Embed Size (px)
Citation preview

Version:X.X
Gültigab:XX.XX.2017
Revision:XX.XX.2019
Verfasser:TR
Geprüft:
Genehmigt:
SOPAkuttherapieSepsis Seite1von3
Bereich: Intensivmedizin
SOP Akuttherapie Sepsis
Bestätigung Sepsisverdacht
Infektionsverdacht / bestätigte Infektion q
≥ 2 SIRS-Kriterien
- Temperatur >38°C oder <36°C - Herzfrequenz > 90 bpm - Atemfrequnez > 20/min - Leukozyten >12.000/mm2 oder <4.000/mm2
q q q q
ODER
qSOFA ≥ 2
- Atemfrequenz ≥ 22 - akute Vigilanzänderung / -minderung (GCS<15) - syst. Blutdruck ≤ 100mmHg /Katecholaminbedarf
q q q
Notfall-PunkteparallelabarbeitenbeiSepsisverdacht–immerInfoanIOI-OA!!!
ZIELE: - Diagnose Sepsis - Diagnose Septischer Schock - Gewinnung adäquater mikrobiologischer Proben
- Eindeutiger infektiologischer Focus: - Septi-Fast durchgeführt
Diagnostik_Notfall (≤1h!)
IOI-Sepsis-Labor, 12-Kanal-EKG, BGA q
Verifikation Infektionsfocus / Focussuche I: TTE, Sono-Pleura, Sono-Abdomen, Wundbefund/Katheter, Urin-Status, ggf. Rö-Thorax
q
Verifikation septischer Schock • BGA: Lactat > 2 mmol/l “UND” • MAP ≥ 65 mmHg nur durch Vasopressoreneinsatz
q
Sepsis-PCR – bei unklarem Infektfocus und /oder septischem Schock q
Blutkulturen abnehmen (3 Pärchen!) q
MiBi-Diagnostik - Basis: Trachealsekret, Urin, Wund-/Drainageabstriche q
Erhebung SOFA-Score bei Aufnahme (Dokumentation ICM!) q
Für 6h nach Aufnahme stündliche BGA´s q

Version:X.X
Gültigab:XX.XX.2017
Revision:XX.XX.2019
Verfasser:TR
Geprüft:
Genehmigt:
SOPAkuttherapieSepsis Seite2von3
Therapie_Notfall (≤1h!)
ZVK-Anlage, bei V.a. katheterassoziierte Infektion oder unklarer Insertionszeitpunkt => Neuanalge ZVK, 1xBlutkultur aus altem ZVK und einschicken.
q
Anlage arterielle Druckmessung q
Beginn kalkulierte Antibiose (RS OA IOI), möglichst nach BK, ABER <1h! q
Hämodynamische Stabilisierung • Flüssigkeitssubstitution (30ml/kg KG über 3h) • Ziel-MAP ≥ 65 mmHg => ggf. Noradrenalin • Evaluierung des Volumenstatus (V.Cava-Sono, TTE, Leg-Raise-Test, PiCCO) • Regrediente Lactatkinetik, Lactat ≤ 2 mmol/l + ScvO2>70%
q q q q
ZIELE: - Beginn adäquater Antibiose - Etablierung ZVK und ART - Hämodynamische Stabilisierung (MAP >65mmHg, Lactat <2 mmol/l, ScvO2, >70%)
Erweiterte Diagnostik (<6h)
TTE/TEE => stagnierende / steigende Lactatkinetik / ScvO2<60% / Rekapillarisierungszeit > 3sec, Ausschluss Endokarditis (TEE)
=> siehe SOP „Echokardiographie“
q
Bronchoskopie => vermehrtes Trachealsekrekt, auffälliges Röntgenbild, eingeschränkter Gasaustausch, eingeschränkte Compliance
=> siehe SOP „Bronchoskopie“
q
Focussuche II => bei noch unklarem infektiologischen Focus => cCT /CT Thorax/Abdomen (mit KM)
q
PiCCO: => bei auffälligem TTE/TEE (EF<40%), Einsatz von Inotropika, erneut steigender Lactatkinetik unter Volumengabe und Vasopressortherapie, >2mg NA/h oder paralleler Einsatz von Vasopressin
=> Fakultativ: bei unklarem Volumenstatus, erhöhtem Volumenbedarf (> +4l/24h)
q
Spezielle MiBi (bei begründetem Verdacht / Risikodisposition) • Sputum: PCR => M. tuberculosis • Giemsa-Färbung: Pneumocystis jiroveci • Serum: Antigen => Galaktomannan - Aspergillose , CMV • Urin: Legionellenantigen • Stuhl: C.Diff. Toxin, Enterotoxin, Rota-/Noroviren • BAL: Galaktomannan – Aspergillose, Kultur: bakt. Atypier • PCR: CMV, HSV,RSV,Influenza, Parainfluenza • Färbung: Pneumocystis jiroveci, Toxoplasmose • Liquor-Probe: Kultur, laborchem. Analyse
q

