Embed Size (px)
Citation preview

Nonrandom Chromosomal Imbalances in PrimaryMediastinal B-Cell Lymphoma Detected by ArbitrarilyPrimed PCR Fingerprinting
Aldo Scarpa,1* Domenica Taruscio,2 Maria Scardoni,1 Francesca Iosi,2 Silvia Paradisi,2 Maria G. Ennas,3Gildas Rigaud,1 Patrick S. Moore,1 and Fabio Menestrina1
1Istituto di Anatomia Patologica, Universita di Verona, Strada Le Grazie, Verona, Italy2Laboratorio di Ultrastrutture, Istituto Superiore di Sanita, Rome, Italy3Dipartimento di Citomorfologia, Universita di Cagliari, Cittadella Universitaria Monserrato, Cagliari, Italy
We used arbitrarily primed polymerase chain reaction (AP-PCR) fingerprinting to identify chromosomal imbalances in sixprimary mediastinal B-cell lymphomas (PMBLs). Seventy-four chromosomal imbalances were detected, consisting of 49sequence gains and 25 losses. Amplifications on chromosome X were seen in five cases, four of which involved the samechromosomal locus. Nonrandom gains at the same locus were also identified on chromosomes 2 and 7 in four cases and onchromosomes 5, 9, and 12 in three cases. Five PMBLs were also analyzed by comparative genomic hybridization (CGH), whichfound chromosome arm 9p amplification as the only nonrandom imbalance. Our data demonstrate that chromosomalamplifications outnumber losses in PMBL. These mainly involve chromosomes 9 and X and may reflect more complexphenomena, such as translocations or other chromosomal rearrangements, as AP-PCR found coexistent gains and losses onthese chromosomes. Comparison between AP-PCR and CGH suggests that anomalies affecting the same chromosomal regionsmay occur at much higher frequencies than expected by CGH, suggesting that genomic amplifications are usually confined toDNA segments smaller than the megabase long segments required for detection in CGH. Modest increases in genetic materialmay be as effective as higher-level amplifications when affecting sites where a proto-oncogene resides. Genes ChromosomesCancer 26:203–209, 1999. r 1999 Wiley-Liss, Inc.
INTRODUCTION
Primary mediastinal B-cell lymphoma (PMBL) isa peculiar clinicopathologic entity among non-Hodgkin’s lymphomas, considered to arise from anoncirculating population of intramedullary, thymicB lymphocytes (Yousem et al., 1985; Addis andIsaacson, 1986; Menestrina et al., 1986; Moller etal., 1986; Davis et al., 1990; Paulli et al., 1997). Itaffects mainly young adult patients and has anaggressive clinical behavior, but correct diagnosisand aggressive therapy may greatly improve theprognosis (Lazzarino et al., 1997). PMBL expressesB-lineage surface molecules such as CD19 andCD20, has its immunoglobulin genes rearranged,and displays severe defects in expression of immu-noglobulin constituents and HLA class I and IImolecules (Menestrina et al., 1986; Moller et al.,1986, 1987a, 1987b; Momburg et al., 1987; Scarpa etal., 1987). Moreover, the MYC and REL proto-oncogenes as well as the TP53 tumor suppressorgene have been shown to be somatically altered in aproportion of cases (Scarpa et al., 1991; Joos et al.,1996; Tsang et al., 1996).
Little is known about chromosomal alterations inPMBL due to the rarity of the disease and thesubsequent difficulty in obtaining fresh material for
preparation of metaphase chromosomes. The onlyinformation on this topic has been obtained usingcomparative genomic hybridization (CGH) on 26cases, showing that chromosomal gains were by farmore frequent than losses and mainly involvedchromosomes 9, 12, and X (30% to 50% of cases;Joos et al., 1996). CGH is based on the use ofdifferentially labeled tumor and reference genomicDNA as probes that are cohybridized on normalmetaphase chromosomes. Chromosomal gains andlosses in the tumor are indicated by the increase ordecrease of the ratio of the signal intensities of thetwo fluorochromes involved, respectively (Kallioni-emi et al., 1992; Du Manoir et al., 1993).
