Embed Size (px)
Citation preview

Journal of Surgical Research 170, e217–e224 (2011)doi:10.1016/j.jss.2011.05.040
NSQIP Reveals Significant Incidence of Death Following Discharge1
Peter Yu, M.D.,2 David C. Chang, Ph.D., M.P.H., M.B.A., Hayley B. Osen, B.A., and Mark A. Talamini, M.D.
Department of Surgery, University of California San Diego, San Diego, California
Submitted for publication March 15, 2011
Background. The rates of post-discharge deaths af-ter surgical procedures are unknown and may repre-sent areas of quality improvement. The NSQIPdatabase captures 30-d outcomes not included withinnormal administrative databases, and can thus differ-entiate between in-hospital andpost-discharge deaths.Methods. Retrospective analysis of NSQIP from
2005 through 2007. Inclusion criteria were procedureswhose median length of stay was greater than 1 d (toexclude outpatient procedures), and whose overalldeath rate was greater than 2% (to include only proce-dures where mortality was a significant issue). Proce-dures where less than 25 deaths occurred wereexcluded (for sample size concerns).Results. There were 363,897 patients with 2236 dif-
ferent CPT codes captured in NSQIP. There were6395 deaths; among them, 1486 (23.2%) occurred afterdischarge. Thirty-eight CPT codes met the analysisthreshold. In two of the CPT codes, there were nopost-discharge deaths (repair of ruptured abdominalaortic aneurysm [AAA], repair of ruptured AAA involv-ing iliacs). In the other 36 CPT codes, the proportion ofdeaths occurring after discharge ranged from 6.3% (re-pair of thoracoabdominal aneurysm) to 50.0% (femoral-distal bypass with vein). The highest percentage ofpost-discharge mortality occurs on d 1 after discharge.Fifty percent of post-dischargemortality occurs by d 7;95% occurs by d 21.Conclusion. Approximately one-fourth of postoper-
ative deaths occur after hospital discharge. There issignificant variation across surgical procedures inthe likelihood of postoperative deaths occurring afterdischarge. These data indicate a need for closer andmore frequent monitoring of post-surgical patients.These data also call into question conclusions drawn
1 Presented at the American College of Surgeons 96th Annual Clin-ical Congress, October 3, 2010, Washington, DC.
2 To whom correspondence and reprint requests should be ad-dressed atDepartment of Surgery,University of CaliforniaSanDiego,San Diego, CA 92103-8402. E-mail: [email protected].
e21
from hospital-based outcomes analyses for at leastsome key diseases/procedures. This analysis demon-strates the power of the risk-adjusted 30-d follow-upNSQIP data, but perhaps more importantly, the re-sponsibility of surgeons to monitor and optimize thedischarge process. � 2011 Elsevier Inc. All rights reserved.
Key Words: NSQIP; death after discharge; 30-dmortality; post-discharge death; risk-adjusted out-comes database; National Surgical Quality Improve-ment Program.
INTRODUCTION
The field of surgery has made rapid and remarkableprogress in the past half century. From John Gibbon’sdevelopment of the heart-lung machine in 1953 [1], toJoseph Murray’s first successful renal transplant in1954 [2], to laparoscopic and robotic surgery presently,providers are able to deliver a level of care to patientsthat was previously unachievable. However, despiteour advances, we face many challenges: to developnew technological innovations; to broaden and expediteaccess to medical care; to constrain spending; to maxi-mize patient satisfaction; and, most importantly, tolimit the morbidity and mortality that result from sur-gical care. In short, we are charged to provide care thatis better, faster, cheaper and safer than before.
To successfully address these challenges, we mustfirst have a thorough understanding of current prob-lems. We have begun to better grasp the frequency ofmorbidity and mortality in our patient population, andare also now aware that a significant percentage of theseare preventable. In a 1999 study of medical injury in15,000 patients in 28 Utah and Colorado hospitals, 3%of surgical patients were found to have experienceda complication, and approximately 6% of adverse eventsled to death [3, 4]. Furthermore, approximately half of
0022-4804/$36.00� 2011 Elsevier Inc. All rights reserved.
