Embed Size (px)
Citation preview

Notionsdebasesurlesprescriptionsdepsychotropeschezl’enfantetl’adolescent
PrOlivierBONNOTCHU&UniversitédeNantes,Psychiatriedel’Enfantetdel’Adolescentwww.u2peanantes.org &[email protected]
EnseignementNantes– Angers2018

Conflitd’interêt quevousdevezconnaître:
A- HonorairesetAdBoard deLaboratoireenlienaveclesMaladiesRares(Orphan &Actelion)+AdBoard deSHIRE(Quasym)
B- Coordonnateurd’étudeindustriellespourlecomptedemonCHUavecOTSUKA(Aripiprazol etLurasidone)etLundbeck(Venlafaxine)

C’estutile

Maisondoitéviterdedéborderducadre…
Mêmesic’esttentant…

Ilexistedesindications,desrecommandations,destravauxscientifiquesetdesmodalitésdesurveillance àconnaître.

Ilexistedesindications,desrecommandations,destravauxscientifiquesetdesmodalitésdesurveillance àconnaître.
Cesdonnéesévoluent régulièrement…
Nousallonsvoir:
ü Lesantipsychotiquesü Lesantidépresseursü Lesstimulantsü Lesthymorégulateursü Etnousfinironsparquelquesgénéralités

Antipsychotiques
• Schizophrénies• TroublesBipolaires• GillesdelaTourette
• AgitationdanslaDI
• Autismeettroublesdudéveloppement

Stahl's Essential Psychopharmacology Online
Revised and Updated Edition 4th Edition
ActionPrincipaleANTAGONISTE
D2
Agoniste partiel :Aripiprazole,Quetiapine et
Clopzapine
ActionsecondaireANTAGONISTE5HT2Aetparfois Agonistes partiels
en+(Ari)
Effet sédatif ++Poids ?
Implicationégalement poidsD2,5HT1A,5HT2C
etalpha
Role++dansl’insensibilité a
l’insuline

Produit IndicationsAMMpédiatrique Dosages recommandés
Risperidone 5-18anspourlesTroublesdesConduites– Nonrecommandé 0.25mgà1mg
Aripiprazole Àpartirde15anspourSchizophréniesÀ partirde13anspourBipolaireNonindiquédansl’Autisme– Nonrecommandéendehorsdecesâges.
5à30mgRecommandationdesurveillancerisquesuicidairechezpatientsà risque
Quetiapine Nonrecommandéavant18ans 50 à300- 600mg
Amisulpride Nonrecommandé avant18ans,CIavant15 400– 800 – 1200mg
Olanzapine Nonrecommandé avant18ans 5– 15mg– 25mg
Clozapine Nedoitpasêtreprescrit avant16ans 100– 450 – 900mg
Paliperidone « pasdedonnées » Ensuitederisperidone 50à100mg/mois(inj)
Cyamenazine Àpartirde3ansdansagitation /agressivité 5- 50– 100mg
Lurasidone PASSUR LEMARCHEENFRANCE
Ziprasidone PASSUR LEMARCHEENFRANCE
Asenapine PASSUR LEMARCHEENFRANCE
Iloperidone PASSUR LEMARCHEENFRANCE
AMMenFranceen2017AdaptéparO.BonnotdeVidalNovembre2017

RecommandationsdesurveillanceCAMESAPringsheim,T.etal.(2012).Paediatr Chil Health Suppl B:12B-21B.
Début 1mois 2mois 3mois 6mois 9mois 1an
Taille,PoidsetIMC X X X X X X XTourdeTaille(ombilic) X X X X X X X
TensionArterielle X X X X X X XExamenNeurologique X X X X X X X
Glycémieàjeun(≤6.1mmol/l)Insulineàjeun(≤100μmol/l)Cholestéroltotal(≤5.2mmol/l)
HDL(≥1.05mmol/l)LDL(≤3.35mmol/l)
Triglycéride(≤1.5mmol/l)
X X X X
ASAT/ALAT X X X X X
Prolactine(1Getrisperidone) X X X
25OHD3 X XTableaudesurveillancedeseffetsindésirablesdesantipsychotiquesadaptédesrecommandationscanadiennesCAMESA(4)Taille,Poids,IMCetTensionArtériellesontenpercentileetenrapportavecl’âgeetlesexe(tableauxhttp://u2pea.free.fr).

RecommandationsdesurveillanceHAS2010calquésurl’adulte.
Début 1mois 2mois 3mois 6mois 9mois 1an
Taille,PoidsetIMC X X X X X XTourdeTaille(ombilic) X X
TensionArterielle X XExamenNeurologique X X
Glycémieàjeun(≤6.1mmol/l)Insulineàjeun(≤100μmol/l)Cholestéroltotal(≤5.2mmol/l)
HDL(≥1.05mmol/l)LDL(≤3.35mmol/l)
Triglycéride(≤1.5mmol/l)
X X X X X XX/5ans
ASAT/ALAT
Prolactine(1Getrisperidone)
25OHD3TableaudesurveillancedeseffetsindésirablesdesantipsychotiquesadaptédesrecommandationscanadiennesCAMESA(4)Taille,Poids,IMCetTensionArtériellesontenpercentileetenrapportavecl’âgeetlesexe(tableauxhttp://u2pea.free.fr).

