100ml -~) were prepared for the measurement of their infra-red spectra. The correlation between glucose con- centrations and the absorption intensities at 1033 cm ~ was examined.
2.2.2 Evaluation in serum and whole-blood samples: Thirty serum and whole-blood samples were obtained before and after each meal from six diabetic patients. Their infra-red absorption spectra were measured to calculate difference absorption spectra with corresponding fasting samples. By using the calibration curve obtained in the recovery test, the increases in glucose concentrations above fasting levels were estimated from the absorption intensities of these difference absorbances. Then, the changes in serum or whole-blood glucose concentrations thus obtained were compared with those measured by the glucose oxidase method (YSI model 23A, Yellow Springs Instruments, USA).
2.2.3 Evaluation in oral mucous membrane: Absorbance spectra obtained through oral mucosa were compared with those obtained from aqueous glucose solutions or blood samples. Thirty absorbance spectra were obtained from oral mucosa of diabetic patients, and their blood glucose levels were measured by the glucose oxidase method. Then, the correlation between blood glucose concentrations and the corresponding absorption intensities at 1033 cm 1 was calculated.
To correct the baseline drifts due to prism attachment to oral mucosa, the peak at 2920cm-~ derived from an asymmetrical stretching of the carbon hydrogen bond in the molecules was used as a reference peak, because the absorption intensity of this band is proportional to the spectral changes due to prism attachment at 1033 cm -~ Thirty infra-red absorbance spectra, under various in- tensities of the prism attachment to oral mucosa, were studied in a healthy subject, whose blood glucose showed
80mg (100m1-~). From these absorbance spectra, the correlations between the second derivatives of absorbance spectra at 1033 cm 1 and those at 2920 cm -~ (LANZA, 1983; CONWAY et al., 1984) were calculated. The linear regression line thus obtained was used to correct the spectral changes caused by different intensities of attachment of the prism to oral mucosa.
Thirty absorbance spectra through the oral mucosa of five diabetic patients were measured to examine the correlation between blood glucose concentrations and the second derivatives of absorption intensities at 1033 cm after correcting the spectral changes due to prism attachment. Then, the correlation was studied between the differences of the second derivatives at 1033 cm ~ with the corresponding fasting samples (corrected second derivative at 1033 cm-~) and the increases in glucose concentration above fasting level by the glucose oxidase method.
3 Results
3.1 Evaluation in glucose aqueous solutions
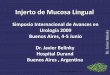
Glucose-specific peaks appeared at approximately 1160, 1107, 1080 and 1033 cm -1, with the 1080 and 1033 cm 1 peaks being the most prominent and indicative of glucose. Among them, the peak intensity at 1033 cm-~ showed the greatest sensitivity to glucose. Therefore, the peak intensity at 1033 cm- ~ was applied for the quantification of glucose concentrations in aqueous solutions. The calibration curve between the peak intensities at 1033 cm ~ and the glucose concentrations in aqueous solutions yielded a slope of 1-689 x 10 -3 ml mg 1 with r = 0"999 (Fig. 1).
'7 E t~
O
~6 .'2-
g o
O .o
o to
.Q O
Fig. 1
Y, x10 -2 2.0
f / z I
. , , /
/ 1 / / J
1 , J " J s ~ / /
/ # �9
1.0 / " . / "
+, ,- / �9
0 " I I • 500 1000
g l u c o s e concen t ra t i on , mg 100 ml -I
Linear regression analysis between glucose concentrations and absorption intensities" at 1033 cm i in glucose aqueous solutions. Correlation between glucose concen- trations (x: mg (lOOml i)) and absorption intensities at 1033cm 1 o f FTIR-ATR absorption spectra (y: absorbance unit) shows y = (1689x + 120) x 10 5 ( r - 0"999; n = 30). Each point represents the mean q f five delerminations. A 95 per cent confidence interval is depicted
3.2 Evaluation in serum and whole-blood samples
In contrast to the glucose in distilled water, the intensity of absorbance at 1080cm ~ was greater than that at 1033 cm i in these samples because of the interference of blood constituents other than glucose. These differences
