Embed Size (px)
Citation preview
©2011, Shelene Giles. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior written permission from the publisher.
Section 5
Burns
WORKBOOK
Nurse Life Care Planning - Through the Ages
©2011, Shelene Giles. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior written permission from the publisher.
Nurse Life Care Planning - Through the Ages Section 5 – Burns
OBJECTIVE 1: Explain the anatomy/physiology/function of the skin. Identify levels of impairment based on severity
of catastrophic burns.
OBJECTIVE 2: Describe acute and chronic complications of catastrophic burns. Identify long term treatment and
outcomes of catastrophic burns.
OBJECTIVE 3: Apply and demonstrate the nursing process as a life care planning foundation for a catastrophic burn
client.
_______________________________________________________________________________________
Agenda
Overview
Nurse Life Care Planning Process
Case Study
_______________________________________________________________________________________
Overview
Incidence
Over 2 million burn cases per year
National Burn Repository (1999 – 2008)
127,016 cases over 10 years
Majority of burns are less than 10% TBSA
_______________________________________________________________________________________
Age
Mean age for all cases - 32 years old
Ages 20-50 years old - highest prevalence of burns treated at burn centers
Patients age 60 or older accounted for 12% of all cases
Children under age 5 accounted for 17% of all cases
Page 3 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Ethnicity
63.0% - Caucasian
17.4% - African American
13.0% - Hispanic
Gender
Majority were men
_______________________________________________________________________________________
Etiology
Location
65.5% - Home
11.1% - Industrial
7.2% - Street/Highway
7.0% - Unspecified
4.5% - Recreation/Sports
2.5% - Public Building
1.1% - Residential Institution
0.9% - Farm
0.1% - Mine/Quarry
_______________________________________________________________________________________
Circumstance
65.0% - Accident/Non-Work Related
15.2% - Accident/Work Related
4.6% - Recreation
4.5% - Unspecified
1.6% - Suspected Assault/Abuse
1.2% - Suspected Self-Inflicted
1.2% - Suspected Child Abuse
0.2% - Suspected Arson
_______________________________________________________________________________________
Cause
41.8% - Thermal (fire/flame)
30.1% - Scald
9.0% - Other (non-burn)
8.5% - Contact with hot object
3.8% - Electrical
2.8% - Chemical
2.4% - Unspecified
Page 4 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
0.8% - Skin disease
0.3% - Radiation
0.3% - Inhalation
_______________________________________________________________________________________
Thermal
Exposure to heat from flame, steam, contact with hot surface, hot liquid, or sun
Most non-work related accidents - occurs at home
More common in adults
Most common cause of severe burns
Most common cause of admission to burn center
Causes superficial to 4th degree burns
_______________________________________________________________________________________
Scald
Severity of scald = temperature x exposure time
Most prevalent in children (under age 5) & elderly
More common in kitchen (not bathroom)
Product (clothing, food, drink, sauces, etc.) worsens severity of injury
_______________________________________________________________________________________
Electrical (HANDOUT - Electrical and Lightning Injuries)
<1,000 volts - low (home)
>1,000 volts - high (industrial)
Actual flow of current most important when considering extent of electrical burn injury
Skin burns where current enters/exits - contact points
Extent of injury deceptive - minimal epidermis/dermis damage & deep tissue damage, damage frequently progresses
_______________________________________________________________________________________
Poly-trauma
Secondary diagnosis - compartment syndrome, cardiac arrhythmias, respiratory, urinary (myoglobinuria),
musculoskeletal (electricity contracts muscles)
Multi-disciplinary team
Long term complications
Neurological symptoms – most common symptoms are memory loss, numbness, headache, chronic pain, weakness
and poor concentration
Musculoskeletal symptoms – most common symptoms are pain, limited range of motion, and contracture
_______________________________________________________________________________________
Page 5 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Chemical
Alkalines (oven cleaners, fertilizer, industrial cleaners), acids (household products), hydroflouric acids ( inorganic
