Embed Size (px)
Citation preview

NPLEX Combination ReviewDermatology
Paul S. Anderson, ND
Medical Board Review Services
Copyright MBRS
Skin Cancer
• Half of all new cancers are skin cancer• Over 1 million cases will be diagnosed this year• 50-80% of photo damage done prior to age 18• Australia-most skin ca in world• Arizona, most skin ca in US• Fair skinned people living in sunny climate

Cancerous / Pre-cancerous Lesions• Solar (Actinic) Keratosis
– Indurated sun exposed skin– Rarely pre-malignant
• Lentigo (“Spots”)– Maligna– Benina
• Basal Cell Carcinoma – Most common– Slow growing– Rare metastasis
• Squamous Cell Carcinoma– Faster growing– Metastatic– DDX: Trichoepithelioma

Actinic Keratosis- Precancers
• Rough, scaling red-brown macules/papule
• Sun exposed skin-face, forearm, hand
• Can progress in to SCC

SCC

Basal Cell Carcinoma
Most common type of cancerFair complexion with sun exposure/sunburnSlow growing Bleeding or scabbing sore that heals and recursNodular: often face; small translucent papule or nodule which appears “pearly” with rolled edges; may be pigmented with small blood vessels on surface or red; usually single lesion

BCC

Melanoma
• Risk-20 fold increase on past 70 years
• 1 out of 70 people • 51,400 cases per
year• 4% of all skin ca• 7,800 deaths per year
• Most common Cancer– women-age 25-29– 2nd to breast in 30-34
• 6th most common cancer in men

High Risk people- 6 key risk factors
• Family history of mm in 1st degree relative
• Fair skinned, red/blond hair, or blue eyes, do not tan well
• Marked freckling of upper back
• Actinic keratosis• Three or more
blistering sun burns prior to age 20
• Three or more yrs with outdoor summer jobs as a teen

4 types
• Superficial spreading– most common– has a radial phase
before invading dermis

Melanoma types
• Nodular– most aggressive– skips radial phase,
goes to vertical

Melanoma types
• Lentigo maligna– elderly– sun exposed areas,
face– occur in large
lentigos(age spots)– occur slowly over 20
years

Melanoma type
• Acral– most common in
darker skinned people– blacks, Asians,
Hispanics– occur on palms/soles.
Nail bed– aggressive and
overlooked

ABCD of moles
• Asymmetry- one half does not match other
• Border- irregular- edges are ragged, notched, blurred
• Color- not uniform or darkening
• Diameter- greater then 6 mm or pencil eraser

Nevi (Moles)
• Junctional-macular• Heredity/sun
exposure determine # of moles
• >50, increases risk for melanoma
• As moles age, raise up & loose color= normal change

Congenital Nevi
• Present at birth & grow
• May thicken & develop hairs
• Tend to be larger/darker
• 10cm have a 10% MM risk
• Excise at puberty

Rough scaly spots on sun-damaged skin are called solar keratoses. They are also known as actinic keratoses. They can give rise to a type of skin cancer called squamous cell carcinoma.

Nevi (Moles)
Moles are common usually harmless skin lesions. Correctly called melanocytic or pigmented nevi, moles may be flat or protruding.
They vary in color from pink flesh tones to dark brown or black. The number of moles a person has depends on genetic factors and on sun exposure.

Atypical Nevi (Moles)
Atypical nevi are moles that have unusual features such as an indistinct edge and/or larger size, often resembling a cancerous mole (melanoma), but are actually benign.

Cellulitis
• Infection of the dermis and subcutaneous tissue following trauma or skin lesions
• Red hot, tender area of skin
• Caused most often by group A beta-hemolytic streptococci or Staphylococcus aureus in adults
• DX: Clinical, culture
Erysipelas
• Superficial cellulitis involving lymphatics
• Usually caused by group A beta-hemolytic Streptococcus pyogenes (GAS)
• Painful, raised sharply demarcated “orange peel” lesion
• Usually fever, malaise, local lymphadenopathy with possible red streaking