Version:X.X
Gültigab:XX.XX.2017
Revision:XX.XX.2019
Verfasser:TR
Geprüft:
Genehmigt:
SOPAkuttherapieSepsis Seite3von3
Erweiterte Therapie (<6h)
Ggf. erweiterter Katheterwechsel (ZVK, ART, Shaldon, DK, Tubus,...) q
Erweitertes pulmonales Management: • NIV via CPAP-Maskentraining • Ggf. Intubation und mechanische Ventilation mit lungenprotektiver Beatmung
(Tidalvol. < 6ml/kg, Pmax <30mmHg, Pmax-PEEP <20mmHg, adäquater PEEP => nach FiO2 (siehe 1)
• Indikation für Bauchlagerung? • Indikation für VV-ECMO => siehe SOP „ECMO“ • Modifiziertes Respiratorsetting => siehe SOP „Beatmungsmanagement“
q q
q q q
Erweitertes kardiales Management: • Indikation für spezielle Inotropika/Inodilatoren • RV-Entlastung • mechanische Assist-Devices (VA-ECMO/ Impella) => siehe SOP „hämodynamisches Management“
q
Erweitertes renales Management: Etablierung kontinuierliche HDF • unzureichende Diuretikawirkung bei Hyperkaliämie oder zur
Negativbilanzierung • ausgeprägte Hypermyoglobinämie
q
Hydrocortisongabe (200mg/24h) erwägen q
Adäquate Thromboseprophylaxe (CAVE DIC) q
Frühzeitige enterale Ernährung => siehe SOP „Ernährung“ q
Abbildungen
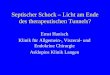
Abbildung1AusARDSNETventilationmanagement
Literaturverzeichnis
1) RhodesA,EvansLE,AlhazzaniW,LevyMM,AntonelliM,FerrerR,KumarA,SevranskyJE,SprungCL,NunnallyME,etal.(2017)SurvivingSepsisCampaign:InternationalGuidelinesforManagementofSepsisandSepticShock:2016.CritCareMed45:486-552.
2) SingerM,DeutschmanCS,SeymourC,etal.(2016)Thethirdinternationalconsensusdefinitionsforsepsisandsepticshock(sepsis-3).JAMA315:801-810
3) SurvivingSepsisCampaignBundles-Revised4/2015bytheSSCExecutiveCommittee,http://www.survivingsepsis.org/bundles/Pages/default.aspx
4) SurvivingSepsisCampaignBundles3h-Bundlehttp://www.survivingsepsis.org/sitecollectiondocuments/bundle-three-hour-ssc.pdf
5) RiversE,NguyenB,HavstadS,etal.Earlygoal-directedtherapyinthetreatmentofseveresepsisandsepticshock.NewEnglandJournalofMedicine.2001;345:1368-1377.
6) DellingerRP,LevyMM,RhodesA,etal.SurvivingSepsisCampaign:Internationalguidelinesformanagementofseveresepsisandsepticshock:2012.CriticalCareMedicine.2013Feb;41(2):580-637.
PEEP finding in ICU The correct PEEP for a patient to be on is a contentious issue.
PEEP has a many beneficial effects: PEEP has many detrimental effects Prevents repetitive recruitment/derecruitment Contributes to Mean Airway Pressure
Increases Pressure Induced Lung Injury Enhances alveolar ventilation
Contributes to overdistension of Alveoli Increases Volume Induced Lung Injury
Recruitment of atelectatic portion of the lung
Reduces venous return enhances sodium and watrer retention aggravates oliguria diminishes cardiac output
Reduce total lung water Enhances cardiac output in face of cardiac failure WIth these difficulties and the fact that many situations can either be an advantage or disadvantage it is recommended that PEEPs should initially be set and adjusted according to the ARDSnet PEEP table see below. Adjustments outside of these levels should only be made by experienced practitioners and the reasons for the particular adjustments carefully noted so that when the PEEP is reviewed by the next practitioner the reasoning can be debated. A PEEP of greater than 15 cm H2O is very rarely indicated and should only be utilised on the specific orders of a specialist whose name and reasoning should be noted so that the matter can be discussed where appropriate
ARDSNET ventilation management Assist control mode—volume ventilation Reduce tidal volume to 6 ml/kg predicted body weight Keep Pplat <30 cm H2O Reduce TV as low as 4 ml/kg predicted body weight* to limit Pplat to <30cmH2O Maintain SaO2/SpO2 88%–95% The chart below gives anticipated PEEP setting at various FIDa requirements:
FIO2 % 30 40 40 50 50 60 70 70 70 80 90 90 90 100
PEEP cmH2O
5 5 8 8 10 10 10 12 14 14 14 16 18 20–24 *Predicted body weight calculation Male = 50+0.91 [height (cm)_152.4] Female = 45.5+0.91 [height (cm)_152.4] TV Tidal volume SaO2 arterial blood saturation SpO2 pulse oximeter blood saturation PEEP, positive end-expiratory pressure
PEEP too low High airway pressure to force open atelectactic lung units, paper clip effect
PEEP too high High airway pressure over distend lung units barotrauma
PEEP correct Maximal tidal volume for lowest pressure change
Recognise when tidal volumes drop as PEEP increased (pressure control) orplateau pressures increase when PEEP increased (volume control)
Recognise when tidal volumes increase as PEEP increased (pressure control) or plateau pressures decrease when PEEP increased (volume control)













![Peer Review Konzept - uniklinikum-jena.de · „Schwere Sepsis oder septischer Schock“ [Indikator 5.4 der Qualitätsberichte] für jede Kategorie (bis 400 Betten, bis 800 Betten,](https://img.pdfslide.net/doc/110x75/5d60910988c993e34a8b88f6/peer-review-konzept-uniklinikum-jenade-schwere-sepsis-oder-septischer.jpg)


![Das Auftreten von unreifzelligen Granulozyten bei ... · Sepsis, schwere Sepsis und septischer Schock getrennt definiert und unter- liegen auch spezifischen Diagnosekriterien [10]](https://img.pdfslide.net/doc/110x75/5e0c03b4db38a55cd046c767/das-auftreten-von-unreifzelligen-granulozyten-bei-sepsis-schwere-sepsis-und.jpg)