Arbitrarily primed polymerase chain reaction (AP-PCR) is a recently developed DNA fingerprintingtechnique that has been successfully used to detectchromosomal abnormalities in cancer (Peinado etal., 1992; Ionov et al., 1993; Achille et al., 1996,1998; Okazaki et al., 1996; Malkhosyan et al., 1998).It uses single primers of arbitrarily defined se-
*Correspondence to: Aldo Scarpa, Istituto di Anatomia Patologica,Universita di Verona, Strada Le Grazie, I-37134 Verona, Italy.E-mail: [email protected]
Received 1 February 1999; Accepted 27 April 1999
GENES, CHROMOSOMES & CANCER 26:203–209 (1999)
r 1999 Wiley-Liss, Inc.

quence, whose annealing at multiple sites gener-ates many PCR products that represent a DNAfingerprint distinctive for any particular templateDNA-primer set. Comparison of AP-PCR finger-prints generated from tumor DNA with those frommatched normal DNA allows the detection ofqualitative and quantitative changes occurring atthe PCR-amplified loci. In particular, decreasedintensity of AP-PCR bands in tumor tissue reflectsallelic losses, whereas increased band intensity intumor DNA reflects the presence of extra copies ofthese sequences, which may be due to either geneamplification or tumor cell aneuploidy. The chromo-somal origins of most fingerprint bands may beeasily assigned by concomitant AP-PCR of somaticmonochromosome cell hybrid panels (Achille et al.,1996, 1998; Yasuda et al., 1996).
We applied AP-PCR analysis using two arbitraryprimers to six PMBLs for which high-molecular-weight DNA from matched tumor and normalsamples was available. For five of these cases, therewas sufficient DNA to perform CGH analysis aswell, which showed the amplification of chromo-some arm 9p as the only nonrandom anomaly.AP-PCR analysis detected a large number of chro-mosomal imbalances. These were mostly repre-sented by gains and mainly affected chromosomesX, 2, 5, and 7.
MATERIALS AND METHODS
Tumor Samples and DNA Extraction
Tumor samples were obtained at mediastinos-copy from untreated patients suffering from amediastinal mass. Fresh tissue fragments weredivided into two parts. One portion was fixed in10% formol-saline and processed for conventionalhistology. The other portion was snap-frozen inliquid nitrogen for immunohistochemistry and DNAanalysis. Diagnosis of PMBL was established ineach case by standard clinical and histopathologiccriteria and by cell marker analysis (Addis andIsaacson, 1986; Menestrina et al., 1986; Moller etal., 1986; Paulli et al., 1997). In all cases, immunohis-tochemical analysis confirmed the lymphoid natureof the neoplastic cells, which expressed panleuko-cyte antigen CD45 and several B-cell–related mark-ers, including CD20 and CD22. In no case couldsurface immunoglobulins be detected. The DNAwas extracted as described (Scarpa et al., 1991).Clonal immunoglobulin gene rearrangement prod-ucts were found in all cases and allowed theassessment of neoplastic cellularity, which wasgreater than 80% in each case. The normal control
DNA was obtained from peripheral blood mono-nuclear cells of each patient prior to treatment.
Arbitrarily Primed Polymerase Chain Reaction
Two arbitrary primers were used: MCG1, 58-AACCCTCACCCTAACCCCAA-38 and AR3, 58-GCGAATTCATGTACGTCAGG-38 (Peinado etal., 1992; Achille et al., 1996). DNA (70 ng) wasincubated with 0.6 unit of Taq polymerase (Perkin-Elmer/Cetus) 125 mM each dNTP, 0.13 µl of[a-32P]dCTP (Amersham, 3000 Ci/mmol), 10-mMTris-HCl, pH 8.2, 50-mM KCl, 5-mM MgCl2, 0.1%gelatin, and arbitrary primer (0.1 mM) in a finalvolume of 15 µl. The reactions were carried out in athermal cycler (PT-100, MJ Research) for fivecycles at low stringency (94°C for 30 sec, 50°C for 1min, and 72°C for 1.5 min) and 25 cycles at highstringency (94°C for 15 sec, 60°C for 15 sec, and72°C for 1 min). Five µl of the AP-PCR productwere diluted in 13 µl of dilution loading buffer(0.01% of each bromophenol blue and xylene-cyanol, 0.01-N NaOH, 0.1-M EDTA, 93% formam-mide), and 3-µl electrophoresed in a 5% polyacryl-amide gel containing 8-M urea set up by wedgespacers (0.4 to 1.2 mm). After electrophoresis, thegel was transferred on filter paper, dried undervacuum, and exposed for multiple times, rangingfrom 12 to 24 hr, to X-ray films (Kodak X-OmatAR). Each experiment was performed in triplicate.