$18 MBEC Kyoto World Congress supplement July 1993

were eliminated by expressing the result as the difference from the fasting sample. The calibration curves between the peak intensities of difference in absorbance at 1033 cm -1 and the increases in glucose concentrations yielded a slope of 1-670 x 10 -3 ml mg -~ with r = 0-998 for serum samples,
"7
E Iooo
, . ~ 0
oE
~ l - - -
g5 o ~ 500 u h
o~
_~
>
0
"7
�9 - o 1000
a
o f f .Q O o s c oE Bo: c
g ~. 500 o �9 m, . .c 0 ~
.o
Fig. 2
// i / / / /
// / //
Ill/I ] ] l ~ ~ [I /r
J 1 / J / ~ 1 / ~ / / / i ! / ' S / ' ~ / !/ 's / / / / / / / / / I
/ ~ 0 / / / /// ~ sY//
/ / / I / , t ~ 1 I
.J
/ ~ , / "
/ ; I X 5 o 1ooo
0 / / / / / / / /
// /
/ / / / /
/ / / / /
l / f l ~ / / ," i
1// i
/ / r / i z~ Q / r
/ /
i / i / I / /
/ I 1 500 1000
increase in glucose concentration above fast ing level measured by the glucose oxidase method,
mg 100 m1-1
b
Linear regression analyses between the increases in glucose concentrations above fasting levels measured by Fourier transform inJ?a-red absorbance spectroscopy and those measured by the glucose oxidase method in serum and whole-blood samples. Correlations between the increases in glucose concentrations measured by the glucose oxidase method (x . m~.l (lOOml 1)) and the changes in glucose concentrations measured by Fourier transJorm infra-red spectroscopy (y: mg ( lOOml- l ) ) show (a) y=O'994x + 1"26, i"= 0"981, n = 30, in serum samples, and (b)
y = 0.999x + 324; r = 0"989; n = 30, in whole-blood samples. The 95 per cent confidence intert~als are depicted
and a slope of 1-691 x 1 0 - 3 with r = 0.999 for whole-blood samples, respectively. By applying the calibration curves thus obtained, excellently high correlations were found between the increases in glucose concentrations above fasting levels measured by the FTIR/ATR method (y: mg (100 ml-1)) and those measured by the glucose oxidase method (x: mg (100ml-1)) (y = 0.994x + 1-26, r = 0-981 for serum samples, and y = 0-999x + 3.24, r = 0-989 for whole-blood samples, respectively; Fig. 2).
3.3 Evaluation in oral mucous membrane
3.3.1 Spectra obtained through oral mucosa and application o f peak intensity method at 1033 c m - 1 : As a whole, spectra obtained through oral mucosa were similar to those obtained fl'om blood samples (Fig. 3). However, the absorbance peak at 1033 cm- t significantly varied with the intensities of prism attachment to oral mucosa. Thus, there was no significant correlation between blood glucose concentrations and corresponding absorption intensities at 1033 cm -~, even if different absorbance spectra were analysed.
3.3.2 Effect o f pr ism at tachment to oral mucosa on absorption spectra: The absorbance spectra at 1033, 1080 and 2920cm ~ were measured with various degrees of pressure of the prism attachment to oral mucosa: loose, moderate and tight. As the attachment varied from loose to tight, the absorbance spectra shifted downwards (Fig. 3). Both the height and width of each peak were changed significantly according to the intensities of attachment. As shown in Fig. 4, the second derivatives of absorbance spectra at 1033 cm-1 (y: cm 2) were significantly correlated with those of absorbance spectra at 2920cm -1 (x: cm 2) (y = 0.295x -0 .077; r = 0-910). This linear regression line was applied to correct the spectral changes caused by the attachment of the prism to oral mucosa in the following analyses.
3.3.3 Correlation between the corrected second derivative at 1033 c m - 1 and the increase in glucose concentration above
fas t ing level: For 30 absorbance spectra through oral mucosa obtained from diabetic patients, first, the second derivatives of absorption intensities at 1033cm -1 were obtained by correcting the spectral changes due to prism attachment, and secondly, the corrected second derivatives were expressed as the difference in absorbance between the postprandial and fasting samples.' As shown in Fig. 5, the significantly high correlation between the corrected second derivatives at 1033cm 1 (y: cm=) and the glucose concentrations (x: mg (100ml 1)) was observed [y = (0-495x- 11.2)x 10-3; r = 0-915]. It was demonstrated, therefore, that blood glucose concentrations could be calculated noninvasively by using this calibration curve.