acids, used in metal processing/cleaning), organic compounds (gasoline, diesel fuel, chemical disinfectants)
Initially unaware of chemical burn
Progressive damage until removed or neutralized
Extent of injury deceptive - superficial progresses to full thickness
Severity depends on chemical, concentration, and contact time
_______________________________________________________________________________________
Inhalation
3 classifications of inhalation injury: carbon monoxide poisoning, upper airway, and lower airway
Most common cause of inhalation injuries & cause of death - house fire
Long term pulmonary complications
_______________________________________________________________________________________
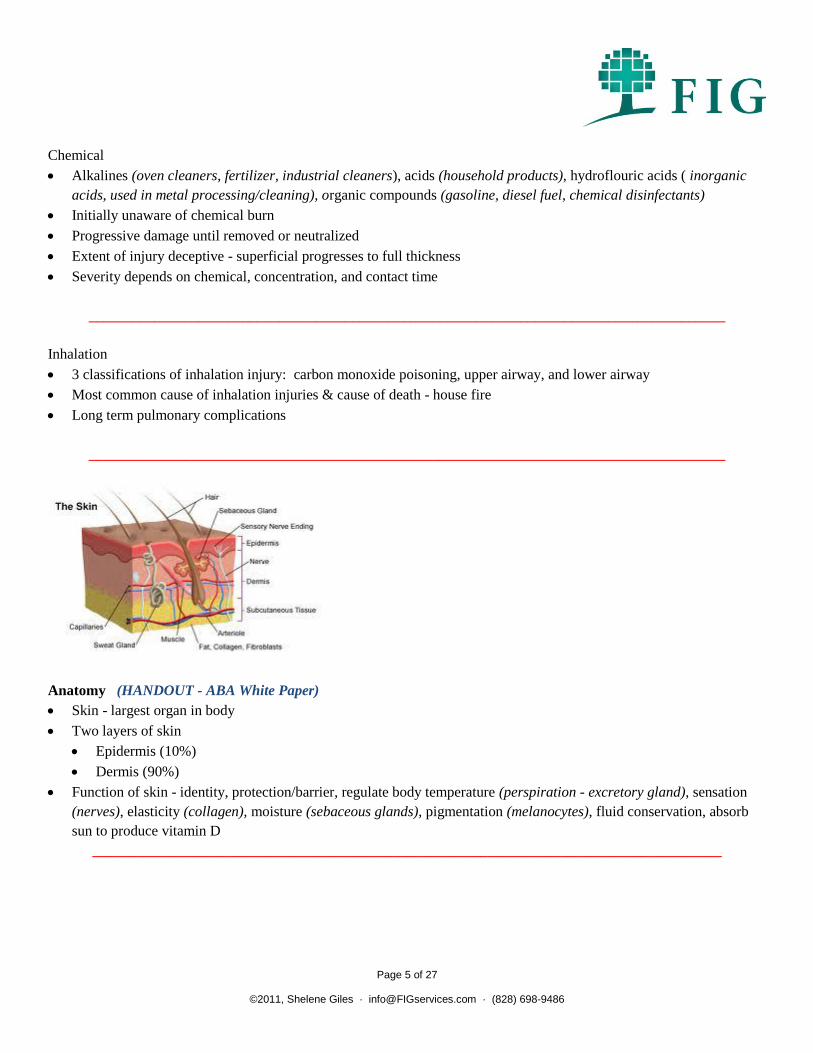
Anatomy (HANDOUT - ABA White Paper)
Skin - largest organ in body
Two layers of skin
Epidermis (10%)
Dermis (90%)
Function of skin - identity, protection/barrier, regulate body temperature (perspiration - excretory gland), sensation
(nerves), elasticity (collagen), moisture (sebaceous glands), pigmentation (melanocytes), fluid conservation, absorb
sun to produce vitamin D
______________________________________________________________________________________
Page 6 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
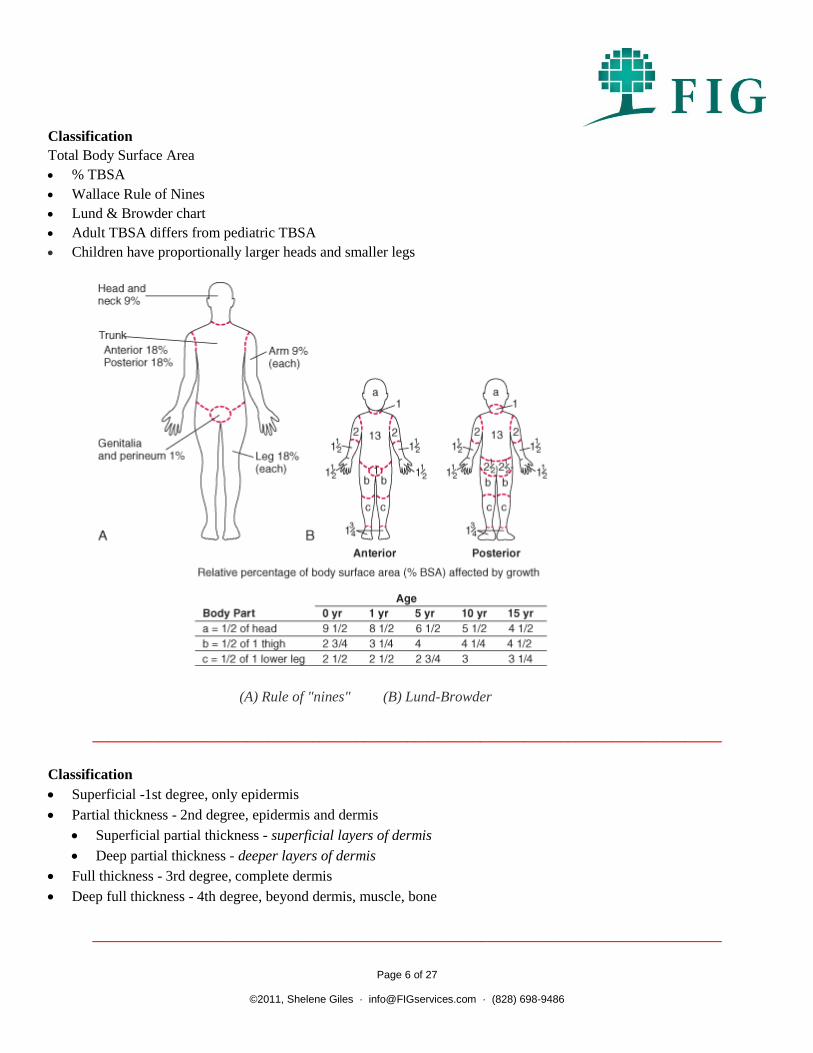
Classification
Total Body Surface Area
% TBSA
Wallace Rule of Nines
Lund & Browder chart
Adult TBSA differs from pediatric TBSA
Children have proportionally larger heads and smaller legs
(A) Rule of "nines" (B) Lund-Browder
______________________________________________________________________________________
Classification
Superficial -1st degree, only epidermis
Partial thickness - 2nd degree, epidermis and dermis
Superficial partial thickness - superficial layers of dermis
Deep partial thickness - deeper layers of dermis
Full thickness - 3rd degree, complete dermis
Deep full thickness - 4th degree, beyond dermis, muscle, bone
______________________________________________________________________________________
Page 7 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Superficial burns
First degree
Involves epidermis
Dry, red skin, no blistering
Blanches with pressure, edema
Painful
Example – sunburn
Heals in 1-7 days
No scarring
0% TBSA
______________________________________________________________________________________
Superficial partial thickness burns
Second degree
Involves epidermis & surface layers of dermis
Weeping, red/pink, blistering
Blanches with pressure, edema
Most painful
Example – scald
Will heal on own and minimal scarring - skin able to re-epithelialize - cells regenerate on top surface, usually no
scarring if healed within 2 weeks
______________________________________________________________________________________
Deep partial thickness burns
Second degree
Involves epidermis & deeper layers of dermis
Large blisters, mottled white/pink or cherry red
Less moist, less blanching, and less painful
Example - flame
Skin grafting and severe scarring - heals by scar contraction & scar deposition (limited epithelium in middle of
wound)
______________________________________________________________________________________
Page 8 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Full thickness burns
Third degree
Involves epidermis & dermis - entire thickness of skin/into fat
Any color (white, gray, red, black/brown)
Dry skin, no sensation, no pain
Example – flame
Skin grafting and severe scarring - heals by scar contraction & scar deposition (no epithelium left in middle of
wound)
______________________________________________________________________________________
Deep full thickness burns
Fourth degree
Involves epidermis, dermis, blood vessel, nerve, tendon, muscle, and bone
Consider amputation
Skin grafting and severe scarring
Poor prognosis
Toxic Epidermal Necrotizing Syndrome (TENS) (HANDOUT - TENS)
______________________________________________________________________________________
Acute Care (HANDOUT - Burns at Extremes of Age)
ABA burn center referral criteria
2nd or 3rd degree burns >10% TBSA (under 10 years and over 50 years of age)
2nd or 3rd degree burns >20% TBSA (in other age groups)
2nd or 3rd degree burns involving face/hands/feet/genitalia/perineum/major joints
3rd degree burns >5% TBSA (any age group)
Electrical burns, including lightning injury
Chemical burns
Inhalation injury (smoke or chemicals)
Pre-existing medical disorders that could complicate management, prolong recovery, or affect mortality
