Embed Size (px)
Citation preview

California Hospital Association1215 K Street, Suite 800Sacramento, CA 95814
916-443-7401www.calhospital.org
Hospital Council of Northern & Central California1215 K Street, Suite 730Sacramento, CA 95814
916-552-7608www.hospitalcouncil.net

LEADERSHIPL E T T E R
Dear Members:
On behalf of our boards of directors, we appreciate your leadership and involvementwith our associations.
Our hospitals and health systems face unprecedented challenges, and the stakes are high.Membership gives your hospital or health system a seat at the table and a voice in the crucial conversations about the future. Your participation has never been more importantand we thank you for your continued support.
Together, as four associations representing 450 California hospitals, we have a far morepowerful presence in Washington, D.C, Sacramento and locally than any single hospitalor system could achieve alone. Together, we champion issues that matter to you — fromreimbursement and policy reform to patient safety and quality — and with the tangibleresults outlined here. For every dollar of dues you paid in 2012, we generated a returnof over $150 for hospitals and health systems statewide.
This report highlights the 2012 successes achieved by the California Hospital Associationand Hospital Council of Northern and Central California in collaboration with each ofyou. Please join me in thanking Duane Dauner, Art Sponseller and their capable staffs forthe outstanding work they do.
Sincerely,
Steven J. Packer, MDCommunity Hospital of the Monterey Peninsula
2012 CHA Chair
John Sigsbury, President/CEOEmanuel Medical Center
2012 Hospital Council Chair
3
BY THE NUMBERS:HOSPITAL SAVINGS / REVENUE FROM ASSOCIATION-LED ADVOCACY, PROGRAMS AND INITIATIVES
30-Month Hospital Fee Program (paid in 2012)
Six-Month Hospital Fee Program (paid in 2012)
Preliminary injunction to challenge Medi-Cal rate reductions to hospital-based skilled nursing facilities
Patient Safety First initiative to improve hospital quality outcomes in six key areas and save lives
Saved more than 973 lives by reducing sepsis infections
Defeated legislation threatening non-profit status for hospitals and other non-profits
Defeated legislation that would have created additional categories for licensure violations
Workers’ Compensation legislative win
Documentation and Coding Adjustment, IPPS Final Rule
Member fee savings on services, publications and educational offerings statewide
$562 Million
$858 Million
$125 Million
$19 Million+
Immeasurable
Immeasurable
$52 Million
$100 - $250 Million
$435 Million
$3 Million

LEADERSHIPL E T T E R
Dear Members:
On behalf of our boards of directors, we appreciate your leadership and involvementwith our associations.
Our hospitals and health systems face unprecedented challenges, and the stakes are high.Membership gives your hospital or health system a seat at the table and a voice in the crucial conversations about the future. Your participation has never been more importantand we thank you for your continued support.
Together, as four associations representing 450 California hospitals, we have a far morepowerful presence in Washington, D.C, Sacramento and locally than any single hospitalor system could achieve alone. Together, we champion issues that matter to you — fromreimbursement and policy reform to patient safety and quality — and with the tangibleresults outlined here. For every dollar of dues you paid in 2012, we generated a returnof over $150 for hospitals and health systems statewide.
This report highlights the 2012 successes achieved by the California Hospital Associationand Hospital Council of Northern and Central California in collaboration with each ofyou. Please join me in thanking Duane Dauner, Art Sponseller and their capable staffs forthe outstanding work they do.
Sincerely,
Steven J. Packer, MDCommunity Hospital of the Monterey Peninsula
2012 CHA Chair
John Sigsbury, President/CEOEmanuel Medical Center
2012 Hospital Council Chair
3
BY THE NUMBERS:HOSPITAL SAVINGS / REVENUE FROM ASSOCIATION-LED ADVOCACY, PROGRAMS AND INITIATIVES
30-Month Hospital Fee Program (paid in 2012)
Six-Month Hospital Fee Program (paid in 2012)
Preliminary injunction to challenge Medi-Cal rate reductions to hospital-based skilled nursing facilities
Patient Safety First initiative to improve hospital quality outcomes in six key areas and save lives
Saved more than 973 lives by reducing sepsis infections
Defeated legislation threatening non-profit status for hospitals and other non-profits
Defeated legislation that would have created additional categories for licensure violations
Workers’ Compensation legislative win
Documentation and Coding Adjustment, IPPS Final Rule
Member fee savings on services, publications and educational offerings statewide
$562 Million
$858 Million
$125 Million
$19 Million+
Immeasurable
Immeasurable
$52 Million
$100 - $250 Million
$435 Million
$3 Million

whomever happens to be that person’s employer,whether the employer is a non-profit organization,small business or investor-owned organization. CHAalso successfully opposed adding volunteers to the listof mandatory child abuse reporters.
Penalties for Licensing ViolationsCHA successfully defeated SB 1246 (Hernandez), whichwould have imposed financial penalties on hospitals forlicensing violations, including violations of PatientClassification Systems and staffing ratios. Potentialsavings of more than $52 million to Californiahospitals.
Workers’ CompensationCHA stopped AB 808 (Skinner), which, for purposes ofqualifying for workers’ compensation benefits, wouldhave created a presumption that any MRSA infectionacquired by a hospital employee was acquired on thejob. Annual savings: $100 million to $250 millionfor workers’ compensation claims by hospitalemployees.
Safe Patient HandlingCHA has been an early and active participant in thepre-regulatory process initiated by Cal/OSHA to imple-ment AB 1136, the Safe Patient Handling law. Earlydiscussions yielded positive interpretations, includingno requirement to utilize lift teams and the ability ofnurses to delegate observation and direction of patienthandling activities. Annual savings: Hundreds ofthousands of dollars in staffing costs avoidedby these interpretations.
CHA’S LEADERSHIP OFFERS TOOLS,ADVOCACY AND A SEAT AT THE TABLEFOR HOSPITALSTransforming for TomorrowWith the assistance of Deloitte Consulting LLP, CHA’sTransforming for Tomorrow Task Force served as athink tank to develop transformational strategies forhospitals and provided recommendations for CHA’spublic policy development to support hospitals’strategic goals.
The Task Force’s final report includes core, differentia-tion and contingent strategies for hospitals and aTransformation Roadmap with resources to assist hospitalsto identify a path for the future and design a tailoredapproach to strategic planning. CHA provided hospitals
with a web seminar series that thoroughly reviewedeach of the major areas of the Transforming forTomorrow program. In December, hospitals received aTransformation Manual and hospital-specific informationfrom the research and data fact base. The informationand materials will continue to be shared and discussedthrough CHA’s committees and policy centers andthrough regional and section meetings. Benefit tohospitals: Tailored information and strategiesfor future direction.
Clinical Laboratory ScientistsCHA was instrumental in the enactment of SB 289(Hernandez, E), which allows hospitals to form trainingconsortiums and work together to train ClinicalLaboratory Scientists (CLS). The costs associated withtraining this hard-to-fillposition can rangefrom $55,000 to$100,000 per trainee;under SB 289, hospitalsare permitted to joinforces to train CLSs,thereby reducing thecost to the individualhospitals. Savings tohospitals in the hun-dreds of thousandsof dollars.
DataSuite ReportsCHA continued to deliver powerful information-based,hospital-specific analysis that models the impact ofMedicare proposed and final rules, proposed and finallegislative changes, and prospective payment systemreport sets for inpatient, outpatient, rehabilitation,skilled-nursing, psychiatric and long-term care payments.This year CHA delivered enhanced reporting on qualitymeasures, including the impact of Medicare’s Value-BasedPurchasing program and the Readmission Reductionprogram. DataSuite Reports put hospital financial andquality data in the hospitals’ hands, in a format that isready to use for strategic planning, budgeting, decisionmaking and advocacy.
