Embed Size (px)
Citation preview

Noonan Syndrome in an Adult Family Presenting with
Chronic Lymphedema
MARVIN MILLER, M.D. ARNO C. MOTULSKY, M.D.
Seattle, Washington
From the Departments of Medicine and Genetics, and Center for Inherited Diseases, University of Washington, Seattle, Washington. This study was supported by U.S. Public Health Service Grant GM 15253. Requests for reprints should be addressed to Dr. Arno C. Motvlsky, Division of Medical Gs- netics, RG20, University of Washington. Seattle, Washitqton 98195. Manuscript accepted February 18, 1978.
A 27 year old man with multiple findlpgs of the Noonan syndrome (“male Turner” phenotype) presented with chronic lymphedema which was also present In his mother. Noonan syndrome should be considered in the differential diagnosis of chronic or familial lymphedema.
The Noonan syndrome is a well recongized condition in pediatrics characterized by congenital heart disease, webbed neck, short stature and occasional mental retardation. Since the Noonan syndrome fre- quently is transmitted as an autosomal dominant condition [ 11, an increasing number of adults with the Noonan phenotype are being detected. We would like to describe a family in whom lymphedema was the presenting feature that led to the diagnosis of the Noonan syndrome.
CASE REPORT
A 27 year old white man first noted edema of both legs from his knees down at age 16. Evaluation at that time showed chronic stasis edema of the legs, bilateral pes cavus and a short, webbed neck. Cardiac examination and roentgenograms of the skull and cervical spine disclosed no abnortnallties. He passed a physical examination for the army at age 17 but was discharged from military service because of the edema. The edema was painless and did not interfere with his work.
The findings on a Doppler examination of his legs at age 19 was interpreted as compatible with incompetent valves in his veins. The diagnosis of Milroy’s disease was entertained, and the patient was fitted with Jobst stockings and has been wearing them ever since. He is able to perform a vigorous daily exercise program and climbs mountains without any difficulty.
At age 27 he presented with the acute onset of fever, chills and pain in his left leg. He was found to have cellulitis of the left leg superimposed upon the chronic lymphedema. He responded well to antibiotic therapy.
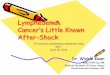
Physical examination showed a well developed man, 6 feet tall, of above average intelligence. A photograph of the proband is shown in Figure I. He had a webbed neck, low posterior hair line, generalized hirsutism, bilateral ptosis, dorsal kyphosis, thoracolumbar scoliosis, high arched palate, mild cubitus valgus, mild epicanthal folds, first degree hypospadias, atrophic right testicle with small left testicle, bilateral pes cavus, micrognathia and camptodactyly of the fifth fingers. There was significant nontender, bilateral woody edema from the knees down to the feet. He did not have distichiasis (double row of eyelashes). These findings suggested the diagnosis of Noonan syndrome. Cardiac examination showed normal first and second heart sounds, without murmurs, but a systolic ejection click was noted. Lateral and anteroposterior chest roentgenograms disclosed no abnormalities. An
August 1978 The Amerkan Joumnl ol Modkin. V&m@ 88 379

NOONAN SYNDROME AND CHRONIC LYMPHEDEMA-MILLER, MOTULSKY
Figure 1. Anteropos terior and lateral view of the proband showing we&bed neck, low posterior hair line, bilateral ptosis, downward slanting palpebral fissures, and micrognathia.
electrocardiogram showed a first, second and third heart sound pattern which was interpreted as a normal variant. Echocardiography showed prolapse of the mitral valve leaflet with no other abnormalities. An intravenous pyelogram showed large, extrarenal pelvices. Nonbanded chromosomes on peripheral blood lymphocytes showed 46/XY karyotype in 35 of 36 cells with 1 cell showing 45/XY which was thought to be artifactual hypodiplokty. Greater than 6 per cent XO/XY mosaicism was ruled out at the 95 per cent confidence level. Two R banded karyotypes and 4 nonbanded karyotypes showed no structural abnormalities. Sperm analysis on two different occasions showed complete azoospermia. Der- matoglyphics were unremarkable showing R-UL, RL, UL, UL, UL, L-W, RL, W, W, UL with no distal triradii.