Concomitant trauma where burn injury poses greatest risk of morbidity or mortality
Children in hospitals without specialized pediatric unit
Patients requiring special social, emotional, or long-term rehabilitation support
______________________________________________________________________________________
Page 9 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Acute Care (HANDOUT - Care of Outpatient Burns) (HANDOUT - Care of Burn Patients in Hospital)
(HANDOUT - Infection Control) (HANDOUT - Nutritional Care) (HANDOUT - Pain Management) (HANDOUT -
Respiratory Care)
Emergency room/transfer to burn center
ABC resuscitation
Fluid resuscitation Intubation
Sedation/Pain management
Diagnostic studies
Prevent infection
Nutritional support
Surgery
Emergency escharotomy and/or fasciotomy
Skin debridement /wound coverage- remove necrotic skin, aggressive wound excision/debridement
Skin grafting
Allograft/homograft - cadaver or porcine skin
Auto graft - own skin, donor site
Split thickness skin graft vs. full thickness skin graft
Cultured epidermal auto graft (CEA)
Wound care/dressing changes
Positioning/splinting/rehabilitation
Psychological support
Transfer to inpatient rehabilitation unit vs. discharge home
______________________________________________________________________________________
Acute Complications (HANDOUT - Review of Burn Injury Research)
Hypothermia
Compartment syndrome - compromises nerves/muscles/blood flow, loss of limb/life without intervention, emergency
escharotomy/fasciotomy, permanent nerve damage
Adult Respiratory Distress Syndrome (ARDS)
Rhabdomyolysis
Myoglobinuria
Respiratory failure - risk increases drastically after 4 days on ventilator, tracheostomy with prolonged ventilator
Organ failure
*Pneumonia - risk increases drastically after 4 days on ventilator, main complication in thermal burns
*Cellulitis - main complication in scald burns
*Urinary tract infection
*most common
Infection (wound/line/systemic)
Septicemia
Renal failure
Page 10 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Arrhythmia
Psychological (HANDOUT - Emotional Distress & Resources) (HANDOUT - Anxiety During Wound Care)
(HANDOUT - Burn Pain and Patients' Responses)
_______________________________________________________________________________________
Length of Stay
61% transferred to burn center
1 day of hospitalization equals 1% TBSA
Mean length of stay in burn center was 9 days
Majority discharged home without home health
96.0% - Lived
4.0% - Mortality
Mean charge for 20-29.9% TBSA = $130,043
Mean charge for 50-59.9% TBSA = $447,705
Mean charge for 70-79.9% TBSA = $741,125
_______________________________________________________________________________________
Health Care Expenses
Primary Payor
21.4% - Government (Medicaid/Medicare)
19.7% - Private health insurance
12.3% - Self pay
8.8% - Workers' compensation
5.6% - Managed care
26.2% - No insurance
_______________________________________________________________________________________
Chronic Care
Discharge home
Wound care
Symptom management (HANDOUT - Neuropathic pain) (HANDOUT - Memories of Pain)
Scar management
Extensive rehabilitation
Psychological services (HANDOUT - Psychosocial Care)
Reconstructive surgeries (HANDOUT - Reconstructive Surgery)
_______________________________________________________________________________________
Wound Care
Page 11 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Dressing changes twice daily
After epithelialization occurs, no further dressing changes
Begin scar management - creams/ointments, moisturizers, sunscreen & scar massage/stretching/ROM daily
Begin compression garments
Begin extensive rehabilitation - OT/PT
6 months to 2 years for burn wound to completely heal
_______________________________________________________________________________________
Nurse Life Care Planning Process
Assessment
Nurse Life Care Plan Assessment
Integumentary
Musculoskeletal
Neurologic
Respiratory
Cardiovascular
Gastro
Urinary
Psychosocial
FIM-FAM
Bathing/showering/hygiene
Grooming
Dressing
Feeding
Mobility
Transportation
Living arrangements
Safety
_______________________________________________________________________________________
Nursing Diagnosis
Impaired skin integrity
Risk for imbalanced body temperature
Risk for impaired nutrition
Impaired social interaction
Disturbed body image
Anticipatory grieving
Risk for infection
Risk for injury
Interrupted family processes
Page 12 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Caregiver role strain
Post-trauma syndrome