Seismic Safety Mandate ReliefCHA successfully encouraged the Committee on Budgetto place language in the Governor’s budget bill AB 1467(Chapter 23, Statutes of 2012), which extended thedeadline for an SB 90 (Chapter 19, Statutes of 2011)letter of intent and schedule to be moved from the
CHA RETURNS REAL MONEY TO HOSPITALS VIA THE HOSPITAL FEE PROGRAMSThe hospital fee programs are the largest influx of new money into the Medi-Cal program since theinception of Medicaid in California, and the Californiaprogram is the largest amount ever approved by theCenters for Medicare & Medicaid Services (CMS).CHA’s efforts on the three hospital fee programswill bring in a total of $8.16 billion into Californiahospitals. The hospital fee programs increase Medi-Cal payments at a time when there is simply no alter-native way to do so.
Six-Month Hospital Fee CHA successfully led the development and implemen-tation of the six-month hospital fee program, resultingin $858 million in new federal funds to improve thehealth care system with supplemental Medi-Cal paymentsto hospitals. The program also provided the state with$210 million in new funding for health care coveragefor children and General Fund savings. Net benefitto California hospitals: $858 million for the six-month program, paid in 2012.
30-Month Hospital Fee Program The 30-month hospital fee program is expected toprovide hospitals with an overall net benefit of $4.6billion once fully implemented. In addition, the programprovides $1.2 billion of support to the state for children’shealth care coverage and General Fund savings.
The 30-month hospital fee program builds on thesuccessful foundation of the prior two programs.Unlike the first two programs, the 30-month hospitalfee program decouples the fee-for-service paymentsfrom the managed care component of the program.The legislation (AB 1476) bifurcating the two compo-nents of the hospital fee program was signed into lawin June of 2012 and allows an earlier implementationof the fee-for-service component as well as the abilityfor hospitals to book the associated revenue in fiscalyear 2012. CHA also worked with the Department ofHealth Care Services to delay the collection of $562million in fees until CMS approves the managed carecomponent of the program in 2013. Net benefit toCalifornia hospitals: $4.6 billion for the periodJuly 1, 2011, through December 31, 2013 and$562 million in improved cash flow for calendaryear 2012.
CHA’S LEGAL ADVOCACY SAVES HOSPITALS MILLIONS IN COSTSCHA secured a preliminaryinjunction to challengeMedi-Cal rate reductionsto hospital-based skillednursing facilities by aprojected 23 percent.Estimated statewideincreased revenue of$125 million.
Meal and Rest Period Law CHA filed an amicus brief with the California SupremeCourt advocating for a reasonable interpretation ofCalifornia’s meal and rest period laws. The CaliforniaSupreme Court’s decision in the Brinker Restaurant casewas largely favorable for employers. Annual savings ofmillions of dollars of potential missed meal andrest period premium payments, and extensivelitigation costs.
CHA’S SUCCESSFUL ADVOCACY DEFEATSCOSTLY, BAD BILLS FOR HOSPITALSHealth Plan NetworkCHA successfully opposed SB 1373 (Lieu), in whichhospitals would have been prohibited from claiming tobe in a health plan’s network unless all physicians pro-viding care in the hospital were also contracted withthe health plan. In addition, hospitals would have beenrequired to disclose to patients prior to care that someof the physicians might be out-of-network and providecost estimates for the hospital and physicians’ services.Finally, the bill would have established punitive alternativereimbursement if a hospital failed to make the requireddisclosures. Benefit to California hospitals: Millionsof dollars in administrative savings and prevent-ing reduced reimbursement.
Protecting Non-Profit StatusCHA led the effort to protect non-profit organizationsfrom automatically losing their non-profit status becauseof an independent criminal act of an employee or personassociated with the organization. AB 1564 (Lara) wouldhave automatically revoked an organization’s non-profitstatus, including hospitals, if an employee failed tocomply with the law regarding child abuse reporting.CHA successfully argued that there is no nexus betweenthe independent criminal act of an employee and
4 5

whomever happens to be that person’s employer,whether the employer is a non-profit organization,small business or investor-owned organization. CHAalso successfully opposed adding volunteers to the listof mandatory child abuse reporters.
Penalties for Licensing ViolationsCHA successfully defeated SB 1246 (Hernandez), whichwould have imposed financial penalties on hospitals forlicensing violations, including violations of PatientClassification Systems and staffing ratios. Potentialsavings of more than $52 million to Californiahospitals.
Workers’ CompensationCHA stopped AB 808 (Skinner), which, for purposes ofqualifying for workers’ compensation benefits, wouldhave created a presumption that any MRSA infectionacquired by a hospital employee was acquired on thejob. Annual savings: $100 million to $250 millionfor workers’ compensation claims by hospitalemployees.
Safe Patient HandlingCHA has been an early and active participant in thepre-regulatory process initiated by Cal/OSHA to imple-ment AB 1136, the Safe Patient Handling law. Earlydiscussions yielded positive interpretations, includingno requirement to utilize lift teams and the ability ofnurses to delegate observation and direction of patienthandling activities. Annual savings: Hundreds ofthousands of dollars in staffing costs avoidedby these interpretations.
CHA’S LEADERSHIP OFFERS TOOLS,ADVOCACY AND A SEAT AT THE TABLEFOR HOSPITALSTransforming for TomorrowWith the assistance of Deloitte Consulting LLP, CHA’sTransforming for Tomorrow Task Force served as athink tank to develop transformational strategies forhospitals and provided recommendations for CHA’spublic policy development to support hospitals’strategic goals.
The Task Force’s final report includes core, differentia-tion and contingent strategies for hospitals and aTransformation Roadmap with resources to assist hospitalsto identify a path for the future and design a tailoredapproach to strategic planning. CHA provided hospitals
with a web seminar series that thoroughly reviewedeach of the major areas of the Transforming forTomorrow program. In December, hospitals received aTransformation Manual and hospital-specific informationfrom the research and data fact base. The informationand materials will continue to be shared and discussedthrough CHA’s committees and policy centers andthrough regional and section meetings. Benefit tohospitals: Tailored information and strategiesfor future direction.
Clinical Laboratory ScientistsCHA was instrumental in the enactment of SB 289(Hernandez, E), which allows hospitals to form trainingconsortiums and work together to train ClinicalLaboratory Scientists (CLS). The costs associated withtraining this hard-to-fillposition can rangefrom $55,000 to$100,000 per trainee;under SB 289, hospitalsare permitted to joinforces to train CLSs,thereby reducing thecost to the individualhospitals. Savings tohospitals in the hun-dreds of thousandsof dollars.
DataSuite ReportsCHA continued to deliver powerful information-based,hospital-specific analysis that models the impact ofMedicare proposed and final rules, proposed and finallegislative changes, and prospective payment systemreport sets for inpatient, outpatient, rehabilitation,skilled-nursing, psychiatric and long-term care payments.This year CHA delivered enhanced reporting on qualitymeasures, including the impact of Medicare’s Value-BasedPurchasing program and the Readmission Reductionprogram. DataSuite Reports put hospital financial andquality data in the hospitals’ hands, in a format that isready to use for strategic planning, budgeting, decisionmaking and advocacy.
Seismic Safety Mandate ReliefCHA successfully encouraged the Committee on Budgetto place language in the Governor’s budget bill AB 1467(Chapter 23, Statutes of 2012), which extended thedeadline for an SB 90 (Chapter 19, Statutes of 2011)letter of intent and schedule to be moved from the
CHA RETURNS REAL MONEY TO HOSPITALS VIA THE HOSPITAL FEE PROGRAMSThe hospital fee programs are the largest influx of new money into the Medi-Cal program since theinception of Medicaid in California, and the Californiaprogram is the largest amount ever approved by theCenters for Medicare & Medicaid Services (CMS).CHA’s efforts on the three hospital fee programswill bring in a total of $8.16 billion into Californiahospitals. The hospital fee programs increase Medi-Cal payments at a time when there is simply no alter-native way to do so.
