Embed Size (px)
Citation preview
10/6/2015
1
Management of Cholesterol
M. Dominique Ashen PhD, CRNP
The Johns Hopkins Ciccarone Center for the Prevention of
Heart Disease
NPAM October 2015
Behavioral Objectives
1. Review 2013 ACC/AHA Guideline on Treatment of Blood Cholesterol, learn how to put it into practice and understand the limitations.
2. Discuss the use of non-traditional risk assessment tools, non-statin therapy, and new drug therapies.
New Guidelines: Atherosclerotic
Cardiovascular Disease (ASCVD)
…..Guidelines should inform clinical judgment, but not replace it…..
Neil Stone, MD, Chair, 2013 ACC/AHA Guidelines on Management of Blood Cholesterol to Reduce Cardiovascular Risk
Lifestyle management remains the cornerstone for reducing CVD risk including achieving and maintaining optimal lipid levels
……even modest weight loss (3-5% of body weight) can result in clinically meaningful benefits for triglycerides, blood glucose, glycated hemoglobin, and development of diabetes (type 2)….
10/6/2015
2
4 Statin Benefit Groups: “reduce risk in those most likely to benefit”
1. With clinical ASCVD without NYHA class II-IV heart failure or hemodialysis.
2. With primary elevations of LDL-C ≥190.
3. 40-75 yo with DM, and LDL-C 70-189 without clinical ASCVD.
4. Without clinical ASCVD or DM, who are 40-75 yo with LDL-C 70-189 and have an estimated 10-year ASCVD risk of >7.5%
When 10-year risk <7.5% or decision is unclear:
• Other factors to enhance treatment making decisions include: – Family history of premature ASCVD
– LDL-C >160
– High-sensitivity C-reactive protein ≥ 2
– CAC score ≥300 or ≥75th % for age, sex, ethnicity
– Ankle-brachial index <0.9
– Elevated lifetime risk of ASCVD
Lifestyle Modifications“both prior to and with drug therapies”
• Regular Exercise:
– regular, aerobic, 3-4 sessions per week, 40 min per session, moderate- to vigorous
• Heart Healthy Diet: (DASH, USDA or AHA diets)
– 5-6% from saturated fat; reduce trans fat
– High in vegetables, fruits, whole grains, low-fat dairy, fish, legumes, poultry, vegetable oils, nuts; limited sugar-sweetened beverages and red meat
• Avoidance of tobacco
• Healthy weight
Highlights: 2013 Cholesterol Guideline
1) New Pooled Cohort Equation for ASCVD risk assessment in primary prevention patients
2) Strong evidence for Statin Rx in 4 groups (reduction of morbidity and mortality)
3) No LDL-C or non-HDL-C treatment targets
4) Non-traditional risk assessment: optional use of coronary artery calcium scan (CAC ) or hsCRP in selected individuals in whom risk is uncertain
Pooled Cohort Equations for Risk Assessment
• Equations predict 10-yr risk of CVA/MI– Former guidelines focused only on MI; now
incudes CVA– Highlights the large burden of disability from
nonfatal events• Lowered treatment threshold to 7.5%
– Former threshold of 20% or >10% with 2 traditional RF
• Separate equations for non-white populations– Importance of race/ethnicity in risk of ASCVD