_______________________________________________________________________________________
Outcomes
Focused on physical and psychosocial impairments and community re-integration
Life expectancy similar to general population - except organ involvement/long term complications
Long term physical, social, and psychological impairments
Symptom management
Prevent complications - physiological and psychological
_______________________________________________________________________________________
Symptom management - improve function/quality of life, reduce symptoms/pain, and prevent complications
Oral/topical medications
Home modalities
Scar management (HANDOUT - Emotional Associations with Skin)
Compression garments
Silicone gel/silicone gel sheets
Moisturizer/lotion
Sunscreen
OT/PT (HANDOUT - Restoration of Function) (HANDOUT - Hand Burns)
Scar massage/desensitization (HANDOUT - Itching, Pain & Anxiety Levels Reduced with Massage Therapy)
Thermo regulated clothing
UV protectant clothing
_______________________________________________________________________________________
Reconstructive surgeries
Excision and complex closure
Excision and advancement flap
Tissue expander - 2 procedures
Z-plasty, Y-plasty, W-plasty
Split/full thickness skin graft - donor site
Removal of lesions/tumors/neuromas
Orthopedic repair
_______________________________________________________________________________________
Page 13 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Psychosocial (HANDOUT - Psychological Health and Function After Burn Injury) (HANDOUT - Community
Integration)
Crisis for patient, family, and social circle
Emotional trauma can physically alter brain
Trauma activates stress response system in brain (fight or flight syndrome)
Severe or chronic stress prevents brain from returning to relaxed state
_______________________________________________________________________________________
Trauma can damage cognitive, behavioral, and physical development in children
Surviving trauma depends on patient/family vulnerability and/or resiliency
Due to severity of medical condition, psychological condition often overlooked
Family psychological condition also often overlooked
_______________________________________________________________________________________
Psychosocial (HANDOUT - Positive Change After Severe Burn Injuries) (HANDOUT - Coping Strategies of Eight
Patients With Significant Burn Injury)
Early diagnosis & intervention improves outcome
Symptoms - sadness, hopelessness, insomnia, nightmares, anxiety
Diagnosis - adjustment disorder, anxiety, depression, Post-Traumatic Stress Disorder (PTSD)
(HANDOUT - Posttraumatic Stress Disorder & Pain Impact Functioning)
Treatment - counseling (individual and family), medications
_______________________________________________________________________________________
Educational/Vocational (HANDOUT - Barriers to Employment)
Restrictions/limitations
Environmental - temperature controlled environment, allergen free/limited dust particles, limited sun exposure
Physical - lifting/carrying/pushing/pulling/reaching, standing/walking, stairs, endurance/stamina
Psychological - societal reaction, disturbed body image
Return to school (HANDOUT - School Re-entry) (HANDOUT - Bullying on Burn Children)
Delayed growth and development
Excessive absences
Learning environment
Classmates/peers
Social scene
Page 14 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Return to work (HANDOUT - Return to Work after Low Voltage Electrical Injury) (HANDOUT - Return to Work
Barriers) (HANDOUT - Barriers Impacting Employment)
Predictors of return to work - classification, TBSA, and location
1 year post burn - predictors of return to work shift to physical abilities, psychosocial factors, and working conditions
Pain and neurological impairments most common reasons for not returning to work
_______________________________________________________________________________________
Outcomes
Collaboration
Burn specialist
Physicians
Therapists (OT, PT, psych)
Home health providers
Equipment vendors
_______________________________________________________________________________________
Medical Research
Model Systems Knowledge Translation Center - Burn
2001 Clinical Practice Guidelines for burn care
American Burn Association/Journal of Burn Care & Research
International Society of Burn Injuries/Burns Journal
(HANDOUT - TENS Clinical Guidelines)
_______________________________________________________________________________________
Chronic Complications (HANDOUT - Long Term Outcomes) (HANDOUT - Long Term Sequelae of Low Voltage