Six-Month Hospital Fee CHA successfully led the development and implemen-tation of the six-month hospital fee program, resultingin $858 million in new federal funds to improve thehealth care system with supplemental Medi-Cal paymentsto hospitals. The program also provided the state with$210 million in new funding for health care coveragefor children and General Fund savings. Net benefitto California hospitals: $858 million for the six-month program, paid in 2012.
30-Month Hospital Fee Program The 30-month hospital fee program is expected toprovide hospitals with an overall net benefit of $4.6billion once fully implemented. In addition, the programprovides $1.2 billion of support to the state for children’shealth care coverage and General Fund savings.
The 30-month hospital fee program builds on thesuccessful foundation of the prior two programs.Unlike the first two programs, the 30-month hospitalfee program decouples the fee-for-service paymentsfrom the managed care component of the program.The legislation (AB 1476) bifurcating the two compo-nents of the hospital fee program was signed into lawin June of 2012 and allows an earlier implementationof the fee-for-service component as well as the abilityfor hospitals to book the associated revenue in fiscalyear 2012. CHA also worked with the Department ofHealth Care Services to delay the collection of $562million in fees until CMS approves the managed carecomponent of the program in 2013. Net benefit toCalifornia hospitals: $4.6 billion for the periodJuly 1, 2011, through December 31, 2013 and$562 million in improved cash flow for calendaryear 2012.
CHA’S LEGAL ADVOCACY SAVES HOSPITALS MILLIONS IN COSTSCHA secured a preliminaryinjunction to challengeMedi-Cal rate reductionsto hospital-based skillednursing facilities by aprojected 23 percent.Estimated statewideincreased revenue of$125 million.
Meal and Rest Period Law CHA filed an amicus brief with the California SupremeCourt advocating for a reasonable interpretation ofCalifornia’s meal and rest period laws. The CaliforniaSupreme Court’s decision in the Brinker Restaurant casewas largely favorable for employers. Annual savings ofmillions of dollars of potential missed meal andrest period premium payments, and extensivelitigation costs.
CHA’S SUCCESSFUL ADVOCACY DEFEATSCOSTLY, BAD BILLS FOR HOSPITALSHealth Plan NetworkCHA successfully opposed SB 1373 (Lieu), in whichhospitals would have been prohibited from claiming tobe in a health plan’s network unless all physicians pro-viding care in the hospital were also contracted withthe health plan. In addition, hospitals would have beenrequired to disclose to patients prior to care that someof the physicians might be out-of-network and providecost estimates for the hospital and physicians’ services.Finally, the bill would have established punitive alternativereimbursement if a hospital failed to make the requireddisclosures. Benefit to California hospitals: Millionsof dollars in administrative savings and prevent-ing reduced reimbursement.
Protecting Non-Profit StatusCHA led the effort to protect non-profit organizationsfrom automatically losing their non-profit status becauseof an independent criminal act of an employee or personassociated with the organization. AB 1564 (Lara) wouldhave automatically revoked an organization’s non-profitstatus, including hospitals, if an employee failed tocomply with the law regarding child abuse reporting.CHA successfully argued that there is no nexus betweenthe independent criminal act of an employee and
4 5

the high cost of new graduate hospital orientation andtraining programs, and provide a valuable resource forhospitals to prepare for the expected exodus of seniornurses as the economy recovers. TPPs are now beingdeveloped in non-traditional areas, primary care, homecare, hospice and school nursing to prepare the nursingworkforce for health care reform.
Representation on the California WorkforceInvestment BoardThe California Workforce Investment Board (Board) is aprivate-sector led body tasked with advising the governoron jobs and workforce development. Over the pasttwo years, CHA has worked closely with the state toimprove health sector representation on the board. Asa result, in 2012, the Board appointed three hospitalmembers representing a cross section of hospital typesand sizes.
FFY 2013 IPPS Final Rule – Documentation and Coding AdjustmentIn response to advocacy by CHA, CMS chose not toimplement a proposed additional 0.8 percent prospectivedocumentation adjustment that would have resulted inan additional $1.19 billion loss in hospital paymentsnationally. CMS finalized an overall rate increase ofapproximately 2.3 percent for FFY 2013 in hospitalinpatient payments, or about $435 million forCalifornia hospitals relative to FFY 2012.
CHA Center for Post-Acute Care CHA established the Center for Post-Acute Care to provide improved support and advocacy for all CHAmembership in the context of health care reform andthe changing health care delivery system. The newCenter provides representation for member providersthroughout the post-acute care continuum, includinghospital-based skilled nursing facilities (SNFs), inpatientrehabilitation facilities (IRFs), long-term, acute-care
hospitals (LTCHs), and hospital and health systemhome health agencies (HHAs) and hospices.
Establishment of a Functional PlanUpdating the facilities component of Title 22 and proposing changes to the 2013 California BuildingStandards Code was the focus of CHA’s advocacy forthe adoption of a Functional Plan prior to project sub-mission to OSHPD. The incorporation of the FunctionalPlan concept into the 2013 California Building StandardsCode should result in millions of dollars of savings byreducing project delays.
The Functional Plan program allows a hospital owner toincorporate the latest 21st century medical treatmentsand technology into a construction/renovation projectby explaining how the project will address operationaland physical functionality. This will enable the CaliforniaDepartment of Public Health (CDPH) Licensing programand OSHPD to approve the functionality of a projectprior to the start of construction, thereby avoidingexpensive delays.
Institutions for Mental Diseases (IMD) DemonstrationCHA’s Center for Behavioral Health played a pivotalrole in ensuring California was one of the states selectedto participate in the three-year Medicaid EmergencyPsychiatric Demonstration program, established underthe Affordable Care Act. Four freestanding acute psy-chiatric hospitals falling under the federal Institutionsfor Mental Diseases (IMD) exclusion criteria will testwhether Medi-Cal beneficiaries experiencing a psychiatricemergency get more immediate and appropriate carewhen IMD receives Medicaid reimbursement.
This demonstration will provide federal Medicaidmatching funds for emergency care provided toMedicaid enrollees ages 21 to 64 who have an acuteneed for treatment. The goals include:
• Expanding coverage (by increasing the numberof inpatient facilities where services are Medi-Calreimbursable)
• Controlling costs (by reducing patient boarding inmedical emergency rooms and inpatient units andreducing emergency care costs to local hospitalsand other emergency service agencies)
• Improving the delivery system (by reducing out-of-county psychiatric facility placements and facilitatingmore rapid and appropriate clinical services for individuals in crisis)
March 31, 2012 deadline to September 30, 2012, thesame date hospital HAZUS reports were due to OSHPD.SB 90 allows hospitals to seek an extension for seismiccompliance up to seven years based on three elements:1) structural integrity of the building; 2) loss of essentialhospital services to the community if the hospital isclosed; or 3) financial hardship. The later deadlineallowed 25 hospitals with a total of 64 SPC-1 buildingsto be eligible for an extension under SB 90. This actionprevented 25 hospitals from being reported to Licensingand potentially being closed for not being in compliancewith the seismic mandate. The 2012 approval of the30-month hospital fee triggered the extension authorizedunder SB 90.
