Embed Size (px)
Citation preview
North Lincolnshire ELC™ PATH Planning Workshop: Keeping Well and Living an
Independent Life PATH Planning Event
26 JUNE 2013

WELCOME
Alison Manson And
Georgina Craig
The Team today
Hilary, Maria, Wendy N Linc ELC™ Practitioner
By the end of today we will have: 1. A clear understanding of what
matters around keeping well and living independently
2. Co created our vision of great support around keeping well in 2016
3. Co created an action plan 4. Individual actions of what we and our
organisations will contribute 5. HAD FUN - doing this in a new,
participative and inspiring way!
The commissioning quesOon
“What needs to happen to keep YOU and YOURS well and living an independent life in North Lincs?”

What we did: talked and learnt from you (March 2013)
Building on existing assets and insights – listening and learning from the community about how best to reach people with this conversation
You said. We did
YOU SAID • “You need to do an on line
survey as well” • “Talk with parents of pre
school children -‐ in Children’s Centres”
• “Don’t run sessions in colleges. Young people won’t engage there”
• “Think about people living with disabili@es”
WE…. • Developed and are running
an online survey in parallel • Ran 5 events in Children’s
Centres, talking to different groups of parents
• Looked for other ways to reach out to young people
• Talked to parents of children living with disabili@es
AND supported 20 Community Networkers (April 2013)

AND exisOng assets… Reviewing all relevant existing insights: • JSNA summary • CCG stakeholder consultation • Carers needs assessment (n=230 people) • Who cares? GP access report • Reports: people living with mental health issues • Ulseby and Haxeby Plans • ELC™ Programmes: Outpatient and End of Life
Care • Reports mental health services • N Lincolnshire ‘In the Pink’ data……AND MANY
MORE!!
This ELC™ Co Design Work A chance to listen deeply to what matters most to people

What we did (07 May – 27 June 2013)
Mapped local peoples’ current and desired experience from the following perspectives: • Parents with young families • Parents of children living with disabilities • Care home residents • Older people • People living in recovery from drug and alcohol issues • People who work (mainly in public services including frontline health professionals and caregivers

The engagement numbers
• 13 Events in 4 weeks
• Over 160 people
• Thousands of insights into what matters around keeping well and independent

What we would like to learn more about in the next 6 months Peoples’ current and desired experience from the following perspectives on keeping well: • Experience of pregnancy and caring for babies 0-2 years • Young people in education and school leavers • Housebound older people • People working (private sector) • Unemployed people • Experiences people from Eastern Europe

INSIGHTS SO FAR
What ma^ers most…. RELATIONSHIPS, RELATIONSHIPS, RELATIONSHIPS • Feeling supported and understood (listened to) by
1. family/friends AND 2. care givers • NHS recognition of importance emotional well being
to keep well / remaining independent • Flexible, reassuring care during crises/ transition • Connection with someone with similar lived
experience (role model/peer who has overcome) to support people through transition/crisis
• Well honed life skills: setting up home; parenting, caring / supporting a loved with a long term health issues – parent, spouse, child
What ma^ers most…. RELATIONSHIPS, RELATIONSHIPS, RELATIONSHIPS • Having a safe person to connect with (relationship)
within the ‘system’ (not always or necessarily a health care professional)
• Keeping mobile as long as possible • Caring for others / contributing • Being happy and feeling safe

People say… DON’T BELIEVE CURRENT SERVICES HELP KEEP THEM WELL AND LIVING INDEPENDENTLY Yet this the essence of what the NHS/Council commissioners seek to do (AND could do as an employer)

