Embed Size (px)
DESCRIPTION
these factors with those for imipenem-susceptible A. baumannii (ISAB) infections. ORIGINAL ARTICLE ISSN 0036-5548 print/ISSN 1651-1980 online © 2010 Informa Healthcare DOI: 10.3109/00365548.2010.489568 Scandinavian Journal of Infectious Diseases, 2010; 42: 741–746 Correspondence: M. Dizbay, Department of Clinical Microbiology and Infectious Diseases, Gazi University School of Medicine, Besevler, 06510, Ankara, Turkey. Tel: 90 312 2025432. Fax: 90 312 2136333. E-mail: [email protected]
Citation preview

Correspondence: M. Dizbay, Department of Clinical Microbiology and Infectious Diseases, Gazi University School of Medicine, Besevler, 06510, Ankara, Turkey. Tel: � 90 312 2025432. Fax: � 90 312 2136333. E-mail: [email protected]
(Received 8 February 2010 ; accepted 19 April 2010 )
Introduction
In the last 2 decades, Acinetobacter baumannii has become an important nosocomial pathogen in Turkey, as well as throughout the world, and is a major problem due to multidrug resistance [1 – 3]. Carbapenems are usually the antibiotics of choice for treating serious infections caused by A. baumannii. However, increasing rates of imipenem resistance in A. baumannii isolates worldwide is of major concern [2 – 4].
Some potential risk factors, such as hospital size of � 500 beds, previous antimicrobial treatment, colonization density, transfusion, intensive care unit (ICU) stay, urinary catheterization, and surgery are documented as risk factors for the acquisition of imipenem-resistant A. baumannii (IRAB) [3,5,6]. The emergence of IRAB strains, especially in ICUs, threatens the successful treatment of A. baumannii infections and leads to high mortality rates [2,3].
The aim of this study was to identify risk factors for nosocomial IRAB infections and to compare
these factors with those for imipenem-susceptible A. baumannii (ISAB) infections.
Materials and methods
Gazi University Hospital is a 1000-bed tertiary care teaching hospital, including 109 ICU beds, in Ankara, Turkey. The number of ICU beds was increased from 39 to 109 between 2003 and 2007. Patients with nosocomial A. baumannii infections during the period January 2003 to December 2007 were included in the study. Consecutive isolates in the same nosocomial infection (NI) episode were excluded from the study. An active NI surveillance was performed by infection control nurses. The data were obtained prospectively from infection control committee records. The diagnosis of NI was assessed according to the Centers for Diseases Control and Prevention (CDC) criteria [7,8]. A urinary tract infection in a patient with an indwelling bladder catheter was diagnosed with the detection of pyuria
ORIGINAL ARTICLE
Nosocomial imipenem-resistant Acinetobacter baumannii infections: Epidemiology and risk factors
MURAT DIZBAY, OZLEM GUZEL TUNCCAN , BUSRA ERGUT SEZER & KENAN HIZEL
From the Department of Clinical Microbiology and Infectious Diseases, Gazi University School of Medicine, Besevler, Ankara, Turkey
Abstract The incidence, clinical characteristics, risk factors, antimicrobial susceptibility, and outcomes of nosocomial imipenem-resistant A. baumannii (IRAB) infections during a 5-y period (2003 – 2007) were retrospectively analyzed. A total of 720 patients with 925 episodes of A. baumannii infection were included in the study. A. baumannii infections were seen mostly in intensive care units. The incidence was 6.2 per 1000 admissions. The most common infections were pneumonias and bloodstream infections. Imipenem resistance among Acinetobacter strains increased signifi cantly each y of the study (from 43.3% to 72.9%). Mortality was related to the presence of imipenem resistance, stay in intensive care unit, female gender, old age, and pneumonia. Haemodialysis, malignancy, and mechanical ventilation were signifi cant risk factors for IRAB infections. Imipenem resistance was higher in strains isolated from patients with pneumonia. IRAB strains showed higher resistance rates to other antibiotics than imipenem-susceptible strains. The most active antimicrobial agents against A. baumannii were cefoperazone – sulbactam and netilmicin. The incidence of A. baumannii infections and imipenem resist-ance increased during the study period. IRAB infections should be considered in patients on mechanical ventilation and haemodialysis and in patients with malignancies.