Measures Reduction – Inpatient andOutpatient Quality Reporting Programs
CHA has long advocated forthe removal of several unreli-able CMS quality measuresto ease the burden of theinpatient quality reportingprogram for hospitals. Inresponse to CHA and others’advocacy, CMS for the firsttime removed 17 measuresfrom the program, including
the claims-based Medicare Healthcare Acquired Conditions(HACs) and Agency for Healthcare Quality and Researchinpatient quality indicators that have been problematic.Also in response to CHA and others’ advocacy, CMS didnot propose any additional quality measures for theOutpatient Quality Reporting Program in the CY2013proposed rule.
Food and Water Storage FlexibilityOSHPD proposed rigorous food and water standards forthe 2013 California Building Standards Code update,under the Hospital Facilities Seismic Safety Act. TheCHA/OSHPD Work Group proposed water and foodstorage code changes; the accepted changes allow forflexibility in meeting the standards. California hospitalswill save millions of dollars with the optionsfor food and water storage in the 2013California Building Standards Code.
Risk Management ToolsCHA’s member tools provide hospitals and healthsystems fast, accurate updates on state and federalchanges. The New Conditions of Participation - CHA’s
Crosswalk On What You Need to Know assists memberhospitals and health systems with their interpretationand implementation of the newly revised Conditionsof Participation (CoPs), (CMS-3244-P, 5/16/12) thatMedicare- and Medicaid-enrolled hospitals must abideby to participate in the federal health care programs.Due to numerous comments, CMS suspended therequirement that hospital governing bodies include amember of the medical staff. Hospitals are not expectedto comply with this revision until CMS has addressedthe issue.
CHA Guidelines for Standing Orders, StandardizedProcedures and Other Delegation Tools provides guid-ance and practical parameters to assist member hospitals with less frequently used order sets, includingstanding orders, standardized procedures, protocols,preformatted/preprinted orders and written instruc-tions. Three descriptive sections for each order typedefine the order set, describe the use of the order setand provide additional guidance applicable toMedicare or Medi-Cal.
Quality and Patient Safety ToolsCHA’s Medication Safety Committee continues to createeffective tools for hospital members. This year thecommittee developed The High Alert AnticoagulationMedication Guideline, summarizing safe-use practices forheparin, warfarin and enoxaparin. Anticoagulation ishigh-risk therapy that involves complex dosing andstringent monitoring, as well as ensuring patientadherence in the outpatient setting.
Nursing WorkforceCHA’s collaboration with the California Institute forNursing and Health Care on the realization of theInstitute of Medicine’s Future of Nursing Report hasyielded more than 26 new nurse Transition to Practice
Programs (TPP) communityschool-based initiatives totrain and increase employa-bility of newly licensed RNs.These programs increasenew graduate skills andcompetencies and bridgeacademia to practice withoutcreating a financial burdenon hospitals and health sys-tems. TPPs allow hospitals tofast-track a newly employedRN into staffing, lowering
6 7

the high cost of new graduate hospital orientation andtraining programs, and provide a valuable resource forhospitals to prepare for the expected exodus of seniornurses as the economy recovers. TPPs are now beingdeveloped in non-traditional areas, primary care, homecare, hospice and school nursing to prepare the nursingworkforce for health care reform.
Representation on the California WorkforceInvestment BoardThe California Workforce Investment Board (Board) is aprivate-sector led body tasked with advising the governoron jobs and workforce development. Over the pasttwo years, CHA has worked closely with the state toimprove health sector representation on the board. Asa result, in 2012, the Board appointed three hospitalmembers representing a cross section of hospital typesand sizes.
FFY 2013 IPPS Final Rule – Documentation and Coding AdjustmentIn response to advocacy by CHA, CMS chose not toimplement a proposed additional 0.8 percent prospectivedocumentation adjustment that would have resulted inan additional $1.19 billion loss in hospital paymentsnationally. CMS finalized an overall rate increase ofapproximately 2.3 percent for FFY 2013 in hospitalinpatient payments, or about $435 million forCalifornia hospitals relative to FFY 2012.
CHA Center for Post-Acute Care CHA established the Center for Post-Acute Care to provide improved support and advocacy for all CHAmembership in the context of health care reform andthe changing health care delivery system. The newCenter provides representation for member providersthroughout the post-acute care continuum, includinghospital-based skilled nursing facilities (SNFs), inpatientrehabilitation facilities (IRFs), long-term, acute-care
hospitals (LTCHs), and hospital and health systemhome health agencies (HHAs) and hospices.
Establishment of a Functional PlanUpdating the facilities component of Title 22 and proposing changes to the 2013 California BuildingStandards Code was the focus of CHA’s advocacy forthe adoption of a Functional Plan prior to project sub-mission to OSHPD. The incorporation of the FunctionalPlan concept into the 2013 California Building StandardsCode should result in millions of dollars of savings byreducing project delays.
The Functional Plan program allows a hospital owner toincorporate the latest 21st century medical treatmentsand technology into a construction/renovation projectby explaining how the project will address operationaland physical functionality. This will enable the CaliforniaDepartment of Public Health (CDPH) Licensing programand OSHPD to approve the functionality of a projectprior to the start of construction, thereby avoidingexpensive delays.
Institutions for Mental Diseases (IMD) DemonstrationCHA’s Center for Behavioral Health played a pivotalrole in ensuring California was one of the states selectedto participate in the three-year Medicaid EmergencyPsychiatric Demonstration program, established underthe Affordable Care Act. Four freestanding acute psy-chiatric hospitals falling under the federal Institutionsfor Mental Diseases (IMD) exclusion criteria will testwhether Medi-Cal beneficiaries experiencing a psychiatricemergency get more immediate and appropriate carewhen IMD receives Medicaid reimbursement.
This demonstration will provide federal Medicaidmatching funds for emergency care provided toMedicaid enrollees ages 21 to 64 who have an acuteneed for treatment. The goals include:
• Expanding coverage (by increasing the numberof inpatient facilities where services are Medi-Calreimbursable)
• Controlling costs (by reducing patient boarding inmedical emergency rooms and inpatient units andreducing emergency care costs to local hospitalsand other emergency service agencies)
• Improving the delivery system (by reducing out-of-county psychiatric facility placements and facilitatingmore rapid and appropriate clinical services for individuals in crisis)
March 31, 2012 deadline to September 30, 2012, thesame date hospital HAZUS reports were due to OSHPD.SB 90 allows hospitals to seek an extension for seismiccompliance up to seven years based on three elements:1) structural integrity of the building; 2) loss of essentialhospital services to the community if the hospital isclosed; or 3) financial hardship. The later deadlineallowed 25 hospitals with a total of 64 SPC-1 buildingsto be eligible for an extension under SB 90. This actionprevented 25 hospitals from being reported to Licensingand potentially being closed for not being in compliancewith the seismic mandate. The 2012 approval of the30-month hospital fee triggered the extension authorizedunder SB 90.
Measures Reduction – Inpatient andOutpatient Quality Reporting Programs
CHA has long advocated forthe removal of several unreli-able CMS quality measuresto ease the burden of theinpatient quality reportingprogram for hospitals. Inresponse to CHA and others’advocacy, CMS for the firsttime removed 17 measuresfrom the program, including
the claims-based Medicare Healthcare Acquired Conditions(HACs) and Agency for Healthcare Quality and Researchinpatient quality indicators that have been problematic.Also in response to CHA and others’ advocacy, CMS didnot propose any additional quality measures for theOutpatient Quality Reporting Program in the CY2013proposed rule.
Food and Water Storage FlexibilityOSHPD proposed rigorous food and water standards forthe 2013 California Building Standards Code update,under the Hospital Facilities Seismic Safety Act. TheCHA/OSHPD Work Group proposed water and foodstorage code changes; the accepted changes allow forflexibility in meeting the standards. California hospitalswill save millions of dollars with the optionsfor food and water storage in the 2013California Building Standards Code.