Chromosomal assignment of AP-PCR fingerprintbands generated by MCG1 primer has been previ-ously described (Yasuda et al., 1996). For the AR-3primer, the chromosomal localization of AP-PCRbands was determined in a similar manner. Briefly,the AR-3 primer was used to amplify DNA (70 ng)from each of 24 monochromosomal hybrids in-cluded in the human/rodent somatic cell hybridpanel 2 (Drwinga et al., 1993). Hamster and mouseDNAs were used as controls. The chromosomalassignment was accomplished by comparing thehuman fingerprints with those obtained from eachmonochromosomal hybrid as described (Achille etal., 1996; Yasuda et al., 1996). To confirm theassignment of the bands, the simultaneous hybrid-ization of arbitrarily primed PCR DNA fingerprint-ing product (SHARP) analysis was used (Yasuda etal., 1996; Achille et al., 1998). The subchromosomalassignment for MCG1 fingerprint bands J and E hasbeen described previously (Malkhosyan et al., 1998),while that of bands A, O, and D was kindlyprovided by Dr. Manuel Perucho (La Jolla CancerResearch Foundation, La Jolla, CA).
204 SCARPA ET AL.

Comparative Genomic Hybridization
Test tumor DNA was labeled in a standardnick-translation reaction with biotin-11-dUTP(Sigma) and reference normal DNA with digoxi-genin-11-dUTP (Boehringer Mannheim). CGH ex-periments were performed as described (Speicheret al., 1995). Briefly, 400 ng each of labeled tumorand control DNA were ethanol-precipitated in thepresence of 50 µg of salmon sperm DNA and 40 µgof the Cot-1 fraction of human DNA (Gibco BRL).The probe mixture was dried and resuspended in10 µl of hybridization solution (50% formamide,10% dextran sulfate in 2 3 SSC). The DNA wasdenatured at 75°C for 5 min and allowed to prean-neal at 37°C for 30 min. The metaphase slides,obtained from phytohemagglutinin-stimulated pe-ripheral blood lymphocytes from normal healthydonors according to routine protocols, were dena-tured at 75°C for 2 min in 70% deionized for-mamide, 2 3 SSC, and were dehydrated throughgraded ethanols. Hybridization was performed for 3days at 37°C. After hybridization, the slides werewashed as described elsewhere (Ried et al., 1992).The biotinylated sequence was detected with avi-din DCS-conjugated fluorescein isothiocyanate (5µg/ml; Vector Laboratory). Probe sequences hap-tenized with digoxigenin were visualized with anti-digoxigenin conjugated to tetramethylrhodamine-isothiocyanate (TRITC; 3 µg/ml; BoehringerMannheim). The slides were counterstained withDAPI (4,6-diamino-2-phenylindole) and coveredwith an antifade solution.
Digital image analysis of CGH was performed byacquisition of three color images, DAPI, FITC, andTRITC, with a cooled charge-coupled device(CCD) camera mounted on a Zeiss Axioskop withan automated CGH analysis software package (Vy-sis). The ratio of FITC/TRITC fluorescence inten-sities was calculated along each chromosome. Ratiovalues obtained from at least 10 metaphase cellswere averaged and to interpret gain or loss of
chromosomal material upper and lower thresholdsof 1.25 and 0.75 were applied, respectively (Joos etal., 1996).
RESULTS
AP-PCR
AP-PCR DNA fingerprinting using MCG1 andAR-3 arbitrary primers was applied to the analysisof chromosomal changes in PMBL. Each primergenerated a fingerprint composed of more than 25bands. A total of 45 bands, 21 from MCG1 and 24from AR-3 fingerprints, had a chromosomal origineither previously determined or determined herein.Eighteen chromosomes were represented by atleast one fingerprint band, although the number ofbands originating from each chromosome varied.Chromosome 7 was represented by five bands,chromosomes 2, 3, and X by four bands, and theremaining chromosomes by three bands or less.Chromosomes 10, 14, 18, 19, and 21 were notrepresented by distinct fingerprint bands.