Scandinavian Journal of Infectious Diseases, 2010; 42: 741–746
ISSN 0036-5548 print/ISSN 1651-1980 online © 2010 Informa HealthcareDOI: 10.3109/00365548.2010.489568

742 M. Dizbay et al.
( � 10 leukocytes/mm 3 ), growth of � 10 5 cfu/ml bac-teria (no more than 2 species) in urine culture, and clinical signs of infection (fever � 38.8 ° C, leukocyto-sis, abnormal macroscopic appearance of urine, pres-ence of urinary nitrites). In patients assisted by mechanical ventilation, pneumonia was diagnosed when a new or progressive infi ltrate or consolidation was found on chest X-ray in the presence of purulent tracheal secretions, supported by a growth of � 10 5 cfu/ml bacteria in a quantitative culture of deep endotracheal aspirate. For non-ventilated patients, the diagnosis of nosocomial pneumonia was consid-ered when they had a compatible chest X-ray and purulent sputum, with Gram stain and sputum cul-ture documenting the presence of a pathogenic microorganism. Surgical site infection was defi ned as the presence of purulent drainage and positive clini-cal fi ndings (incision site pain, tenderness, localized swelling, redness or heat, spontaneous opening of the incision) supported by microbiological analysis of specimens. Sepsis was diagnosed by the presence of the sepsis criteria and positive blood cultures. Patients colonized with A. baumannii were excluded.
The following data were collected and analyzed: age, sex, ward, length of hospitalization, risk factors (neutropenia, immunosuppressive therapy, mechani-cal ventilation, haemodialysis, tracheostomy, central venous catheter, urinary catheter, nasogastric cath-eter) and underlying diseases (malignancy, trauma, diabetes mellitus), the type of NI, microbiological data, and mortality. The crude mortality rate was calculated as the ratio between the number of deaths among patients with A. baumannii infection. Data on the risk factors for IRAB infection were analyzed according to the number of NI episodes.
Microorganisms were identifi ed by the BBL Crys-tal Enteric/Nonfermenter ID Kit (Becton Dickinson, USA). Susceptibility testing was done using the disk diffusion method according to the Clinical and Lab-oratory Standards Institute (CLSI) criteria [9].
The statistical analysis of the data was performed using SPSS version 17.0 software package (SPSS Inc., Chicago, IL, USA). Categorical variables were analyzed using the Chi-square or Fisher ’ s exact test where appropriate. A univariate analysis was performed
to detect the risk factors for imipenem resistance. Variables with a p -value of � 0.05 in the univariate analysis were included in the multivariate analysis. To test the independence of the risk factors for imi-penem resistance, a multivariate analysis was per-formed by logistic regression. Statistical signifi cance was set at a p -value of � 0.05.
Results
During the study period, A. baumannii was isolated from various clinical specimens of 1147 NI episodes in 752 patient. In only 925 NI episodes in 720 patients was A. baumannii accepted as a causative agent of nosocomial infection. One hundred and sixty-nine (22.8%) patients had more than 1 episode. According to hospital surveillance data, 16.6% of all NI isolates and 23.5% of Gram-negative isolates were A. bau-mannii during the study period. There was an accom-panying pathogen in 11% of A. baumannii infections. The presence of polymicrobial infection did not sig-nifi cantly increase mortality ( p � 0.289).
The nosocomial A. baumannii infection incidence was 6.2 per 1000 admissions. The majority of A. bau-mannii infections were in ICUs (68.9%). Although the number of ICU beds increased over the study y, this was not signifi cant ( p � 1.00). The incidence of A. baumannii infection and imipenem resistance among A. baumannii isolates increased signifi cantly from 43.3% to 72.9% between 2003 and 2007 ( p � 0.001). The incidence of A. baumannii infections and the percentage among nosocomial pathogens over the study period are shown in Table I. Respira-tory tract infections (52.5%) were the most frequent infections caused by A. baumannii, followed by bloodstream infections (25.6%) and surgical site infections (10.2%). Respiratory tract infections and bloodstream infections were seen mostly in ICUs at 80.7% and 71.3%, respectively.