• www.clincalc.com
12

10/6/2015
3
Rosuvastatin 20 mg (N=8901) MIStroke
UnstableAngina
CVD DeathCABG/PTCA
JUPITERMulti-National Randomized Double Blind Placebo Controlled Trial of
Rosuvastatin in the Prevention of Cardiovascular EventsAmong Individuals With Low LDL and Elevated hsCRP
4-week run-in
No Prior CVD or DM
Men >50, Women >60LDL <130 mg/dLhsCRP >2 mg/L Placebo (N=8901)
Baseline LDLC 104 mg/dLBaseline HDLC 49 mg/dLBaseline hsCRP 4.2 mg/L
Women 6,800Non-Caucasian 5,000 Ridker et al, NEJM 2008359:2195-07
Primary Prevention and the Use of Statins
Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER)
17,802 men (>50 yrs) and women (>60) with LDL-C <130 mg/dL and hs-CRP >2 mg/L randomized to rosuvastatin (20 mg) or placebo for up to 5 yrs*
Statin benefits those with mean age of 66 and elevated hsCRP
0 1 2 3 4
0.00
0.04
0.08
Follow-up (years)
RosuvastatinPlacebo
44% RRR
P<0.00001, NNT=25Cum
ulat
ive
inci
denc
e of
CV
deat
h, M
I, st
roke
, hos
pita
lizat
ion
for u
nsta
ble
angi
na, a
nd
arte
rial
rev
ascu
lari
zati
on
Ridker PM et al. NEJM 2008;359:2195-2207*The study was stopped prematurely after 1.9 years
HMG-CoA Reductase Inhibitor Evidence: Primary Prevention
LaRosa JC et al. NEJM 2005;352:1425-1435
CARE=Cholesterol and Recurrent Events Trial, HPS=Heart Protection Study, LIPID=Long-term Intervention with Pravastatin in Ischaemic Disease; 4S=Scandinavian Simvastatin Survival Study, TNT=Treating to New Targets
30
25
20
15
10
5
00 70 90 110 130 150 170 190 210
LDL-C (mg/dL)
TNT (atorvastatin 80 mg/d)TNT (atorvastatin 10 mg/d)
HPSCARE
LIPIDLIPID
CAREHPSE
vent
(%
) 4S
4SStatinPlacebo
Relationship between LDL-C Levels and Event Rates in Secondary Prevention Statin Trials of Patients with Stable CHD
HMG-CoA Reductase Inhibitor: Secondary Prevention
LDL-C=Low density lipoprotein cholesterol
No Cholesterol Treatment Target Goals
• Appropriate intensity statin Rx recommended to reduce ASCVD risk by lowering LDL-C and non-HDL-C– High intensity statin: daily dose lowers LDL by
> 50%
– Moderate intensity statin: daily dose lowers LDL-C by approx 30% to <50%
• “Treat to target” is no longer advocated
• More trials needed to prove this approach
Law MR et al. BMJ 2003;326:1423-1427
78 (42)69 (37)60 (32)51 (27)Simvastatin
108 (58)99 (53)90 (48)80 (43)Rosuvastatin§
62 (33)53 (29)45 (24)37 (20)Pravastatin
83 (45)68 (37)54 (29)39 (21)Lovastatin‡
61 (33)50 (27)39 (21)29 (15)Fluvastatin
102 (55)91 (49)80 (43)69 (37)Atorvastatin
80 mg/d40 mg/d20 mg/d10 mg/dStatin
Data presented as absolute reductions in LDL-C* (mg/dL) and percent reductions in LDL-C (in parentheses)*Standardized to LDL-C 186 mg/dL (mean concentration in trials) before Rx.† Independent of pre-Rx LDL-C‡Maximum dose of 80 mg/d administered as two 40-mg tablets§Not FDA approved at 80 mg/d
A Meta-analysis of 164 Trials*†
HMG-CoA Reductase Inhibitor: Reduction in LDL-C