Risk Management ToolsCHA’s member tools provide hospitals and healthsystems fast, accurate updates on state and federalchanges. The New Conditions of Participation - CHA’s
Crosswalk On What You Need to Know assists memberhospitals and health systems with their interpretationand implementation of the newly revised Conditionsof Participation (CoPs), (CMS-3244-P, 5/16/12) thatMedicare- and Medicaid-enrolled hospitals must abideby to participate in the federal health care programs.Due to numerous comments, CMS suspended therequirement that hospital governing bodies include amember of the medical staff. Hospitals are not expectedto comply with this revision until CMS has addressedthe issue.
CHA Guidelines for Standing Orders, StandardizedProcedures and Other Delegation Tools provides guid-ance and practical parameters to assist member hospitals with less frequently used order sets, includingstanding orders, standardized procedures, protocols,preformatted/preprinted orders and written instruc-tions. Three descriptive sections for each order typedefine the order set, describe the use of the order setand provide additional guidance applicable toMedicare or Medi-Cal.
Quality and Patient Safety ToolsCHA’s Medication Safety Committee continues to createeffective tools for hospital members. This year thecommittee developed The High Alert AnticoagulationMedication Guideline, summarizing safe-use practices forheparin, warfarin and enoxaparin. Anticoagulation ishigh-risk therapy that involves complex dosing andstringent monitoring, as well as ensuring patientadherence in the outpatient setting.
Nursing WorkforceCHA’s collaboration with the California Institute forNursing and Health Care on the realization of theInstitute of Medicine’s Future of Nursing Report hasyielded more than 26 new nurse Transition to Practice
Programs (TPP) communityschool-based initiatives totrain and increase employa-bility of newly licensed RNs.These programs increasenew graduate skills andcompetencies and bridgeacademia to practice withoutcreating a financial burdenon hospitals and health sys-tems. TPPs allow hospitals tofast-track a newly employedRN into staffing, lowering
6 7

HIGHLIGHTSSummitThe Hospital Council con-vened 108 members and 94 sponsors and staff at itssuccessful Annual Summit inSan Francisco, featuringpower-packed meetingagendas and multiple net-working opportunities.Attendees congratulated theHospital Council for raisingthe bar and producing out-standing conferences yearafter year. Visit the HospitalCouncil website at www.hospitalcouncil.net/photo-slideshow/2012-hospital-council-summit-photos toview the photo gallery fromthis event.
CHPACThe Hospital Council raised more than $330,000 forthe California Hospital Association Political ActionCommittee. The Hospital Council also supportedCHPAC through two hosted events in Sacramento andChico, with representation from local officials.
Health Care Heroes Awards• San Francisco: In July, the San Francisco Business Times
and the Hospital Council held the Second AnnualHealth Care Heroes Awards. More than 30 finalists—chosen from more than 100 nominees—were hon-ored for their tireless commitment to health care.
• Santa Clara: The HospitalCouncil hosted the Second Annual Health Care Heroes Awards in May, partnering with the Silicon Valley Business Journal. Twenty-five finalists were nominated for their outstanding contribu- tions to the health care field in the categories of Administration, Board Member, Community
Advocate, Future Leader,Nurse and Provider. More than 215 people
attended the event.
• Sacramento: Also in May, the Hospital Councilpartnered with the Sacramento Business Journal topresent the first Health Care Heroes awards in theSacramento region. Leaders and physicians from allfour health care systems in the area were nominatedas award recipients. All of the inspiring events refo-cused on the core mission of member hospitals—patient care and community health.
STATE AND FEDERAL ADVOCACYHospital Council Increases MemberEngagement in State and Federal Advocacy• Through legislative briefings, launched collaboration
and opened the lines of communication among local,state and federal elected officials and staff, hospitalexecutives, physician leaders and business leaders,among others.
• Hosted section meetings with local, state and federalelected officials to discuss health care reform, resultingin relationship-building opportunities and improvedaccess to government officials.
• Led health care participation in two annual chamberadvocacy events in Washington, D.C., allowing delegates 32 meetings with elected officials and their staff to help promote fiscal responsibility andsustainability in the health care sector.
• In collaboration with CHA and the Council’sHealthcare Laboratory Workforce Initiative (HLWI),proposed and supported SB 289 to allow ClinicalLaboratory Science (CLS) training programs to formconsortiums, thereby allowing hospitals to becomeclinical training sites, sharing the financial burdenand responsibilities of training. The governorapproved the bill in September.
• Provided ongoing advocacy for hospitals related to thegovernance and financial operation of the state-pro-posed expansion of managed care into 25 counties inthe Hospital Council region. The CaliforniaDepartment of Health Care Services intends to enrollcurrent Medi-Cal beneficiaries, Healthy Families, dualeligibles and Medicaid Expansion beneficiaries. TheHospital Council and CHA provided recommendationsto the state, emphasizing the importance of communityinvolvement, county options for a plan provider, holdharmless reimbursement, a longer planning and coor-dination period before implementation, the fragilenature of the rural provider network, and demonstrationof community support by bidding health plans. The
8 9
Hospital Council also provided ongoing advocacy withrural counties in the north state to add Lake, Humboldt,Del Norte, Trinity, Shasta, Siskiyou, Modoc, Lassenand Tehama to the existing COHS (county-operatedhealth system) operated by Partnership HealthPlan ofCalifornia.
LOCAL ADVOCACYHospital Council Helps Ensure LocalGovernment Policies and Actions SupportHospitals• By increasing community awareness, defeated an
effort to create a seven-bed congregate living healthfacility (CLHF) connected to an ambulatory surgerycenter, thus creating a small specialty hospital in SanJose. Hospital Council sent a representative to speakagainst the appeal for a CLHF at the San Jose PlanningCommission, formed a coalition of various health careproviders to speak against the project, and worked withthe area’s State Assembly Member to obtain a letterfrom California Department of Public Health outliningwhy the CLHF should not be licensed. The applicantwithdrew its application as a result of this advocacy.
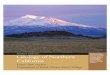
• Led the development of four economic impact studiesand presented them in their respective communities.The studies showed that in just 14 counties, hospitalsrepresent a total annual economic impact of $48 billionand 300,000 jobs. Additional studies will be done inFresno, Madera, Contra Costa, Alameda and Solanocounties.
• Convened hospital executives, community stakeholdersand local government officials to build alliances, shareinformation on facilities, programs and key issues, andaccelerate hospital and health system readiness forhealth care reform throughout the region in: Alameda,Butte, Colusa, Contra Costa, Fresno, Glenn, Kern,Lassen, Modoc, Monterey, Plumas, Santa Cruz, SanBenito, San Francisco, Shasta, Sierra, Siskiyou, Solano,Tehama and Trinity counties.
• Presented an overview of the Economic ImpactAnalysis commissioned by the Hospital Council and allthe hospitals in Santa Clara County at the County ofSanta Clara Economic Summit on Health Care, alongwith Stanford Hospital and Kaiser Permanente.
• Led a delegation from Fresno to visit San Antonio,Texas to view firsthand the innovative and highly successful methods of the City of San Antonio in integrating its mental health, substance abuse andcriminal justice systems. The Hospital Council continuesto work with this delegation to find similar solutionsfor Fresno.
• Improved care transitions for the Medicare fee-for-service population in Kern County through collabora-tion between hospitals and community partners lead-ing to the CMS Community-Based Care TransitionProgram grant. Participating hospitals gathered root-cause analysis data on readmissions and worked withPartners in Care Foundation to aggregate the data toidentify community interventions and submit thegrant application.
• The Hospital Council’s advocacy led to CMS awardingSan Francisco one of four Transitional Care Grantsgiven in California. The Hospital Council hostednumerous meetings of the hospitals to collect the nec-essary data and funded a grant writer to assist in thegrant preparation. This joint effort convinced CMS toaward San Francisco the grant, which will fund athree-year study on the effectiveness of various sup-portive programs to reduce readmissions of thosedischarged to a home setting.