People say… ITS FEELS LIKE UNTIL YOU HIT CRISIS, HEALTH SERVICES ARE ABSENT. WHEN YOU ARE IN CRISIS, PEOPLE FEEL UNSUPPORTED Currently commissioned services are reactive – not proactive and do not focus on prevention
We saw… FAMILIES WITH PRE SCHOOL CHILDREN, CARERS, OLDER PEOPLE, PEOPLE EARLY IN RECOVERY ARE ESPECIALLY VULNERABLE They are often in transition. They need a close relationship with someone supportive connected to the ‘system’ (not always a health care professional)
We saw… THE LIFE SKILLS YOU LEARN DETERMINE YOUR ABILITY TO KEEP WELL – AS DOES THE COPING STRATEGIES YOU ARE ABLE TO CHOOSE AND EMOTIONAL WELL BEING Commissioners can invest in building these skills and emotional well being

We say and people say… WE WANT TO GIVE BACK / MAKE A DIFFERENCE – INCLUDING THOSE WHO MAY HAVE BEEN/FEEL ‘WRITTEN OFF’ Commissioners can build on this by investing in managing and developing the rich seam of community good will through volunteering

Emotional maps CURRENT
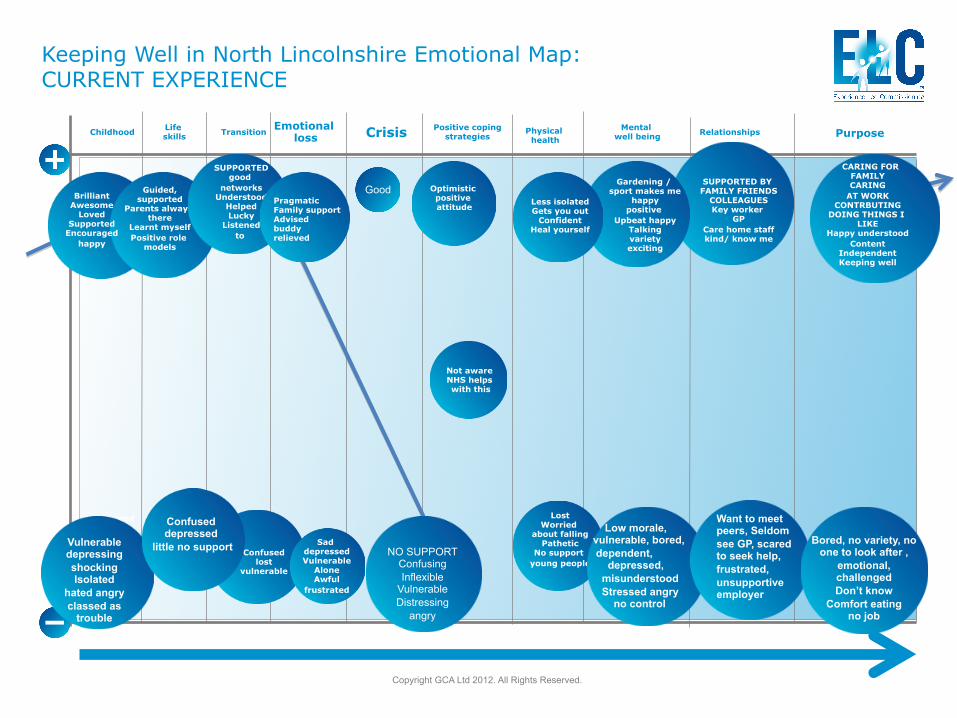
Keeping Well in North Lincolnshire Emotional Map: CURRENT EXPERIENCE
Childhood
Copyright GCA Ltd 2012. All Rights Reserved.
Life skills Transition Emotional
loss Crisis Positive coping strategies
Physical health
Mental well being Relationships
Purpose
uninformed about stroke
prevention
Guided, supported
Parents always there
Learnt myself Positive role
models
SUPPORTED good
networks Understood
Helped Lucky
Listened to
Brilliant Awesome
Loved Supported
Encouraged happy
Confused lost
vulnerable
Sad depressed Vulnerable
Alone Awful
frustrated
CARING FOR FAMILY CARING
AT WORK CONTRBUTING
DOING THINGS I LIKE
Happy understood Content
Independent Keeping well
Pragmatic Family support Advised buddy relieved
Optimistic positive attitude
Not aware NHS helps with this
Lost Worried
about falling Pathetic
No support young people
SUPPORTED BY FAMILY FRIENDS
COLLEAGUES Key worker
GP Care home staff kind/ know me
Gardening /
sport makes me happy
positive Upbeat happy
Talking variety exciting
Less isolated Gets you out
Confident Heal yourself
Vulnerable depressing shocking Isolated
hated angry classed as
trouble
Confused depressed
little no support NO SUPPORT Confusing Inflexible
Vulnerable Distressing
angry
Good
Low morale, vulnerable, bored, dependent, depressed, misunderstood Stressed angry no control
Want to meet peers, Seldom see GP, scared to seek help, frustrated, unsupportive employer
Bored, no variety, no one to look after ,
emotional, challenged Don’t know
Comfort eating no job