FDA=Food and Drug Administration, LDL-C=Low density lipoprotein cholesterol, Rx=Treatment
Non-Traditional Risk Assessment
• 2013 guidelines emphasize the importance of chronologic age
• People age differently health age (“vascular age”) may not always correlate with chronologic age
• Assessing a person’s “vascular age” (using a CAC) may allow for a more accurate CVD risk assessment and appropriate management decisions especially in presence of normal lipids
10/6/2015
4
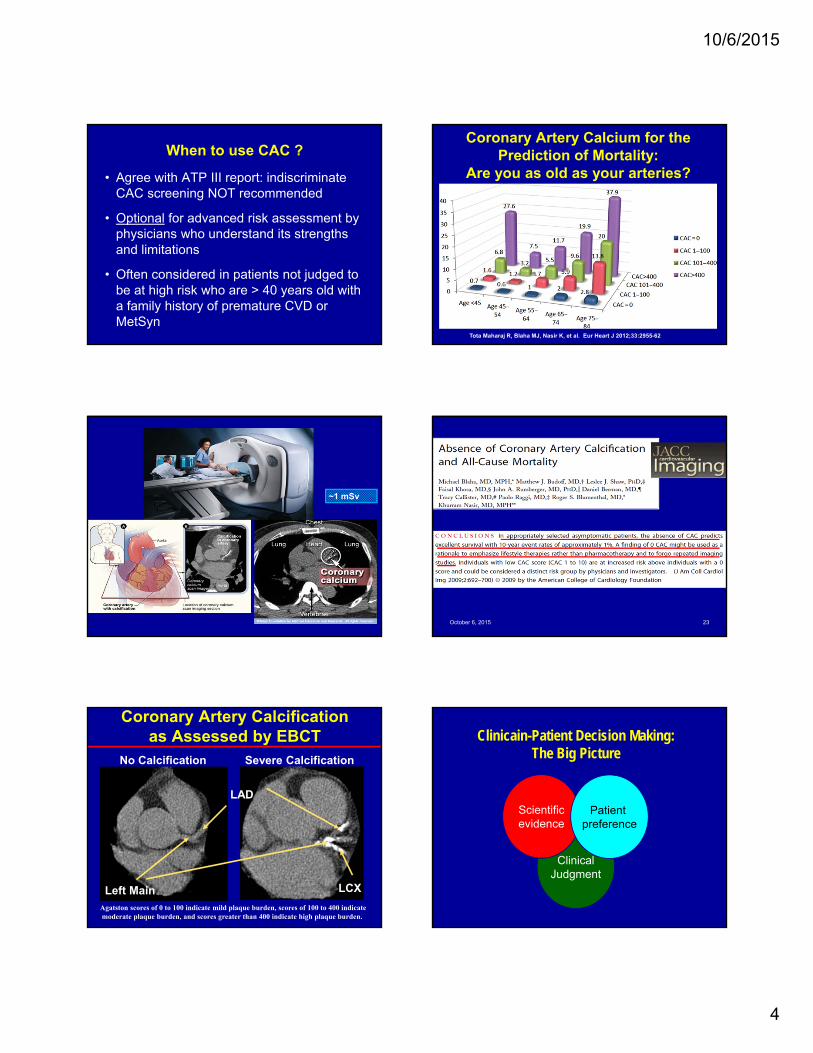
When to use CAC ?
• Agree with ATP III report: indiscriminate CAC screening NOT recommended
• Optional for advanced risk assessment by physicians who understand its strengths and limitations
• Often considered in patients not judged to be at high risk who are > 40 years old with a family history of premature CVD or MetSyn
~1 mSv
No Calcification Severe Calcification
Left Main
LAD
LCX
Coronary Artery Calcification as Assessed by EBCT
Agatston scores of 0 to 100 indicate mild plaque burden, scores of 100 to 400 indicatemoderate plaque burden, and scores greater than 400 indicate high plaque burden.
Coronary Artery Calcium for the Prediction of Mortality:
Are you as old as your arteries?
Tota Maharaj R, Blaha MJ, Nasir K, et al. Eur Heart J 2012;33:2955-62
October 6, 2015 23
ClinicalJudgment
Scientificevidence
Patient preference
Clinicain-Patient Decision Making: The Big Picture
10/6/2015
5
Concerns:
• Even greater dependence on chronologic age
• Death of the “Intermediate Risk” group
• Risk overestimation
Improvements:
• Provide guidance on evaluation of cholesterol
• More formally acknowledge “lower is better”
• Allow for optional non-HDL-C goals
• Align with international guidelines to try to achieve consensus
Guidelines: Concerns and Improvements
Application with the use of Case Studies
Case Study: CS 63 yo caucasian female
• Personal History: HTN and dyslipidemia
• Current Meds: Amlodipine 2.5 mg qd
• Lipids: TC 240, TG 54, HDL 68, LDL 156
• Height/Weight/BMI: 5’ 1.5”;120 lbs; 22
• BP: 128/74
Case Study (cont): CS 63 yo female• Lifestyle:
– Diet: tendency for high saturated fat foods (especially cheese); 1-2 glasses of wine qhs
– Exercise: Regular for many years; 5 days per week walking/biking outdoors
– Smoking: Former; 9 years, quit 1981
• Family history: – Brother (alive)dyslipidemia; mother died at age
90; father died at age 73 of pancreatic cancer
ASCVD Risk Prediction:
• 10-year ASCVD risk (%) = 6.1%
• 10-year ASCVD risk (%) for someone the same age with optimal risk factors levels = 3.2%
10/6/2015
6
Does she belong to one of the Statin Benefit Groups?
• With clinical ASCVD without NYHA class II-IV heart failure or hemodialysis. NO
• With primary elevations of LDL-C ≥190. NO
• 40-75 yo with DM, and LDL-C 70-189 without clinical ASCVD. NO
• Without clinical ASCVD or DM, who are 40-75 yo with LDL-C 70-189 and have an estimated 10-year ASCVD risk of >7.5% NO
What lifestyle modifications could be made?