A pedigree of the patient’s family is shown in Figure 2. The patient has one step sister by his mother who is normal. The patient’s mother had a history of chronic leg edema since age 7. She was thought to have elephantiasis and underwent several leg operations including a Kondoleon procedure as a child to correct the edema. The procedures were of little success. She still has a leg edema which, like her son’s, is not painful and does not interfere with her ambulation. She has had a total of two pregnancies and has no history of congenital heart disease. Neither of her parents or three other sisters had lymphedema, and she was born when her father was 27 years old. She has taken digitalis for long-standing paroxysmal atriil tachycardia which reverts to a normal sinus rhythm with a Valsalva maneuver. At age 63 she underwent an aortoiliac bypass for severe aortoiliac disease.
We examined the proband’s mother shortly after seeing
him. She was of normal stature and intelligence. There were no facial dysmorphisms, and there were no abnormalities of the neck. Cardiac examination showed normal first and second heart sounds without murmurs. Dermatoglyphics showed R-UL, UL, UL, UL, UL, L-RL, A, RL, W, UL with no distal triradii. Other than the lymphedema there were no other signs suggesting the Noonan syndrome. Photographs of her parents and three sisters showed no evidence of the Noonan syndrome. A photograph of the legs of the proband’s mother is shown in Figure 3. A chest film was within normal limits as was an echocardiogram which showed normal flows and echoes of the mitral valve. Since her evaluation, the pro- band‘s mother has required hospitalization for treatment of a skin ulcer over the lymphedematous part of her leg. An electrocardiogram showed a normal sinus rhythm except during episodes of palpitations which showed paroxysmal atrial tachycardia.
COMMENTS
We have interpreted the chronic lymphedema in this mother and son to be a part of the Noonan syndrome with the son having other stigmata of the syndrome, but the mother having no others. Pulmonic stenosis, short stature and mental retardation, three common features of the Noonan syndrome, were not present in either the proband or his mother. The proband had a prolapsed mitral valve, and we are aware of one other patient with the Noonan syndrome with this finding [2]. The signif- icance of this finding in Noonan syndrome remains
300 August 1978 The Amdcan Journal ol Medicine Volume 65

NOONAN SYNDROME AND CHRONIC LYMPHEDEMA-MILLER. MOTULSKY
heart disease
61 58
LEGEND-
0 l examined by authors
No evidence of Noonan syndrome by history or on examination of their pictures *
No evidence of Noonon syndrome by history *
-
Figure 2. Pedigree.
Noonan syndrome with chronic lymphederno + no evidence of lymphedemo, congemtol heart disease, short stature, webbed neck, mental deflclency, or dysmorphlc facial feotures.
unclear in view of the relatively high frequency of mitral valve prolapse 231.
The outstanding feature of the Noonan syndrome in these two affected persons is the chronic, long- standing, relatively nondisabling lymphedema of the legs. The lymphedema of the Noonan syndrome, like other primary familial edemas, can be present at birth or thereafter and usually persists. It is thought that the webbed neck seen in Noonan syndrome and in Turner syndrome reflects edema fluid that has collected in the neck and has been subsequently resorbed prenatally, leaving the once tight skin loose and webbed [4]. It is estimated that about 15 per cent of the subjects with the Noonan syndrome have edema [5]. Although the leg edema is usually not incapacitating, it predisposes to local infection as was demonstrated in the proband.
There is increasing evidence that the Noonan syn- drome is inherited as an autosomal dominant condition. Collins and Turner [6] described three cases of familial Noonan syndrome ascertained from 18 probands with the Noonan syndrome. In the series of Char et al. [ 71, of the 45 cases of Noonan syndrome, five were familial; three of these were mother to daughter transmission and two were affected siblings. These two series suggest that about seven-eighths of the cases of the Noonan syndrome are new mutations and one-eighth have a positive family history.
The relatively high proportion of affected subjects arising from new mutations is in accord with the low biologic fitness of the subjects with the Noonan syn-
Figure 3. Photograph showing bilateral woody edema of legs of proband’s mother.