Emotional maps DESIRED

Keeping Well in North Lincolnshire Emotional Map: DESIRED EXPERIENCE
Childhood
Copyright GCA Ltd 2012. All Rights Reserved.
Supported Stable Loved
Encouraged Guided
Life skills Transition Emotional
loss Crisis Positive coping strategies
Physical health
Mental well being Relationship
Purpose
uninformed about stroke
prevention
Guided Encouraged Prepared Involved
Supported Informed Cared for
CARING FOR FAMILY
CARING THROUGH WORK
Gardening sport Sharing knowledge
Volunteering Learning
Being independent Hopeful
Optimistic engaged
SUPPORTED Competent
Easy to access/ navigate Compassion
Understanding Flexible
non judgemental Safe
Dr fantastic
Listened to Support
Reassured Understood Cared for
Guided Able
Prepared
Listened to understood
SAFE At ease Inspired informed
Supportive Peer support
GP knows me well Flexible
HAPPY Support each
other family\ Friends
Colleagues Understood independent
Fresh air Accessible cheap
Connected Walking Guided
Reassured Motivated Confident
Family activity
Current emoOonal ‘lows’ • Coping with emotional loss • Maintaining emotional well being • Feeling support through times of transition (especially if a person has no family support) • Improved experience of crises in care

The essence of keeping well • Support • Being listened to/understood as a person • Caring for others (making a difference)
This fits with what we know from the evidence and research into well being /
happiness

The mismatch with health and care service experience The things services often fail to do are: • Support people when life is tough • Listen to/understanding the person • Support people to retain their sense of purpose e.g. care for others, make a difference, do things that make them happy ESPECIALLY DURING CRISIS/TRANSITIONS
What we found out (exisOng insights from other CCG work)
• Carers • People at end of life • People living with 4 long term conditions
Key messages: carers • Do not see themselves as ‘carers’ – get a huge sense of
meaning and purpose from caring for their loved ones…. (this keeps them well!)
• Unaware of welfare benefits, local ‘carers payments’/’breaks services’, training they can tap into ( poor uptake impacts on their financial health and emotional/physical wellbeing – and life chances young carers)
• Scared /reluctant about leaving loved ones with others; need lots of reassurance about quality (FIRST respite experience really matters)
• Want greater understanding of loved one’s health condition so they can care/ advocate better. Feel ignored by health/care system.
Key messages: carers • FLEXIBLE support (training) ‘life skills’; managing personal/
medical care • Ignore their own health needs and focus instead on the
person. Often means seek help too late and become ill – HIGH RISK GROUP
• Great local assets to build on: the voluntary sector - especially Carers Support Centre – potential for a hub and network to support carers/families to keep well and live independently (can be COMMISSIONED TO IMPROVE OUTCOMES for carers)
• Being able to work keeps carers well. Understanding, flexible employers critical - public sector = major employer – ‘could do better’
Key messages: people at end of life • Talk more about death and dying– a big culture change • Create a systemaOc way to support forward plans for
desired end of life experience – so friends/ family/health care system all know what ma^ers
• Involve nurses in sharing bad news • Focus on improving end of life care older people and
those without a diagnosis of cancer • Make end of life care ‘everybody’s business’ • Support carers around end of life especially well Vision of great care: “Person centred, community based 24/7 care that focuses on ‘what ma;ers to person/family’ delivered by compassionate, well supported teams working flexibly because of great relaDonships with each other (care professionals) and with people/families -‐ coupled with smooth, appropriate admission/discharge from hospital and peer support.”