The crude mortality rate was 56.8% for A. bau-mannii infections, highest in pneumonias (67.7%), followed by bloodstream infections (59.6%), urinary tract infections (25.5%), and surgical site infections (16.5%).
Table I. Incidence of Acinetobacter baumannii infections and isolation percentages by y.
2003 2004 2005 2006 2007 Total
Number of A. baumannii isolates 67 115 189 296 278 925Incidence (per 1000 admission) 2.35 3.86 6.81 9.06 7.94 6.22% of A. baumannii among NI isolates 7.2 12.4 20.4 32 27.9 16.6% of A. baumannii among Gram-negative isolates 11.8 15.9 23.7 28.5 30.2 23.5% imipenem-resistant 43.3 47.8 44.4 56.8 72.9 56.6Mortality rate 50.7 65.2 61.3 53.0 55.8 56.8Number of ICU beds 43 60 66 72 80
NI, nosocomial infection; ICU, intensive care unit.
Epidemiology of Acinetobacter infections 743
The male/female ratio was 1.28 and the mean age 55.99 y (standard deviation (SD) � 24.09 y, median 61 y). The crude mortality rate was statistically higher in females (62.2% in females, 51.6% in males; p � 0.004) and in patients over 65 y old (55% vs 44.9%; p � 0.001). Mean duration of hospitalization was 24.29 days (SD � 28.86, median 24 days). There was no statistical difference in duration of hospitalization with regard to mortality (23.9 vs 21.2 days; p � 0.192). ICU patients accounted for 65% of the infected patients. A fatal outcome was seen in 72.6% of the patients in the ICU setting and in 25.7% in non-ICU settings ( p � 0.001).
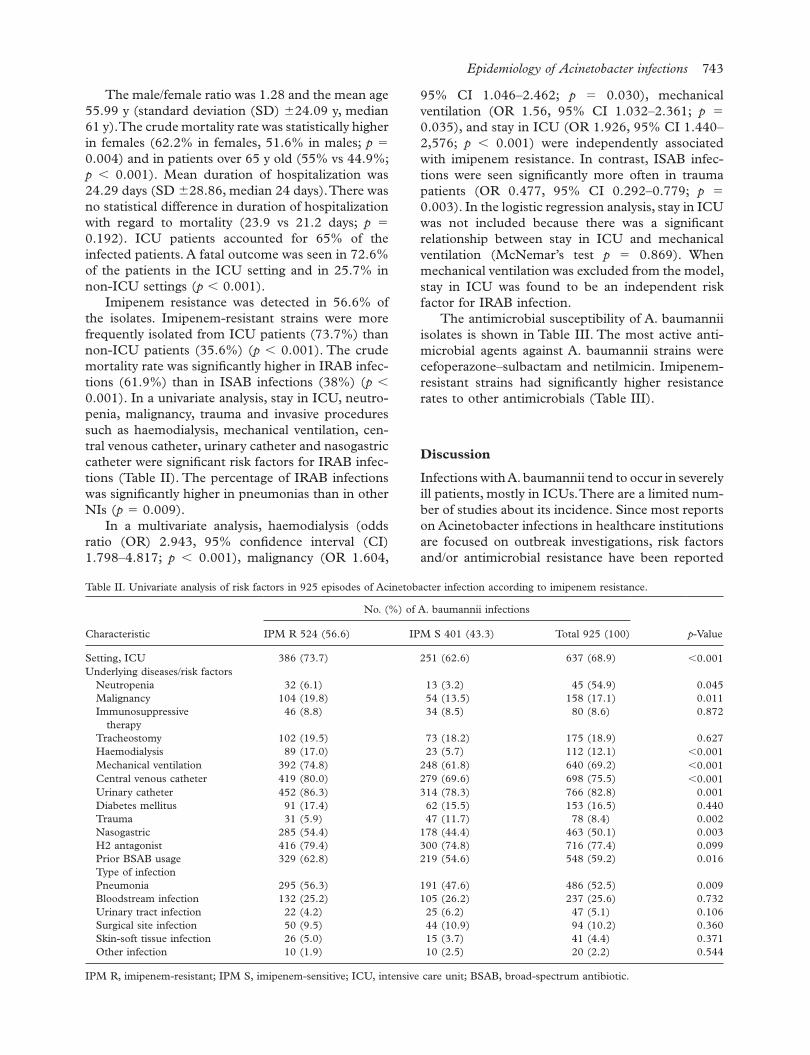
Imipenem resistance was detected in 56.6% of the isolates. Imipenem-resistant strains were more frequently isolated from ICU patients (73.7%) than non-ICU patients (35.6%) ( p � 0.001). The crude mortality rate was signifi cantly higher in IRAB infec-tions (61.9%) than in ISAB infections (38%) ( p � 0.001). In a univariate analysis, stay in ICU, neutro-penia, malignancy, trauma and invasive procedures such as haemodialysis, mechanical ventilation, cen-tral venous catheter, urinary catheter and nasogastric catheter were signifi cant risk factors for IRAB infec-tions (Table II). The percentage of IRAB infections was signifi cantly higher in pneumonias than in other NIs ( p � 0.009).
In a multivariate analysis, haemodialysis (odds ratio (OR) 2.943, 95% confi dence interval (CI) 1.798 – 4.817; p � 0.001), malignancy (OR 1.604,