7

JOURNAL OF SURGICAL RESEARCH: VOL. 170, NO. 2, OCTOBER 2011e218
all adverse events were deemed preventable [3]. In thisstudy, eight operations had a significantly higher inci-dence of preventable surgical adverse events: abdominalaortic aneurysm repair, lower extremity bypass graft,coronary artery bypass graft (CABG)/valve surgery, co-lon resection, cholecystectomy, transurethral resectionof the prostate/transurethral resection of bladder tumor(TURP/TURBT), hysterectomy, and appendectomy.
These findings provided validity for earlier reports ofthe Harvard Medical Practice Study, which analyzedthe records of approximately 30,000 randomly selectedpatients in New York in 1984. In this landmark study,adverse events occurred in 3.7% of hospitalizations;13.6% of these led to infections (14%) and technical com-plications (13%). Almost half of all adverse events death[5]. Nearly 30% of adverse events were attributed tonegligence [5]. Drug complications were the most com-mon type of adverse event (19%), followed by wound(48%) associated with an operation [6].
Recent surgical literature research has sought to bet-ter characterize surgical morbidity and mortality. Forexample, it has been noted that for a subset of major op-erations (eg, cardiac surgery), inpatient mortality riskis lower in high-volume hospitals than in low-volumehospitals [7]. Interestingly, this positive volume-outcomes relationship may plateau at a certain pointand then diminish. In a study of hepatic resection,greater volume was associated with improvements inmortality up to an annual caseload of 50; the mortalityrate then increased when greater than approximately70 cases were performed per annum [8]. This may re-flect the high degree of complexity seen at the largestreferral centers. Other studies have focused on correlat-ing patient characteristics with inpatient morbidityand mortality. For instance, in an analysis of morethan 1 million records of the Nationwide InpatientSample (NIS), socioeconomic status at the level of theindividual patient has a statistically significant effecton operative mortality such that patients in the lowestsocioeconomic strata experience the highest operativemortality [9]. As another example, multiple studieshave demonstrated female gender to be an independentrisk factor for complications after CABG [10].
Literature has pointed out that postoperative in-hospital care has a profound impact on outcomes,spawning a new era of heightened vigilance in themedical care of our patients. Great strides have thusbeen made in characterizing surgical mortality. Thenext logical step is to evaluate morbidity and mortalityin the post-discharge period. If high, this should bea targeted area of intervention. To date, surgical mor-tality has largely been defined as those deaths that oc-cur during the inpatient hospitalization period prior todischarge. Many databases commonly accessed inoutcomes research, such as NIS, do not collect data
pertaining to the post-discharge period. As such, therates of post-discharge deaths after surgical proce-dures are unknown and may represent areas of qualityimprovement. However, the National Surgical QualityImprovement Program (NSQIP) database captures30-d outcomes not included within normal administra-tive databases, and can thus differentiate betweenin-hospital and post-discharge deaths. This study em-ploys the NSQIP database to characterize surgicalmortality occurring in the post-discharge period.
METHODS
This is a retrospective analysis of the NSQIP participant use datafile from the American College of Surgeons for the years 2005 through2007. The NSQIP is a nationally validated, risk-adjusted, outcomes-based program to measure and improve the quality of surgical care.The program employs a prospective, peer controlled, nurse-abstracted, and validated database to quantify 30-d risk-adjusted sur-gical outcomes.
Inclusion criteria for this study were procedures whose medianlength of stay was greater than 1 d (to exclude outpatient procedures),andwhose overall death ratewas greater than 2% (to include only pro-cedures where mortality was a significant issue). Procedures whereless than 25 deaths occurred were excluded for sample size concerns.
A post-discharge death was defined as a patient whose interval be-tween operation and death is greater than the interval between oper-ation and hospital discharge.