Key messages: people with long term health
Outpatient services: • Frustrating experience that adds little value;
unclear why need to go there. Often wait hours for tests; appointments cancelled or no one expecting them when they arrive
• Learn nothing to help improve ability to self care and manage their condition.
• Often have mobility issues so getting to outpatients difficult - because of location, car parking. Going to bursars office on a separate floor and pharmacy difficult too
• Staff frustrated and buried in paperwork that adds no value to care quality. Can’t book transport; leaves them feeling guilty/powerless
• Going through discharge lounge improves experience; even if long wait, at least this is a nice place to wait

What we found out about talking with the community • Pre school families • Families with children at school • Families with a disabled child • Older people who live in care homes • Older people living in their own homes • People in recovery drug and alcohol misuse • People who work (mainly in public services)

Key messages: preschool families (Childrens Centres) • Invisible to system unless have a child • Want to learn life skills. Crave connection with older role models
(male/female). If no family, less able to develop coping strategies • Deny impact smoking on child health (CCG work) • UNSUPPORTED through transition e.g. birth, crises and emotional
loss e.g. relationship break up • UNSUPPORTED (no relationship) midwives; evidence undiagnosed
depression; no help with bottle feeding only breast feeding = pressure
• Want to be listened to (esp single parents) and trusted. • No emotional support NHS; want information about sources
support and easy DROP IN INFORMAL ACCESS SUPPORT including: child health advice, someone to talk to (feel alone)
• Childrens Centres ‘fantastic’ – build on this asset; support from other mums valued too. More family orientated fitness activities; not much for babies (less than used to be)
Key messages: families with children at school • Mixed experiences of learning life skills • NHS not a source of support with emotional loss • Poor experiences of crises in care • Parents mixed confidence levels around keeping physically/
emotionally well; coping strategies. • Signs of a sub group not coping well (underlying anxiety) – may be
they at high risk mental health issues • Friends/family - and caring for others = key purpose • Some struggle to exercise / keep physically well
This group are keeping well and coping better than younger parents. They may be an asset to support younger parents to
transition and others. There are some who may be at risk

Key messages: families with disabled children • Strong sense of community - special school acts as a source of support (access hub) to keep well • Siblings and grandchildren play a key role in supporting parents /grandparents with disabled children • Working provides respite, keeps parents well and able to care • Are a resilient group

Key messages: older people living in care homes • Feel well cared for; ‘wonderful’ care home staff • Seeing a GP/nurse is rare. NHS absent. Scared to go to GP when ill.
Fear what the GP will say. Worry about health issues; especially falling and failing mobility - frustrates and depresses them
• Crave variety: meeting new people; more fresh air, ‘getting out’, exercise, music, being alone – regardless of mobility. Some would like more control and choice – including more privacy; more space
• Want to keep as independent as possible - do things for themselves as long as possible. Being dependent gets people down
• Looking after and talking with other residents keeps people well –- PURPOSE
• Visits from family are VERY important. Supporting older family members to live in the same home and close to relatives makes visiting and keeping connection easier. This keeps people well
• Good care home staff with a bit more time to ‘understand who I am’ critical to well being