Electrical Injury) (HANDOUT - Risk Factors for Ophthalmic Complications in Patients With Burns)
Hypertrophic or keloid scarring
Pruritis
Pigmentation changes
Altered sensations
Fragile skin
Temperature regulation (HANDOUT - Temperature Responses)
Loss of sebaceous glands
Pimples/blackheads
Altered hair growth pattern
Peripheral neuropathy
Vision impairment
Page 15 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Epidermal inclusion cysts
Marjolin's ulcers (HANDOUT - Marjolin's Ulcers)
Skin cancer
Nerve impingement (HANDOUT - Compression Neuropathy)
Amputation
Contractures (HANDOUT - Joint Contracture)
Heterotopic ossification (HANDOUT - Heterotopic Ossification)
Osteomyelitis
Osteoarthritis/degenerative joint disease
Vascular compromise
Loss of ability to protect from sun exposure
Ulcerations and skin breakdown
Poor temperature regulation
Pain (HANDOUT - Pain Management after Electrical Injury)
Inhalation injury - progression of pulmonary insufficiency
Electrical injury - cardiovascular disease, progressive degeneration of neurological system, early arthritis, early cataract
Psychological factors (HANDOUT - Psychiatric Sequelae) (HANDOUT - Nightmares & PTSD)
_______________________________________________________________________________________
Planning
Treatment Recommendations in Nurse Life Care Plan
Medical
Physician appointments/evaluations
Burn Specialist
Plastic Surgeon
Dermatologist
Physiatrist/Pain Management
Neurological
Musculoskeletal
Respiratory
Cardiovascular
Genitourinary
Gastrointestinal
Endocrinology
Vascular
ENT
Psychiatrist
Audiologist
Ophthalmologist
_______________________________________________________________________________________
Page 16 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Surgeries/Procedures (invasive vs. non-invasive)
Reconstructive surgeries
Kenalog injections
Laser resurfacing
Dermabrasion
Tattooing
Orthopedic - contractures
Hospitalizations
Pneumonia
Infection
_______________________________________________________________________________________
Therapeutic Evaluations
OT
PT
Lymphadema
Neuropsych - cognitive
Nutrition
Speech
Psychological (HANDOUT - Acute Stress in Young Children) (HANDOUT - Rates, Trends, and Severity of
Depression after Burn Injuries)
_______________________________________________________________________________________
Therapeutic Modalities
OT (HANDOUT - The Effect of Hand Burns on Quality of Life in Children)
PT
Lymphadema
Cognitive
Nutrition
Speech
Psychological (individual & family) (HANDOUT - Behavioral Perceptions)
Recreational
_______________________________________________________________________________________
Page 17 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Diagnostic studies
Musculoskeletal - x-rays, MRI/CT scan, bone scan
Neurological - EMG/NCV studies
Vascular -ultrasound, Venous Doppler study
Lab work
Comprehensive metabolic panel - includes BUN & creatinine (liver & kidney function - should establish baseline &
then periodic follow-up
_______________________________________________________________________________________
Medications
Analgesic
Non-steroidal anti-inflammatory
Itching
Vitamin D supplement
Depression/anxiety
Sexual function
_______________________________________________________________________________________
Medical supplies
Wound care/dressing changes
Skin care
TED hose
_______________________________________________________________________________________
Scar Management
Compression garments
Silicone gel sheets
Splinting
Scar massage
Moisturizer
Sunscreen
UV protectant clothing
Thermo regulated clothing
Cooling agents
_______________________________________________________________________________________
Page 18 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Durable Medical Equipment/Aids for Independent Function
Specifics of DME is dependent on level of physical/functional ability, and secondary issues related to burns
Examples of DME
Hospital bed
Wheelchair/walker/crutches/cane
Humidifier
Air purifier
Allergen free products
Climate controlled environment
Mattress/overlay
Anti-scald hand held shower head
Shower chair
Adaptive clothing
Household aids
_______________________________________________________________________________________
Prosthesis/Orthosis
Upper extremity splints
Upper extremity prosthesis - for function or cosmesis
Lower extremity orthosis
Lower extremity prosthesis - for function or cosmesis
Customized shoes
OT evaluation/re-evaluation
