Embed Size (px)
Citation preview

Ondrej Daum
Biopticka laborator & Sikl´s Institute of Pathology
Plzen, Czech Republic
(not related to GERD and systemic diseases)

(to say nothing of the GERD and the systemics)
Infectious esophagitis Viral (HSV, VZV, CMV, HIV)
Fungal (Candida, Aspergillus, Histoplasma, Cryptococcus, Blastomyces, Mucor, Coccidioides)
Bacterial (including Mycobacteria and Actinomyces)
Parasitic (Toxoplasma)
Eosinophilic esophagitis
Corrosive esophagitis
Radiation esophagitis
Toxic and drug/pill-associated esophagitis

LOW POWER• recognition / confirmation of
inflammatory nature
MEDIUM to HIGH
POWER• distribution and composition
of inflammatory infiltrate
• epithelial injury
• causative agent
Dg.
Personal
history
SerologyVirologyImmuno-
logy
Gross
Endo
Finding
Blood
count

Lymphocytic
Purulent
Eosinophilic
Granulomas
Sparse
GERD
Infectious
Crohn
GERD
Infectious
Drug/pill-associated
GERD
Eosinophilic esophagitis
Infectious
Crohn
Sarcoidosis
Mycobacterial
Corrosive
GVHD, Radiation
Toxic and drug-associated
Others

+ Eos & Neus
+ CLE
+ Eos & Neus
+ keratosis
+ mykoorganisms
focal distribution
+ granulomas
Lichenoid
interface changes
GERD
Candida
Crohn
Lichen planus
Lymphocytic
esophagitis

Lymphocytic esophagitis
? Definition:
> 20 (or 30 or 50) IELs/HPF
Peripapillary accentuation of IELs
Absent or rare Neus/Eos
Spongiosis
Absence of a known primary condition
Pattern associations:
Crohn diseases (pediatric biopsies!)
GERD (adults)
Allergic / Autoimmune / Immune deficiency (incl. HIV)
GSE
Achalasia
Infections
Personal history & Endoscopy:
Dysphagia, heartburn, bellyaches
Normal to BE
Hiatal hernia
Rings and furrows

Male, 12 years of age, esophageal ulcers


+ Eos & Lys
+ CLEGERD
+ keratosis
+ mykoorganisms
(+ Eos)
Candida
+ viral inclusions Viral esophagitis
+ pills in the ulcer
+ midesophagusPill esophagitis
History, serology,
immunology, IHC, virology
“Real” disease
Bystander

Candida in the esophagus
Clinical history:
Debilitated, immunocompromised (or not)
Dysphagia, odynophagia
“globus sensation”
“Real” candida
esophagitisBystander
Endoscopy:
Friable, hyperemic mucosa
White plaques to pseudomembranes
(sometimes black)
In advanced cases narrowed esophagus
Clinical history:
Non-specific
Symptoms of underlying disease
Endoscopy:
Usually a non-specific ulcer
Subtle white patch may be present
Inflammatory
infiltrate rich
in Neus
Pseudohyphae
Budding yeasts

“Real” candida
esophagitisBystander

Actinomyces in the esophagus
Usually an innocent bystander
Probably an ingested colony trapped
in an ulcer

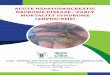
Herpetic esophagitis
Clinical history:
Neonates, babies
Immunocompromised
Reactivation in immunocompetent
Acute odynophagia, chest pain, fever
Endoscopy:
Distal half
Vesicles → Punched-out ulcers
↑ → Confluent ulcers
↑ → Haemorrhagic esophagitis
Enlarged ground glass cytoplasm
Cowdry A nuclear inclusions
Multinucleated squamous cells
BUT:
HSV proven by molecular genetics

CMV esophagitis
Clinical history:
Elderly
Debilitated
Immunocompromised
Non-specific symptoms
Endoscopy:
Distal half
Superficial ulcers
Squamous epithelium usually
shows only reactive changes and
inflammatory infiltrate
Eosinophilic intranuclear (and
small basophilic cytoplasmic)
inclusions are found in
endothelial cells, myofibroblasts
and macrophages
Courtesy of Cord Langner, M.D.

Pill esophagitis
Most common pills:
Doxycycline
Iron
Alendronate
Not the real pills:
Kayexalate
(sorbitol)

+ keratosis
+ mykoorganisms
(+ Neus)
Candida
+ viral inclusions Viral esophagitis
+ granulomas
+ distal GIT
involved
Crohn disease
+ parasites Parasitic esophagitis
+ blood Eos >1500/µl >
6 months
+other organs involved
HES
Features favoring EoE over GERD
↑ incidence of allergic diseases
Food impaction common
Dysphagia common
Mucosal rings and furrows common
Ulcers uncommon
pH commonly normal
Distal esophagus less severely affected
No response to PPIs
Response to immunosupression

Eosinophilic esophagitis
Histological signs of EoE
Eos count > 15/HPF (?)
Eo clusters to microabscesses
Degranulation of Eos
Epithelial spongiosis
Subepithelial sclerosis
?

Distal esophagus Proximal esophagus


Other differential dx.
Disease Clues
Eosinophilic gastroenteritis Gastrointestinal eosinophilia
Achalasia Endoscopy, motility studies
Drug hypersensitivity Pharmacological history
Vasculitis Complex symptomatology (and investigation)
Pemphigus Suprabasal clefts, akantholysis, skin manifestation, serology
Connective tissue diseases Complex symptomatology (and investigation)
GvHD Apoptosis, BMT history

Crohn disease
Up to 10% of CD cases
Most commonly pattern of lymphocytic esophagitis
Granulomas reported in up to 40%
Ileocolonic involvement crucial for the diagnosis
Other differential dx.
Sarcoidosis
Mycobacteria
Funghi
Vasculitis

Entity Clues
Corrosive esophagitis
History
Acute acidic: coagulative necrosis
Acute alkaline: liquefactive necrosis
Late stage: fibrosis
Sloughing esophagitis Debilitated patients, superficial coagulative necrosis
GvHD ↑ apoptosis, dyskeratotic keratinocytes, history
Mycophenolate esophagitis ↑ apoptosis, history
Colchicine toxicity Mitotic arrest, history
Taxanes toxicity Mitotic arrest, history
Scleroderma Submucosal fibrosis

Radiation esophagitis
Clinical history:
Dysphagia, odynophagia
Disordered motility
Possible additive effect of chemotherapy
Early findings:
Edematous, hyperemic mucosa
Erosions to ulcers
Degenerative and regenerative changes of
epithelium
Late findings:
Fibrosis
Strictures and webs
Acanthosis, parakeratosis

"Battle of Raab Campaign June 1809 " by Djmaschek at English Wikipedia.
Licensed under CC BY-SA 3.0 via Wikimedia Commonshttp://commons.wikimedia.org/wiki/File:Battle_of_Raab_Campaign_June_1809.JPG#/media/File:Battle_of_Raab_Campaign_June_1809.JPG
2000:900