• Regular Exercise:
– regular, aerobic, 3-4 sessions per week, 40 min per session, moderate to vigorous
• Heart Healthy Diet: (DASH, USDA or AHA diets)
– 5-6% of calories from saturated fat; reduction in trans fat reduce saturated fat consumption in her diet (cheese)
– High in vegetables, fruits, whole grains, low-fat dairy, fish, legumes, poultry, vegetable oils, nuts; limited sugar-sweetened beverages and red meat
• Avoidance of tobacco
• Healthy weight
Her 10-year ASCVD risk is less than 7.5%. What can help make the decision?
– Family history of premature ASCVD NO
– LDL-C >160 NO
– High-sensitivity C-reactive protein ≥ 2 Not evaluated
– CAC score ≥300 or ≥75th % for age, sex, ethnicity Not evaluated
– Ankle-brachial index <0.9 Did not discuss
– Elevated lifetime risk of ASCVD Cannot calculate >59 yo
Process of Risk Reduction for Patient:• Statin was suggested given high LDL (156)
• Pt very resistant to use of statin; requested initial trial of lifestyle. Whether she uses a statin or not, she needs to improve her dietary habits (lower saturated fat).
• 3 Month follow-up: With reduction in saturated fats in her diet she reduced LDL to 142
Process of Risk Reduction cont.:
• Discussed CAC scan pros and cons• 1 mSv radiation exposure (3 mSv/yr from
naturally occurring radioactive materials, cosmic radiation)
• Evaluates calcified plaque, not soft plaque
• Cost not covered by insurance
• Identifies subclinical atherosclerosis; optimizies risk stratification; can “de-risk:
• Result of CAC: Agatston score 10 (“mild”); 85th percentile for age, gender, ethnicity (“above average”)
Discussion Points:• Use of risk assessment tool in women
– Likely to be below 7.5%; use scores 5-7.5% for discussion of CVD prevention and tools for treatment making decisions
• What drives risk with this tool
– Age, high SBP (and treatment), cholesterol
• Role of non-traditional tools to detect subclinical disease
• Risk discussion with the patient

10/6/2015
7
Case Study #2• MA 66 yo male• PMH: HTN, • Family History: No CVD history in first degree
relatives• Lifestyle: Denies cigarette smoking, exercises
regularly, follows healthy dietary habits• Medications: Lisinopril 40 mg qd• Lab Results: Total cholesterol 185 mg/dL, LDL-C
122 mg/dL, HDL-C 42 mg/dL, triglycerides 102 mg/dL, glucose 96 mg/dL liver and kidney function wnl
• PE: BP 132/78, BMI 24, waist circumference 38”
ASCVD Risk Prediction:
• 10-year ASCVD risk (%) = 17.4%
• 10-year ASCVD risk (%) for someone the same age with optimal risk factors levels = 9.6%
Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER)
17,802 men (>50 yrs) and women (>60) with LDL-C <130 mg/dL and hs-CRP >2 mg/L randomized to rosuvastatin (20 mg) or placebo for up to 5 yrs*
Statin benefits those with mean age of 66 and elevated hsCRP
0 1 2 3 4
0.00
0.04
0.08
Follow-up (years)
RosuvastatinPlacebo
44% RRR
P<0.00001, NNT=25Cum
ulat
ive
inci
denc
e of
CV
deat
h, M
I, st
roke
, hos
pita
lizat
ion
for u
nsta
ble
angi
na, a
nd
arte
rial
rev
ascu
lari
zati
on
Ridker PM et al. NEJM 2008;359:2195-2207*The study was stopped prematurely after 1.9 years
HMG-CoA Reductase Inhibitor Evidence:Primary Prevention
Law MR et al. BMJ 2003;326:1423-1427
78 (42)69 (37)60 (32)51 (27)Simvastatin
108 (58)99 (53)90 (48)80 (43)Rosuvastatin§
62 (33)53 (29)45 (24)37 (20)Pravastatin
83 (45)68 (37)54 (29)39 (21)Lovastatin‡
61 (33)50 (27)39 (21)29 (15)Fluvastatin
102 (55)91 (49)80 (43)69 (37)Atorvastatin
80 mg/d40 mg/d20 mg/d10 mg/dStatin
Data presented as absolute reductions in LDL-C* (mg/dL) and percent reductions in LDL-C (in parentheses)*Standardized to LDL-C 186 mg/dL (mean concentration in trials) before Rx.† Independent of pre-Rx LDL-C‡Maximum dose of 80 mg/d administered as two 40-mg tablets§Not FDA approved at 80 mg/d
A Meta-analysis of 164 Trials*†
HMG-CoA Reductase Inhibitor: Reduction in LDL-C
FDA=Food and Drug Administration, LDL-C=Low density lipoprotein cholesterol, Rx=Treatment
Elevated LFTs:
•0.5-2.0% incidence of elevated hepatic transaminases
• Dose-dependent phenomenon
• Usually reversible and rarely leads to progressive hepatic failure
Hepatocyte
Skeletal myocyte
Myalgias:
•5% incidence of myalgias (rare significant rise in CPK)
• 0.1% incidence of myositis (with CPK up to 10 times the upper limit of normal)
• 0.0001% incidence of fatal rhabdomyolysis. Pasternak RC et al. Circulation 2002;106:1024-1028
HMG-CoA Reductase Inhibitor: Adverse Effects
Strategies for Statin Intolerant Patients:
• Switching to a different statin
• Reducing the frequency of statin administration
• Substituting statins with other LDL-C-lowering agents (e.g. ezetimibe, colesevelam or nicotinic acid)
• Combining low-dose statin treatment with other lipid-modifying drugs.