Stasis DermatitisStasis Dermatitis
Chronic venous insufficiency (CVI) results from failure of return of venous blood and increased capillary pressure
The resultant changes include edema, hyperpigmentation, fibrosis of the skin and subcutaneous tissue of the leg, and ulceration

Arachnid
• Black widow– Neurotoxin- intense
pain in regional node, spreads outward
– starts 10 min after bite– original bite is painless
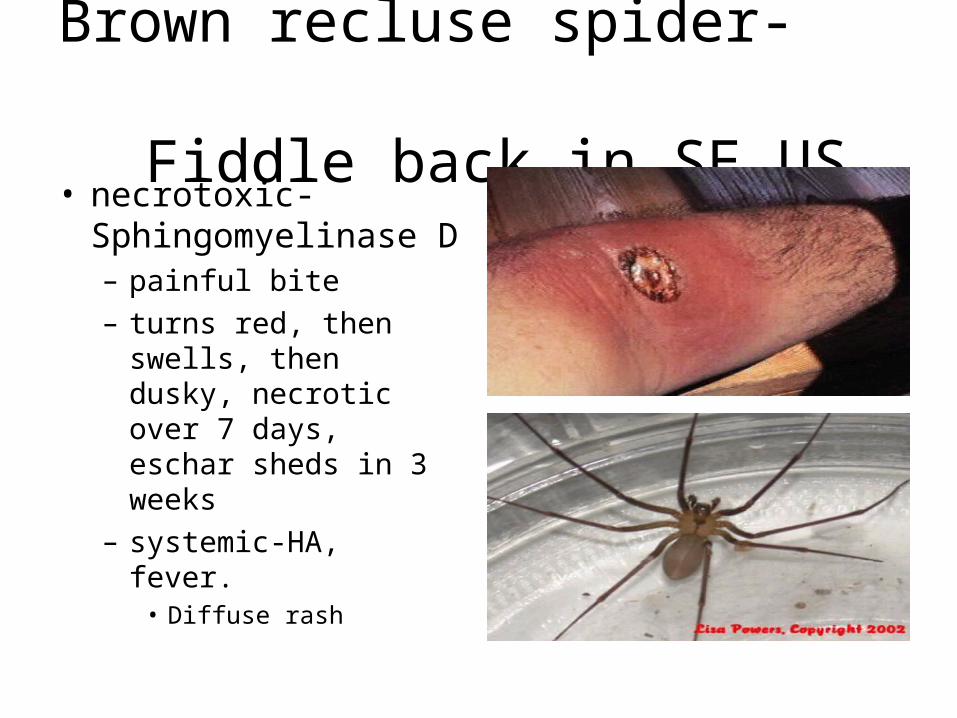
Brown recluse spider- Fiddle back,in SE US
• necrotoxic-Sphingomyelinase D– painful bite– turns red, then swells,
then dusky, necrotic over 7 days, eschar sheds in 3 weeks
– systemic-HA, fever.• Diffuse rash

Pemphigus vulgaris
Middle aged or elderly, rare, autoimmune
Intra-epidermal blisters (vesicles and bullae) that move into painful erosions; randomly scattered
Nikolsky’s Sign: with pressure blister spreads
Lab: microscopy, immunofluorescence (IF) shows IgG in skin and serum

Pemphigus vulgaris

Urticaria
• Location-anywhere• Shape-round, oval, polycyclic, changing• Color- red-white• Lesion type- edematous plaque• If linear- think dermatographism


Physical Urticaria
• Cholinergic– small papules– from overheating/
exercise, emotional stress
– start in few minutes and last 30 min

Physical Urticaria
• Dermatographism– most common– pressure induced– chronic– can test patient for by
rubbing
Causes
• Acute– infection
• viral• bacterial-sinusitis, tooth
abscess, UTI
– drugs• ASA• Antibiotics
• Chronic– R/O internal diseases
• Thyroid dis, Cancer, Lupus,
– Infections– Ingestants
• Food, additives, drugs, dyes
• Aeroallergens (dust, mold, pollen)

Urticaria

Erythema multiforme
Acute illness; hypersensitivity; drugs
Round lesions on forearms, hands, knees or feet
lesions appear like a target with fluid filled blister in center
Major: less common, involves the eyes, mouth or genitals (Stevens-Johnson Syndrome)
Minor: common, self-limiting
DX: Clinical or biopsy

Erythema multiforme
Target LesionTarget Lesion

Drug Eruptions
• Onset within one day to three weeks of drug therapy.– Depends upon prior sensitization in most
cases.
• Urticarial variety is the most common.– Eczema may be in the DDX but should itch
more severely than a drug rash.