4 Discussion
In previous experiments, we have reported that a specific absorption of glucose molecules was at the wave number of 1033 cm- 1, compatible with those reported by BACK et al. (1984), BAUER and FLOYD (1987) and HOPKINSON et al. (1987), although there were very small differences between
1 their wave numbers, such as 1036, 1036 and 1031 cm respectively. It is already known that this absorption corresponds to the stretching motion or rotation of the pyran ring of glucose molecules (BACK et al., 1984), and that its absorbance varies in a dose-dependent manner according to Lambert-Beer's law. We found that, in glucose
MBEC Kyoto World Congress supplement July 1993 $19

Fig. 3
0.1
0"05
0
-0 .05
0.3
0.2
0 . Q
o o.1
blood glucose concentration 80mglOOm[ -1
-0.I , , 3000 2000
asymmetr ica l stretching band of CH 2
2920
tight
' 28'00 ' 3000 2900 2700 1200
I
1500 10'00
i i / glucose-speci f ic band
m oder , , i \
intensity of attachment
wove number, cm -1
1080 1033 i i
I ; I J 1100 1000 900
b c
Spectral changes caused by various pressures o f attachment o f an attenuated total reflection prism to oral mucosa. The top figure demonstrates that absorbance varies with various intensities o f attachment o f the A T R prism to oral mucosa. (b) and (c) indicate the expanded views o f (a) around 1033 and 2920 cm = 1, respectively
06 �9
.ID t-4
a E
5~ o.3 �9
0 1.0 ;~.0 second derivative of absorbance at 2920 cm -1,
xcm 2
Fig. 4 Linear regression analysis between the second derivatives o f infra-red absorbance spectra through oral mucosa at 1033cm -I (y: absorbance unit • cm 2) and those at 2920 cm ] (x: absorbance unit • cm 2) in a heahhy subject whose blood glucose shows 80 mg (100 ml 1). Correlation shows y = 0"295x + 0"077; r = 0"910; n = 30
aqueous solutions, there was a significantly high correlation between the absorption intensities at 1033 cm-1 and the glucose concentrations. We also reported that, in serum and whole-blood samples, red blood cell corpuscles, serum albumin and serum 7-globulin interfered with the absorbance spectra of glucose at 1033 cm 1 and shifted their baselines upwards significantly. However, by obtain- ing the difference between postprandial and the basal or fasting sample as an individual characteristic, we could eliminate these interferences and measure glucose con- centrations in serum and whole-blood samples quantitat- ively (KAJIWARA et al., 1989a; 1989b; 1990; 1991; SmcmR1, 1989).
In this study, we have found the same absorbance peak at 1033 cm 1 as in a glucose aqueous solution by analysing spectra through oral mucosa. However, these glucose specific peaks significantly varied with the pressure variation of ATR prism attachment to mucous membrane, so that the peak intensities at 1033cm 1 were poorly correlated with the blood glucose concentration.
To quantify blood glucose concentrations from absor-
$ 2 0 M B E C K y o t o W o r l d C o n g r e s s s u p p l e m e n t J u l y 1 9 9 3

0 .10
5 >
",7. E v ~ " 0 - 0 5 x "13 - gv
~ 0
o u 0
Fig. 5
�9 ~ O 0
/ e e
�9 e o
i i o 1oo 200
i n c r e a s e in g l u c o s e c o n c e n t r a t i o n a b o v e fasting l e ve l , mg l O O m i -1
Linear regression analysis between the corrected second derivatives o f infra-red absorbance spectra through oral mucosa at 1033cm -1 (y: absorbance unit + cm 2) and increases in glucose concentrations above fasting levels measured by the glucose oxidase method (x: mg (lOOml 1)). Correlation shows y = (0"499x-11"2) • 10 3; r = 0"915; n = 30
bance spectra through oral mucosa noninvasively, we first tried to correct these spectral changes due to the prism attachment to oral mucosa. The second derivatives of absorption spectra at 2920 cm - 1 were especially useful for this purpose, because the glucose-specific bands were not found near the wave number of 2920 cm - 1. This absorbance peak was reported to be derived from asymmetrical stretching of the carbon hydrogen bond in the polypeptide or lipid molecule (MIYAZAWA et at., 1956). In this experiment, we found that the spectral changes at 2920 cm- 1 were parallel to the changes at 1033 cm- 1 due to the various pressures of attachment of the ATR prism to the mucous membrane. Therefore, at first, to correct these spectral changes, we constructed the calibration curve between the second derivatives of the absorbance peak at 1033 cm 1 and those at 2920 cm - 1. Then, by obtaining the second derivatives of the differences between the post- prandial absorbance peaks and those of the fasting samples, thus eliminating an individual characteristic from this measurement, high correlations between the corrected second derivatives of absorbance spectra through the mucous membrane of the lip and the increases in blood glucose concentrations above the fasting level were observed. A more accurate calibration curve could be obtained by developing the method of quantifying the intensities of prism attachment to the human body.