95% CI 1.046 – 2.462; p � 0.030), mechanical ventilation (OR 1.56, 95% CI 1.032 – 2.361; p � 0.035), and stay in ICU (OR 1.926, 95% CI 1.440 – 2,576; p � 0.001) were independently associated with imipenem resistance. In contrast, ISAB infec-tions were seen signifi cantly more often in trauma patients (OR 0.477, 95% CI 0.292 – 0.779; p � 0.003). In the logistic regression analysis, stay in ICU was not included because there was a signifi cant relationship between stay in ICU and mechanical ventilation (McNemar ’ s test p � 0.869). When mechanical ventilation was excluded from the model, stay in ICU was found to be an independent risk factor for IRAB infection.
The antimicrobial susceptibility of A. baumannii isolates is shown in Table III. The most active anti-microbial agents against A. baumannii strains were cefoperazone – sulbactam and netilmicin. Imipenem-resistant strains had signifi cantly higher resistance rates to other antimicrobials (Table III).
Discussion
Infections with A. baumannii tend to occur in severely ill patients, mostly in ICUs. There are a limited num-ber of studies about its incidence. Since most reports on Acinetobacter infections in healthcare institutions are focused on outbreak investigations, risk factors and/or antimicrobial resistance have been reported
Table II. Univariate analysis of risk factors in 925 episodes of Acinetobacter infection according to imipenem resistance.
Characteristic
No. (%) of A. baumannii infections
p -ValueIPM R 524 (56.6) IPM S 401 (43.3) Total 925 (100)
Setting, ICU 386 (73.7) 251 (62.6) 637 (68.9) � 0.001Underlying diseases/risk factors
Neutropenia 32 (6.1) 13 (3.2) 45 (54.9) 0.045Malignancy 104 (19.8) 54 (13.5) 158 (17.1) 0.011Immunosuppressive
therapy46 (8.8) 34 (8.5) 80 (8.6) 0.872
Tracheostomy 102 (19.5) 73 (18.2) 175 (18.9) 0.627Haemodialysis 89 (17.0) 23 (5.7) 112 (12.1) � 0.001Mechanical ventilation 392 (74.8) 248 (61.8) 640 (69.2) � 0.001Central venous catheter 419 (80.0) 279 (69.6) 698 (75.5) � 0.001Urinary catheter 452 (86.3) 314 (78.3) 766 (82.8) 0.001Diabetes mellitus 91 (17.4) 62 (15.5) 153 (16.5) 0.440Trauma 31 (5.9) 47 (11.7) 78 (8.4) 0.002Nasogastric 285 (54.4) 178 (44.4) 463 (50.1) 0.003H2 antagonist 416 (79.4) 300 (74.8) 716 (77.4) 0.099Prior BSAB usage 329 (62.8) 219 (54.6) 548 (59.2) 0.016Type of infectionPneumonia 295 (56.3) 191 (47.6) 486 (52.5) 0.009Bloodstream infection 132 (25.2) 105 (26.2) 237 (25.6) 0.732Urinary tract infection 22 (4.2) 25 (6.2) 47 (5.1) 0.106Surgical site infection 50 (9.5) 44 (10.9) 94 (10.2) 0.360Skin-soft tissue infection 26 (5.0) 15 (3.7) 41 (4.4) 0.371Other infection 10 (1.9) 10 (2.5) 20 (2.2) 0.544
IPM R, imipenem-resistant; IPM S, imipenem-sensitive; ICU, intensive care unit; BSAB, broad-spectrum antibiotic.