• Organized a Billing Committee in San Francisco withrepresentatives from all local hospitals to discuss waysto improve patient satisfaction with the billing process.UCSF has introduced a “one bill” system that includeshospital, physician and any other associated services.San Francisco hospitals continue to work towardincreasing patient satisfaction scores throughimprovement of billing systems.
COUNTY/AREA JOBS LABOR INCOME OUTPUT
Santa Clara 64,000 $5.9 Billion $14.3 Billion
San Joaquin Valley 52,101 $2.9 Billion $6.7 BillionSan JoaquinAmadorCalaverasStanisiausTuolumneMerced
Greater Sacramento 84,176 $5.3 Billion $11.7 BillionSacramentoYoloPlacerEl DoradoYubaSutter
San Francisco 98,994 $7.2 Billion $15.2 Billion
Totals 299,271 $21.3 Billion $47.9 Billion

HIGHLIGHTSSummitThe Hospital Council con-vened 108 members and 94 sponsors and staff at itssuccessful Annual Summit inSan Francisco, featuringpower-packed meetingagendas and multiple net-working opportunities.Attendees congratulated theHospital Council for raisingthe bar and producing out-standing conferences yearafter year. Visit the HospitalCouncil website at www.hospitalcouncil.net/photo-slideshow/2012-hospital-council-summit-photos toview the photo gallery fromthis event.
CHPACThe Hospital Council raised more than $330,000 forthe California Hospital Association Political ActionCommittee. The Hospital Council also supportedCHPAC through two hosted events in Sacramento andChico, with representation from local officials.
Health Care Heroes Awards• San Francisco: In July, the San Francisco Business Times
and the Hospital Council held the Second AnnualHealth Care Heroes Awards. More than 30 finalists—chosen from more than 100 nominees—were hon-ored for their tireless commitment to health care.
• Santa Clara: The HospitalCouncil hosted the Second Annual Health Care Heroes Awards in May, partnering with the Silicon Valley Business Journal. Twenty-five finalists were nominated for their outstanding contribu- tions to the health care field in the categories of Administration, Board Member, Community
Advocate, Future Leader,Nurse and Provider. More than 215 people
attended the event.
• Sacramento: Also in May, the Hospital Councilpartnered with the Sacramento Business Journal topresent the first Health Care Heroes awards in theSacramento region. Leaders and physicians from allfour health care systems in the area were nominatedas award recipients. All of the inspiring events refo-cused on the core mission of member hospitals—patient care and community health.
STATE AND FEDERAL ADVOCACYHospital Council Increases MemberEngagement in State and Federal Advocacy• Through legislative briefings, launched collaboration
and opened the lines of communication among local,state and federal elected officials and staff, hospitalexecutives, physician leaders and business leaders,among others.
• Hosted section meetings with local, state and federalelected officials to discuss health care reform, resultingin relationship-building opportunities and improvedaccess to government officials.
• Led health care participation in two annual chamberadvocacy events in Washington, D.C., allowing delegates 32 meetings with elected officials and their staff to help promote fiscal responsibility andsustainability in the health care sector.
• In collaboration with CHA and the Council’sHealthcare Laboratory Workforce Initiative (HLWI),proposed and supported SB 289 to allow ClinicalLaboratory Science (CLS) training programs to formconsortiums, thereby allowing hospitals to becomeclinical training sites, sharing the financial burdenand responsibilities of training. The governorapproved the bill in September.
• Provided ongoing advocacy for hospitals related to thegovernance and financial operation of the state-pro-posed expansion of managed care into 25 counties inthe Hospital Council region. The CaliforniaDepartment of Health Care Services intends to enrollcurrent Medi-Cal beneficiaries, Healthy Families, dualeligibles and Medicaid Expansion beneficiaries. TheHospital Council and CHA provided recommendationsto the state, emphasizing the importance of communityinvolvement, county options for a plan provider, holdharmless reimbursement, a longer planning and coor-dination period before implementation, the fragilenature of the rural provider network, and demonstrationof community support by bidding health plans. The
8 9
Hospital Council also provided ongoing advocacy withrural counties in the north state to add Lake, Humboldt,Del Norte, Trinity, Shasta, Siskiyou, Modoc, Lassenand Tehama to the existing COHS (county-operatedhealth system) operated by Partnership HealthPlan ofCalifornia.
LOCAL ADVOCACYHospital Council Helps Ensure LocalGovernment Policies and Actions SupportHospitals• By increasing community awareness, defeated an
effort to create a seven-bed congregate living healthfacility (CLHF) connected to an ambulatory surgerycenter, thus creating a small specialty hospital in SanJose. Hospital Council sent a representative to speakagainst the appeal for a CLHF at the San Jose PlanningCommission, formed a coalition of various health careproviders to speak against the project, and worked withthe area’s State Assembly Member to obtain a letterfrom California Department of Public Health outliningwhy the CLHF should not be licensed. The applicantwithdrew its application as a result of this advocacy.
• Led the development of four economic impact studiesand presented them in their respective communities.The studies showed that in just 14 counties, hospitalsrepresent a total annual economic impact of $48 billionand 300,000 jobs. Additional studies will be done inFresno, Madera, Contra Costa, Alameda and Solanocounties.
• Convened hospital executives, community stakeholdersand local government officials to build alliances, shareinformation on facilities, programs and key issues, andaccelerate hospital and health system readiness forhealth care reform throughout the region in: Alameda,Butte, Colusa, Contra Costa, Fresno, Glenn, Kern,Lassen, Modoc, Monterey, Plumas, Santa Cruz, SanBenito, San Francisco, Shasta, Sierra, Siskiyou, Solano,Tehama and Trinity counties.
• Presented an overview of the Economic ImpactAnalysis commissioned by the Hospital Council and allthe hospitals in Santa Clara County at the County ofSanta Clara Economic Summit on Health Care, alongwith Stanford Hospital and Kaiser Permanente.
• Led a delegation from Fresno to visit San Antonio,Texas to view firsthand the innovative and highly successful methods of the City of San Antonio in integrating its mental health, substance abuse andcriminal justice systems. The Hospital Council continuesto work with this delegation to find similar solutionsfor Fresno.
• Improved care transitions for the Medicare fee-for-service population in Kern County through collabora-tion between hospitals and community partners lead-ing to the CMS Community-Based Care TransitionProgram grant. Participating hospitals gathered root-cause analysis data on readmissions and worked withPartners in Care Foundation to aggregate the data toidentify community interventions and submit thegrant application.
• The Hospital Council’s advocacy led to CMS awardingSan Francisco one of four Transitional Care Grantsgiven in California. The Hospital Council hostednumerous meetings of the hospitals to collect the nec-essary data and funded a grant writer to assist in thegrant preparation. This joint effort convinced CMS toaward San Francisco the grant, which will fund athree-year study on the effectiveness of various sup-portive programs to reduce readmissions of thosedischarged to a home setting.
• Organized a Billing Committee in San Francisco withrepresentatives from all local hospitals to discuss waysto improve patient satisfaction with the billing process.UCSF has introduced a “one bill” system that includeshospital, physician and any other associated services.San Francisco hospitals continue to work towardincreasing patient satisfaction scores throughimprovement of billing systems.