RESULTS
There were 363,897 patients with 2236 different CPTcodes captured in NSQIP. There were 6395 deaths,which results in an overall procedural mortality rateof 1.76%; among them, 1486 (23.2%) occurred afterdischarge.
Table 1, part A, listsmortality rates for all proceduresthat met inclusion criteria for this study (i.e., medianlength of stay greater than 1 d; overall death rategreater than 2%; and procedures where 25 or moredeaths occurred). In total, 38 procedureswere captured;of these, 23 were general surgery procedures and 15were vascular surgery procedures. Overall mortalityranged from a low of 2.4% (peripheral bypass withvein, as well as cholecystectomy) to a high of 37.2% (re-pair of ruptured abdominal aortic aneurysm). The gen-eral surgical procedure with the highest overallmortality was partial colectomywith colostomy or ileos-tomy and creation ofmucofistula (16.2%). Box 1 lists thetop 10 procedures with highest overall post-surgicalmortality rates.
Table 1, part B, lists the proportion of all death occur-ring after discharge for the 38 procedures captured inpart A. This proportion was calculated as number ofpost-discharge deaths in a specific procedure dividedby total deaths in that procedure. Two procedures, re-pair of ruptured abdominal aortic aneurysm and repairof abdominal aortic aneurysm involving iliac vessels,

TABLE 1
Part A. Overall Mortality Rates for all Captured Procedures. Part B. Proportion of Death Occurring AfterDischarge, Calculated as Number of Post-Discharge Deaths in That Procedure Divided by Total Deaths in
that Procedure
A B
CPT code CPT descriptionTotal
patientsTotaldeath
Proceduralmortality rate
TotalDeath
Post-dischargedeaths
Proportion of alldeath occurringafter discharge
35566 Bypass graft, with vein, femoral-anteriortibial, posterior tibial, peroneal artery,or other distal vessels
1076 26 2.4% 26 13 50.0%
34101 Embolectomy of thrombectomy, with orwithout catheter; axillary, brachial,innominate, subclavian artery, by armincision
226 30 13.3% 30 14 46.7%
27590 Amputation, thigh, through femur, anylevel
1444 179 12.4% 179 81 45.3%
43820 gastrojejunostomy, without vagotomy 446 36 8.1% 36 16 44.4%44130 Enteroenterostomy, anastomosis of
intestine, with or without cutaneousenterostomy (separate procedure)
464 40 8.6% 40 17 42.5%
35656 Bypass graft, with other than vein,femoral-popliteal
1305 32 2.5% 32 12 37.5%
27880 Amputation of leg, through tibia and fibula 1713 118 6.9% 118 43 36.4%35371 Thromboendarterectomy, including path
graft, if performed; common femoral733 28 3.8% 28 9 32.1%
44310 Ileostomy or jejunostomy, non-tube 427 41 9.6% 41 13 31.7%38100 Splenectomy; total (separate procedure) 698 39 5.6% 39 12 30.8%44320 Colostomy or skin level cecostomy 929 82 8.8% 82 22 26.8%47600 Cholecystectomy 3237 79 2.4% 79 20 25.3%34201 Embolectomy or thrombectomy, with or
without catheter, femoropopiteal,aortoiliac artery, by leg incision
747 96 12.9% 96 22 22.9%
44005 Enterolysis (freeing of intestinal adhesion)(separate procedure)
2425 122 5.0% 122 25 20.5%
44144 Colectomy, partial; with resection, withcolostomy or ileostomy and creation ofmucofistula
671 109 16.2% 109 21 19.3%
44143 Colectomy, partial, with end colostomy andclosure of distal segment (Hartmanntype procedure)
2172 244 11.2% 244 47 19.3%
35654 Bypass graft, with other than vein,axillary-femoral-femoral
189 26 13.8% 26 5 19.2%
35091 Direct repair of aneurysm,pseudoaneurysm, or excision (partial ortotal), and graft insertion, with orwithout patch graft; for aneurysm,pseudoaneurysm, and associatedocclusive disease, abdominal aortainvolving visceral vessels (mesenteric,celiac, renal)
448 26 5.8% 26 5 19.2%
48150 Pancreatectomy, proximal subtotal withtotal duodenectomy, partialgastrectomy, choledochoenterostomy,and gastrojejunostomy (Whipple-typeprocedure), with pancreatojejunostomy)