The results of AP-PCR analysis in the six PMBLsare summarized in Table 1 and detailed in Tables 2and 3. Representative examples are shown in Fig-ures 1 and 2. Chromosomal imbalances were foundin all six tumors. A total of 74 nonrandom chromo-somal imbalances were detected, consisting of 49sequence gains and 25 losses. The chromosomesmost frequently affected by sequence imbalanceswere 5 and X (6/6 cases) and chromosomes 2, 6, and9 (5/6 cases; Table 1). Considering individual finger-print bands, gains affecting chromosomes 2, 7, andX occurred at the same locus in four cases (Tables 2and 3). Gains affecting the same locus in at leastthree cases were also considered as nonrandom andwere observed on chromosomes 5, 9, 12, and 16.Among the 25 total losses detected, only thoseaffecting chromosome 8, 9q22.3, and 13q31.32 oc-curred at the same locus in more than one case.
TABLE 1. Chromosomal Imbalances in Six Primary Mediastinal B-Lymphomas Detected by AP-PCR Fingerprintinga
Case
Chromosome
1 2 3 4 5 6 7 8 9 10b 11 12 13 14b 15 16 17 18b 19b 20 21b 22 23 X
ML1 1 1 1 1 1 2 1 2 1 1ML2 2 1/2 1 1 1/2 2 1 2 1 1ML3 1 1 1 2ML4 1 1 1 1 1 1 1 1 1ML5 1 1 1 2 2 2 1/2 2 1 1 1ML6 2 1/2 2 1/2 1 1/2 2 1/2 2 1 2 1 1
a1 and 2 indicate gain and loss in intensity of fingerprint bands, respectively.bChromosomes not represented by distinct AP-PCR bands. All others show no chromosomal changes.
205CHROMOSOMAL IMBALANCES IN PMBL

The ability of AP-PCR to detect moderatechanges in chromosomal copy number is clearlydemonstrated by the unequivocal determination ofsubject gender by the intensity of AP-PCR bandsoriginating from the X chromosome. Comparingnormal DNAs, the intensity of bands T1 in theAR-3 fingerprint and G in the MCG1 fingerprintcorresponds to the copy number of the X chromo-some in the template DNA (Figs. 1 and 2).
CGH Analysis
The chromosomal losses and gains observed inCGH analysis of five PMBLs are summarized inFigure 3. The most prominent chromosomal imbal-ance identified was the overrepresentation of theshort arm of chromosome 9 in three cases (patients2, 3, and 5). The minimal amplified region in thesecases was 9p24–p22. Case 4 showed amplificationof several bands of the X chromosome, includingXp11.2–q13, Xq21–q26, and Xq27–q28. Other ge-netic aberrations identified in single tumors weregains of chromosome 1 between bands 1q11 and1q21.1 in case 1, 3p26–p24 in case 5, and 6q22 incase 3. A genomic loss was found only in one case,mapping to 15q24–q25. As suggested by validationprocedures of the CGH technique, all the amplifica-
tions found in pericentromeric and telomeric re-gions as well as anomalies in chromosome 19 andthe distal part of chromosome arm 1p were ex-cluded from the results (Hermsen et al., 1996; Jooset al., 1996).
DISCUSSION
We obtained a molecular karyotype of six cases ofPMBL using AP-PCR fingerprinting of matchednormal and tumor DNA with two arbitrary primers.Nonrandom imbalances were observed on sevendifferent chromosomes, namely, 2, 5, 7, 9, 12, 16,and X. By CGH, only the amplification of the shortarm of chromosome 9 was found to be nonrandom.
The X chromosome showed gains by AP-PCR infive of six cases, suggesting that this chromosomalimbalance may in fact be characteristic, althoughnot specific, for PMBL. Gains of the X chromosomehave been seen in different B-cell lymphoma types,but with a reported frequency of about only 30%(Hammond et al., 1992). Furthermore, as eachAP-PCR band originates from a particular chromo-somal locus, the finding that the same band (e.g.,band G of MCG1 fingerprint) showed gain ofintensity in four of the six cases points to theexistence of a common amplified region on the Xchromosome in PMBL. Interestingly, a candidate
TABLE 2. Results of AP-PCR Using AR-3 Primera
Band Chromosome
Case
1 2 3 4 5 6
B 1 s s s s s .
S 2 m . s m m m
C 3 s s s s s .
R0 3 s s s s s .