744 M. Dizbay et al.
rather than surveillance data. In a multicentre pro-spective study performed in Spain, the overall inci-dence of A. baumannii infection and/or colonization was 0.39 cases per 1000 patient-days, ranging from 0.14 to 4.55 cases per 1000 patient-days in ICUs [10]. A. baumannii infections were more prevalent in our hospital. The incidence of A. baumannii infec-tions increased signifi cantly in our hospital between 2003 and 2007, and A. baumannii has been the most commonly isolated microorganism in nosocomial infections since 2006. The incidence of A. baumannii was 6.22 patients per 1000 admission during the study period, ranging from 2.35 to 9.06. The inci-dence among Gram-negative isolates increased from 11.8% to 30.2%. Moreover, most of the A. bauman-nii infections (68.9%) occurred in ICUs. This increase in A. baumannii infections in ICUs can be explained by a failure of the physical conditions in ICUs, (e.g. lack of 1 isolation room for each 6 patients), inadequate staff numbers and the increas-ing number of ICU beds. Although the number of ICU beds throughout the y has increased in our hos-pital, the increase was not signifi cant. Therefore we did not consider it as a confounding factor.
The risk factors associated with the acquisition of A. baumannii have been described previously, but predictors for mortality have not been adequately explored. Multidrug-resistant Acinetobacter infec-tions usually occur in severely ill patients in the ICU. The associated crude mortality rate is high, ranging from 26% to 68% [2]. To distinguish morbidity and mortality attributable to A. baumannii is diffi cult. The crude mortality rate of A. baumannii infections was 56.8% in our study. It is diffi cult to ascribe this high mortality rate to the presence of A. baumannii infections because of the patients ’ severe underlying diseases. We did not evaluate attributable risk factors for mortality in this study, and only focused on the factors affecting mortality in patients with A. bau-
mannii infections. Infection with pandrug-resistant strains of A. baumannii has been reported as an inde-pendent risk factor for mortality, as well as blood-stream infection and inadequate antimicrobial therapy [11]. Similarly, in our study imipenem resis-tance was related to higher mortality. Mortality was also signifi cantly higher in ICU patients, females, patients aged over 65 y, and patients with pneumo-nia. There was no association between mortality and duration of hospitalization before A. baumannii infection.
Resistance rates to carbapenems, quinolones and aminoglycosides, which are commonly used in the treatment of A. baumannii infections, have increased worldwide in the last 2 decades. The incidence of imipenem resistance in Acinetobacter spp. was 6 – 8% in the USA and Canada, 10% in Latin America, and 16% in Europe [3,12,13]. In the MYSTIC Study in 1997 – 2000, susceptibility to meropenem was between 0% and 7% in many countries, whereas it was 30% in Italy and the UK and 35% in Turkey [12]. Multidrug resistance in Acinetobacter spp. appears to be a particular problem in Turkey. Car-bapenem resistance in A. baumannii has been reported at between 55% and 63% in various stud-ies from Turkey performed in ICUs [14,15]. The results of the MYSTIC Study, which was performed at 9 centres in Turkey from 2000 to 2003, revealed that 48% of the A. baumannii isolates were resistant to imipenem and one-third (33.3%) were resistant to all antibiotics tested [16]. Imipenem resistance was detected in 56.6% of A. baumannii isolates in our study. The resistance rate for imipenem increased signifi cantly between 2003 and 2007. The most likely explanation for this increase may be the increased number of ICU beds by y as well as over-use of antibiotics, particularly carbapenems in our hospital, and a lack of proper infection control measures.