10/6/2015
8
Case Study #3• KL 57yo male• PMH: HIV, Above average coronary calcification for
his age.• Family History: Adopted• Lifestyle: Former cigarette smoker; does not
exercise; is very careful about his diet (low saturated fat); drinks 2-3 alcoholic beverages 3-4x per week
• Medications: HIV meds, Lipitor 40 mg• Lab Results: TC168, TG322, HDL24, LDL80,
glucose 105• PE: BP 136/68, BMI 24, waist circumference 36”
AIM HIGH Results: Statin + Niacin
• 3414 subjects; > 45 yo; in patients with established vascular disease and atherogenic dyslipidemia; 34% with T2DM and 71% with MetS; 94% prior statins
• Randomized to Simvastatin to reduce LDL-C < 80 mg/dL; then Niacin ER 2 gm added in 1718 or PBO in 1696
• Baseline lipids: LDL-C 71TG 161HDL 35
• Primary endpoint composite: No difference in primary end points (CHD Death, MI, or hi-risk ACS hospitalization after 32 months).
• Increased stroke (1.6% vs. 6.7%); trial stopped early.
Lifestyle Management of High Triglycerides
1. Regular aerobic exercise
2. Decrease consumption of simple sugars and white carbs (bread, rice, pasta and potatos)
3. Moderate alcohol consumption
4. Weight reduction
5. Fish oil
VERY EFFECTIVE!!
Case Study #4• TH 48 yo male• PMH: dyslipidemia, family hx of high cholesterol (mother
and all siblings)• Medications: None; encouraged by his PCP to start a
statin; he does not want to• Lifestyle: Denies cigarette smoking, basketball 4x per
week and treadmill on weekends, low saturated fat diet, healthy choices
• Laboratory results: total cholesterol 315 mg/dL, triglycerides 135 mg/dL, HDL-C 42 mg/dL, LDL-C 246 mg/dL, glucose 92 mg/dL, liver and kidney function wnl
• PE: 112/74 mmHg HR: 60 bpm BMI: 22
IMProved Reduction of Outcomes: Vytorin Efficacy International Trial
IMPROVE-IT
A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Simvastatin Monotherapy in
High-Risk Subjects Presenting With Acute Coronary Syndrome