S3 3 s m s s s s
T3 3 s . s m m s
H 4 s s s s s s
Q 4 s s s s s s
A 5 s s s s s s
G 5 s s m m s s
N 5 m s s m s m
M 6 s s s s s .
S4 6 s m m s s s
L 7 s s s s s s
L1 7 s . s s s s
U 7 s s s s s .
R 8 s s s s . .
X 9 s . s m m m
D 15 s s s s s s
J 16 m . s m m s
E 17 s s s s s s
O 20 s m m s s s
R1 X s m s s s m
T1 X m s s m s m
aChange in intensity of the indicated AP-PCR bands is shown by: m, gain;., loss; s, no change.
TABLE 3. Results of AP-PCR Using MCG1 Primera
Band Chromosome
Case
1 2 3 4 5 6
Q0 1p m s s m s s
Q 1q m s s s m s
B1 2 s s s s s .
H 2 m s s s s s
P 2 m s s s s .
SO 6 m s s s . m
I 7 m m s m s m
R 7 s s s s s s
O 8q24.22 s s s s s .
D 8q24.3 s s s s s .
A 9q22.3 . s s s . .
B 11 s s s s s .
K 12 s s s s s s
S 12 m s s m s m
J 13q14.1–14.3 s m s s . s
E 13q31.32 . s s s s .
B0 16 s s s s s s
R0 17 s s s s m m
M 22 s s s s s s
B2 X s s s s s s
G X s m . m m m
aChange in intensity of the indicated AP-PCR bands are shown by: m,gain; ., loss; s, no change.
206 SCARPA ET AL.

oncogene has recently been identified on Xq22–24(Prosniak et al., 1998).
That additional chromosomes also have commonamplified regions in PMBL is evident by theanalysis of those chromosomes represented by atleast three AP-PCR fingerprint bands. For ex-ample, one of the five bands originating fromchromosome 7 showed sequence gains in four ofthe six cases (band I of MCG1 fingerprint), whilethe other four bands showed no change or a singleloss in each of two bands. Likewise, chromosome 2showed amplification at the same locus in fourPMBLs (band S of AR-3 fingerprint), but no
consistent change in the other three loci (bands B1,H, and P of MCG1 fingerprint).
Our data are consistent in many respects with theonly other genetic data available on PMBL (Joos etal., 1996). In that CGH study, amplification of9p23–24 was found in 50% of the cases. Our CGHanalysis also detected amplification of the short armof chromosome 9 in three of five cases, with aminimal common amplified region at 9p24–p22.Furthermore, as identified by AP-PCR, the amplifi-cations on chromosomes 2, 7, and X are additionalnonrandom events in PMBL, which is in agreementwith the previous CGH study (Joos et al., 1996). Inparticular, genetic overrepresentation was seen onthe short arm of chromosome 2, the long arm ofchromosome 7, and one region on each arm of the Xchromosome. Similarly, amplifications on chromo-somes 5, 12, and 16 were suggested to be nonran-dom events in PMBL by AP-PCR and were de-tected by CGH in about 25% of the cases (Joos etal., 1996). However, while both AP-PCR and CGHfound anomalies associated with the same chromo-somes, the former would appear to be more sensi-tive. In fact, our study on the same five casesrevealed 39 gains and 12 losses (10.2 imbalances percase) by AP-PCR and only 7 gains and 1 loss byCGH. Similarly, the CGH study involving 26 casesidentified 99 gains and 11 losses (4.2 per case; Jooset al., 1996). CGH detects imbalances involvinglarge chromosomal segments ($ 1 MB), unlesshigh-copy amplifications have occurred (Solinas-Toldo et al., 1996). These anomalies are likely to beless frequent than more modest genetic alterationsinvolving smaller chromosomal fragments detect-able by AP-PCR. This is clearly demonstrated byits ability to determine gender by the quantitativeamplification of sequences located on the X chromo-some. Thus, it can be postulated that the chromo-somal anomalies found by CGH are in fact morecommon in PMBL (e.g., X chromosome), as sug-gested by AP-PCR.