1588 52 3.3% 52 10 19.2%
44140 Colectomy, partial, with anastomosis 7323 325 4.4% 325 61 18.8%35646 Bypass graft, with other than vein,
aortobifemoral837 28 3.3% 28 5 17.9%
43632 Gastrectomy, partial, distal, withgastrojejunostomy
575 28 4.9% 28 5 17.9%
44141 Colectomy, partial, with skin levelcecostomy or colostomy
754 79 10.5% 79 14 17.7%
(Continued )
YU ET AL.: INCIDENCE OF DEATH FOLLOWING DISCHARGE e219

TABLE 1
(Continued )
A B
CPT code CPT descriptionTotal
patientsTotaldeath
Proceduralmortality rate
TotalDeath
Post-dischargedeaths
Proportion of alldeath occurringafter discharge
44120 Enterectomy, resection of small intestine,single resection, and anastomosis
4803 390 8.1% 390 62 15.9%
49000 Exploratory laparotomy, exploratoryceliotomy with or without biopsy(s)(separate procedure)
3753 576 15.3% 576 87 15.1%
44602 Suture of small intestine (enterorrhaphy)for perforated ulcer, diverticulum,wound, injury or rupture, singleperforation
392 61 15.6% 61 9 14.8%
44160 Colectomy, partial, with removal ofterminal ileum with ileocolostomy
3287 129 3.9% 129 19 14.7%
44155 Colectomy, total, abdominal, withproctectomy with ileostomy
487 37 7.6% 37 5 13.5%
44125 Enterectomy, resection of small intestine,with enterostomy
234 33 14.1% 33 4 12.1%
43840 Gastrorrhaphy, suture of perforatedduodenal or gastric ulcer, wound, orinjury
735 94 12.8% 94 11 11.7%
44150 Colectomy, total, abdominal, withoutproctectomy, with ileostomy orileoproctostomy
1137 144 12.7% 144 16 11.1%
35081 Direct repair of aneurysm,pseudoaneurysm, or excision (partial ortotal) and graft insertion, with orwithout patch graft; for aneurysm,pseudoaneurysm, and associatedocclusive disease, abdominal aorta
1160 56 4.8% 56 6 10.7%
49020 Drainage of peritoneal abscess or localizedperitonitis, exclusive of appendicealabscess, open
453 42 9.3% 42 4 9.5%
35102 Direct repair of aneurysm,pseudoaneurysm, or excision (partial ortotal) and graft insertion, with orwithout patch graft; for aneurysm,pseudoaneurysm, and associatedocclusive disease, abdominal aortainvolving iliac vessels (common,hypogastric, external)
710 35 4.9% 35 3 8.6%
49002 Reopening of recent laparotomy 614 99 16.1% 99 7 7.1%33877 Repair of thoracoabdominal aortic
aneurysm with graft, with or withoutcardiopulmonary bypass
297 32 10.8% 32 2 6.3%
35082 Direct repair of aneurysm,pseudoaneurysm, or excision (partial ortotal) and graft insertionwith or withoutpatch graft; for ruptured aneurysm,abdominal aorta
293 109 37.2% 109 0 0.0%
35103 Direct repair of aneurysm,pseudoaneurysm, or excision (partial ortotal) and graft insertionwith or withoutpatch graft; for ruptured aneurysm,abdominal aorta involving iliac vessels(common, hypogastric, external)
110 27 24.5% 27 0 0.0%
JOURNAL OF SURGICAL RESEARCH: VOL. 170, NO. 2, OCTOBER 2011e220
had no deaths post-discharge. In the other 36 CPT co-des, the proportion of deaths occurring after dischargeranged from 6.3% to 50.0%. Peripheral bypass with
vein demonstrated the highest proportion of death oc-curring after discharge (50%). There were several pro-cedures (upper extremity thrombectomy or
BOX 1
Top 10 Procedures with the Highest OverallProcedural Mortality Rate
ProcedureTotal
patientsTotaldeath
Proceduralmortality
rate
Ruptured AAA 293 109 37.2%Ruptured AAA, involving iliac vessels 110 27 24.5%Partial colectomy w/ mucofistula 671 109 16.2%Reopening of recent laparotomy 614 99 16.1%Suture repair of small intestine 392 61 15.6%Exploratory laparotomy 3753 576 15.3%SBR w/enterostomy 234 33 14.1%Axillary-femoral-femoral bypass 189 26 13.8%Embolectomy/thrombectomy, arm 226 30 13.3%Embolectomy/thrombectomy, leg 747 96 12.9%
AAA ¼ abdominal aortic aneurysm; SBR ¼ small bowel resection.