_______________________________________________________________________________________
Mobility
Wheelchair evaluation
Manual wheelchair
Power assist wheelchair
Power wheelchair
Scooter
Wheelchair maintenance/repair
Wheelchair accessories
_______________________________________________________________________________________
Page 19 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Non-medical
Home care/living arrangements
Present options (present pros & cons)
Home - apartment, renovate home vs. purchase home
Assisted living
Skilled nursing facility
Housekeeping
Home/lawn maintenance
_______________________________________________________________________________________
Home health care vs. respite care
Levels of home care
Skilled (RN or LPN)
Unskilled (Certified Nursing Assistant/Home Health Aide, Personal Care Attendant, or Companion) -
bathing/showering, hygiene, grooming, dressing, feeding, cooking, cleaning, transportation, errands
Level of skilled or unskilled care dependent on nursing board in state of residence
_______________________________________________________________________________________
Architectural renovations
Safety
Barrier free
Wheelchair accessible design
Assistive technology
OT home evaluation
Contractor home evaluation
_______________________________________________________________________________________
Transportation
Airfare/overnight expenses
Driver evaluation
Wheelchair accessible transportation
Personal vehicle
Handicap parking permit
Tinted windows
Climate controlled vehicle
Public transportation
_______________________________________________________________________________________
Page 20 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Educational/Vocational (HANDOUT - Military Return to Duty & Civilian Return to Work)
Vocational evaluation
Vocational case management
Vocational retraining
Vocational modifications
Restrictions - climate controlled environment, limited sun exposure, limited dust particles, limited
lifting/carrying/pulling/pushing, limited standing/walking/stairs
_______________________________________________________________________________________
Other (HANDOUT - Summer Camps) (HANDOUT - Burn Camp) (HANDOUT - Sources of Support)
(HANDOUT - Burn Survivor Perspective)
Case management
Support group - burn associations/conferences - Burn World Conference
Burn camp/family camp
Fitness - gym vs. home
Recreational modifications
Cosmetics
_______________________________________________________________________________________
Page 21 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Case Study
Name: Mr. Burned
DOB: 10/19/79, Age 31
DOI: 12/19/06
Brief description of injury/accident:
Flash/flame burns
41% TBSA
Complications requiring extended 3 month hospital stay
Diagnoses:
Deep partial to majority full thickness burns to 41% total body surface area (TBSA) including face, mouth, neck, hands,
upper extremities, abdomen, back, and lower extremities
S/P compartment syndrome of upper extremities
S/P emergency escharotomies & fasciotomies, S/P skin debridement/grafting
late affects of thermal burns
hypertrophic scarring
abdominal contour deformity
inclusional cysts
chronic pruritis
S/P coccygeal and buttocks pressure ulcers (stage II – III)
S/P acute respiratory failure
S/P pneumonia
S/P hypermetabolism
S/P malnutrition
S/P pinning & arthrodesis of right little proximal interphalangeal (PIP) joint
MRSA
diffuse/chronic pain
neuropathy
adjustment disorder
post traumatic stress disorder (PTSD)
major depression
Acute Care:
escharotomies and fasciotomies
skin debridement
skin grafting (temporary & permanent)
ventilator support for ARDS
Cardiac pulmonary monitoring
Page 22 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
OT/PT
Psychological support
3 months in hospital
Complications:
Life threatening compartment syndrome/escharotomies and fasciotomies
Adult Respiratory Distress Syndrome (ARDS)
Systemic infections
Pneumonia
Difficulty weaning from ventilator
Decubitus ulcers
Hypertension
Hypertrophic granulation tissue
Insomnia
Intense pain
Current Care:
Dr. Turner (Burn Specialist) deferred future reconstructive surgery recommendations to Dr. Fogert (Reconstructive
Surgeon). Dr. Turner's last dictation - MMI (12 months) after last reconstructive surgery - timeframe unknown, long term
disability related to the burn accident.
Dr. Fogert's last dictation indicated – recovering from recent reconstructive surgery to right upper extremity, post-op
dressing changes, wound care, medications, OT, customized Jobst compression garments, and physician follow up.