Urticarial (hive) drug reaction• Drugs (e.g., penicillins) are a
common cause of urticaria, but urticaria can be precipitated by other internal and external factors
• Primary lesion is a wheal, a flesh-
colored to pink, well circumscribed plaque caused by dermal edema; itchy!
• Individual lesions last only a few hours, never more than 24 hours
• When caused by drugs, may be IgE mediated, triggering mast cell granule release; or drug may directly cause mast cell granule release

Morbilliform drug eruption (exanthematous drug eruption, maculopapular drug eruption):
• "morbilliform" refers to a resemblance to the rash of measles (morbilli is Latin for measles); measles is a rare disease now, but morbilliform eruptions are common
• a morbilliform eruption is symmetrically distributed on the trunk and proximal extremities, and consists of bright pink macules and slightly raised papules ("maculopapular")

Fixed drug eruption
• “Fixed" in that it occurs at same sites with each episode – OTC drugs containing phenolphthalein, pseudoephedrine, etc.
common culprits – tetracyclines, barbiturates, phenothiazines, sulfonamides – oval, itchy or burning dusky red plaque

Toxic Epidermal Necrolysis / Stevens-Johnson Syndrome
• Severe life threatening blistering disorder• Patients normally have fever, pruritis,
conjunctivitis…• May also appear as an erythema-multiforme
type rash• 30% Fatal• Almost always due to a drug reaction• Tx: Emergent referral
– Electrolyte replacement– Maybe high dose IV steroids (2 mg / kg)

SJS

SJS

SJS

SJS

NPLEX Combination ReviewDermatology - 2
Paul S. Anderson, ND
Medical Board Review Services
Copyright MBRS

Seborrheic Keratosis
• Greasy,scaly, or verrucous, flat papules to plaques
• Appear stuck on skin• Occur more in sun
exposed areas• More in aging adults• Can get inflamed &
simulate a skin ca.

Skin tags
• Tag like growths around neck, axilla, under breasts, in groin
• Color-skin toned, brown, or pink
• If removing an unusual or inflamed tag, send in to path
• Scissor removal
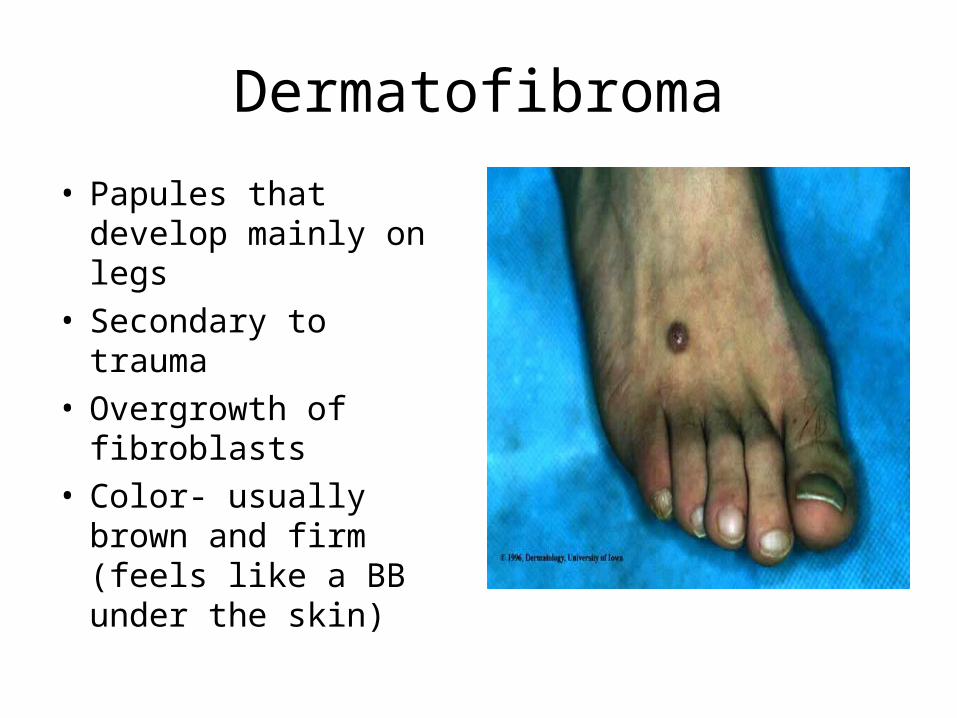
Dermatofibroma
• Papules that develop mainly on legs
• Secondary to trauma• Overgrowth of
fibroblasts• Color- usually brown
and firm (feels like a BB under the skin)