• ComparaisonOlanzapine &Risperidone vsAP1G(n=100)8semaines:PasdedifférencesurlaPANNS
Linemarie Sikich etcoll.,2008AJP,TEOSSstudy results inthesamelineasSikich 2004etGothelf 2003
PourquoiutiliserdesAP1Genalternative?

Shawetal.,2006
No statistical difference but a little advantage for Clozapine
• Kumra compare la clozapine(n=18) et lʼolanzapine (n=21) àforte dose (26.2 mg [10-30])
• Lʼétude de Shaw comparant laclozapine (n=12) et lʼolanzapine(n=13) à des doses classiques
More patient are responding to Clozapine (66 vs 33)
Efficacy profil is similar (Clz better on SANS p = .1)
Kumra etal.,2009
L’olanzapine estelleunealternativealaclozapine ?

Antipsychotique2ème G
RisperidoneAripriprazoleQuetiapine
Continuer6-9moispuischercherdoseminimaleefficace.
ChangerpourunautreAP2GPas
d’améliorationet/ouEI
améliorationetpeud’EI
Pasd’amélioration
et/ouEI
Discuter:1. Olanzapine fortedose2. Clozapine3. AP1G4. Association2AP?
améliorationetpeud’EI
améliorationetpeud’EI
Pasd’amélioration
et/ouEI
Discuterautrealternativeci-dessus
Pasd’amélioration
et/ouEI
Discuter:1. ECT2. rTMS3. dTCS
Pasd’améliorationpenser:1. Noncompliance=DOSAGEMED2. PathosOrganiquesAssociées=BILAN
StratégiethérapeutiquemédicamenteusedanslesSchizophréniesdel’Enfantetdel’AdolescentAdaptéparO.BonnotdeNICE2014(https://www.nice.org.uk/guidance/cg178),AACAP2013(http://www.jaacap.com/article/S0890-8567(13)00112-3/pdf),HAS2013
CalculactivitéCYP2D6informatif

Ilexisteplusde18typesdeCytochromeP450
LeplusintéressantenpsychiatrieestleCYP2D6
IlexisteunecentainedepolymorphismesduCYP2D6
UltraRapidPoorExtensive
= - +
EI EI
Moinsefficace

Metformininpreventionandtreatmentofantipsychoticinducedweightgain:asystematicreviewandmeta-analysis
• BMCPsychiatry,2016
• Revuesystématique
• Quel est lerationnel ?
Onparlebcp delaMetformine,KESACO?
chronique etaigue
Enfantvsadulte

Metformininpreventionandtreatmentofantipsychoticinducedweightgain:asystematicreviewandmeta-analysis
• BMCPsychiatry,2016
• Revuesystématique
• Quel est lerationnel ?
Onparlebcp delaMetformine,KESACO?
chronique vsaigue
Enfantetadulte

Aquelle dose?
Onparlebcp delaMetformine,KESACO?
Pourquoi ?• EtudeDanoise,2016(Rajkumar etal.,2016)
• AmericanJournalofPsychiatry
• 2700000personnes de77à 2013
• 14118avecdiabète (0.52%)
• 8945avecschizophrénie (0.33%)
Ratioderisque 3.64 entreSchizo avecousanstraitement parrapportaudiabète !3.06 aveclesAP1Get3.44 aveclesAP2G(sansdifférence staths entrelesdeux)

Signes NeurologiquesInduits
Descriptionsuccinte Traitement :toujours trouver ladoseminimale efficace etenvisager dedonner delaclozapine
Parkinsonisme Tremblements,lenteur,symptômes unilateraux Anticholinergique, propanolol,clonazepam,amantadineou mirtazapine
DyskinésieMouvement anormaux,faceetboucherépétitifs
Clonazepamou tetrabénazine,voire lévétiracétam
Akathisie Besoindebougersansarrêt Tardive:peu dettt efficace,tetrabénazine,reserpineou lorazépam
Dystonie Postureanormalducoprs totaleoupartielle
Tardive:Anticholinergique etsi inneficace envisager toxine botulique voirestimulationcérabrale profondeAigue :Diphénhydramine ou anticholinergique ou diazépam IV
Et aussi,dysarthrie,dysphonie,hypersialorrhée,criseoculogyreoubradycinésie
Unpetitrappelutile…

Efficacitémodéréemaispasnullesurlestroublesducomportementdansl’autismeavecousansDIavecdesOdd Rationplutôtcorrectde6à12,enfaveurdelarisperidone d’etre groupe,répondeur.
Cohenetal,2013
Autisme

Antidépresseurs
üEtatDépressifMajeurüAnxiétéüTroubleObsessionnelCompulsif

TADSteam,AmJPsy,2009
Acute Consolidation Continuation Follow-up
Le traitement combiné accélère et le traitement long renforce les bénéficesLe traitement combiné diminue le risque suicidaire.
The Treatment for Adolescents With Depression Study (TADS): Outcomes Over 1 Year of Naturalistic Follow-Up

23
Pharmacothérapie jamais en premiere intention : TCC et Thérapie Interpersonnelle sont les seulesefficaces.…Zhou X, Qin B, Whittington C, et al.. 2015 Word Psychiatry

LaFluoxetineest leseul plusefficace quelePlacébo Cipriani2016Lancet

LaFluoxetineest leseul plusefficace quelePlacébo Cipriani2016Lancet
Fluoxetine pourladépression,c’estclair?