Further insight into the nature of the chromo-somal anomalies occurring in PMBL can be exem-plified by a more detailed analysis of the availabledata on chromosome 9. By AP-PCR, sequenceamplifications were detected in three of five cases,only one of which was also seen in CGH. This caneasily be explained by the fact that chromosome 9was represented by only two AP-PCR bands, oneoriginating from the long arm and the other withunknown sublocalization. Nonetheless, AP-PCRalso detected losses on this chromosome, suggest-ing that these imbalances may be a consequence ofmore complex phenomena, such as translocations
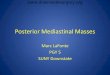
Figure 1. AP-PCR fingerprints from primary mediastinal B-lymphomapatients using AR-3 arbitrary primer. Case number is reported on thetop, where N and T indicate the lanes containing matched normal andtumor DNA, respectively. The bands composing the fingerprints areindicated by letters to the left, while their chromosomal origin isindicated to the right. nd, not determined. The arrows indicate selectedbands showing an increased (upward arrows) or decreased (downwardarrows) intensity in tumor with respect to normal DNA, after subtrac-tion of background. Note for example the disappearance of bandsoriginating from different sites of chromosome 7 in cases 2 and 6 (bandsL1 and U, respectively), and the gain in intensity of chromosome 9 (bandZ) in cases 4 and 6. The intensity of band T1 allows identification ofpatient gender, that is, corresponds to copy number of the X chromo-some in the template DNA. Patients 4 and 6 are males, whereas patients3 and 2 are females (see also Fig. 2). The amplification of the Xchromosome in the lymphomas of both male patients is also evident.Exposure times different from that shown in this picture allowed betterappreciation of the differences in particular bands.
207CHROMOSOMAL IMBALANCES IN PMBL

or other chromosomal rearrangements. It is worthnoting that case 6, which showed a loss in intensityof the AP-PCR bands generated from chromosome8, also had a MYC gene rearrangement of the typeseen in t(8;14) translocations of sporadic Burkitt’slymphomas (Scarpa et al., 1991).
In conclusion, molecular karyotyping using AP-PCR showed that nonrandom chromosomal anoma-lies occurring in PMBL include gains involving fiveautosomes (2, 5, 7, 9, 12) and sex chromosome X, ingood agreement with the findings obtained withCGH analysis on a larger panel of cases (Joos et al.,1996). Using a different technique, the presentstudy provides the first confirmation of the onlypublished study about cytogenetic anomalies inPMBL. Moreover, these nonrandom chromosomalanomalies may play a more central role in thepathogenesis of PMBL than previously expected.The same amplified chromosomal loci detectedby CGH may be affected by sequence gains ofsmaller chromosomal regions in a higher propor-tion of cases. Gains of chromosomal material havelong been known to be associated with neoplasia(Rabinowitz and Sachs, 1970; Spira et al., 1979;Klein, 1981). AP-PCR is highly sensitive at de-tecting moderate increases in copy number ofsmall chromosomal amplicons. These modest in-creases in genetic material may be as effective ashigher-level amplifications in disease pathogenesiswhen affecting sites where a proto-oncogene re-sides.
ACKNOWLEDGMENTS
This study is supported by a cofinanced grantfrom Verona University and Ministero Universita eRicerca Scientifica e Tecnologica to Fabio Menes-trina and a grant from Associazione Italiana Ricercasul Cancro, Milan, Italy. Maria G. Ennas is sup-ported by a grant from Regione Autonoma Sardaand from Cagliari University.
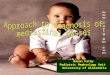
Figure 2. AP-PCR fingerprints from primary mediastinal B-lymphoma patients using MCG1 arbitrary primer. A portion of the gel isshown. Case number is reported on the top, where N and T indicate thelanes containing matched normal and tumor DNA, respectively. Thebands are identified by letters on the left and their chromosomal originon the right. The intensity of the G-bands in normal DNA allows
identification of patient gender as indicated, corresponding to copynumber of the X chromosome in the template DNA (see also band T1 ofFig. 1). Tumors 2, 4, 5, and 6 showed amplification and tumor 3 loss ofintensity in bands G, whereas tumor 1 showed no anomaly with respectto the intensity of matched normal DNA. The loss of intensity of band Ein tumor 1 and bands D and E in tumor 6 can also be noted.
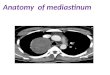
Figure 3. Results of CGH analysis on five primary mediastinal B-celllymphomas. Chromosomal gains are indicated by black bars on the rightof the chromosome ideogram. Losses are indicated by bars to the left ofthe ideograms. The profiles show the mean green-to-red fluorescenceratio along the chromosomes. The line in the middle of the profileindicates the base line ratio (1.0); the left and the right lines indicate ratiovalues of 0.75 and 1.25, taken as the threshold limits for chromosomallosses and gains, respectively.