Key messages: older people living independently • Worry about dementia (failing mental health) more
than physical health • As get older, easier to cope with life’s ups and
downs • Want to look after themselves as much as possible
e.g. emergency medication to prevent exacerbation, information and support to self care
• Volunteering and caring for others (family, friends) keeps older people well
• Regular health checks reassure people • Walking and getting out and about is really
important – doing it together gives people confidence; sense of being safe and provides a chance to meet others / connect. Facilitating this is key

Key messages: people in recovery drug /alcohol misuse • Common trigger for substance misuse is not coping with
emotional loss; child hood experiences; being in care • Often learnt life skills from peers – less often from parents. May
have had few inspirational adult role models when growing up • Put off and fear seeking help – in case they are arrested when they
are in crisis • May be happy in what other see as crisis. Get huge sense of
belonging from taking drugs; numbs emotional pain. • Through recovery, the pain is still there. This is a critical transition
to support and it is often neglected / less well supported • Close, supportive relationships with care workers are critical and
support recovery and keeping well • People in recovery have learnt to embed positive coping strategies.
They have a lot of experience and wisdom to share with others – not just those who – like them - are in recovery!
Key messages: people who work (mainly in public services) • Strong sense of energy around ‘purpose’ = to care and make a
difference to people’s lives and experience of hospital • NLAG workforce feels very low at the current time • Front line do not feel NHS supports them to keep well – even
routine check ups difficult = ironic • People feel guilty taking time off when ill = letting colleagues down • Peer support is massively important to well being; needs to be built
with intention and supported by managers • Management disconnected from front line staff – unaware of the
value staff are adding – and so missing opportunities to accelerate improvement in services and care experience
• Strong dissatisfaction to GP service provision • Perception that managers do not understand what adds value
(including discharge lounge) • Clinical supervision helps; buddy system gone; peer support key

EMERGING IMPROVEMENT CHALLENGES NORTH LINCS

Emerging improvement challenges N Lincs
• Build relationship based care and community – especially around existing community hubs (including childrens centres, hospital, special schools, care homes, outpatients, carers centre)
• GPs more proactive (especially in care homes)
• Look after NHS employees better • Understand and leverage services that are
delivering value (and those not)
Emerging improvement challenges N Lincs
• Get transition right • Prevent crisis by understanding/mapping
how people experience transitions – including emotional loss
• Support carers • Be understanding employer; keep
employees well • Improve experience of crisis • Focus on supporting people with
emotional well being; building positive coping strategies

Emerging improvement challenges N Lincs
• Invest in life skills support – especially for vulnerable young people (those in care; less supportive family background)
• Build peer support networks / mentoring/ role models
• Give NHS staff space to support each other
• Help people maintain sense of purpose (especially older people; those in care homes)
• Measure different things
IntroducOon to PATH Planning
Alison Manson ELC™
Today’s work….. Develop a PATH Plan and focus on the question: “What needs to happen to
keep people well and independent around
here?”
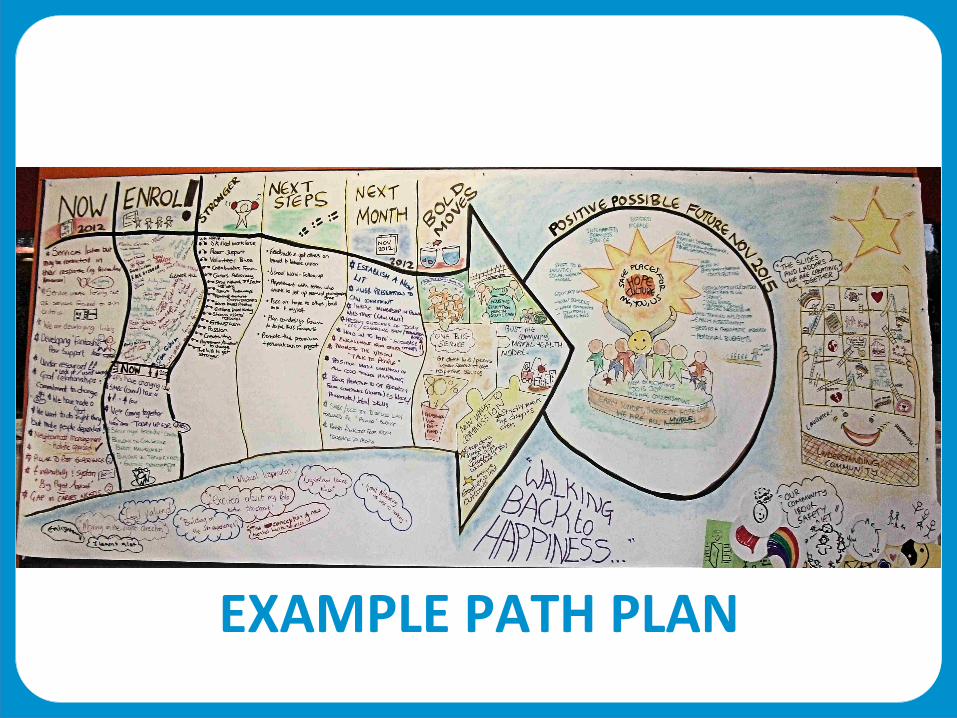
EXAMPLE PATH PLAN