Dr. Whetherford – chronic pain evals every two months, long term medications for pain management
Mr. Cary – psychological care every two weeks, suggested marriage counseling due to strain of injury
Urologist – evaluation recommended due to erectile dysfunction related to PTSD
Dr. Primary Care - see prn for overall health related to burn accident
OT - continues OT sessions twice weekly during recovery of right upper extremity reconstructive surgery, goal –
transition to independent home program
Scar management – wife provides care at home
Nurse case management services - coordinate medical care
Health for home based therapies & home health aide as needed after surgeries
Medical supplies/DME - see below
Page 23 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Medications:
Oxycontin 30mg every 8 hours
Oxycodone 2-3 pills every 4-5 hours
Ibuprofen 800mg 1-2 times daily
Neurontin 600mg twice day
Valium 5mg twice day
Zoloft 50mg twice day
OTC Zyrtec as needed (1-2 times per week)
OTC Benadryl as needed (average daily)
Vitamin D supplement (#30)
Centrum multivitamin (#120)
Medical Supplies/DME/Aids for Independent Function:
Customized right upper extremity splint, neoprene sleeve - daily
Medical supplies for dressing changes (Xeroform, Aquacel, Silvagel, gauze, tape, etc.) - daily
Gel mattress pad (queen size)
Allergen control products (non-allergenic soaps, laundry detergent, lotion)
Humidifier
Air purifier
Shower head with anti-scald valve
Medical alert bracelet
Symptoms/Limitations:
Skin
Hypertrophic scarring on burn sites/graft sites
Pigmentation changes on burn sites/graft sites/donor sites
Significant muscle loss/atrophy on abdomen/flank/back
Scar contractures on right arm, abdomen, and back
Extreme skin tightness/scar bands/scar contractures causing limited range of motion
Takes a while to stretch and get going in the mornings due to scar tightness/scar bands/scar contractures
Skin tearing/shearing with range of motion due to scar bands/scar contractures
Extremely fragile skin, frequent breakdown/shearing/open areas of skin with slightest friction
Chronic skin breakdown/ulcerations/open wounds on arms and back
Several areas of ulceration/discoloration/bruising
Delayed wound healing
Chronic itching, increased with warm/hot environment
Clothes rub/irritate/blister skin, especially flank/waist line
Bleeding on clothes and bed sheets, frequent replacement
Excessive dryness/flaking/peeling skin, requires frequent moisturizer
Impaired temperature regulation
Inability to regulate body temperature
Temperature hypersensitivity
Easily overheated, prefers to stay inside, only outside when going to/from car
Only able to tolerate being outside for few minutes in shade/indirect sunlight (i.e., father building covered
back porch)
Takes a while to „cool down‟ once overheated, causes fatigue/exhaustion
Altered sensation over burn scars/graft sites
Unable to feel light touch on burn scars/graft sites
Page 24 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Extreme sensitivity with loss of fascia/muscle and thin skin on bone
Unable to feel shower water on skin, unable to determine temperature of shower/bath water
Altered hair growth pattern
Altered perspiration
Excessive perspiration on unburned areas
Self conscious of burn scars and disfigurement
Upper extremity
Right little finger nonfunctional
Unable to flex/extend right little finger, fusion of PIP joint
Limited range of motion in right upper extremity, including shoulder
Scar band/contracture radiating from right flank into right shoulder/elbow/hand
Limited strength in right upper extremity
Limited grip strength in right hand
Limited gross motor coordination in right hand
Extremely limited fine motor coordination in right hand (i.e., unable to pick up small objects)
Vibration bothersome, both hands
Limited writing or typing with right hand
Unable to perform repetitive motion in right hand/wrist
Left hand/wrist pain with repetitive motion due to scar tightness
Right hand numbness/tingling
Right hand/wrist pain/throbbing
Drops objects when lifting/carrying with right hand
Limited abduction in right wrist
Increased symptoms with activity (less than 5 minutes) of right hand (i.e., washing dishes)
Numbness/tingling with prolonged position (longer than 20 minutes)
Tends to hold arms above head to lessen symptoms
Cold weather exacerbates symptoms
“Pain to the bone” during cold weather
Constantly wears insulated leather gloves during cold weather
Joints click/pop
Limited with caution and short timeframe for reaching/lifting/ pushing/pulling due to skin graft tightness and pressure on
scars, causes increased symptoms
Lower extremity
Lower extremity numbness/tingling with prolonged position (20 minutes)
Knee stiffness
Joints click/pop
Slow, guarded walking
Able to walk short distances
Prolonged walking/standing causes increased symptoms and fatigue (i.e., grocery shopping)
Aches/pains with prolonged walking/standing
Unable to run
Sitting causes increased symptoms (i.e., prefers to sit in recliner chair or lie on couch at home)
Unable to sit on hard surfaces due to loss of buttocks muscle, back pain, tightness with scarring, and skin
sensitivity
Limited with caution and short timeframe for crawling/kneeling/squatting/bending/stooping due to skin graft
tightness and pressure on scars, causes increased symptoms and numbness/tingling
Legs go to sleep with kneeling
Page 25 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Difficulty with rising from sitting position or getting up from floor
Unable to climb ladders/heights
Other
Sharp, aching, burning, throbbing pains on 24/7 basis
Back pain
Difficulty with bending at waist
Low back pain due to weakness and skin tightness
Pain/symptoms increase with activity/prolonged position (longer than 10-20 minutes)
Pain/symptoms increase with warm/hot temperature
Pain/symptoms decrease with medications and rest/lying down
Vision worse
Sensitivity to outside light, wears sunglasses
Prefers lights off while inside
Noise sensitivity & distraction (i.e., prefers radio off while riding in car)
Throat soreness following each surgery due to intubation
Difficulty starting/stopping urine stream (Foley catheter for two months while hospitalized)