208 SCARPA ET AL.

REFERENCES
Achille A, Biasi M, Zamboni G, Bogina G, Magalini A, Pederzoli P,Perucho M, Scarpa A. 1996. Chromosome 7q allelic losses inpancreatic carcinoma. Cancer Res 56:3808–3813.
Achille A, Baron A, Zamboni G, Di Pace C, Orlandini S, Scarpa A.1998. Chromosome 5 allelic losses are early events in tumors of thepapilla of Vater and occur at sites similar to those of gastric cancer.Br J Cancer 78:1653–1660.
Addis B, Isaacson P. 1986. Large cell lymphoma of the mediastinum:a B-cell tumour of probable thymic origin. Histopathology 10:379–390.
Davis R, Dorfman R, Warnke R. 1990. Primary large-cell lymphomaof the thymus. Hum Pathol 21:1262–1268.
Drwinga HL, Toji LH, Kim CH, Greene AE, Mulivor RA. 1993.NIGMS human/rodent somatic cell hybrid mapping panel 1 and 2.Genomics 16:311–314.
Du Manoir S, Speicher M, Joos S, Schrock E, Popp S, Dohner H,Kovacs G, Robert-Nicoud M, Lichter P, Cremer T. 1993. Detec-tion of complete and partial chromosome gains and losses bycomparative genomic in situ hybridization. Hum Genet 90:590–610.
Hammond DW, Goepel JR, Aitken M, Hancock BW, Potter AM,Goyns MH. 1992. Cytogenetic analysis of a United Kingdomseries of non-Hodgkin’s lymphomas. Cancer Genet Cytogenet61:31–38.
Hermsen M, Meijer G, Baak J, Joenje H, Walboomers J. 1996.Comparative genomic hybridization: a new tool in cancer pathol-ogy. Hum Pathol 27:342–349.
Ionov Y, Pineado MA, Malkhosyan S, Shibata D, Perucho M. 1993.Ubiquitous somatic mutations in simple repeated sequencesreveal a new mechanism for colonic carcinogenesis. Nature 363:558–561.
Joos S, Otano-Joos MI, Ziegler S, Bruderlein S, du Manoir S, BentzM, Moller P, Lichter P. 1996. Primary mediastinal (thymic) B-celllymphoma is characterized by gains of chromosomal materialincluding 9p and amplification of the REL gene. Blood 87:1571–1578.
Kallioniemi A, Kallioniemi OP, Sudar D, Rutovitz D, Gray JW,Waldman F, Pinkel D. 1992. Comparative genomic hybridizationfor molecular cytogenetic analysis of solid tumors. Science 258:818–821.
Klein G. 1981. The role of gene dosage and genetic transpositions incarcinogenesis. Nature 294:313–318.
Lazzarino M, Orlandi E, Paulli M, Strater J, Klersy C, Gianelli U,Gargantini L, Rousset MT, Gambacorta M, Marra E, Lavabre-Bertrand T, Magrini U, Manegold C, Bernasconi C, Moller P. 1997.Treatment outcome and prognostic factors for primary mediastinal(thymic) B-cell lymphoma: a multicenter study of 106 patients. JClin Oncol 15:1646–1653.
Malkhosyan S, Yasuda J, Soto J, Sekiya T, Yokota J, Perucho M. 1998.Molecular karyotype (amplotype) of metastatic colorectal cancerby unbiased arbitrarily primed PCR DNA fingerprinting. ProcNatl Acad Sci USA 95:10170–10175.
Menestrina F, Chilosi M, Bonetti F, Lestani M, Scarpa A, Novelli P,Doglioni C, Todeschini G, Ambrosetti A, Fiore Donati L. 1986.Mediastinal large-cell lymphoma of B-type, with sclerosis: histo-pathologic and immunohistochemical study of 8 cases. Histopathol-ogy 10:589–600.
Moller P, Lammler B, Eberlein-Gonska M, Feichter GE, HofmannWJ, Schmitteckert H, Otto HF. 1986. Primary mediastinal clearcell lymphoma of B-cell type. Virchows Arch A Pathol AnatHistopathol 409:79–92.
Moller P, Herrmann B, Moldenhauer G, Momburg F. 1987a. Defec-tive expression of MHC class I antigens is frequent in B-celllymphomas of high-grade malignancy. Int J Cancer 40:32–39.