PATH FLOW 1. Or Ambition: North Star Dream 2. Our possible, positive future in
3 years 3. Now 4. Enrolment 5. Strengths 6. Bold Steps 7. Next Month 8. Next Steps

PATH Process • Working in our table groups –
highly participative • Table top facilitator at each
table to support you • Feedback from the room;
individually and by table • Consensus building as we
complete graphics and commit anything to the PATH
THIS IS YOUR PATH !
Our AmbiOon: North Star Dream Orientation: our guide; draws us toward our best work. Unreachable and inspiring, The north star reminds why we are doing this work on our bad days… Action: • Slow down. Think deeply. • Notice what comes to your mind first. • Jot down the words. Notice and hold onto the images • Share the words and images that come to mind.

PosiOve Possible Future 2016 Orientation: after HARD WORK and GOOD LUCK, we have made great progress. Standing in the future, describe what we have achieved... Actions: • Describe the detail of the vision • Focus on possible and positive change
Now Orientation: Come back to now. We want to realise that future. Describe where we are starting today. It's about describing the facts. Not fixing them Action: • Capture the top three things we need to notice about now

Enrolment • Sign the PATH if you want to come with us and make this improvement happen • Who else do we need to enroll to make this happen?

Strengths Orientation: now we know who is coming with us, what assets/ strengths do we already have and what do we need to build? Action: • Complete proforma table provided • Pick the most important strengths and share with the group

Our Bold Moves Orientation: these are our ‘headlines’ - the main themes in our story of change. They are game changers that accelerate progress and our best work. They are the brave risks – the leaps we will take to make big change happen. Action: • Identify 2-3 Bold Moves • For each, agree 3 key actions

Next month Orientation: to maintain momentum, taking action in the next month is critical. What happens now sets the tone and the foundations for success. We want quick wins to spur us on. Action: • Identify key actions for next month • Share and agree the critical ones

First Steps Orientation: what you personally commit to doing in the next 24 hours? A social interaction works best e.g. telling someone something; asking for help Action: • Think of ONE thing YOU will do to move this work forward • Write it down. Commit to doing it
AppreciaOon Orientation: reflect on how doing PATH planning has made you feel. Action: • Discuss and reflect • Share your thoughts • Write them on the PATH • NAME the PATH together
Feedback is a gid …
1. What went well today? 2. What could we improve?

Thank you for your hard work and commitment today

Close & Next Steps
Caroline Briggs North Lincolnshire CCG

Two ways we will be using this work to help us
Pioneers for integration Sustainable services

Our framework for supporOng our community to keep well
• Conception to 2 years • Children with disabilities • 16-24 year olds • Frail older people

THANK YOU SO MUCH