Further studies are also necessary to obtain a final conclusion as to whether or not this infra-red spectroscopy can be applied clinically. For this purpose, we have to improve or develop the system in the areas of both hardware and software. The use of lasers in infra-red spectroscopy allows an improvement in measuring sensitiv- ity of a factor of 100 compared with the conventional technique, and can reduce the size of the system (KAISER, 1978; 1979).
In conclusion, as an alternative method of long-term glycaemic monitoring, a noninvasive blood glucose measurement system has been developed. Although the development of a sophisticated glucose measurement system will be a key technology, this method might provide
a useful monitoring system of the artificial endocrine pancreas for diabetic patients in the near future.
Acknowledgments--This work was supported in part by research grants from the Scientific Research Fund of the Ministry of Education, Science & Culture, Japan, and research grants from Nakatani Electronic Measuring Technology Association of Japan, Tokyo, Japan.
References BACK, D.M., MICHALSKA, D.F. and POLAVARAPU, P.L. (1984)
Fourier transform infrared spectroscopy as a powerful tool for the study of carbohydrates in aqueous solutions. Appl. Spectrosc., 38, 173-180.
BAUER, B. and FLOYD, T.A. (1987) Monitoring of glucose in biological fluid by Fourier transformation infrared spectroscopy with a cylindrical internal reflectance cell. Anal, Chim. Acta, 197, 295-301.
CONWAY, J.M., NORRIS, K.H. and BODWELL, C.E. (1984) A new approach for the estimation of body composition: infrared interactance. Am. J. Clin. Nutr., 40, 1123-1130.
HOPK1NSON, J.H., Movsxou, C., REYNOLDS, N. and NEWBERY, J.E. (1987) Application of attenuated total reflection of carbohy- drates and biological whole cell samples in aqueous solution. Analyst, 112, 501-505.
KAISER, N. (1978) Laser absorption spectroscopy with an ATR prism. Appl. Phys., 17, 1-4.
KAISER, N. (1979) Methods for determining the contents of metabolic products in the blood. IEEE Trans., BME-26, 597-600.
KAJIWARA, K., FUKUSHIMA, H., SHICHIRI, M., KAWAMORI, R. and YAMASAKI, Y. (1989a) Non-invasive measurement of glucose concentrations. J. Artif. Organs, 18, 1328 1331.
KAJIWARA, K., FUKUSHIMA, H., SAKAKIDA, M. and SHICHIRI, M. (1989b) Development of artificial endocrine pancreas-possibility of non-invasive measurement of blood glucose using infra-red spectroscopy with an ATR prism. In Recent advances in insulin therapy. LEE, T.H., HuH, K.B. and BABA, S. (Eds.), Excerpta Medica, Elsevier Science Publishers B.V., Amsterdam, 357-360.
KAJIWARA, K., FUKUSHIMA, H., SAKAKIDA, M. and SHICmRI, M. (1990) Non-invasive measurement of glucose concentrations. Interferences of biosubstances with the spectrum of glucose. Jap. J. Art i f Organs, 12, 881-884.
KAJIWARA, K., FUKUSHIMA, H., SAKAKIDA, M., HASHIGUCHI, Y. and SHICmRI, M. (1991a) Development of non-invasive measurement of glucose concentrations - Application of subtraction method. Ibid., 20, 183-187.
KAJIWARA, K., FUKUSHIMA, H., KISHIKAWA, H., NISHIDA, K., HASHIGUCHI, Y., SAKAKIDA, M., UEHARA, M. and SHICHIRI, M. (1991b) Spectroscopic quantitative analysis of blood glucose by Fourier transform infrared spectroscopy with an attenuated total reflection prism. Med. Prog. Through Technol., 17, (in press).
LANZA, E. (1983) Determination of moisture, protein, fat and calories in raw pork and beef by near infrared spectroscopy. J. Food Sci., 48, 471474.
MIYAZAWA, T., SH1MANOUCH1, T. and MIZUSHIMA, S. (1956) Characteristic infrared bands of monosubstituted amides. J. Chem. Phys., 24, 408418.
SHICHIRI, M., KAWAMORI, R., YAMASAKI, Y., HAKUI, N. and ABE, H. (1982) Wearable artificial endocrine pancreas with needle-type glucose sensor. The Lancet, il, 1129-1131.
SHICHIRI, M., KAWAMORI, R., YAMASAKI, Y., HAKUI, N. and ABE, H. (1984) Closed-loop glycemic control with a wearable artificial endocrine pancreas. Variations in daily insulin requirements to glycemic response. Diabetes, 33, 1200-1202.