Epidermal inclusion cyst(sebaceous cyst)
• Movable skin colored papules to nodules
• Subcutaneous• Face, back, ears, groin• Sack of epidermis under
skin, filled w/keratin/sebum
• Smell• Can get inflamed, usually
not infected

Lipomas
• Subcutaneous movable nodule
• Fatty growth/lobules• Hereditary/ numerous• Arms, trunk• Usually asymptomatic or
painful• Sometimes can not differ
from an EIC until surgery• Can recur after removal

Pilar cysts (wen)
• On scalp, subcutaneous movable nodule
• Have firmer keratin then EIC/ no smell
• Usually, pop out during surgery

Discoid Lupus Erythematosus
Chronic recurrent autoimmune disorder primarily affecting the skin.Unknown etiology; IgG and IgM deposited in skinExposure to sunlight frequently precedes lesionsMore common in females (10x), onset usually in 30’s

Discoid Lupus Erythematosus
ClinicalLesions are rather distinctive, but sometimes resemble those of SLE
LabNo anemia, normal ESR, ANA absent or low, anti-DNA absent
Differential DxSLE, rosacea, seborrhea, photosensitivity dermatitis

Genital Warts (HPV)
• 80 types of HPV; 20 can infect genital area; usually HPV 6 and 11
• Soft, moist, skinned colored (or pink or red) pinhead papules to cauliflower-like masses
• HPV 16, 18, 31, 33 may lead to cervical dysplasia

Genital Warts (HPV)

Types of Hemangiomas
Capillary“Strawberry”Superficial angiomatous neviAffect the blood vessels in uppermost layers of the skin
CavernousSubcutaneous angiomatous neviMore deeply set in the dermis and subcutis

Hemangiomas in Adulthood
Cherry AngiomaOccur most often around the midtrunk
They increase in number from about the age of 40
Cause is unknown
They can be simply removed by diathermy or laser, but are usually left alone.

Cherry Hemangioma

Impetigo
Skin infection caused by bacteria (Streptococcus pyogenes and/or Staphylococcus aureus)
Pruritic pustules, vesicles, bullae with “honey-colored” crust
DX: Clinical, culture or Gram stain

Impetigo

Herpes Simplex
• One of the most common infections• Two main types:
– HSV Type 1: mainly facial infection; mainly infants and young children
– HSV Type 2: mainly genital infection; mainly after puberty, often sexual transmitted
• Latent state in the nerves; spread by direct contact with infected secretions

Herpes Simplex
• Prodromal tingling or itching; maybe fever• Oral (white patches on tongue, throat, palate
and inside cheeks): small fluid filled vesicles (blisters) on erythematous base; may be painful; usually burst and leave yellowish crust
• Genital: penile ulcerations on glans, foreskin or shaft; mucosa of vulva, vagina and cervix

Herpes Simplex

Herpes Zoster (Shingles)
Painful blistering rash caused by Chicken Pox (varicella) virus
Latent in nerves which supply sensation to the skin
Increased incidence with age Pain (maybe fever, HA); tenderness to
sensory nerve pathway

Herpes Zoster (Shingles)
Molluscum contagiosum
• Viral skin infection
• Small harmless skin growths
• Resemble pimples at first and later the spots enlarge
• Waxy pinkish look and small central pit
• Can spread person-to-person

