Embed Size (px)
Citation preview

MDFS/ Diabetic Foot Clinic Blueprint
Community Podiatry Blueprint (Foot Protection Service)
Primary Care Blueprint
(Click here)
At first diabetic visit Ad hoc GP appointment
Annual foot review GP out of hours
Initial assessment Referral from GP Referral other professional Referral from hospital/ MDFT
GP referral Attends A&E Sent to A&E from MDFT
Sent to A/E from Outpatients Referred to MDFT from ward
(Click here)
North West Coast Strategic Clinical Network
Diabetes Footcare Blueprint
Overall footcare pathway
(Click here)
October 2018 (to be reviewed June 2019)
Risk Stratification Tool(Click here)
Page 1
Forward
(Click here)

A Document or Template
Primary Care Foot Team
GP / Practice Secondary CareFoot Protection Service MDFT
A process step
Primary Care Footcare Blueprint
Contents:
· Blueprint· Foot Examination Template· Stratification Tool· Template forms
Blueprint key:
Colour code for responsible organisation:
Type of blueprint action: A sub-processA decision
pointStarting point
Click for Homepage
Back Forward
You are free to:
· Share - copy and redistribute the material in any medium or format · Adapt - remix, transform, and build upon the material
Attribution - You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may doso in any reasonable manner, but not in any way that suggests the licensor endorses you or your use:
“Adapted or adopted from the North West Coast Strategic Clinical Network (NWCSCN)”
Non-Commercial - You may not use the material for commercial purposes.
Full information https://creativecommons.org/licenses/by-nc/2.0/uk/
Attribution-Non Commercial 2.0 UK: England & Wales (CC BY-NC 2.0 UK)
Page 2