Table III. Antibiotic resistance rates in 925 episodes of Acinetobacter infection according to imipenem resistance.
Antibiotics
No. (%) of A. baumannii infections
p -ValueIPM R ( n � 524) IPM S ( n � 401) Total ( n � 925)
Amikacin 434 (82.8) 198 (49.4) 632 (68.3) � 0.001Ampicillin – sulbactam 446 (85.3) 228 (56.9) 674 (72.9) � 0.001Gentamicin 455 (86.8) 247 (61.8) 702 (75.9) � 0.001Piperacillin – tazobactam 509 (97.1) 244 (60.8) 753 (81.4) � 0.001Ceftazidime 493 (90.3) 308 (76.8) 781 (84.4) � 0.001Ceftriaxone 515 (98.3) 353 (88.0) 868 (93.8) � 0.001Ciprofl oxacin 502 (95.8) 249 (62.1) 751 (81.2) � 0.001Cefoperazone – sulbactam 233 (44.6) 146 (36.4) 379 (41.0) 0.013Trimethoprim – sulfamethoxazole 501 (95.6) 307 (76.6) 808 (87.4) � 0.001Cefepime 466 (89.1) 280 (69.8) 746 (80.7) � 0.001Netilmicin 172 (32.8) 48 (12.0) 220 (23.8) � 0.001Tobramycin 386 (73.8) 112 (27.9) 498 (53.9) � 0.001
IPM R, imipenem-resistant; IPM S, imipenem-sensitive.

Epidemiology of Acinetobacter infections 745
When the risk factors were compared in IRAB and ISAB infections, neutropenia, malignancy, hae-modialysis, stay in ICU, and invasive procedures such as mechanical ventilation, central venous cath-eter, urinary catheter and nasogastric catheter were found to be signifi cant risk factors for IRAB infec-tions. Similar risk factors have been described in pre-vious studies. Particularly, stay in ICU and previous antibiotic exposure are the most important risk fac-tors for IRAB infections [3,5,17]. Patients in ICUs who require invasive procedures such as mechanical ventilation and central venous catheters are at risk for IRAB infections [3]. In a nationwide study from Spain, a hospital size of � 500 beds, previous antimi-crobial therapy, urinary catheter and surgery were independent risk factors for the acquisition of IRAB [4]. Distinct from other studies, neutropenia, malig-nancy and haemodialysis were found to be signifi cant risk factors in our study. Frequent hospitalization, use of antibiotics and invasive procedures may be an explanation for the high rates of IRAB infection in these patients. ISAB infections were seen signifi cantly more often in trauma patients. Contamination of wounds with ISAB from the environment and cross-infection in fi eld and referral hospitals may be expla-nations. In a multivariate analysis, haemodialysis, mechanical ventilation and malignancy were found to be independent risk factors for IRAB infections in our study. Although most A. baumannii infections occurred in the ICU (73.7%), stay in ICU was found not to be an independent risk factor for IRAB infec-tions in our study.
IRAB strains are endemic in many hospitals worldwide and frequently cause epidemics [18]. A. baumannii infections tend to occur in ICUs, espe-cially in intubated and mechanically ventilated patients [19]. In some institutions and geographic areas, Acinetobacter have accounted for 13 – 49% of ventilator-associated pneumonia [18,20,21]. Respi-ratory tract infections caused by A. baumannii were the most common in our study, and the proportion of IRAB infections was signifi cantly higher than ISAB infections ( p � 0.009). There were no statisti-cal differences in urinary tract, bloodstream, surgical site, and skin-soft tissue infection with regard to imi-penem resistance.