ANXIETE
Locheretal,2017,JAMA

TOCou SOC
Gelleretal,2003,AmJPsy
EfficacesurleTOC
ES=0.46modérée
CLOM Anafranil>
SSRI

TOCou SOC
Locheretal,2017,JAMA

TOC
Sertraline àpartirde6ans,Fluoxetine (8ans),Fluvoxamine (8ans)
Continuer6moisà1ansmoisencherchantdoseminimaleefficace
ChangerpourunautreIRSPas
d’améliorationet/ouEI
améliorationetpeud’EI
Pasd’amélioration
et/ouEI
Discuter:1. AP2. Clozapine3. Clonidine siTourette
améliorationetpeud’EI
améliorationetpeud’EI
Pasd’amélioration
et/ouEI
Discuterautrealternativeci-dessus
Pasd’amélioration
et/ouEIDiscuter:Stimulationcérébrale
Pasd’améliorationpenser:1. Noncompliance=DOSAGEMED2. Patho OrganiqueAssociée=BILAN
StratégiethérapeutiquemédicamenteusedanslesTOC,l’anxiétéetleTouretteAdaptéparO.BonnotdeNICE2010etHAS
L’associationavecunepsychothérapie,préférentiellementTCCsitrèshandicapant,estIMPERATIVE

Hammad,T.A.etal.ArchGenPsychiatry2006
RRX2pourlesidéesETlestentativesdesuicides
LaquestiondurisqueSuicidaire