Ezetimibe: Background
– Ezetimibe inhibits Niemann-Pick C1-like 1 (NPC1L1) protein
• located primarily on the epithelial brush border of the GI tract
• resulting in reduced cholesterol absorption
– Two recent human genetic analyses have correlated polymorphisms in NPC1L1 with lower levels of LDL-C and lower risk of CV events*
*MI Genetics Consortium Investigators NEJM 2014; online Nov 12; Ference BA et al AHA 2014
10/6/2015
9
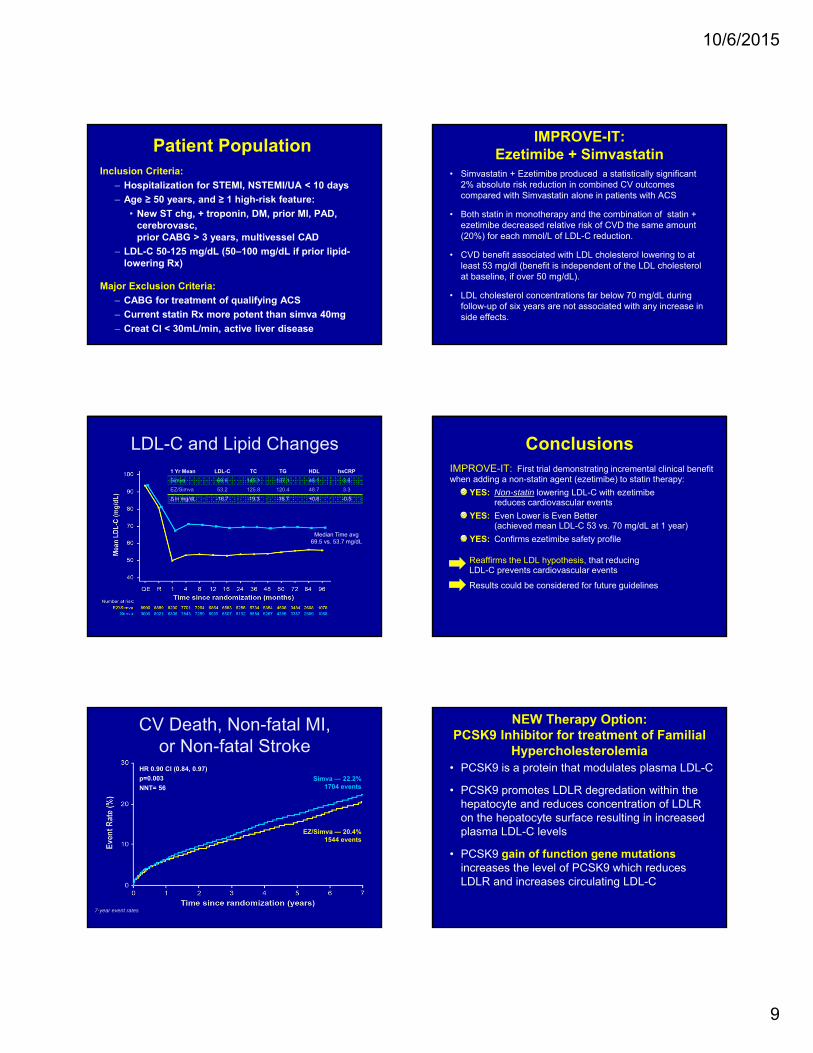
Patient PopulationInclusion Criteria:
– Hospitalization for STEMI, NSTEMI/UA < 10 days
– Age ≥ 50 years, and ≥ 1 high-risk feature:
• New ST chg, + troponin, DM, prior MI, PAD, cerebrovasc, prior CABG > 3 years, multivessel CAD
– LDL-C 50-125 mg/dL (50–100 mg/dL if prior lipid-lowering Rx)
Major Exclusion Criteria:
– CABG for treatment of qualifying ACS
– Current statin Rx more potent than simva 40mg
– Creat Cl < 30mL/min, active liver disease
LDL-C and Lipid Changes1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
Δ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5
Median Time avg69.5 vs. 53.7 mg/dL
Simva — 22.2% 1704 events
EZ/Simva — 20.4% 1544 events
HR 0.90 CI (0.84, 0.97)
p=0.003
NNT= 56
CV Death, Non-fatal MI, or Non-fatal Stroke
7-year event rates
IMPROVE-IT: Ezetimibe + Simvastatin
• Simvastatin + Ezetimibe produced a statistically significant 2% absolute risk reduction in combined CV outcomes compared with Simvastatin alone in patients with ACS
• Both statin in monotherapy and the combination of statin + ezetimibe decreased relative risk of CVD the same amount (20%) for each mmol/L of LDL-C reduction.
• CVD benefit associated with LDL cholesterol lowering to at least 53 mg/dl (benefit is independent of the LDL cholesterol at baseline, if over 50 mg/dL).
• LDL cholesterol concentrations far below 70 mg/dL during follow-up of six years are not associated with any increase in side effects.