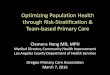
No neuropathy AND No limb ischaemia AND No skin changes or foot deformity AND No previous ulcer or amputation AND Not on renal replacement therapy
Neuropathy OR Non critical limb ischaemia OR Foot deformity OR Skin changes other than callus
Neuropathy + non critical limb ischaemia OR
Neuropathy + callus/deformity OR Non critical limb ischaemia + callus/
deformity OR Previous ulceration or amputation
OR On renal replacement therapy high risk of foot ulceration,
amputation and/ or premature death
Ulceration Suspected Charcot neuroarthropathy Cellulitis or spreading infection
Low
Moderate
High
Active foot disease
Recall for annual foot screening
Administer Foot Care Bundle
Refer IMMEDIATELY to acute services A/E and provide leaflet D
Diabetes Footcare Blueprint 2018
Acute foot attack
Active foot disease AND systemically ill Ulceration with limb ischaemia Critical limb ischaemia or gangrene Deep seated infection including
abscess or osteomyelitis
High Risk Feet
Moderate Risk Feet
Low Risk Feet
Looking After Your Foot Ulcer
Inpatient Foot Pathway
Outpatient Record Sheet
MDT Discharge Summary
Additional Information to MDFT after discharge from Emergency Floor
Focussed Foot Examination
Risk Stratification & Referral Form
Footcare Bundle
Forms and Guidance & Patient Information
GP/Primary Care
Community Podiatry (Foot Protection Service)
MDFT/ Diabetic Foot Clinic
Initial diagnosis of diabetes confirmed
at consultation with the patient in
primary care
Does the patient have any IMMEDIATE
foot problems?
Carry out a full foot
assessment immediately
Arrange up to 3 contact sessions with the practice nurse
to include:footcare education within 1
week
Patient attends primary/community
care appt
Complete Risk stratification
form, document risk and follow
risk stratification pathway
No
Complete initial foot assessment within 12 weeks
(either GP or community
podiatry team/ foot protection
service)
Patient attends with foot problem or foot problem detected at
Annual Review
Yes
Referral received from GP to Community Podiatry/ FPS:
Discharge Summary received from MDFT to Community Podiatry/ FPS:
Step down high or moderate risk, continued foot screening, Continued
management of stable foot ulcer
Local Community Podiatry/ Foot
Protection Service Referral method
Carry out a full foot
assessment
GP
FPS
Administer Footcare bundle & provide leaflet A-H as appropriate
Annual Foot Review - Ensure this is arranged
3
Refer to Community Podiatry/Foot Protection Service if not already known to them.
Administer Foot Care Bundle & leaflet A-H as appropriate
Guidance note: Ensure patient has appointment within 6-8 weeks. If already under Foot Protection Service then recall for assessment in 3-6 months
Refer to Community Podiatry/ Foot Protection Service if not already known to them.
Administer Foot Care Bundle & leaflet A-H as appropriate
Guidance note: Ensure patient has appointment within 2-4 weeks. If already under Foot Protection Service, then recall for assessment in 1-2 months (1-2 weeks if there is immediate concern)
Use local Community Podiatry/ Foot Protection Service Referral method
And/OR
Copy of Form 2 to GP
ALERT
If concerns of vascular compromise, in the
absence of foot ulcer - follow vascular
pathway (click here)
Same day referral to Hospital Multidisciplinary Foot/Diabetic Foot Clinic. Patient to be seen by MDFT within 1 working day. Provide leaflet D
Risk Stratification and Referral
Form to MDFT
Discharge Letter Following Inpatient Stay
Inpatient stay for management of foot ulcer (must be seen by MDFT
within 72 hours before or after discharge)
Referred from GP/other healthcare practitioner
Referred via Foot Protection Service
Patient presents with foot problem at A&E
Hospital entry via MDFT Clinic
Referred from GPReferred from FPS
Assessment of patients feet(as per Trust decision aid)
Admission required for foot disease
Admission not required for foot disease
Discharged back to GP and FPS with standard discharge summary
plus form 8
Initiate management/treatment, if any required
Refer to MDFT with local/standard discharge
summary plus form 7
Assessment of patients feet(as per Trust policy)
Admission required for foot disease
Admission not required for foot disease
Discharged back to GP
and FPS
Patient with diabetes admitted
for any other reason
Problem detected?
Monitor as part of pressure area care
Outpatient management of foot ulcer (must be seen by MDFT within 1 working
day)
Legs and feet MUST be checked
within 24 hours
No
Yes
Hospital Entry
Foot screening and risk stratification toolFoot screening and risk stratification tool
To view/download forms, please click the appropriate number/letter
October 2018 revision
Click for Homepage
Back Forward
A
B3
C3
D
D
2
2
1
1
6
2
6
5
8
47
1
1
2
3
4
5
6
7
8
A
B
C
D
Click here to access the Claudication and Neuropathic Pain Assessment
Page 3
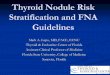
NICE GUIDANCE NG19annotated on Primary Care, Community/FPS, Hospital Blueprints & Forms/guidance & Patient Information
Quality standard QS6 quality statement 5
Quality standard QS6 quality statement 6