Tiihonenetal,2006,ArchGenPsy
issues, partly because deaths and severe suicidal behav-ior are too infrequent incidents to be detected in suffi-cient numbers for statistical analyses. Our database in-cluded follow-up data from 100% of all hospital-treatedsurvivors of attempted suicide in Finland from 1997 to2003. Thus, it was possible to detect more than 600 sui-cides and 7000 severe suicide attempts leading to hos-pitalization. Both of these numbers are more than 5-foldgreater than the figures of any previous studies.10,12-14,27
Our results suggest that the discrepancy between RCTs10-12
(showing an increase in suicide attempts) and observa-tional studies6-9 (showing a decrease in completed sui-cides) can be explained by the fact that antidepressantuse is associated with an increased risk of nonfatal sui-cidal behavior and, at the same time, a decreased risk offatal suicidal behavior. This opposite type of effect onfatal vs nonfatal suicidal behavior may be explained byan increased risk of intoxication because of easy avail-ability of means (antidepressant medication), resultingin an increase in nonfatal suicidal behavior, and by adecrease in the incidence of violent and more fatal meth-ods of suicide attempts, such as hanging and shooting.
It is not possible to adjust all confounding factors ina nonrandomized observational study. Our results showthat previous suicide attempts and antidepressant treat-ment were the most important background variables con-tributing to the risk of forthcoming suicidal behavior, aspreviously observed by Jick et al.14 In our study, it wasnot possible to obtain information on psychiatric diag-noses (except a psychosis diagnosis, which was an ex-clusion criterion). The main results were not affected byadjustment of these and numerous other background vari-ables (ie, the crude and adjusted RRs were basically thesame, except for the risk of suicide during SNA use andfor the risk of death during TCA and SNA use). How-ever, it is possible that despite an adjustment of the mostimportant confounding factors,14 there may be the pos-sibility of residual bias, which could contribute to an in-
creased risk of suicide attempts among patients with medi-cation. To minimize the residual confounding caused bypatient selection, we analyzed the risk of attempted sui-cide, completed suicide, and death (Table 7) among pa-tients who had never used antidepressants, those who had
Table 4. Data for Suicide Attempts Obtained by Using Medication as a Time-Dependent Variable*
MedicationNo. of
Person-YearsNo. of Suicide
Attempts
Incidenceper 1000
Person-Years
RR (95% CI)
P ValueCrude Adjusted
TCAs 923 159 172.3 1.28 (1.09-1.49) 1.60 (1.33-1.91) !.001Amitriptyline 469 89 189.8 1.40 (1.14-1.73) 1.67 (1.31-2.11) !.001Doxepin hydrochloride 454 70 154.2 1.14 (0.90-1.44) 1.49 (1.13-1.95) .004
SSRIs 6946 1224 176.2 1.36 (1.28-1.48) 1.54 (1.42-1.66) !.001Fluoxetine 2081 394 189.3 1.42 (1.28-1.57) 1.54 (1.37-1.74) !.001Citalopram hydrobromide 2752 478 173.7 1.30 (1.19-1.43) 1.55 (1.38-1.74) !.001Paroxetine hydrochloride 845 139 164.5 1.22 (1.03-1.44) 1.63 (1.33-1.99) !.001Sertraline 850 126 148.2 1.09 (0.92-1.30) 1.41 (1.15-1.72) .002Fluvoxamine maleate 418 87 207.9 1.54 (1.25-1.90) 1.75 (1.38-2.22) !.001
SNAs 3736 663 177.5 1.34 (1.24-1.45) 1.57 (1.42-1.73) !.001Mianserin hydrochloride 600 107 178.2 1.32 (1.09-1.60) 1.58 (1.29-1.94) !.001Mirtazapine 2113 362 171.3 1.28 (1.15-1.42) 1.50 (1.32-1.70) !.001Venlafaxine hydrochloride 1022 194 189.8 1.41 (1.22-1.63) 1.79 (1.52-2.11) !.001
Other antidepressants 4146 1178 284.2 2.31 (2.17-2.46) 1.87 (1.70-2.06) !.001All antidepressants 15 751 3224 204.7 1.93 (1.84-2.20) 1.64 (1.54-1.74) !.001No antidepressant use 36 836 3912 106.2 1.00 1.00 NA
Abbreviations: See Table 3.*The RRs were adjusted as explained in the second footnote to Table 3.
0 1 2 3 4 5Adjusted Relative Risk
Med
icat
ion
TCAs
Amitriptyline
Doxepin
SSRIs
Fluoxetine
Citalopram
Paroxetine
Sertraline
Fluvoxamine
SNAs
Mianserin
Mirtazapine
Venlafaxine
Other Antidepressants
All Antidepressants
No Antidepressant Use
Figure 3. Relative risk and 95% confidence interval of suicide attemptsamong subjects aged 10 to 19 years obtained by using medication as atime-dependent variable. The relative risks were adjusted as explained in thelegend to Figure 1. Because of the restricted scale of the figure, the upperends of the confidence intervals for TCAs, amitriptyline, mianserin, andvenlafaxine are not shown. Abbreviations and complete drug names aregiven in the legend to Figure 1.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 63, DEC 2006 WWW.ARCHGENPSYCHIATRY.COM1363
©2006 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 11/27/2014
attempts leading to hospitalization, and 1583 deaths wererecorded during the follow-up (mean, 3.4 years). Table1shows the sociodemographic and clinical data of pa-tients with vs those without antidepressant use duringfollow-up, and the relative effect of background vari-ables on the risk of suicides, suicide attempts, and mor-tality is shown in Table 2. The number of previous sui-cide attempts was the strongest predictor of suicideattempt, and age was the strongest predictor of death andsuicide.
SUICIDES
The risks of suicide associated with the use of each typeof TCA, SSRI, and SNA vs no antidepressant use areshown in Figure 1 and Table 3. The adjusted RR forsuicide with the use of any antidepressant vs no use was0.91. Selective serotonin reuptake inhibitor use was asso-ciated with a slightly lower, and SNA use with a slightlyhigher, risk of suicide than no antidepressant use, butthese differences were not statistically significant. Fluox-etine use was associated with significantly decreasedrisk, and venlafaxine use with increased risk, of suicide.In the subpopulation of subjects aged 10 to 19 years, 28suicides were recorded (7 during any antidepressant useand 21 during no antidepressant use) (RR, 1.33; 95%confidence interval [CI], 0.50-3.51). No significant dif-ferences (P!.18) were observed between the antidepres-sant groups (TCA, SSRI, and SNA) or specific antidepres-sants vs no use.
SUICIDE ATTEMPTS
The RR of suicide attempts leading to hospitalization wasmarkedly increased during the use of all antidepres-sants when compared with no antidepressant use(Figure 2 and Table 4). The results among the sub-group of subjects aged 10 to 19 years indicated a slightlyhigher risk increase than in the total population duringthe use of SSRIs (Figure 3 and Table 5).
TOTAL MORTALITY
Mortality was substantially (31%-41%) lower during theuse of all antidepressants in the group comparison (TCA,SSRI, or SNA vs no antidepressant use), and the RR forthe use of any antidepressant (vs no antidepressant use)was 0.64, corresponding to a population-attributable frac-tion of 12%. In the analysis of specific medications, fluox-etine, citalopram, sertraline, mianserin, and mirtaza-pine use differed significantly from the mortality duringno antidepressant use (Figure 4 and Table 6). Only44 deaths were detected among subjects aged 10 to 19years, and no significant differences were observed be-tween antidepressant use and no use, except for parox-etine (RR, 5.44; 95% CI, 2.15-13.73; P".001) (4 deathsper 99 person-years). The causes of death during parox-etine use were suicide (n=1), drowning (n=1), and un-intentional injuries (n=2). Also, fluvoxamine (RR, 10.13;95% CI, 2.14-47.95) was associated with an increased riskof death, but this was based on only 1 death during 45person-years.
The risk of death during antidepressant use vs no usewas further studied in a secondary analysis on the causesof death by analyzing mortality in the 4 most frequentcategories (unintentional injuries and violence, n=825;diseases of the circulatory system, n=256; neoplasms,n=97; and diseases of the respiratory system, n=49).26
Antidepressant medication (any medication vs no medi-cation) was associated with a significantly lower mortal-ity in the category of diseases of the circulatory system(RR, 0.48; 95% CI, 0.34-0.68; P=.002), but not in othercategories. Selective serotonin reuptake inhibitor usewas associated with substantially decreased risk of allcardiovascular- and cerebrovascular-related deaths (RR,0.42; 95% CI, 0.24-0.71; P=.001) (RR for the risk ofcardiovascular-related death, 0.37 [95% CI, 0.17-0.78];and RR for the risk of cerebrovascular-related death,0.13 [95% CI, 0.02-1.06]). Serotonergic-noradrenergicantidepressant use was associated with a borderline sig-nificant decrease of all cardiovascular- and cerebro-vascular-related deaths (RR, 0.53; 95% CI, 0.29-0.98;P=.043). No statistically significant (P!.23) effects wereobserved for any other class of antidepressants or causesof deaths.
0 1 2 3Adjusted Relative Risk
Med
icat
ion
TCAs
Amitriptyline
Doxepin
SSRIs
Fluoxetine
Citalopram
Paroxetine
Sertraline
Fluvoxamine
SNAs
Mianserin
Mirtazapine
Venlafaxine
Other Antidepressants
All Antidepressants
No Antidepressant Use
Figure 1. Relative risk and 95% confidence interval of suicides obtained byusing medication as a time-dependent variable. The relative risks wereadjusted with the propensity score method, and by including sex, age,geographical location (as strata), number of suicide attempts before theindex hospitalization, number of suicide attempts during follow-up, use ofmultiple antidepressant medications, and number of purchasedantidepressant prescriptions during the previous year in the model.SNA indicates serotonergic-noradrenergic antidepressant; SSRI, selectiveserotonin reuptake inhibitor; and TCA, tricyclic antidepressant. Citalopramwas given as citalopram hydrobromide; doxepin, as doxepin hydrochloride;fluvoxamine, as fluvoxamine maleate; mianserin, as mianserin hydrochloride;paroxetine, as paroxetine hydrochloride; and venlafaxine, as venlafaxinehydrochloride.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 63, DEC 2006 WWW.ARCHGENPSYCHIATRY.COM1361
©2006 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 11/27/2014
SuicideTentativedeSuicide
Finland – 1997-2003 All hospitalized patients because of Suicide Attempt N = 15390 F/U = 3.4 years 602 suicide, 1583 deaths 7466 SA leading to hospital
Antidepressants andtherisk ofsuicide,SA,andoverall Mortality inanationwide cohort

