Embed Size (px)
Citation preview

1November 4, 2014
Substance Use Disorders Consultation Service (SUDS): Integrating Addiction Services in an Acute Medical Setting
Anika Alvanzo, MD, MS
The Maryland Addictions Directors Council (MADC)
2014 Mid-Atlantic Behavioral Health Conference

2
Rationale for SUD Consultation Specialty Services
• Hospitalization may be “teachable moment” • Brief interventions demonstrate reduction in
alcohol consumption and death rates• Provider factors
– under diagnose – under treat– lack confidence in treating
McQueen, et al., 2011Murphy, et al., 2009Moore, et al., 1989

3
Historical Perspective
Intervention Services: 1970’s – ~2000
First Step Day Hospital: 1997 – 2010
SUDS: 2010 – present

4
Mission
The Mission of the Johns Hopkins Hospital Substance Use Disorders Consultation Service (SUDS) is to improve the health and quality of life of patients with substance addiction by providing non-judgmental, comprehensive, and patient-centered care and education. The SUDS performs brief behavioral interventions and counseling to patients, facilitates linkage to hospital and community-based alcohol and drug treatment programs, provides guidance on the clinical management of substance withdrawal syndromes, and educates patients, families, healthcare professionals and the community to prevent, identify, and treat persons living with addiction.

5
SUDS Team

6
Who We Are
• Medical Director– Anika Alvanzo, MD, MS
• Nurse– Patricia Burgee, RN, MSN, MBA
• Senior Addictions Therapist– Diane Moses, MSW, M.Ed, LCAD-C
• Interventionist– vacant

7
What We Do
• Services– Brief Interventions
• Motivational Interviewing
– Linkage to Treatment Programs– Medical Management of Withdrawal – Pain Management in Patients with Opioid
Use Disorders– Buprenorphine Bridging– Patient and Family Education– Healthcare Professional Education

8
Accomplishments
• Electronic Documentation– Qualified Service Organization Agreement (QSOA)
• Relationship Building– Program Visits
• Clinical Database• Improved Clinical Care
– Opioid and alcohol withdrawal protocols
• Customer Survey– 14-item survey using a 5-pt Likert scale (3.1 – 4.8)

9
Challenges
• Staffing– Referrals ↑ ~ 30%– 23% not seen (January – March 2014)– Vacation Coverage– No Medical Management Tues/Friday

10
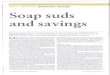
Referral Volume: FY11 – FY14
July
Augus
t
Septe
mbe
r
Octob
er
Novem
ber
Decem
ber
Janu
ary
Febru
ary
Mar
chApr
ilM
ayJu
ne0
20
40
60
80
100
120
140
160
180
FY 2011 (893)
FY 2012 (1430)
FY2013 (1457)
FY2014 (1876)
↑ 29% from last year

11
Challenges
• Clinical Database– Difficult to bring current and maintain
• Manpower issue– Medical tutorial and undergraduate students
• Demonstrating our value– Not a revenue generating service– Must be able to demonstrate cost savings
• Readmission, ED visits, LOS, expenditures• Treatment entry & engagement

12
Pearls…
• Start building relationships now• Work out policies on information
exchange• Standardize procedures and documents• Clinical database
– Integration with Electronic Medical Record• Determine outcomes and plan for
measurement in advance