Embed Size (px)
Citation preview
Northern England Strategic Clinical Network Conference
Thyroid Sub-group Update
Dr Sath NagConsultant EndocrinologistVice Chair, Thyroid NSSG
South Tees Hospitals Foundation Trust
Thyroid Cancer
• Most common endocrine malignant tumour, but represents only about 1% of all malignancies
• In the UK in 2011 around 2,700 people were diagnosed with thyroid cancer
• More common in women than men.
cruk.org/cancerstats

Thyroid cancer
• Half of all cases in the UK diagnosed in people aged under 50– under-50s accounting for a higher proportion of
female cases (52%) than male cases (40%)
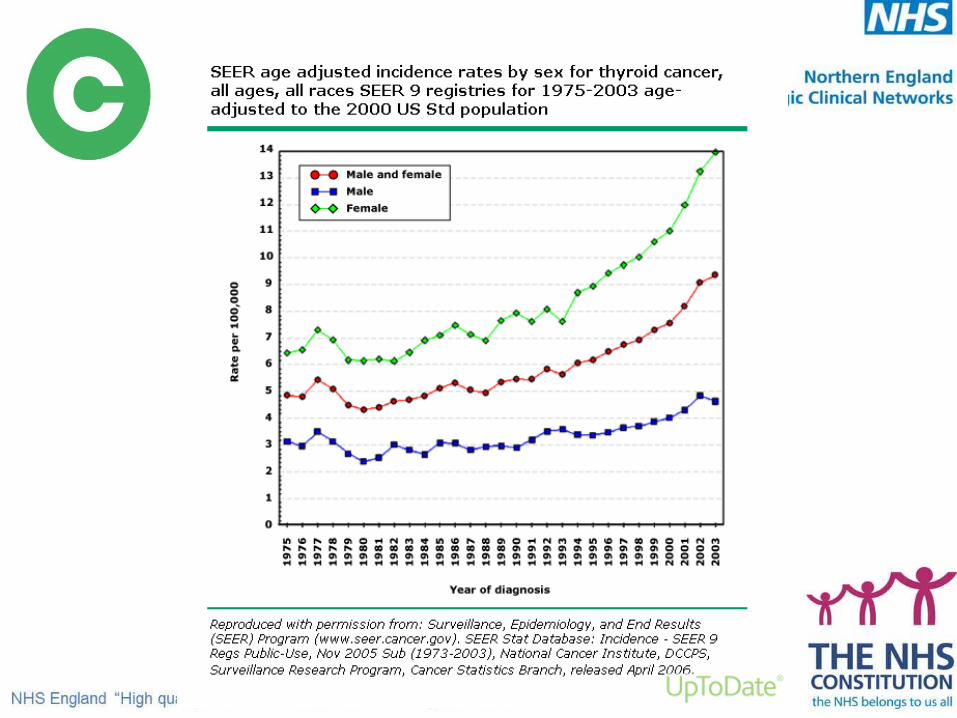
• Incidence rates have doubled in males and more than doubled in females since the 1990s
cruk.org/cancerstats
Thyroid cancer
• Global increase in incidence mainly due to papillary carcinomas
• Bulk of disease in lower stage tumours due to increased detection of papillary microcarcinomas

Mortality
• In 2012, around 374 deaths from thyroid cancer– Accounting for <1% of all cancer deaths
• Mortality rates stable– reduced by >50% in women in the last 40 years. – Reduced by about 30% in men
• UK mortality rate is sixth lowest in Europe for males and ninth lowest for females.
cruk.org/cancerstats
Incidence
• Rising incidence possibly due to:
• Genuine increase• Better detection• Changing iodine status• Exposure to radiation

Public health and prevention
• Nuclear fallout
• Therapeutic and diagnostic X-rays in childhood possible causes of thyroid cancer in adults
Thyroid cancer
Diagnostic update
Molecular diagnostics
• BRAF mutation present in a large proportion of papillary thyroid cancers
• Preoperative BRAF mutation testing of fine-needle aspiration biopsy – Assists with preoperative risk stratification strategy– Potentially predicts extent of initial disease and
subsequent clinical outcomes

Proteomic signatures
• Differentiate thyroid cancer subtypes
• Identify prognostic signatures that guide treatment
• Help distinguish recurrent/residual disease from disease free state
Thyroid Cancer
Therapeutic update

Kinase Inhibitors
KIATP KI
PY Y
ATP
Activated pathway
Cancer
Activated Pathway Cancer
VEGFR inhibition
Tumor
angiogenesisTumor
growth
RET, BRAF….. inhibition

Graphic adapted fromKeefe SM, et al. Clin Cancer Res. 2010;16:778-83.
MotesanibSorafenibSunitinibVandetanibXL-184
Axitinib MotesanibSorafenibSunitinibVandetanib
Vandetanib
Sorafenib Sorafenib
Targeting cell signalling in thyroid cancer
RET/PTC
• HIF1a• Inhibition of apoptosis• Migration
EGFR
PI3K
VEGFR-2
Endothelial Cell
• Migration• Angiogenesis
Ras
B-Raf
MEK
ERK
PI3K
AKT
mTOR
S6K
Ras
Raf
MEK
ERK
AKT
mTOR
S6K
Tumor Cell
• Growth• Survival• Proliferation
• Growth• Survival• Proliferation
EverolimusSirolimus
EverolimusSirolimus
Achievements
Challenges
• Increasing incidence of thyroid cancer
• Dealing with non-iodine avid refractory recurrent disease
• Emerging role of Tyrosine Kinase inhibitors
• Restricted access driven by cost despite emerging evidence base in progressive disease





