August 1979 The American Journal of Mediclne Volume 65 391

NOONAN SYNDROME AND CHRONIC LYMPHEDEMA-MILLER, MOTULSKY
TABLE I Genetic Lymphedema Syndromes
Condition Inheritance Age ot Onset Associated Clinical Features’
Milroy’s disease [lo] Meige’s disease [ 111
Yellow nail syndrome [ 121 Distichiasis-lymphedema
syndrome [ 141
Autosomal dominant Autosomal dominant
Autosomal dominant Autosomal dominant
Noonan syndrome [l] Autosomal dominant
Lymphedema associated with cerebrovascular malformation [ 151
Lymphedema and cholestasis
I161 Turner syndrome [ 171
Lymphedema associated with ptosisx [ 181
Autosomal dominant
Autosomal recessive
Chromosomal-X0
Autosomal dominant
Congenital Puberty and later
Adults Puberty and later
Puberty and later
Puberty and later
Congenital or early childhood
Newborn period
Puberty
Pleural effusion, chylous ascites One pedigree suggestive of autosomal
recessive inheritance reported [lo] Dystrophic. yellow nails,+ pleural effusions [ 131 Extra row eyelashes,+ partial ectropion lower
lid, vertebral anomalies, webbed neck, spinal extra dural cysts
Facial dysmorphia, congenital heart disease, webbed neck, atrophic testes, short stature, mental deficiency
Cranial bruit frequent, primary pulmonary hypertension
Recurrent cholestastic jaundice+ described in Norwegian families
Edema of dorsum of hands and feet-usually resolves in months or years, coarctation of aorta, short stature, small chin, webbed neck
Ptosist
l Not all clinical features are present in each case of a given syndrome. + Constant feature of syndrome. $ This condition may be an expression of Noonan syndrome.
drome, particularly males, and is seen in other auto- somal dominant diseases such as achondroplasia. The low fitness arises from the congenital heart disease and infertility that are associated with the Noonan syndrome, both of which seem to be more common in affected males. Collins and Turner [6] described 11 of 15 males with cryptorchidism of which only one of five treated by orchiopexy had normal testes microscopically at sur- gery. In the same series, these investigators also re- ported a greater incidence of congenital heart disease in males (13 of 15) as compared to females (5 of 12). It is thus not surprising that in all three two-generation familial cases reported by Char and Turner, the gene was transmitted through a female. This is similar to our case. There are, however, familial cases of the Noonan syndrome transmitted through males [8,9]. Considering the fact that the diagnosis of Noonan syndrome is based on a constellation of clinical findings, etiologic heter- ogeneity is not unlikely so that not all sporadic cases of Noonan syndrome may be new mutations.
The differential diagnosis of lymphedema not ex- plained by infections, neoplasia, allergies, trauma or postthrombotic causes should include the nine genetic conditions listed in Table I. All are thought to result from absence or hypoplasia of lymphatic channels. Most are
l (0.008 X 0.1 X 0.08 X 2 = l/8,000)
transmitted as autosomal dominant traits and usually involve the lower extremities. A careful history re- garding age at onset, occurrence of jaundice and a physical examination with special attention to facial appearance, nails, eyelashes, cranial bruits and con- genital heart disease in conjunction with a careful family history (see Table I for details) readily allows diagnosis of the various syndromes.
Isolated cases of lymphedema without a family his- tory may be seen as new mutations, as chromosomal abnormalities (i.e., Turner syndrome) or in small families particularly with autosomal recessive inheritance. The various genetic lymphedema syndromes, therefore, should be considered in the differential diagnosis of every case of idiopathic lymphedema.
Using the facts that (1) the incidence of congenital heart disease is about 0.8 per cent [ 191, (2) the cause of about 10 per cent of congenital heart disease is isolated pulmonary stenosis [ 201, (3) about 8 per cent of all cases of isolated, congenital pulmonary stenosis occur in the Noonan syndrome [ 2 1 ] and (4) about 50 per cent of the subjects with the Noonan syndrome have pulmonic stenosis [ 221, a tentative calculation” for the frequency of the Noonan syndrome can be made which is about l/8,000. Since 15 per cent of the subjects with Noonan syndrome have lymphedema, it is important to recognize this finding as a possible presenting feature of this not uncommon syndrome.