Tiihonenetal,2006,ArchGenPsy
issues, partly because deaths and severe suicidal behav-ior are too infrequent incidents to be detected in suffi-cient numbers for statistical analyses. Our database in-cluded follow-up data from 100% of all hospital-treatedsurvivors of attempted suicide in Finland from 1997 to2003. Thus, it was possible to detect more than 600 sui-cides and 7000 severe suicide attempts leading to hos-pitalization. Both of these numbers are more than 5-foldgreater than the figures of any previous studies.10,12-14,27
Our results suggest that the discrepancy between RCTs10-12
(showing an increase in suicide attempts) and observa-tional studies6-9 (showing a decrease in completed sui-cides) can be explained by the fact that antidepressantuse is associated with an increased risk of nonfatal sui-cidal behavior and, at the same time, a decreased risk offatal suicidal behavior. This opposite type of effect onfatal vs nonfatal suicidal behavior may be explained byan increased risk of intoxication because of easy avail-ability of means (antidepressant medication), resultingin an increase in nonfatal suicidal behavior, and by adecrease in the incidence of violent and more fatal meth-ods of suicide attempts, such as hanging and shooting.
It is not possible to adjust all confounding factors ina nonrandomized observational study. Our results showthat previous suicide attempts and antidepressant treat-ment were the most important background variables con-tributing to the risk of forthcoming suicidal behavior, aspreviously observed by Jick et al.14 In our study, it wasnot possible to obtain information on psychiatric diag-noses (except a psychosis diagnosis, which was an ex-clusion criterion). The main results were not affected byadjustment of these and numerous other background vari-ables (ie, the crude and adjusted RRs were basically thesame, except for the risk of suicide during SNA use andfor the risk of death during TCA and SNA use). How-ever, it is possible that despite an adjustment of the mostimportant confounding factors,14 there may be the pos-sibility of residual bias, which could contribute to an in-
creased risk of suicide attempts among patients with medi-cation. To minimize the residual confounding caused bypatient selection, we analyzed the risk of attempted sui-cide, completed suicide, and death (Table 7) among pa-tients who had never used antidepressants, those who had
Table 4. Data for Suicide Attempts Obtained by Using Medication as a Time-Dependent Variable*
MedicationNo. of
Person-YearsNo. of Suicide
Attempts
Incidenceper 1000
Person-Years
RR (95% CI)
P ValueCrude Adjusted
TCAs 923 159 172.3 1.28 (1.09-1.49) 1.60 (1.33-1.91) !.001Amitriptyline 469 89 189.8 1.40 (1.14-1.73) 1.67 (1.31-2.11) !.001Doxepin hydrochloride 454 70 154.2 1.14 (0.90-1.44) 1.49 (1.13-1.95) .004
SSRIs 6946 1224 176.2 1.36 (1.28-1.48) 1.54 (1.42-1.66) !.001Fluoxetine 2081 394 189.3 1.42 (1.28-1.57) 1.54 (1.37-1.74) !.001Citalopram hydrobromide 2752 478 173.7 1.30 (1.19-1.43) 1.55 (1.38-1.74) !.001Paroxetine hydrochloride 845 139 164.5 1.22 (1.03-1.44) 1.63 (1.33-1.99) !.001Sertraline 850 126 148.2 1.09 (0.92-1.30) 1.41 (1.15-1.72) .002Fluvoxamine maleate 418 87 207.9 1.54 (1.25-1.90) 1.75 (1.38-2.22) !.001
SNAs 3736 663 177.5 1.34 (1.24-1.45) 1.57 (1.42-1.73) !.001Mianserin hydrochloride 600 107 178.2 1.32 (1.09-1.60) 1.58 (1.29-1.94) !.001Mirtazapine 2113 362 171.3 1.28 (1.15-1.42) 1.50 (1.32-1.70) !.001Venlafaxine hydrochloride 1022 194 189.8 1.41 (1.22-1.63) 1.79 (1.52-2.11) !.001
Other antidepressants 4146 1178 284.2 2.31 (2.17-2.46) 1.87 (1.70-2.06) !.001All antidepressants 15 751 3224 204.7 1.93 (1.84-2.20) 1.64 (1.54-1.74) !.001No antidepressant use 36 836 3912 106.2 1.00 1.00 NA
Abbreviations: See Table 3.*The RRs were adjusted as explained in the second footnote to Table 3.
0 1 2 3 4 5Adjusted Relative Risk
Med
icat
ion
TCAs
Amitriptyline
Doxepin
SSRIs
Fluoxetine
Citalopram
Paroxetine
Sertraline
Fluvoxamine
SNAs
Mianserin
Mirtazapine
Venlafaxine
Other Antidepressants
All Antidepressants
No Antidepressant Use
Figure 3. Relative risk and 95% confidence interval of suicide attemptsamong subjects aged 10 to 19 years obtained by using medication as atime-dependent variable. The relative risks were adjusted as explained in thelegend to Figure 1. Because of the restricted scale of the figure, the upperends of the confidence intervals for TCAs, amitriptyline, mianserin, andvenlafaxine are not shown. Abbreviations and complete drug names aregiven in the legend to Figure 1.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 63, DEC 2006 WWW.ARCHGENPSYCHIATRY.COM1363
©2006 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 11/27/2014
attempts leading to hospitalization, and 1583 deaths wererecorded during the follow-up (mean, 3.4 years). Table1shows the sociodemographic and clinical data of pa-tients with vs those without antidepressant use duringfollow-up, and the relative effect of background vari-ables on the risk of suicides, suicide attempts, and mor-tality is shown in Table 2. The number of previous sui-cide attempts was the strongest predictor of suicideattempt, and age was the strongest predictor of death andsuicide.