Refer to Community Podiatry/Foot Protection Service if not already known to them.
Administer Foot Care Bundle & leaflet A-H as appropriate
Same day referral to Hospital Multidisciplinary Foot/Diabetic Foot Clinic. Patient to be seen by MDFT within 1 working day. Provide leaflet D
No neuropathy AND No limb ischaemia AND No skin changes or foot deformity
AND No previous ulcer or amputation
AND Not on renal replacement therapy
Neuropathy OR Non critical limb ischaemia OR Foot deformity OR Skin changes other than callus
Neuropathy + non critical limb ischaemia OR
Neuropathy + callus/deformity OR Non critical limb ischaemia +
callus/deformity OR Previous ulceration or amputation
OR On renal replacement therapyhigh risk of foot ulceration, amputation and/ or premature death
Ulceration Suspected Charcot
neuroarthropathy Cellulitis or spreading infection
Low
Moderate
High
Active foot disease
Refer to Community Podiatry/ Foot Protection Service if not already known to them.
Administer Foot Care Bundle & leaflet A-H as appropriate
Send directly to emergency services A/E and provide
leaflet D
Primary Care Footcare Blueprint 2018
ALERT
If concerns of vascular compromise, in the
absence of foot ulcer - follow vascular
pathway (click here)
Acute foot attack
Active foot disease AND systemically ill
Ulceration with limb ischaemia Critical limb ischaemia or
gangrene Deep seated infection including
abscess or osteomyelitis
Risk Stratification and Referral
Form to MDFT
GP/Primary Care
Community Podiatry (Foot Protection Service)
MDFT/ Diabetic Foot Clinic
GP
MDFT
FPS
Roles and Responsibilities
To assess new diabetes patients feet
Utilise risk stratification tool
READ code appropriate activity
Receive and act upon the GP referral within appropriate
timescales
Provide discharge information as required - Inform GP practice
Receive and act upon the GP referral within appropriate
timescales
Provide discharge information as required - Inform GP practice
Patient
Inform the GP of any foot problems
Attend any appointment
Receive information leaflets
Initial diagnosis of diabetes confirmed
at consultation with the patient in
primary care
Does the patient have any IMMEDIATE
foot problems?
Carry out a full foot
assessment immediately
Arrange up to 3 contact sessions with the practice nurse to include:footcare education within 1 week
Yes
Patient attends primary/
community care appt.
Complete Risk stratification
form, document risk and follow
risk stratification pathway
Complete initial foot assessment within 12 weeks
(either GP or community podiatry team/ foot protection service)
No
Yes
Guidance note: Ensure patient has appointment within 6-8 weeks. If already under Foot Protection Service then recall for assessment in 3-6 months
Guidance note: Ensure patient has appointment within 2-4 weeks. If already under Foot Protection Service, then recall for assessment in 1-2 months (1-2 weeks if there is immediate concern)
Patient attends with foot problem or foot problem detected at
Annual Review
Foot screening and risk stratification toolFoot screening and risk stratification tool
Administer Footcare bundle & provide leaflet A-H as appropriate
Annual Foot Review - Ensure this is arranged
Use local Community Podiatry/ Foot Protection Service Referral method
Copy of Form 2 to GP
D
D
Click for Homepage
Back Forward
1
2
3 A
3 B
3 C
2
Page 4
NG191.3.3
NG191.3.3
NG191.3.6
as per NG19 - 1.2.2
as per NG19 - 1.2.3
NG191.3.7
NG191.3.8
NG191.3.9
NG191.3.9
NG191.4.2
NG191.4.1
High Risk Feet
Moderate Risk Feet
Low Risk Feet
Looking After Your Foot Ulcer
Inpatient Foot Pathway
Outpatient Record Sheet
MDT Discharge Summary
Additional Information to MDFT after discharge from Emergency Floor
Focussed Foot Examination
Risk Stratification & Referral Form
Footcare Bundle
Forms and Guidance & Patient Information
Discharge Letter Following Inpatient Stay
To view/download forms, please click the appropriate number/letter
1
2
3
4
5
6
7
8
A
B
C
D
Click here to access the Claudication and Neuropathic Pain Assessment