BOX 2B
Top 10 Procedures With the Highest Proportion ofDeath Occurring After Discharge
ProcedureTotaldeath
Post-dischargedeath
Proportionof deathoccurring
afterdischarge
Femoral-distal bypass w/vein 26 13 50.00%Embolectomy/thrombectomy, arm 30 14 46.70%Amputation, thigh 179 81 45.30%Gastrojejunostomy, without
vagotomy36 16 44.40%
Anastomosis of intestine 40 17 42.50%Femoral-popliteal bypass w/graft 32 12 37.50%Below knee amputation 118 43 36.40%Common femoral
thromboendarterectomy28 9 32.10%
Ileostomy or jejunostomy 41 13 31.70%Total splenectomy 39 12 30.80%
YU ET AL.: INCIDENCE OF DEATH FOLLOWING DISCHARGE e221
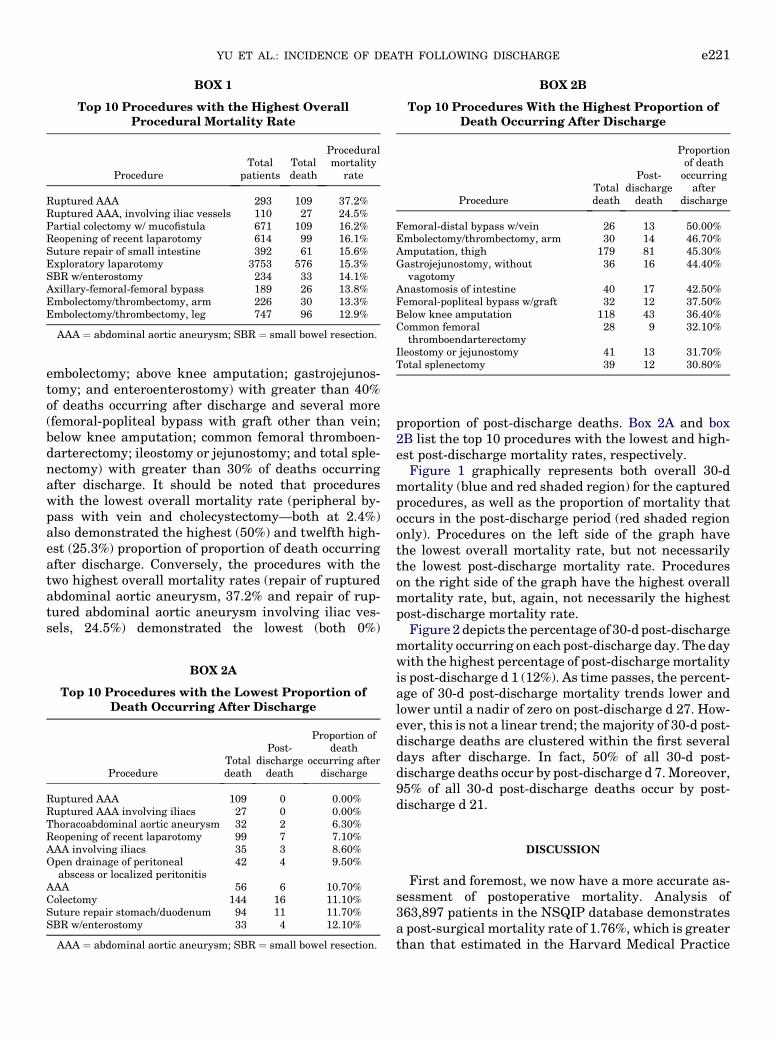
embolectomy; above knee amputation; gastrojejunos-tomy; and enteroenterostomy) with greater than 40%of deaths occurring after discharge and several more(femoral-popliteal bypass with graft other than vein;below knee amputation; common femoral thromboen-darterectomy; ileostomy or jejunostomy; and total sple-nectomy) with greater than 30% of deaths occurringafter discharge. It should be noted that procedureswith the lowest overall mortality rate (peripheral by-pass with vein and cholecystectomy—both at 2.4%)also demonstrated the highest (50%) and twelfth high-est (25.3%) proportion of proportion of death occurringafter discharge. Conversely, the procedures with thetwo highest overall mortality rates (repair of rupturedabdominal aortic aneurysm, 37.2% and repair of rup-tured abdominal aortic aneurysm involving iliac ves-sels, 24.5%) demonstrated the lowest (both 0%)
BOX 2A
Top 10 Procedures with the Lowest Proportion ofDeath Occurring After Discharge
ProcedureTotaldeath
Post-dischargedeath
Proportion ofdeath
occurring afterdischarge
Ruptured AAA 109 0 0.00%Ruptured AAA involving iliacs 27 0 0.00%Thoracoabdominal aortic aneurysm 32 2 6.30%Reopening of recent laparotomy 99 7 7.10%AAA involving iliacs 35 3 8.60%Open drainage of peritoneal
abscess or localized peritonitis42 4 9.50%
AAA 56 6 10.70%Colectomy 144 16 11.10%Suture repair stomach/duodenum 94 11 11.70%SBR w/enterostomy 33 4 12.10%