SUICIDES
The risks of suicide associated with the use of each typeof TCA, SSRI, and SNA vs no antidepressant use areshown in Figure 1 and Table 3. The adjusted RR forsuicide with the use of any antidepressant vs no use was0.91. Selective serotonin reuptake inhibitor use was asso-ciated with a slightly lower, and SNA use with a slightlyhigher, risk of suicide than no antidepressant use, butthese differences were not statistically significant. Fluox-etine use was associated with significantly decreasedrisk, and venlafaxine use with increased risk, of suicide.In the subpopulation of subjects aged 10 to 19 years, 28suicides were recorded (7 during any antidepressant useand 21 during no antidepressant use) (RR, 1.33; 95%confidence interval [CI], 0.50-3.51). No significant dif-ferences (P!.18) were observed between the antidepres-sant groups (TCA, SSRI, and SNA) or specific antidepres-sants vs no use.
SUICIDE ATTEMPTS
The RR of suicide attempts leading to hospitalization wasmarkedly increased during the use of all antidepres-sants when compared with no antidepressant use(Figure 2 and Table 4). The results among the sub-group of subjects aged 10 to 19 years indicated a slightlyhigher risk increase than in the total population duringthe use of SSRIs (Figure 3 and Table 5).
TOTAL MORTALITY
Mortality was substantially (31%-41%) lower during theuse of all antidepressants in the group comparison (TCA,SSRI, or SNA vs no antidepressant use), and the RR forthe use of any antidepressant (vs no antidepressant use)was 0.64, corresponding to a population-attributable frac-tion of 12%. In the analysis of specific medications, fluox-etine, citalopram, sertraline, mianserin, and mirtaza-pine use differed significantly from the mortality duringno antidepressant use (Figure 4 and Table 6). Only44 deaths were detected among subjects aged 10 to 19years, and no significant differences were observed be-tween antidepressant use and no use, except for parox-etine (RR, 5.44; 95% CI, 2.15-13.73; P".001) (4 deathsper 99 person-years). The causes of death during parox-etine use were suicide (n=1), drowning (n=1), and un-intentional injuries (n=2). Also, fluvoxamine (RR, 10.13;95% CI, 2.14-47.95) was associated with an increased riskof death, but this was based on only 1 death during 45person-years.
The risk of death during antidepressant use vs no usewas further studied in a secondary analysis on the causesof death by analyzing mortality in the 4 most frequentcategories (unintentional injuries and violence, n=825;diseases of the circulatory system, n=256; neoplasms,n=97; and diseases of the respiratory system, n=49).26
Antidepressant medication (any medication vs no medi-cation) was associated with a significantly lower mortal-ity in the category of diseases of the circulatory system(RR, 0.48; 95% CI, 0.34-0.68; P=.002), but not in othercategories. Selective serotonin reuptake inhibitor usewas associated with substantially decreased risk of allcardiovascular- and cerebrovascular-related deaths (RR,0.42; 95% CI, 0.24-0.71; P=.001) (RR for the risk ofcardiovascular-related death, 0.37 [95% CI, 0.17-0.78];and RR for the risk of cerebrovascular-related death,0.13 [95% CI, 0.02-1.06]). Serotonergic-noradrenergicantidepressant use was associated with a borderline sig-nificant decrease of all cardiovascular- and cerebro-vascular-related deaths (RR, 0.53; 95% CI, 0.29-0.98;P=.043). No statistically significant (P!.23) effects wereobserved for any other class of antidepressants or causesof deaths.
0 1 2 3Adjusted Relative Risk
Med
icat
ion
TCAs
Amitriptyline
Doxepin
SSRIs
Fluoxetine
Citalopram
Paroxetine
Sertraline
Fluvoxamine
SNAs
Mianserin
Mirtazapine
Venlafaxine
Other Antidepressants
All Antidepressants
No Antidepressant Use
Figure 1. Relative risk and 95% confidence interval of suicides obtained byusing medication as a time-dependent variable. The relative risks wereadjusted with the propensity score method, and by including sex, age,geographical location (as strata), number of suicide attempts before theindex hospitalization, number of suicide attempts during follow-up, use ofmultiple antidepressant medications, and number of purchasedantidepressant prescriptions during the previous year in the model.SNA indicates serotonergic-noradrenergic antidepressant; SSRI, selectiveserotonin reuptake inhibitor; and TCA, tricyclic antidepressant. Citalopramwas given as citalopram hydrobromide; doxepin, as doxepin hydrochloride;fluvoxamine, as fluvoxamine maleate; mianserin, as mianserin hydrochloride;paroxetine, as paroxetine hydrochloride; and venlafaxine, as venlafaxinehydrochloride.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 63, DEC 2006 WWW.ARCHGENPSYCHIATRY.COM1361
©2006 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 11/27/2014
Suicide
TentativedeSuicide
Finland – 1997-2003 All hospitalized patients because of Suicide Attempt N = 15390 F/U = 3.4 years 602 suicide, 1583 deaths 7466 SA leading to hospital
Antidepressants andtherisk ofsuicide,SA,andoverall Mortality inanationwide cohort
Adulte :Augmentationdunombre deTSpaspasde
Suicide,voire effectprotecteur /suicide