COUNTY/AREA JOBS LABOR INCOME OUTPUT
Santa Clara 64,000 $5.9 Billion $14.3 Billion
San Joaquin Valley 52,101 $2.9 Billion $6.7 BillionSan JoaquinAmadorCalaverasStanisiausTuolumneMerced
Greater Sacramento 84,176 $5.3 Billion $11.7 BillionSacramentoYoloPlacerEl DoradoYubaSutter
San Francisco 98,994 $7.2 Billion $15.2 Billion
Totals 299,271 $21.3 Billion $47.9 Billion

• With its Napa/Solano Workforce Task Force, theHospital Council launched a new perioperative (OR)nurse training program at Napa Valley College. Bypartnering with Napa Valley College, hospitals com-bine their resources to provide this specialized trainingand increase the overall pool of available perioperativenurses in the area. The program will also provide anew career opportunity for experienced nurses, thusfreeing up jobs for new nurse graduates.
• The Hospital Council, Blue Shield, hospitals and hospitalconsultants collaborated on solutions to reduce claimrejections through an innovative program calledPOET (Partnership in Operational Excellence andTransparency). POET brings together the operationalhospital staff, Blue Shield and Triage Consulting Group(a neutral hospital consulting organization) to findways to remove barriers to claims processing.
• Initiated and led the collaborative effort to ensure SanFrancisco is the World Leading Center for Innovation inHealth Care and Research. The collaborative – comprisedof the Chamber of Commerce, Pharma, BayBio,
Department of Public Health,UCSF Medical School, SanFrancisco Center for EconomicDevelopment, SF Travel and theHospital Council – workeddirectly with the mayor andboard of supervisors. Major
goals of this project: develop a home-grown workforcefrom middle schools through high school health andbio-tech academies, support for the 50 medical andbiotech programs at City College, the nursing and clin-ical lab scientists programs at San Francisco State andUSF, and the highest level medical training at UCSFMedical School, and promote more medical conven-tions when the Moscone Center is expanded to allowmedical visitation from experts throughout the world.
PUBLIC ADVOCACYThrough Conversations and Connections programs, the Hospital Council EngagesCommunity Leaders and Stakeholders toSupport Hospital Issues• Convened a Conversation and Connections session
at Saint Agnes Medical Center for Fresno-Madera-Tulare-Kings counties, bringing together nearly 100people representing all points along the continuumof care to discuss opportunities to streamline thepatient’s care experience and reduce unnecessary
readmissions to hospitals. All agreed to form theCentral Valley Care Transitions Collaborative.
• Developed the Kern County Care TransitionsCollaborative, a group of hospitals and other com-munity members across thecontinuum of care commit-ted to improving the caretransitions for all patientsthey serve.
• In collaboration with the San Francisco Medical Society,the Community Clinic Consortium and University ofSan Francisco, organized “Show Me the Money, Part 2,”a Conversations and Connections program. The program was devoted to Team-Based Care—a strategyto achieve ACA Triple Aim, with an audience of morethan 60 physicians, nurse leaders and floor nurses,public health leaders and students. Programs like thesehelp build relationships between medical groups tobetter serve the community.
• Facilitated a Community Health Forum on CommunityHealth Needs Assessment to discuss solutions for com-munities and specific groups within San Joaquin Countyexperiencing health disparities – especially as they relateto chronic disease. Over 120 community leadersbusiness partners, physicians and hospital leaderscame together for this conversation. The San JoaquinCounty Public Health Officer introduced the issuediscussion as a community health decision processwhich will be implemented by the County andreported to community leaders.
PROGRAMS AND SERVICESHospital Council Accelerates Initiatives to Improve Clinical and Operational Performance• Patient Safety First…A California Partnership for
Health united California’s three Regional HospitalAssociations, National Health Foundation (NHF) andAnthem Blue Cross in a four-year initiative focusedon reducing hospital-acquired infections and sepsis
mortality, as well asimproving perinatalcare. To date, morethan 173 hospitalsacross the state areparticipating in thisunique initiative, 62 ofwhich are members ofHospital Council of
10 11
Northern and Central California. Program resultsfrom the first two years:
• More than 973 lives have been saved as a resultof reducing sepsis mortality.
• An estimated $19 million in costs were avoided asa result of this statewide patient safety initiative,$3.75 million of which was a result of reducingearly elective deliveries.
• At the Hospital Council’sthird annual BEACONCollaborative FallExchange, 300 attendees engaged in peer-to-peerlearning and best practices on sepsis, perinatal andhospital-acquired infections.
• The Hospital Council’s Medication Safety TrainingSymposiums throughout the region offered forumsfor peer-to-peer sharing and networking for pharma-cists, clinical leaders, and regulatory and compliancehospital leaders.
• Case Management Transformation Initiative (CMTI):The Hospital Council created a Case ManagementInitiative, which helps hospitals transform their existingcase management programs into outcomes-based,physician-centric, case manager-as-care-coordinatorprograms to improve the organization’s standing relativeto value-based purchasing and the pay-for-performancereimbursement models. CMTI, led by Marsh, realizedannual savings and new revenue of up to $1 million foreach participating hospital.
• Lean Management Training: Teaming with theInstitute for Performance Excellence, the HospitalCouncil provides Lean training, program developmentand support services for member hospitals. Lean man-agement practices increase overall efficiency, cut costs,improve quality and drive customer satisfaction. As ofJuly 2012, the Hospital Council offered 25 Lean-relatedprograms in the region.
• New Directions: Providing intensive case managementservices to frequent users of EDs, the Hospital Council’sNew Directions program has enrolled and served morethan 568 patients. The program seeks to reduce avoid-able emergency room visits, inpatient hospital stays andtheir associated costs, thereby improving the quality ofpatients’ lives and health through better access to careand other life essentials. Hospital Council facilitated thecreation of a video telling the story of three formerlyhomeless clients of the New Directions program as theyshare their experiences of being homeless on the streets
of Santa Clara County, the challenges they faced duringtheir transitions into permanent housing, and thesupport they gained from the New Directions casemanagers. To view the video, go to: www.hospitalcouncil.net/announcement/new-directions-video-0.
• Gang Awareness Training and Education: TheHospital Council partnered with law enforcement andhospital security in Fresno, Kern and Tulare counties toprovide essential gang awareness trainings for hospitalstaff. With increasing violence in hospitals, there is agrowing need for hospital staff to refine their knowledgeand awareness of gangs and work toward improvedsystems of organization and communication.
• Hep B FreeSanta Clara County: The Hospital Council, an activemember of the Hep B Free: Santa Clara Countycampaign, links hospitals and the Hep B Free Group.Nationwide, chronic hepatitis B causes up to 80percent of all liver cancer cases. The Hospital Councilconnects the Hep B Free Group to hospitals to provideinformation and screening to the community.
San Francisco: The Hospital Council played a key rolein reaching out to physicians in the San Francisco areato join in the Hep B Free campaign. San Francisco hasthe highest liver cancer rate in the nation. With thehelp of Hospital Council, more than 1,000 SanFranciscan clinicians joined the Hep B Free HonorRoll, pledging to eliminate Hep B by screeningpatients at risk of Hep B according to Centers forDisease Control and Prevention guidelines. The cam-paign reaches out through medical groups, hospitals,clinics, the San Francisco Medical Society Magazine andother resources in which physicians interact.
• Educational ProgrammingThis year, the Hospital Council formed the EducationDevelopment Group (EDGE) to develop an annual planand produce programs that provide maximum mem-ber value. The EDGE takes a collaborative approach toeducational programming, working across the regionalassociations and with CHA to unify, collaborate andcoordinate resources when possible in program devel-opment. This year’s educational programs includedcare transitions, vaccinations of health care workers,affiliations, CMS and JC regulations, wound care andhuman resources topics. Programming for 2012included 50 programs, with over 400 attendees, andan overall satisfaction score of 4.74 out of 5. To furtherenhance program value, Hospital Council is working toform a Member Education Advisory Group.