Easily fatigued/tired (i.e., became drowsy/sleepy after 3 hours into Life Care Plan assessment)
Fatigue/tiredness, needs frequent rests/breaks
Decreased stamina/endurance
Frequent breaks/rest with shopping/running errands
Overall weakness
Overall limited range of motion
Overall limited strength
Piddles around on good days
Stays on couch/recliner chair on bad days
Psychological & cognitive
No loss of consciousness during burn accident
Detailed memories of accident
Remembers fire, jumping off ladder, and being on fire
Remembers seeing clothes burning and burned/melted skin on arms
In/out of consciousness during emergency room
Hallucinations/nightmares/reliving accident while in sedated coma and on medications
Sadness/depression
Anxiety/nervousness toward accident
Increased anxiety/nervousness “over things I cannot control, such as wife driving or electrical”
Easily agitated
Easily frustrated
Easily angered
Anger toward accident, limitations, and lifestyle changes
Becomes emotionally upset with limitations and pain/symptoms
Becomes upset following EMDR sessions which surface feelings/emotions
Short tempered
Responses to situations are over exaggerated
Unable to concentrate with environmental stimuli
Short term memory deficit (i.e., forgets little things)
Requires reminders of appointment dates/times (i.e., forgot time of Life Care Plan assessment)
Forgetful (i.e., lost train of thought several times during Life Care Plan assessment)
Page 26 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Difficulty planning ahead, relies on wife
Difficulty with watching others perform work (i.e., “I feel less a man”)
High fear of re-injury (i.e., putting up Christmas lights)
Overly cautious with electrical and flames (i.e., increased anxiety/fears when children around electrical
products and open flames)
Very protective regarding family due to high fear/anxiety/paranoia of injury
Increased fear/anxiety when “I cannot control situation”
Limits children‟s play/activities due to increased anxiety/fear of injury (i.e., playing outside)
No longer attends bon fire with friends
No longer uses lighter fluid on charcoal when grilling out
No longer comfortable around electricity
Self conscious toward burn/graft site scars, affects community outings/social interaction
Bothersome with public stares, directness of inquiries, and comments
Doesn‟t leave house without wearing compression garments and long sleeves to cover scarring/disfigurement
Nightmares (i.e., burn accident, trauma, hallucinations, and family being injured)
Flashbacks with seeing flames or being around electrical equipment
Difficulty sleeping, doesn‟t sleep thru night, doesn‟t feel rested in morning
“My life is centered around this”
Sexual/erectile dysfunction
Psychosocial:
Lives with common law wife since 1999
Has two children ages 6 & 8 (daughters)
Lives in mobile home
Very sedentary lifestyle indoors
Limited recreational activities/outings to the spring, fall and winter
Activities limited due to fatigue/tiredness and reducing sun exposure
Relies on his wife for wound care/dressing changes
Wife provides assistance with ADL‟s
Requires assistance with home maintenance, yard work, finances, and errands/shopping
Wife does not work outside the home
Fearful of strangers reactions to his scars
Right hand dominant
Height: 6‟ inches
Weight: 205 lbs.
Educational/Vocational:
High school graduate 1998
Attended electrical classes in high school
Started working in 10th grade as electrical apprentice
Employed with same employer since 10th grade
Performed odd jobs on the side
Out of work since accident
Page 27 of 27
©2011, Shelene Giles · [email protected] · (828) 698-9486
Collaboration (communication with treating providers):
Medical questionnaires - forwarded to Dr. Fogert, Dr. Turner, Dr. Whetherford, Mr. Cary to address Mr. Burned‟s present
and future medical treatment.
Evaluation performed and discussions held with Dr. Burncare/Bernice Smith - Physician Assistant:
Dr. Burncare (Burn Specialist) noted: severe unstable scarring with chronic, open areas - attributed to scar
bands/contractures, delayed healing - immuno-compromised system, recommended long-term medical care, specialty
consultations, diagnostic studies, reconstructive surgeries/procedures, therapeutic evaluations/modalities, psychological
evaluations and counseling sessions (individual and family), medications for symptom management, lab work, long-term
scar management, and anticipated complications. Complications more likely than not in future: hypertrophic scarring,
pigmentation changes, altered sensations, tenderness at burn/graft sites, heat/cold intolerance, at higher risk for sunburn,
at higher risk for skin cancer (Basal cell carcinoma), allergic reactions/sensitivity to products
Dr. Turner‟s response: Diagnosis: S/P 40% TBSA
Current treatment plan: long-term medical care, specialty consultations, periodic diagnostic studies, reconstructive
surgeries/procedures as per Dr. Fogert, intermittent psychological evaluations and counseling sessions (individual and
family), long-term medications for symptom management, periodic lab work, long-term scar management, and anticipated
complications
Will Mr. Burned need ongoing/lifetime medical care related to burns? Yes
Will Mr. Burned need ongoing/lifetime medical care under specialty physicians? Yes
Dr. Whetherford‟s response: Diagnosis: diffuse pain to back/arms/abdomen 2nd
to scar formation with skin graft
placement.
Current treatment plan: long-term medical care, periodic diagnostic studies, psychological evaluations/ counseling
sessions (individual and family), long-term medications unknown duration, periodic lab work, anticipated complications
of drug dependency and constipation
Mr. Cary‟s response: Diagnosis of PTSD, major depressive episode, pain associated with both psychological factors and a
general medical condition
Current treatment plan: EMDR for PTSD, and cognitive behavioral therapy for depression and chronic pain management;
long term psychological care every two weeks; anticipated complications of adjustment to chronic pain, marital issues,
social issues, occupational issues, support issues, and economic issues