The lack of molecular studies to show clonal relationships among the A. baumannii strains was the most important limitation of our study. Therefore we are not able to reveal the risk factors that might be related to specifi c clones. As another limitation, our study was performed at 1 centre, and the results might not be applicable to others with different epidemiology. Each centre should determine its own epidemiological data to combat A. baumannii infections.
Carbapenem-resistant A. baumannii strains are often resistant to other antibiotic groups such as cephalosporins, aminoglycosides and fl uoroquinolo-nes [3,12,22]. Although the resistance in ISAB to aminoglycosides, fl uoroquinolones and cephalosporins was high in our study, the resistance rates were sig-nifi cantly higher in IRAB strains. Netilmicin and cefoperazone – sulbactam were the most active antibi-otics against both IRAB and ISAB strains. Baran et al. [3] reported similar results to our study. They found high resistance rates to various antibiotics in A. baumannii strains, and IRAB strains had higher resis-tance rates. Resistance limits the therapeutic options for the treatment of A. baumannii infections. Recently, a number of studies have reported on the effi cacy of colistin and tigecycline against multidrug-resistant A. baumannii strains [2,23,24]. However, these anti-biotics were not investigated in our study.
In conclusion, imipenem resistance is a growing problem in the ICU, especially in patients with pneu-monia caused by Acinetobacter strains. Furthermore, resistance to other antibiotics was higher among IRAB strains. Mortality was also higher in IRAB infections. Imipenem-resistant A. baumannii should be considered when treating nosocomial infections empirically, especially in patients on mechanical ven-tilation and haemodialysis and in those who have a malignancy.
Declaration of interest: The authors report no confl icts of interest. The authors alone are respon-sible for the content and writing of the paper.
Refere nces
Hanlon GW. The emergence of multidrug resistant Acineto-[1] bacter species: a major concern in the hospital setting. Lett Appl Microbiol 2005;41:375 – 8. Maragakis LL, Perl TM. Acinetobacter baumannii: epidemi-[2] ology, antimicrobial resistance, and treatment options. Clin Infect Dis 2008;46:1254 – 63. Baran G, Erbay A, Bodur H, Onguru P, Akinci E, Balaban N, [3] et al. Risk factors for nosocomial imipenem-resistant Acineto-bacter baumannii infections. Int J Infect Dis 2008;12:16 – 21. Cisneros JM, Rodriguez-Bano J, Fernandez-Cuenca F, [4] Ribera A, Vila J, Pascual A, et al. Spanish Group for Noso-comial Infection (GEIH) for the Spanish Society of Infec-tious Diseases and Clinical Microbiology (SEIMC): Risk-factors for the acquisition of imipenem-resistant Aci-netobacter baumannii in Spain: a nationwide study. Clin Microbiol Infect 2005;11:874 – 9. Lee SO, Kim NJ, Choi SH, Hyong Kim T, Chung JW, Woo [5] JH, et al. Risk factors for acquisition of imipenem-resistant Acinetobacter baumannii: a case-control study. Antimicrob Agents Chemother 2004;48:224 – 8. Playford EG, Craig JC, Iredell JR. Carbapenem-resistant [6] Acinetobacter baumannii in intensive care unit patients: risk factors for acquisition, infection and their consequences. J Hosp Infect 2007;65:204 – 11.