Moller P, Moldenhauer G, Momburg F, Lammler B, Eberlein-Gonska M, Kiesel S, Dorken B. 1987b. Mediastinal lymphoma ofclear cell type is a tumor corresponding to terminal steps of B celldifferentiation. Blood 69:1087–1095.
Momburg F, Herrmann B, Moldenhauer G, Moller P. 1987. B-celllymphomas of high-grade malignancy frequently lack HLA-DR,-DP and -DQ antigens and associated invariant chain. Int J Cancer40:598–603.
Okazaki T, Takita J, Kohno T, Handa H, Yokota J. 1996. Detection ofamplified genomic sequences in human small-cell lung carcinomacells by arbitrarily primed-PCR genomic fingerprinting. HumGenet 98:253–258.
Paulli M, Lazzarino M, Gianelli U, Strater E, Orlandi E, Klersy C,Viglio A, Rosso R, Gambacorta M, Rousset T, Morra E, Lavabre-Bertrand T, Bernasconi C, Manegold C, Magrini U, Moller P. 1997.Primary mediastinal B-cell lymphoma: update of its clinicopatho-logic features. Leuk Lymphoma 26(suppl 1):115–123.
Peinado MA, Malkhosyan S, Velazquez A, Perucho M. 1992. Isola-tion and characterization of allelic losses and gains in colorectaltumors by arbitrary primed polymerase chain reaction. Proc NatlAcad Sci USA 89:10065–10069.
Prosniak M, Dierov J, Okami K, Tilton B, Jameson B, Sawaya BE,Gartenhaus RB. 1998. A novel candidate oncogene, MCT-1, isinvolved in cell cycle progression. Cancer Res 58:4233–4237.
Rabinowitz Z, Sachs L. 1970. Control of the reversion of propertiesin transformed cells. Nature 225:136–139.
Ried T, Baldini A, Rand T, Ward D. 1992. Simultaneous visualizationof seven different DNA probes by in situ hybridization usingcombinatorial fluorescence and digital image microscopy. ProcNatl Acad Sci USA 89:1388–1392.
Scarpa A, Bonetti F, Menestrina F, Menegazzi M, Chilosi M, LestaniM, Bovolenta C, Zamboni G, Fiore Donati L. 1987. Mediastinallarge-cell lymphoma with sclerosis: genotypic analysis establishesits B nature. Virchows Archiv 412:17–21.
Scarpa A, Borgato L, Chilosi M, Capelli P, Menestrina F, Bonetti F,Zamboni G, Pizzolo G, Hirohashi S, Fiore-Donati L. 1991.Evidence of c-myc gene abnormalities in mediastinal large B-celllymphoma of young adult age. Blood 78:780–788.
Solinas-Toldo S, Wallrapp C, Muller-Pillasch F, Bentz M, Gress T,Lichter P. 1996. Mapping of chromosomal imbalances in pancre-atic carcinoma by comparative genomic hybridization. Cancer Res56:3803–3807.
Speicher M, Jauch A, Jochum W, du Manoir S, Ried T, Walt H,Cremer T. 1995. Correlation of microscopic phenotype withgenotype in a formalin fixed, paraffin embedded testis tumorusing universal DNA amplification, comparative genomic hybrid-ization and interface cytogenetics. Am J Pathol 146:1332–1340.
Spira J, Wiener F, Ohno S, Klein G. 1979. Is trisomy cause orconsequence of murine T cell leukemia development? studies onRobertsonian translocation mice. Proc Natl Acad Sci USA 76:6619–6621.
Tsang P, Cesarman E, Chadburn A, Liu YF, Knowles DM. 1996.Molecular characterization of primary mediastinal B cell lym-phoma. Am J Pathol 148:2017–2025.
Yasuda J, Navarro JM, Malkhosyan S, Vealzquez A, Arribas R, SekiyaT, Perucho M. 1996. Chromosomal assignment of human DNAfingerprint sequences by simultaneous hybridization to arbitrarilyprimed PCR products from human/rodent monochromosome cellhybrids. Genomics 34:1–8.
Yousem S, Weiss L, Warnke R. 1985. Primary mediastinal non-Hodgkin’s lymphomas: a morphological and immunologic study.Am J Clin Pathol 83:676–680.
209CHROMOSOMAL IMBALANCES IN PMBL