LaquestiondurisqueSuicidaire
TSetIS=0.009 (CI0.005 -0.028)Excèsderisqueparrapportauplaceboestde9sujetsur1000,maisattentionçapeutallerde5 à28
2015

Cipriani,Lancet2016
Ici lavenlafaxineest malplacéemais lesautres sont nontestables.
Leschiffres vs placebo
LaquestiondurisqueSuicidaire

Pasd’augmentationdurisquedesautresIRS
comparésàlafluoxetineN=
Cooperetal,Pediatrics 2014
LaquestiondurisqueSuicidaire

36
LaquestiondurisqueSuicidaire
Letaux desuicidediminue en fonction
dutaux deprescriptiond’AD
(Adulte AdoEnfant)

Métanalyse sur 35 RCT
Variable d’efficacité :
réponse à 8 s
Mieux sur les plus sevère
Kirsh et al.,Plos One 2008; 5(2):260-8
RAPPEL CHEZ L’ADULTERappelchezl’adulte

Stimulants
• L’attention est le facteur pronostic +++• Sont associés : dépression (50%), anxiété (35%) et pauvre
estime de soi (tous ?)• Traitements combinés TJRS
• Amphétamine efficace dans le THADA connu depuis 1937 (Bradley)
38

ØRitaline
ØRitaline LP
ØConcerta
ØQuasym
39
Methylphénidate
Effetmaxen2h,puis/2en2h
Effetmaxen1h,durée8h(2pics)
Ascendant,12hd’action.Quasi100MPHLP
Durée8h70%LP

MultimodalTreatmentStudyA14-monthrandomizedclinicaltrialoftreatmentstrategiesforattention-deficit/hyperactivitydisorder.TheMTACooperativeGroup.MultimodalTreatmentStudyofChildrenwithADHD.ArchGenPsychiatry.1999Dec;56(12):1073-86
0
10
20
30
40
50
60
70
Témoins TCCseule Traitementseul Combiné
2534
5668
%derépondeur
Dosesmoins importantes dans legroupe combiné -20%EffectSizeest de0.9à 0.95(immédiat etProlongé respectivement)

Contreindications:• Schizophrénies• Arythmiescardiaques,l’insuffisancecoronaire,l’hypertensionartérielle,l’hyperthyroïdieetleglaucome.
Surveillanceparticulière• Tics,lestroublesenvahissantsdudéveloppement,lesabusdesubstances,lestroublesdel’humeur,leretardmentalsévère.
• L’épilepsiebienstabiliséen’estpasaggravéesoustraitementpsychostimulant.
Effetsindésirableslesplusfréquents• Insomnie,lescéphalées,lesdouleursabdominales,lanervositéetladiminutiondel’appétit.Ilssontgénéralementtransitoires.
Lestroublesdel’endormissementpeuventêtreliésàl’actionduproduitluimêmeouêtreenrapportaveclaréapparitionvoirel’exacerbationdessymptômesduTDAHenfindejournée.
Leretentissementsurlacroissanceestpossiblemaissonimpactsurlataillefinaleestincertain.à3ansdel’étudeenmoyenne,2cmdemoinsquelesautresavecuneffetmaximumaucoursdelapremièreannéedetraitement,etsansimpactsignificatifaucoursdelatroisièmeannée 41