AAA ¼ abdominal aortic aneurysm; SBR ¼ small bowel resection.
proportion of post-discharge deaths. Box 2A and box2B list the top 10 procedures with the lowest and high-est post-discharge mortality rates, respectively.
Figure 1 graphically represents both overall 30-dmortality (blue and red shaded region) for the capturedprocedures, as well as the proportion of mortality thatoccurs in the post-discharge period (red shaded regiononly). Procedures on the left side of the graph havethe lowest overall mortality rate, but not necessarilythe lowest post-discharge mortality rate. Procedureson the right side of the graph have the highest overallmortality rate, but, again, not necessarily the highestpost-discharge mortality rate.
Figure 2 depicts the percentage of 30-d post-dischargemortality occurring on eachpost-discharge day. Thedaywith the highest percentage of post-dischargemortalityis post-discharge d 1 (12%). As time passes, the percent-age of 30-d post-discharge mortality trends lower andlower until a nadir of zero on post-discharge d 27. How-ever, this is not a linear trend; themajority of 30-d post-discharge deaths are clustered within the first severaldays after discharge. In fact, 50% of all 30-d post-discharge deaths occur by post-discharge d 7.Moreover,95% of all 30-d post-discharge deaths occur by post-discharge d 21.
DISCUSSION
First and foremost, we now have a more accurate as-sessment of postoperative mortality. Analysis of363,897 patients in the NSQIP database demonstratesa post-surgical mortality rate of 1.76%, which is greaterthan that estimated in the Harvard Medical Practice

FIG. 1. Post-discharge mortality versus 30-d mortality.
FIG. 2. Percentage of mortality occurring on each post-dischargeday.
JOURNAL OF SURGICAL RESEARCH: VOL. 170, NO. 2, OCTOBER 2011e222
Study (0.5%) and the Utah/Colorado study (0.2%). Thishigher rate of postoperative mortality can be attributedin part to the significant number of post-dischargedeaths (23.2% of all deaths) that are not includedwithinnormal administrative database reviews.