Molluscum contagiousum

Venous UlcersVenous Ulcers

Granuloma annulare
Characterized by a ring of small, firm, flesh-colored or red papulesLateral or dorsal surfaces of hands and feetBegins with asymptomatic, flesh-colored papule that undergoes central involutionOver months size increases up to 5 cmSpontaneous involution or lasts for yearsHistology shows collagen degenerationTreatment:
Intralesional injections with triamcinolone


Infestations
• Scabies-mite– very pruritic, especially
night– red papules,
excoriations, burrows• Hands. Wrists,
elbows,axilla, umbilicus, groin/penis
– contagious– takes 6 weeks to show
after exposure
Elimite, neck down for 8 hours

Lice• Body Louse– Less common in US– poverty,war– live in clothes
• Pubic “crabs”– sexually transmitted– Pruritus
• Retreat in 1 week• Remove nits
– vinegar/H20 rinse– Lice/nit comb

Arthropod bite
• Flea bites– around ankles, go for
people once dog’s gone
– can be dormant for 1 yr
• Chiggers– bite in 3’s, like were
clothes bind (waist,socks.ankle)

Arthropod
• Mosquito bites– pink papule to nodule
to bulla
• Ant bites– papules to bulla– pustules in fire ants
• Sand flea– toes, buttocks (sitting
in sand)
• Pattern– red papule w/central
puncta, linear-grouped– vesicles– giant wheals(urticaria)– nodules

NPLEX Combination ReviewDermatology - 3
Paul S. Anderson, ND
Medical Board Review Services
Copyright MBRS

Nail Diseases
Acute ParonychiaPainful, bright red swelling of proximal and lateral nailfold
Chronic type associated with contact with water
Keep hands dry is best treatment-lotions and ointments should be avoided
Separation of nail plate (onycholysis) may predispose to Pseudomonas infection

Paronychia

Nail Diseases
Fungal
Tinea unguium
Trauma predisposes to infection
DDX: Psoriasis (pitting not found in tinea)
Treatment orally with fluconazole or itraconazole

Tinea Unguium

Contact DermatitisContact Dermatitis
Contact dermatitis is a reaction, which occurs when skin comes in contact with certain substances.
Irritant contact dermatitisOrganic solvents or soaps
Allergic contact dermatitisDelayed hypersensitivityHapten (low molecular weight substance)Cross-sensitization

DiagnosisHistory of onset; work-home exposure; skin care; medications; soaps; clothing (be persistent with questioning)
If problem does not clear:
According to the American Academy of Allergy, Asthma, and Immunology, "Patch testing is the gold standard for contact allergen identification”
Not to be used for irritant contact dermatitis
Contact DermatitisContact Dermatitis

Irritant Vs A llergic D erm atitis
B o rd e rs U su a lly N o n d is tin ct
N o n im m u no lo g icH ig h C on ce n tra tio n o f S u b s ta n ce
G ra du a l M od e o f O n se t
Irritant
M a y C o rre sp on d to C on tac ta n t
D e la ye d H yp e rsen s it iv ity R e a c tionU su a lly L ow S u b s ta n ce E xpo su re
U su a lly R a p id O n se t A fte r S e ns it ized
Allergic
C ontact D erm atitis

Contact dermatitis due to allergy to rubber antioxidant in brassiere

Contact Dermatitis

Atopic DermatitisAtopic Dermatitis
Major CriteriaPruritus Flexural lichenification (thickening of the skin) and linearity in adults Facial and extensor involvement in infants and young children Chronic or chronically relapsing dermatitis Personal or family history of atopy (asthma, allergic rhinoconjunctivitis, atopic dermatitis)
Labsserum IgE elevated above 200 IU/ml in 80-90%Eosinophilia



Psoriasis
About 2% of adults (Psoriasis vulgaris)
Triggers: rash starts after emotional stress, trauma to skin (Koebner’s phenomenon), strep throat
Red scaly-white papules and plaques; removal of scale results in blood drops (Auspitz phenomenon)