332 August 1978 The American Journal of Medlclne Volume 65

2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
NOONAN SYNDROME AND CHRONIC LYMPHEDEMA-~-MILLER. MOTULSKY
REFERENCES
Nora JJ, Nora AN, Sinha AK, et al.: The Ullrich-Noonan syn- drome (Turner phenotype). Am J Dis Child 127: 48, 1976.
Towne WD. et al.: Systolic prolapse of the mitral valve in Noonan’s syndrome. Am Heart J 90: 499, 1975.
Devereux RB, Perloff JK, Reichek N, et al.: Mitral valve pro- lapse. Circulation 54: 3, 1976.
Sunderland WA: Fluid-filled pterygium colli (X0 Turner’s syndrome). Am J Dis Child 119: 352, 1970.
Minkin W, Frank SB, Wolman SR, et al.: Lymphedema in Noonan’s syndrome. Int J Dermatol 18: 179, 1974.
Collins E, Turner G: The Noonan syndrome-a review of the clinical and genetic features of 27 cases. J Pediatr 83: 941, 1973.
Char F. Fernandez HL, Scott Cl. et al.: The Noonan syn- drome-a clinical study of 45 cases. Proceedings of the Fourth Conference on the Clinical Delineation of Birth Defects, Part XV, The Cardiovascular System (Gergsma D, ed). Birth Defects 8: 110, 1972.
Baird PA, DeJong BP: Noonan’s syndrome (XX and XY Turner phenotype) in three generations of a family. J Pediatr 80: 110, 1972.
Bolton MR, Pugh DM, Mattioli LF, et al.: The Noonan syndrome: a family study. Ann Intern Med 80: 626, 1974.
Esterly JR: Congenital hereditary lymphedema. J Med Genet 2: 93, 1965.
Goodman RM: Familial lymphedema of the Meiges type. Am J Med 32: 651. 1962.
Wells GC: Yellow nail syndrome: with familial primary hypo-
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
plasia of lymphatics, manifest late in life. Proc R Sot Med 59: 447, 1966.
Zerfas AJ, Wallace HJ: Yellow nail syndrome with bilateral bronchiectasis. Proc R Sot Med 59: 448, 1966.
Robinow M, Johnson GF, Verhagen AD: Distichiasis-lym- phedema. Am J Dis Child 119: 343, 1970.
Avasthey P, Roy SB: Primary pulmonary hypertension, cere- brovascular malformation, and lymphoedema feet in a family. Br Heart J 30: 769, 1968.
Aagenaes 0: Hereditary recurrent cholestosis with lym- phoedema-two new families. Acta Paediatr Stand 63: 465, 1974.
Smith DW: Recognizable Patterns of Human Malformations. Genetic, Embryologic and Clinical Aspects, 2nd ed, Phila- delphia, W.B. Saunders, 1976, p 46.
Bloom D: Hereditary lymphedema (Nonne-Milroy-Meige). N Y J Med 41: 856, 1941.
Mitchess SC, Dorones SB. Berendes HW: Congenital heart disease in 56,109 births. Incidence and natural history. Circulation 43: 323, 1971.
Nadas AS, Fyler DC: Pediatric Cardiology, 3rd ed. Philadelphia, W.B. Saunders, 1972, p 534.
Celermajer JM, Bowdler JD, Cohen DH: Pulmonary stenosis in patients with Turner phenotype in the male. Am J Dis Child 116: 351, 1968.
Siggers DC. Polani PE: Congenital heart disease in male and female subjects, with somatic features of Turner’s syn- drome and normal sex chromosomes (Ullrich’s and related syndromes). Br Heart J 34: 41, 1972.
August 1978 The American Journal of Medicine Volume 65 383


















![[02] Lymphedema](https://img.pdfslide.net/doc/110x75/55cf8dfd550346703b8d6373/02-lymphedema.jpg)