With respect to the mortality associated with specificprocedures, it is not surprising that cholecystectomy islowest, but it is surprising that peripheral bypass withvein also has the lowest mortality given the inherentmorbidity of that patient population. It is not surprisingthat repair of ruptured AAA has the highest overallmortality, but it is extremely surprising that there areno post-discharge deaths after repair of ruptured AAAor ruptured AAA involving iliacs. In other instances,however, the rate of post-discharge mortality does cor-relate with the complexity of the procedure, such as inthe case of femoral-distal bypass surgery (proportionof mortality occurring post-discharge: 50%). Therefore,the rates of post-discharge death do not necessarily, orintuitively, correlate with complexity of the surgicalprocedure.
It is concerning that peripheral bypass with vein hasan extremely high proportion of death occurring afterdischarge (50%). In light of this data, care should betaken to make sure these patients (as well as patientswho have undergone other surgical procedures withhigh rates of post-discharge death) are fully optimizedprior to discharge. Some assurance can be found in
the fact that peripheral bypass with vein has the lowestoverall mortality rate, and thus the high percentage ofpost-discharge deaths actually equates to a low abso-lute number of deaths. Also concerning is the possibilitythat patients discharged to rehabilitation facilities havedifficulty following up with primary care physicians.For example, the patients with femoral-tibial diseaseare predisposed to postoperative complications, yet wesend them to rehabilitation facilities that target physi-cal therapy, while cutting themoff from their internists.

YU ET AL.: INCIDENCE OF DEATH FOLLOWING DISCHARGE e223
One solution may be to implement a multidisciplinaryclinic approach to evaluating these patients preopera-tively and managing them postoperatively with sur-gery, cardiology, internal medicine, and physicaltherapy all involved. The multidisciplinary approachhas proven effective in bariatric surgery and other spe-cialties; it stands to reason it may help in vascular sur-gery. This is another area for improvement if we are todecrease the rate of post-discharge morbidity andmortality.
Perhaps the most concerning aspect of this studycomes from the revelation that there are a multitudeof procedures with a large proportion (30%–50%) ofoverall mortality occurring after hospital discharge.This data must impact our care of post-surgical pa-tients. It may warrant prolonged inpatient stay for ten-uous patients after specific procedures, earlier andmore frequent follow-up, and home health care visits.The timing of when post-discharge deaths occur is an-other factor that may justify prolonged inpatient stayfor certain patient populations as well as earlier outpa-tient follow-up. It is important to remember that thegreatest proportion (12%) of post-discharge deaths oc-cur on post-discharge d 1; thus, keeping certain pa-tients in the hospital one extra day may savea significant number of lives. Furthermore, as 50% ofpost-discharge deaths occur by post-discharge d 7, weshould not be waiting longer than 1 wk to see our pa-tients in the office. Delaying follow-up for 3 wk ormore would be folly, as 95% of mortal complicationswill have already occurred by this time. With insurancecompanies "grading" physicians and hospitals, the em-phasis by hospitals is to transfer patients who are likelynot to survive to hospice units, rehabilitation facilities,and so forth to improve the mortality rate, which cur-rently only measures inpatient deaths. This trend willlikely becomemore prevalent in a ‘‘pay for performance’’mentality. This will likely result in physicians (withpressure from the hospital administrators) to ‘‘turndown’’ the patients for high-risk procedures. Thus, re-porting 30-d outcomes (including those deaths that oc-cur after discharge) would be valuable and should betempered by the fact that the greater the length oftime after a procedure occurs, the more frequently areconfounders introduced.