Contre indications:
• Schizophrénies
• Arythmies cardiaques, l’insuffisance coronaire, l’hypertension artérielle, l’hyperthyroïdie et le glaucome.
Surveillance particulière
• Tics, les troubles envahissants du développement, les abus de substances, les troubles de l’humeur, le retard mental sévère.
• L’épilepsie bien stabilisée n’est pas aggravée sous traitement psychostimulant.
Effets indésirables les plus fréquents
• Insomnie, les céphalées, les douleurs abdominales, la nervosité et la diminution de l’appétit. Ils sont généralement transitoires.
Les troubles de l’endormissement peuvent être liés à l’action du produit lui même ou être en rapport avec la réapparition voire l’exacerbation des symptômes du TDAH en fin de journée.
Le retentissement sur la croissance est possible mais son impact sur la taille finale est incertain. à 3 ans de l’étude en moyenne, 2 cm de moins que les autres avec un effet maximum au cours de la première année de traitement, et sans impact significatif au cours de la troisième année
42
Surveillance
ECG Taille
AppétitTics
CéphaléesTremblements

O.5 à 1.5 mg /kg par jour en paliers progressifs
Pour 28 jours (dates strictes)
Prescritions hospitalieresannuelles
Ordonnance sécurisée
43
Pour28jours
PharmacieduCentredesCongrèsdeLyon
ORDONNANCEHOSPITALIEREANNUELLEdu29novemebre 2017
Dixmilligrammestouslesjourssaufledimanche
ENTOUTELETTRE
MathéoTRUCHOUETTE
9ans,34kg

Quelle place pour les thymorégulateurs ?
AcideValproïque
Tolérance
• RisqueTératogène
• Poids• Hépatique
Indication
• Pasd’AMMpourTB(F&USA)
• PossibleefficacitédansTBetImpulsivité

Quelle place pour les thymorégulateurs ?
LITHIUM
Tolérance
• Fonctionrénale,
• Ionogramme,TSH,glycémieàjeun,NFSetECG
• testdegrossesse
Indication
• 16ansTB(12auxUSA)
• PossibleefficacitéImpulsivité

Kovess,Choppin etal.2015
Surunéchantillon randomisée de1%desdonnées CPAMNationales en2010
46
Quelle est la place actuelle des préscriptions ?

Quelle est la place actuelle des prescriptions ? ANXIOLYTIQUES ET HYPNOTIQUES
Ataraxa70-80%saufpourAdolescentouc’est50-55%

Quelle est la place actuelle des préscriptions ? ANTIDEPRESSEURS

Quelle est la place actuelle des préscriptions ? STIMULANTS

50
Quelle est la place actuelle des préscriptions ?
Acquaviva,Legleye etal.2009
ConsommationPsychotropes(donnéesCPAMRegion FrancheComté2009)

Quelle est la place actuelle des préscriptions ?
10XplusdefamillealaCMUdontlesenfantssontsousAP

Quelle est la place actuelle des préscriptions ?
1/3desprescriptionssontENCOREdesAP1ere Génération


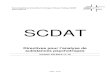
Figure 2. Forest plot of effect size (Hedges’s g) values for FDA-registered premarketing trials of second-generation antipsychotics.The black horizontal bars highlight the four unpublished trials, three of which demonstrated no statistically significant advantage for the drug overplacebo. The fourth unpublished trial showed that the drug was superior to placebo but statistically inferior to the active comparator haloperidol.Below the first dotted horizontal line, subtotal effect size and confidence interval values are shown for the subset of published trials and for thesubset of unpublished trials. The difference in effect size between the published and unpublished trials was statistically significant (see text). Belowthe second dotted horizontal line, the FDA-based effect size is shown for all trials combined (0.44). The effect sizes shown for iloperidone trials 3000,3004, and 3005 are based on the full sample of patients recruited, i.e., those with either schizophrenia or schizoaffective disorder, as opposed to thesubset of patients with schizophrenia only (see text for details).doi:10.1371/journal.pmed.1001189.g002
Publication Bias in Antipsychotic Trials
PLoS Medicine | www.plosmedicine.org 9 March 2012 | Volume 9 | Issue 3 | e1001189
TurnerPlos Medicine 2012
L’Effect Sizedesétudespubliéesestsignificativementinférieuràceluidesétudesnon
publiées.
Pas de méfiance mais une certaineprudence et un esprit critique sontnécessaire…

Figure 3. Forest plot of mean weighted effect size (Hedges’s g) values by drug and data source. The figure is sorted according to theeffect size point estimates derived from the FDA data; these are shown with gray-filled squares. The point estimates derived from the correspondingjournal articles are shown with open circles. Horizontal lines indicate 95% confidence intervals around the effect size point estimates. The right-handcolumn shows the percent differences between the FDA-based and the journal-based effect size point estimates. (These percent differences arebased on estimates accurate to three decimal places, while the estimates shown are rounded to two decimal places.) The differences ranged from24% to +20%, depending on the drug. For the entire drug class (labeled ‘‘overall antipsychotics’’), publication bias increased apparent effect size by8%. To provide context, previously published data on antidepressants [8] are shown at the bottom in gray. Note that the 8% increase with
Publication Bias in Antipsychotic Trials
PLoS Medicine | www.plosmedicine.org 10 March 2012 | Volume 9 | Issue 3 | e1001189
C’estplusmarquépourlesADquelesAP
Entoutétatdecausel’accèsouvertauxdonnéesdes
laboratoiresestindispensable
++++
TurnerPlos Medicine 2012
Pas de méfiance mais une certaineprudence et un esprit critique sontnécessaire…

Vouspouvezmecontacter:[email protected] mesuivresurtwitter@BonnotOlivier
Ettrouvercetteprésentationsurnotresite:www.u2peanantes.org
Mercidevotre attention…