Patient Safety FirstSaved Hospitals
$19 million

• With its Napa/Solano Workforce Task Force, theHospital Council launched a new perioperative (OR)nurse training program at Napa Valley College. Bypartnering with Napa Valley College, hospitals com-bine their resources to provide this specialized trainingand increase the overall pool of available perioperativenurses in the area. The program will also provide anew career opportunity for experienced nurses, thusfreeing up jobs for new nurse graduates.
• The Hospital Council, Blue Shield, hospitals and hospitalconsultants collaborated on solutions to reduce claimrejections through an innovative program calledPOET (Partnership in Operational Excellence andTransparency). POET brings together the operationalhospital staff, Blue Shield and Triage Consulting Group(a neutral hospital consulting organization) to findways to remove barriers to claims processing.
• Initiated and led the collaborative effort to ensure SanFrancisco is the World Leading Center for Innovation inHealth Care and Research. The collaborative – comprisedof the Chamber of Commerce, Pharma, BayBio,
Department of Public Health,UCSF Medical School, SanFrancisco Center for EconomicDevelopment, SF Travel and theHospital Council – workeddirectly with the mayor andboard of supervisors. Major
goals of this project: develop a home-grown workforcefrom middle schools through high school health andbio-tech academies, support for the 50 medical andbiotech programs at City College, the nursing and clin-ical lab scientists programs at San Francisco State andUSF, and the highest level medical training at UCSFMedical School, and promote more medical conven-tions when the Moscone Center is expanded to allowmedical visitation from experts throughout the world.
PUBLIC ADVOCACYThrough Conversations and Connections programs, the Hospital Council EngagesCommunity Leaders and Stakeholders toSupport Hospital Issues• Convened a Conversation and Connections session
at Saint Agnes Medical Center for Fresno-Madera-Tulare-Kings counties, bringing together nearly 100people representing all points along the continuumof care to discuss opportunities to streamline thepatient’s care experience and reduce unnecessary
readmissions to hospitals. All agreed to form theCentral Valley Care Transitions Collaborative.
• Developed the Kern County Care TransitionsCollaborative, a group of hospitals and other com-munity members across thecontinuum of care commit-ted to improving the caretransitions for all patientsthey serve.
• In collaboration with the San Francisco Medical Society,the Community Clinic Consortium and University ofSan Francisco, organized “Show Me the Money, Part 2,”a Conversations and Connections program. The program was devoted to Team-Based Care—a strategyto achieve ACA Triple Aim, with an audience of morethan 60 physicians, nurse leaders and floor nurses,public health leaders and students. Programs like thesehelp build relationships between medical groups tobetter serve the community.
• Facilitated a Community Health Forum on CommunityHealth Needs Assessment to discuss solutions for com-munities and specific groups within San Joaquin Countyexperiencing health disparities – especially as they relateto chronic disease. Over 120 community leadersbusiness partners, physicians and hospital leaderscame together for this conversation. The San JoaquinCounty Public Health Officer introduced the issuediscussion as a community health decision processwhich will be implemented by the County andreported to community leaders.
PROGRAMS AND SERVICESHospital Council Accelerates Initiatives to Improve Clinical and Operational Performance• Patient Safety First…A California Partnership for
Health united California’s three Regional HospitalAssociations, National Health Foundation (NHF) andAnthem Blue Cross in a four-year initiative focusedon reducing hospital-acquired infections and sepsis
mortality, as well asimproving perinatalcare. To date, morethan 173 hospitalsacross the state areparticipating in thisunique initiative, 62 ofwhich are members ofHospital Council of
10 11
Northern and Central California. Program resultsfrom the first two years:
• More than 973 lives have been saved as a resultof reducing sepsis mortality.
• An estimated $19 million in costs were avoided asa result of this statewide patient safety initiative,$3.75 million of which was a result of reducingearly elective deliveries.
• At the Hospital Council’sthird annual BEACONCollaborative FallExchange, 300 attendees engaged in peer-to-peerlearning and best practices on sepsis, perinatal andhospital-acquired infections.
• The Hospital Council’s Medication Safety TrainingSymposiums throughout the region offered forumsfor peer-to-peer sharing and networking for pharma-cists, clinical leaders, and regulatory and compliancehospital leaders.
• Case Management Transformation Initiative (CMTI):The Hospital Council created a Case ManagementInitiative, which helps hospitals transform their existingcase management programs into outcomes-based,physician-centric, case manager-as-care-coordinatorprograms to improve the organization’s standing relativeto value-based purchasing and the pay-for-performancereimbursement models. CMTI, led by Marsh, realizedannual savings and new revenue of up to $1 million foreach participating hospital.
• Lean Management Training: Teaming with theInstitute for Performance Excellence, the HospitalCouncil provides Lean training, program developmentand support services for member hospitals. Lean man-agement practices increase overall efficiency, cut costs,improve quality and drive customer satisfaction. As ofJuly 2012, the Hospital Council offered 25 Lean-relatedprograms in the region.
• New Directions: Providing intensive case managementservices to frequent users of EDs, the Hospital Council’sNew Directions program has enrolled and served morethan 568 patients. The program seeks to reduce avoid-able emergency room visits, inpatient hospital stays andtheir associated costs, thereby improving the quality ofpatients’ lives and health through better access to careand other life essentials. Hospital Council facilitated thecreation of a video telling the story of three formerlyhomeless clients of the New Directions program as theyshare their experiences of being homeless on the streets
of Santa Clara County, the challenges they faced duringtheir transitions into permanent housing, and thesupport they gained from the New Directions casemanagers. To view the video, go to: www.hospitalcouncil.net/announcement/new-directions-video-0.
• Gang Awareness Training and Education: TheHospital Council partnered with law enforcement andhospital security in Fresno, Kern and Tulare counties toprovide essential gang awareness trainings for hospitalstaff. With increasing violence in hospitals, there is agrowing need for hospital staff to refine their knowledgeand awareness of gangs and work toward improvedsystems of organization and communication.
• Hep B FreeSanta Clara County: The Hospital Council, an activemember of the Hep B Free: Santa Clara Countycampaign, links hospitals and the Hep B Free Group.Nationwide, chronic hepatitis B causes up to 80percent of all liver cancer cases. The Hospital Councilconnects the Hep B Free Group to hospitals to provideinformation and screening to the community.
San Francisco: The Hospital Council played a key rolein reaching out to physicians in the San Francisco areato join in the Hep B Free campaign. San Francisco hasthe highest liver cancer rate in the nation. With thehelp of Hospital Council, more than 1,000 SanFranciscan clinicians joined the Hep B Free HonorRoll, pledging to eliminate Hep B by screeningpatients at risk of Hep B according to Centers forDisease Control and Prevention guidelines. The cam-paign reaches out through medical groups, hospitals,clinics, the San Francisco Medical Society Magazine andother resources in which physicians interact.
• Educational ProgrammingThis year, the Hospital Council formed the EducationDevelopment Group (EDGE) to develop an annual planand produce programs that provide maximum mem-ber value. The EDGE takes a collaborative approach toeducational programming, working across the regionalassociations and with CHA to unify, collaborate andcoordinate resources when possible in program devel-opment. This year’s educational programs includedcare transitions, vaccinations of health care workers,affiliations, CMS and JC regulations, wound care andhuman resources topics. Programming for 2012included 50 programs, with over 400 attendees, andan overall satisfaction score of 4.74 out of 5. To furtherenhance program value, Hospital Council is working toform a Member Education Advisory Group.
Patient Safety FirstSaved Hospitals
$19 million

California Hospital Association1215 K Street, Suite 800Sacramento, CA 95814
916-443-7401www.calhospital.org
Hospital Council of Northern & Central California1215 K Street, Suite 730Sacramento, CA 95814
916-552-7608www.hospitalcouncil.net