746 M. Dizbay et al.
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. [7] CDC defi nitions for nosocomial infections. Am J Infect Con-trol 1988;16:128 – 40. Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. [8] CDC defi nitions of nosocomial surgical site infection, 1992: a modifi cation of CDC defi nition of surgical wound infec-tions. Infect Control Hosp Epidemiol 1992;13:606 – 8. Clinical and Laboratory Standards Institute (CLSI). Per-[9] formance standards for antimicrobial susceptibility testing. 15 th Informational supplement. M100-S15. Wayne, PA: CLSI; 2005. Rodriguez-Bano J, Cisneros JM, Fernandez-Cuenca F, [10] Ribera A, Vila J, Pascual A, et al. Grupo de Estudio de Infec-ci ó n Hospitalaria (GEIH): Clinical features and epidemiol-ogy of Acinetobacter baumannii colonization and infection in Spanish hospitals. Infect Control Hosp Epidemiol 2004;25:819 – 24. Apisarnthanarak A, Pinitchai U, Thongphubeth K, Yuekyen [11] C, Warren DK, Fraser VJ. A multifaceted intervention to reduce pandrug-resistant Acinetobacter baumannii coloniza-tion and infection in 3 intensive care units in a Thai tertiary care center: a 3-year study. Clin Infect Dis 2008;47:760 – 7. Turner PJ, Greenhalgh JM. The activity of meropenem and [12] comparators against Acinetobacter strains isolated from European hospitals, 1997 – 2000. Clin Microbiol Infect 2003;9:563 – 7. Gales AC, Jones RN, Forward KR, Li ñ ares J, Sader HS, [13] Verhoef J. Emerging importance of multidrug-resistant Aci-netobacter species and Stenotrophomonas maltophilia as pathogens in seriously ill patients: geographic patterns, epi-demiological features, and trends in the SENTRY Antimi-crobial Surveillance Program (1997 – 1999). Clin Infect Dis 2001;32(Suppl 2):104 – 13. Yucesoy M, Yulug N, Kocagoz S, Unal S, Cetin S, Calangu S. [14] Antimicrobial resistance of Gram-negative isolates from intensive care units in Turkey: comparison to previous three years. J Chemother 2000;12:294 – 8. Aksaray S, Dokuzoguz B, Guvener E, Yucesoy M, Yulug N, [15] Kocagoz S, et al. Surveillance of antimicrobial resistance
among Gram-negative isolates from intensive care units in eight hospitals in Turkey. J Antimicrob Chemother 2000;45:695 – 9. Korten V, Ulusoy S, Zarakolu P, Mete B. Turkish MYSTIC [16] Study Group: Antibiotic resistance surveillance over a 4-year period (2000 – 2003) in Turkey: results of the MYSTIC Pro-gram. Diagn Microbiol Infect Dis 2007;59:453 – 7. del Mar Tomas M, Cartelle M, Pertega S, Beceiro A, Llinares P, [17] Canle D, et al. Hospital outbreak caused by a carbapenem-resistant strain of Acinetobacter baumannii: patient progno-sis and risk-factors for colonisation and infection. Clin Microbiol Infect 2005;11:540 – 6. Ferrara AM. Potentially multidrug-resistant non-fermenta-[18] tive Gram-negative pathogens causing nosocomial pneumo-nia. Int J Antimicrob Agents 2006;27:183 – 95. Garnacho-Montero J, Ortiz-Leyba C, Fern á ndez-Hinojosa [19] E, Aldab ó -Pall á s T. Acinetobacter baumannii ventilator-asso-ciated pneumonia: epidemiological and clinical fi ndings. Int Care Med 2005;31:649 – 55. Clark NM, Patterson J, Lynch PJ III. Antimicrobial resist-[20] ance among Gram-negative organisms in the intensive care unit. Curr Opin Crit Care 2003;9:413 – 23. Chastre J. Infections due to Acinetobacter baumannii in the [21] ICU. Semin Respir Crit Care Med 2003;24:69 – 78. Fluit AC, Jones ME, Schmitz FJ, Acar J, Gupta R, Verhoef J. [22] Antimicrobial susceptibility and frequency of occurrence of clinical blood isolates in Europe from the SENTRY antimi-crobial surveillance program, 1997 and 1998. Clin Infect Dis 2000;30:454 – 60. Dizbay M, Altuncekic A, Sezer BE, Ozdemir K, Arman D. [23] Colistin and tigecycline susceptibility among multidrug-resistant Acinetobacter baumannii isolated from ventilator-associated pneumonia. Int J Antimicrob Agents 2008;32:29 – 32. Sader HS, Jones RN, Dowzicky MJ, Fritsche TR. Antimi-[24] crobial activity of tigecycline tested against nosocomial bacterial pathogens from patients hospitalized in the intensive care unit. Diagn Microbiol Infect Dis 2005;52:203 – 8.
Copyright of Scandinavian Journal of Infectious Diseases is the property of Taylor & Francis Ltd and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.