We should also not assume that seemingly less com-plex surgery (i.e., cholecystectomy) has less morbidityor mortality and can go for a longer period before beingfollowed-up as an outpatient, whereas complex surgery(ie, ruptured AAA repair) should be seen as soon aspossible after discharge, which is the tendency ofmany health-care providers. We now know that AAArepair actually has no post-discharge death. It is possi-ble this is a consequence of the natural history of rup-tured AAA, that this patient population undergoes
rigorous follow-up, or that the patient populationmay be discharged to rehabilitation facilities, wheretheir progress remains monitored.
The bottom line is that these data point out a need toimprove our current follow-up system. It can be con-ceded that prolonged inpatient stay for the majority ofsurgical patients is costly andnot realistic in our currenthealth-care market. As previously mentioned, prolong-ing hospitalization by 1 or 2 d for select patients (thosestatus-post peripheral bypass, for example) may bea reasonable compromise. Other solutions, which mayvary in their feasibility, include earlier follow-up withphysicians, earlier and more frequent follow-up withmidlevel providers, and the use of technology (ie, homemonitoring, video-conferencing, e-mail, etc.) to trackthe well-being of discharged patients.
CONCLUSION
There is a significant incidence of death that occursafter discharge. Minimization or even elimination ofpost-discharge deaths alone could decrease our post-procedural mortality from 1.76% to as low as 1.35%.There is significant variation across surgical proce-dures in the likelihood of postoperative deaths occur-ring after discharge. Fifty percent of post-dischargedeaths occur by post-discharge d 7, and 95% ofpost-discharge deaths occur by post-discharge d 21,indicating that our current protocol of collectingpost-discharge mortality information up to 30 d afterhospital discharge is adequately inclusive. On theother hand, many currently employed inpatientoutcomes data systems that do not collect post-discharge data are under-representing post-surgicalcomplications. These data call into question conclu-sions drawn from hospital-based outcomes analysesfor at least some key diseases/procedures. Thesedata can also aid the decision-making process regard-ing the management of post-surgical patients, espe-cially with regard to the timing of discharge, timingand frequency of follow-up, and utilization of homenursing visits. Future studies must delve into thecause of post-discharge deaths so that a more thor-ough understanding and appropriate interventionscan be achieved. This analysis demonstrates thepower of the risk-adjusted 30-d follow-up NSQIPdata.
REFERENCES
1. Stoney WS. Evolution of cardiopulmonary bypass. Circulation2009;119:2844.
2. GuildWR, Harrison JH,Merrill JP, et al. Successful homotrans-plantation of the kidney in an identical twin. Trans AmClin Cli-matol Assoc 1955;67:167.

JOURNAL OF SURGICAL RESEARCH: VOL. 170, NO. 2, OCTOBER 2011e224
3. Gawande AA, Thomas EJ, Zinner MJ, et al. The incidence andnature of surgical adverse events in Colorado and Utah in1992. Surgery 1999;126:66.
4. ThomasEJ, StuddertDM,BurstinHR, et al. Incidence and typesof adverse events and negligent care in Utah and Colorado. MedCare 2000;38:261.
5. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverseevents and negligence in hospitalized patients. Results of theHarvard Medical Practice Study I. N Engl J Med 1991;324:370.
6. Leape LL, Brennan TA, Laird N, et al. The nature of adverseevents in hospitalized patients. Results of the Harvard MedicalPractice Study II. N Engl J Med 1991;324:377.
7. EggliY,HalfonP,MeylanD,et al. Surgical safetyandhospital vol-ume across a wide range of interventions. Med Care 2010;48:962.
8. Kohn GP, Nikfarjam M. The effect of surgical volume and theprovision of residency and fellowship training on complicationsof major hepatic resection. J Gastrointest Surg 2010;14:1981.
9. Bennett KM, Scarborough JE, Pappas TN, et al. Patient socio-economic status is an independent predictor of operativemortal-ity. Ann Surg 2010;252:552. discussion 557.
10. KimC,RedbergRF, Pavlic T, et al. A systematic review of genderdifferences in mortality after coronary artery bypass graft sur-gery and percutaneous coronary interventions. Clin Cardiol2007;30:491.





