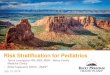
Community Podiatry/ Foot Protection Service Footcare Blueprint 2018
GP
MDFT/Hospital
FPS
Roles and Responsibilities
Refer appropriate patients
To receive patient discharge
summary and code on GP clinical system.
Manage active foot ulceration
Discharge mod /high back to FPS
Provide discharge information to GP/FPS
Review patient within appropriate
timescales
Receive and act upon discharge
information or referral
Patient
Ensure that appointments are kept
Contact GP or FPS if any new
problems occur
Referral received from GP to Community Podiatry/ FPS:
Discharge Summary received from MDFTto Community Podiatry/ FPS:
Step down high or moderate risk, continued foot screening, Continued management of stable foot ulcer and
housebound
Recall for assessment in 3-6 months Administer Foot Care Bundle & leaflet A-H as
appropriate
Or, if stable ulcer, continue ongoing monitoring
No neuropathy AND No limb ischaemia AND No skin changes or foot deformity
AND No previous ulcer or amputation
AND Not on renal replacement therapy
Neuropathy OR Non critical limb ischaemia OR Foot deformity OR Skin changes other than callus
Neuropathy + non critical limb ischaemia OR
Neuropathy + callus/deformity OR Non critical limb ischaemia +
callus/deformity OR Previous ulceration or amputation
OR On renal replacement therapyhigh risk of foot ulceration, amputation and/ or premature death
Ulceration Suspected Charcot
neuroarthropathy Cellulitis or spreading infection
Low
Moderate
High
Active foot disease
Recall for assessment in 1-2 months the frequency might be increased to 1-2 weeks if there is immediate concern for those at higher risk
Administer Foot Care Bundle & leaflet A-H as appropriate
Send directly to emergency services A/E and provide
leaflet D
ALERT
If concerns of vascular compromise, in the
absence of foot ulcer - follow vascular
pathway (click here)
Acute foot attack
Active foot disease AND systemically ill
Ulceration with limb ischaemia Critical limb ischaemia or
gangrene Deep seated infection including
abscess or osteomyelitis
Risk Stratification and Referral
Form to MDFT
GP/Primary Care
Community Podiatry (Foot Protection Service)
MDFT/ Diabetic Foot Clinic
Foot screening and risk stratification toolFoot screening and risk stratification tool
Adminster Footcare bundle & leaflet A-H as appropriate
Annual Foot Review - Ensure this is arranged
Copy of Form 2 to GP
Local Community Podiatry/ Foot
Protection Service Referral method
Carry out a full foot
assessment
Risk stratify and document
risk
Same day referral to Hospital Multidisciplinary Foot/Diabetic Foot Clinic. Patient to be seen by MDFT within 1 working day. Provide leaflet D
D
D
2
Click for Homepage
Back Forward
6
12
A3
B3
3 C
2
Page 5
as per NG19 - 1.2.2
as per NG19 - 1.2.3
as per NG19 - 1.2.1
as per NG19 - 1.2.1 & 1.3.8
as per NG19 – 1.3.8
NG191.3.6
NG19 1.3.10
NG191.3.11
NG191.3.11
NG191.3.7
NG191.3.11
NG191.4.2
NG191.4.1
High Risk Feet
Moderate Risk Feet
Low Risk Feet
Looking After Your Foot Ulcer
Inpatient Foot Pathway
Outpatient Record Sheet
MDT Discharge Summary
Additional Information to MDFT after discharge from Emergency Floor
Focussed Foot Examination
Risk Stratification & Referral Form
Footcare Bundle
Forms and Guidance & Patient Information
Discharge Letter Following Inpatient Stay
To view/download forms, please click the appropriate number/letter
1
2
3
4
5
6
7
8
A
B
C
D
Click here to access the Claudication and Neuropathic Pain Assessment

Inpatient stay for management of foot ulcer
(must be seen by MDFT within 72 hours before or
after discharge)
Referred from GP/other healthcare practitioner
Referred via Foot Protection Service
Patient presents with foot problem at A&E
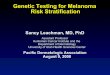
Hospital Care Footcare Blueprint 2018
GP
MDFT
FPS
Roles and Responsibilities
Receive patient discharge summary and code on
GP clinical system.
Identify a named consultant for patient care
Provide timely follow-up appointment
Completion of referral/ discharge forms
Refer to FPS for ongoing management/
continued screening on discharge
Review patient within appropriate timescales
Receive an act upon discharge information or
referral
Patient
Ensure that appointments are kept
Contact GP or Foot protection service if any new
problems occur
Hospital entry via MDFT Clinic
Referred from GPReferred from FPS
Assessment of patients feet
(as per Trust
decision aid)
Admission required for foot disease
Admission not required for foot
disease
Discharged back to GP and FPS with standard
discharge summary plus form 8
Initiate management/treatment, if any
required
Refer to MDFT with local/standard discharge
summary plus form 7
Assessment of patients feet
(as per Trust policy)
Admission required for foot
disease
Admission not required for foot
disease
Discharged back to GP and FPS
Patient with diabetes admitted for any other reason
Problem detected?
Monitor as part of pressure area care
Outpatient management of foot ulcer (must be seen by MDFT within 1 working
day)
Hospital Entry via A&E/AMUHospital Entry via A&E/AMU
Legs and feet MUST be checked
within 24 hours
Yes
No
Click for Homepage
Back Forward
7
48
5 6
1
Page 6
NG191.1.1
as per NG19 - 1.2.2
as per NG19 - 1.2.3 & accessing other services according to 1.2.4
NG191.6.8
NG191.7.3
NG191.6.8
NG191.3.3.
NG191.3.4.
NG19 1.1.3:assessment within 24hrs and MDT within 24hrs of examination
NG19 1.1.2:named consultant for overall care
NG19 1.1.3: transfer responsibility to a consultant member of the MDFT service if a diabetic foot problem is the dominant factor for inpatient care
High Risk Feet
Moderate Risk Feet
Low Risk Feet
Looking After Your Foot Ulcer
Inpatient Foot Pathway
Outpatient Record Sheet
MDT Discharge Summary
Additional Information to MDFT after discharge from Emergency Floor
Focussed Foot Examination
Risk Stratification & Referral Form
Footcare Bundle
Forms and Guidance & Patient Information
Discharge Letter Following Inpatient Stay
To view/download forms, please click the appropriate number/letter
1
2
3
4
5
6
7
8
A
B
C
D
Click here to access the Claudication and Neuropathic Pain Assessment