ConclusionsIMPROVE-IT: First trial demonstrating incremental clinical benefit when adding a non-statin agent (ezetimibe) to statin therapy:
YES: Non-statin lowering LDL-C with ezetimibereduces cardiovascular events
YES: Even Lower is Even Better(achieved mean LDL-C 53 vs. 70 mg/dL at 1 year)
YES: Confirms ezetimibe safety profile
Reaffirms the LDL hypothesis, that reducing LDL-C prevents cardiovascular events
Results could be considered for future guidelines
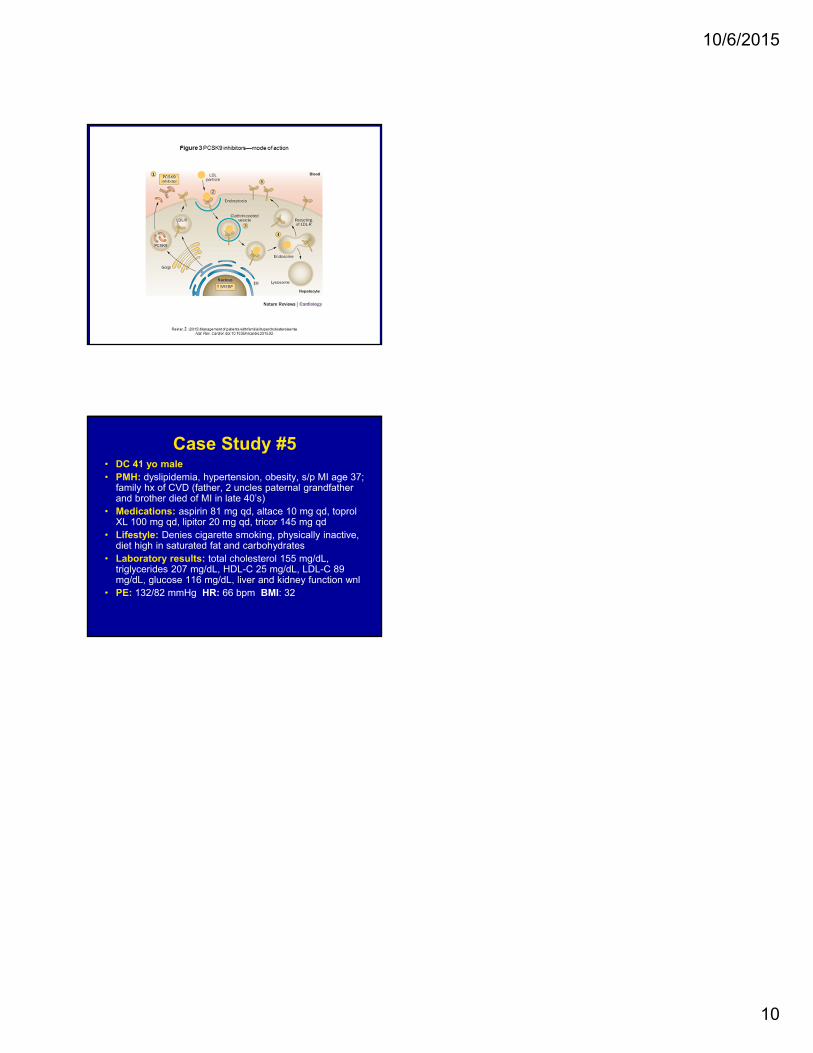
NEW Therapy Option:PCSK9 Inhibitor for treatment of Familial
Hypercholesterolemia• PCSK9 is a protein that modulates plasma LDL-C
• PCSK9 promotes LDLR degredation within the hepatocyte and reduces concentration of LDLR on the hepatocyte surface resulting in increased plasma LDL-C levels
• PCSK9 gain of function gene mutations increases the level of PCSK9 which reduces LDLR and increases circulating LDL-C
10/6/2015
10
Treatment of Familial Hypercholesterolemia: PCSK9 Inhibitor
Case Study #5• DC 41 yo male• PMH: dyslipidemia, hypertension, obesity, s/p MI age 37;
family hx of CVD (father, 2 uncles paternal grandfather and brother died of MI in late 40’s)
• Medications: aspirin 81 mg qd, altace 10 mg qd, toprol XL 100 mg qd, lipitor 20 mg qd, tricor 145 mg qd
• Lifestyle: Denies cigarette smoking, physically inactive, diet high in saturated fat and carbohydrates
• Laboratory results: total cholesterol 155 mg/dL, triglycerides 207 mg/dL, HDL-C 25 mg/dL, LDL-C 89 mg/dL, glucose 116 mg/dL, liver and kidney function wnl
• PE: 132/82 mmHg HR: 66 bpm BMI: 32