Psoriasis
• Plaque• Guttate-strep induced• Palmoplantar
pustulosis• Inverse

Psoriasis

Seborrheic dermatitis
Chronic superficial inflammatory process of hairy regions of the body
Pityriasis capitis (dandruff)
Cradle Cap (thick, yellow, crusty scalp lesions in infants)
Proliferation of Pityrosporum ovale (yeast)
Triggered by stress, fatigue, change of season or reduced general health

Seborrheic Dermatitis

Acne vulgaris
• Location-sebaceous skin– face, chest, back
• Lesion type– non-inflammatory
• comedone-open/closed• cyst
– inflammatory• papule(red), pustule,
nodule

AV

Treatment
• Correct abnormal keratinization (plugging)– Vit A cream
• Kill bacteria– topical ABX, oral ABX,
Benzoyl peroxide
• Decrease inflammation– Tetracycline family
• Minocycline
– Diet- decrease refined sugars/fried foods.
– Sunlight/blue light
• Correct hormone imbalance

Rosacea
• In adults• Two components
– redness/flushing/telangiectasia-burning
– papules/pustules– No comedones
• Location-mid face, around eyes

Etiology
• Unknown- some relation to acne
• Racial group – Northern Europeons– Celtic– Men worse than
women
• Triggers– Emotional stress-
people who blush– Hot/cold air (exercise)– Food
• cheese, wine, spicy food, coffee
• Very Chronic

Pityriasis albaPityriasis alba
Children and young adults
Round or oval; slightly elevated, fine scaling plaque that leave pale marks (hypopigmented) usually on face, neck and arms
DDX: vitiligo, tinea versicolor (How do you tell?)
Vitiligo and tinea versicolor appear white; borders are distinct in vitiligo; tinea versicolor is rare on the face and areas more numerous and often confluent; KOH to settle the debate
Vitiligo and tinea versicolor appear white; borders are distinct in vitiligo; tinea versicolor is rare on the face and areas more numerous and often confluent; KOH to settle the debate

Pityriasis alba

Pityriasis rosea
• Teenagers and young adults; benign• No known cause but linked to
mycoplasma, picornavirus and human herpesvirus 7
• “Harold Patch” (plaque) precedes eruption then followed by smaller plaques (0.5 to 2 cm in diameter)
• Follows long axes parallel lines of cleavage starting at spine (Christmas tree-like pattern)

Harold PatchSlightly erythematous,
scaly, with slightly raised bordersPityriasis rosea

Lichen simplex (neurodermatitis)
Common disorder, usually adults
Repeated rubbing or scratching resulting in itchy patch of skin
Sharply demarcated, red, scaly plaque with prominent skin lines

Lichen Simplex

Lichen planus
• Very pruritic rash on palms, wrists
• Polyangular, flat topped pink papules w/ wickham’s striae– criss/cross white lines

Verruca vulgaris (warts)
Epithelial tumors caused by at least 60 types of human papillomavirusFrequent in older children, uncommon in elderlyCommon Type: flesh-colored papules evolve to dome-shaped, gray-brown, hyperkeratotic growths with black dots on the service

Verruca vulgaris (Common)

Tinea
Tinea incognito when the clinical appearance has changed because of inappropriate treatment

Tinea versicolor
• Chronic yeast overgrowth in skin increased by heat
• Pityrosporium obiculare
• Not contagious• white, brown, pink
scaling oval patches on trunk

Candidiasis
Oral called thrush in infantsAdult: check for diabetes, depressed immunity, elderly and patients with cancerProlonged corticosteroids or broad spectrum antibioticsCandidiasis of large skin folds
Warm and moist areas (under breasts, groin and armpits, diapers)

Dyshidrotic EczemaDyshidrotic Eczema
Symmetric, vesicular hand and foot dermatitis
Preceded by moderate to severe itching
Palms may be red and sweating
Aggravated by contact with irritants such as water, detergents and solvents
High incidence of nickel allergy


Vitiligo
• Pigment cells are destroyed resulting in white patches
• Associated with increased risk of autoimmune disorders (thyroid, pernicious anemia, Addison’s, and alopecia areata)

Vitiligo