SHICH1RI, M., YAMASAKI, Y., NAO, K., SEKIYA, M. and UH)A, N. (1988) In viva characteristics of needle-type glucose sensor. Measurement of subcutaneous glucose concentrations in human volunteers. Harm. Metab. Res., 20, Suppl., 17 20.
SHICHIRI, M. (1989) The future of insulin therapy. Towards a closed-loop system. In Proceedings o f 13th IDF Congress. LARKINS, R.G., ZIMMET, P.Z. and CHISHOLM, D.J. (Eds.), Excerpta Medica, Amsterdam, 23-27.
MBEC Kyoto'World Congress supplement July 1993 $21

Authors" biographies ~ ~ '~,~; ~ Ken-ichiro Kajiwara graduated from Kuma- .......
moto University Medical School, Kumamoto, i'i Japan, in 1984. After completing his training as
t a Junior Resident, he commenced research in Medical & Biological Engineering at the Department of Metabolic Medicine, Kuma- moto University Medical School. Since 1988, he has been a postgraduate student at Kumamoto University Medical School. His
major research fields include the artificial organ (pancreas) and its optical glucose sensor.
Dr Takero Uemura graduated from Kuma- moto University Medical School, Kumamoto, Japan, in 1986, and now is working as a Senior Resident on the development of noninvasive glucose monitoring based on Fourier transform infra-red spectroscopy in the Department of Metabolic Medicine, Kumamoto University Medical School.
Hideki Kishikawa graduated from Kumamoto University Medical School, Japan, in 1980. After completing his training as a junior resident in the Department of Geriatrics of Kumamoto University Hospital, he com- menced research work in diabetes at the Department of Metabolic Medicine, Kuma- moto University Medical School. Since 1983, he has been a Research Assistant there,
receiving a PhlD. in 1988. His major research fields include the artificial endocrine pancreas and cell biology in diabetes.
Dr Kenro Nishida graduated from Kumamoto University Medical School, Japan, in 1988, and now is working as a postgraduate student in the Department of Metabolic Medicine, Kuma- moto University Medical School, on the development of a needle-type glucose sensor covered with newly designed biocompatible membrane.
Dr Yasuyuki Hashiguchi graduated from Kumamoto University Medical School, Japan, in 1987, and now is working as a post-graduate student in the Department of Metabolic Medicine, Kumamoto University Medical School, on the development of extracorporeal glucose monitoring based on microdialysis sampling method.
Dr Masaya Uehara graduated from Kuma- moto University Medical School, Kumamoto, Japan, in 1986, and now is working as a postgraduate student on the developments and clinical applications of artificial endocrine pancreas, especially on the development of computer algorithms for insulin and glucagon infusions, in the Department of Metabolic Medicine, Kumamoto University Medical School.
Dr Michiharu Sakakida graduated from Ehime University Medical School, Japan, in 1980. After completing his training as a junior resident in the Department of Geriatrics of Kumamoto University Hospital, he began research work in diabetes at the Department of Metabolic Medicine, Kumamoto University Medical School. Since 1984, he has been a Research Assistant there, receiving a Ph.D. in
1992. His major research fields include the development and clinical applications of glucose sensors and artificial endocrine pancreas.
Kenshi Ichinose graduated from Ginkyo Gakuen College, Kumamoto, Japan, in 1974. Since 1975, he has been working as a Associate Technician on medical and biological engineer- ing at the Department of Metabolic Medicine, Kumamoto University Medical School.
Dr Motoaki Schichiri obtained his Medical Degree from Osaka University Medical School, Japan, in 1959, and Ph.D. from the Post- graduate School of Medicine, Osaka Uni- versity, in 1964. He then studied at the Department of Medicine, Case Western Re- serve University, Cleveland, Ohio, USA. He was a Research Associate (1967-78), Assistant Professor (1978-85) and Associate Professor
(1985-87) at the First Department of Medicine, Osaka University Medical School. In 1987, he was appointed Professor of Medicine, Kumamoto University Medical School. His main research activities are the development and clinical applications of glucose sensors and artificial endocrine pancreas.
S22 MBEC Kyoto World Congress supplement July 1993
![Research Article EVALUATION OF ANTI-INFLAMMATORY … · Percentage inhibition= [(absorbance of blank – absorbance of sample)/(absorbance of blank)]×100 1 In-vitro anti-inflammatory](https://img.pdfslide.net/doc/110x75/5e832a1607bd17145979ab05/research-article-evaluation-of-anti-inflammatory-percentage-inhibition-absorbance.jpg)