RISK STRATIFICATION TOOL
Low Risk
Moderate Risk
High Risk
Active Foot Disease
Acute Foot Attack
DEFINITION· No neuropathy AND· No limb ishaemia AND· No skin changes or foot deformity AND· No previous ulcer or amputation· Not on renal replacement therapy
· Neuropathy OR· Non critical limb ischaemia OR· Foot deformity Or· Skin changes other than callus
· Neuropathy + non critical limb ischaemia OR· Neuropathy + callus/deformity OR· Non critical limb ischaemia + callus/deformity
OR· Previous ulceration or amputation OR· On renal replacement therapy
· Ulceration· Suspected Charcot neuroarthropathy· Cellulitis or spreading infection
· Active foot disease AND systemically ill· Ulceration with limb ischaemia· Critical limb ischaemia or gangrene· Deep seated infection including abscess
or osteomyelitis
ACTION
· Administer Foot Care Bundle· Recall for Annual Foot Screening
· Administer Foot Care Bundle· Refer to Foot Protection Service – Ensure
patient has appointment within 6-8 weeks
· Administer Foot Care Bundle· Refer to Foot Protection Service – Ensure
patient has appointment within 2-4 weeks
· Administer Foot Care Bundle· Refer IMMEDIATELY to acute services
· Administer Foot Care Bundle· Refer to Foot Protection Service – Ensure
patient has appointment within 1 working day
FOOT CARE BUNDLE· Document risk level for each foot individually· Inform patient of risk for each foot individually· Provide general foot care advice· Provide Foot Care Information Leaflets based on individual risk· Provide emergency contact numbers in case of development of acute foot problems
Click for Homepage
Back Forward
LEVEL OF RISK
Page 7
Supporting NG19 1.3.6
NG191.3.7.
NG191.3.8 &
1.3.9
NG191.3.8 &
1.3.9

AClick for Homepage
Back Forward
Click To Download
Click To Download
Page 8

BClick for Homepage
Back Forward
Page 9
Supporting NG19 1.3.13& 1.4.3
Click To Download
Click To Download

CClick for Homepage
Back Forward
Page 10
Supporting NG19 1.3.13& 1.4.3
Click To Download
Click To Download

DClick for Homepage
Back Forward
Page 11
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 12
NG19 1.3.4 & supporting
1.5.1
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 13
Supporting NG19 1.5.1
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 14
NG191.3.7
Click To Download
Click To Download

Click for Homepage
Back Forward
Click for Homepage
Page 15
NG191.1.1, 1.5.1& supporting1.5.4, 1.6.1, 1.6.2
NG191.6.8
NG191.7.11.7.4
NG191.7.11.7.4
NG191.7.2
Back Forward
Click To Download
Click To Download
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 16
NG191.5.2
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 17
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 18
SupportingNG19 1.5.13
Click To Download
Click To Download

Click for Homepage
Back Forward
Page 19
SupportingNG19 1.5.13
Click To Download
Click To Download

Click for Homepage
Page 20
Back
Click To Download
Click To Download
Click To Download
Click To Download
Click To Download
Click To Download