Embed Size (px)
Citation preview
Nurse practitioners as primary careproviders: Creating favorable practiceenvironments in New York Stateand Massachusetts
Lusine Poghosyan
Jingjing Shang
Jianfang Liu
Hermine Poghosyan
Nan Liu
Bobbie Berkowitz
Background: Policy makers, health care organizations, and health professionals are calling for the expansion of thenurse practitioner (NP) workforce in primary care to ensure access to high-quality, cost-effective care. However, todate, little is knownaboutNPpractice environments inprimary care settings andhow theymay affect the expansionofthis workforce and their practice.Purposes: The aims of this study were to investigate NP practice environments in two states, Massachusetts (MA) andNew York State (NY), and determine the impact of state and organization on NP practice environment.Methodology: A cross-sectional survey design was used. Practice environments were measured using the NursePractitioner Primary CareOrganizational ClimateQuestionnaire in terms ofNPYphysician relations, NPYadministrationrelations, support, NP role comprehension, and NP independent practice. In MA, 291 NPs were recruited from theMassachusetts Provider Database through mail surveys. In NY, 278 NPs were recruited from the NY NursePractitionerAssociationmembership list throughonline surveys.Datawere collected fromMaythroughSeptember2012.
Key words: Nurse practitioner, practice environment, primary care
Lusine Poghosyan, PhD, MPH, RN, is Assistant Professor, Columbia University School of Nursing, New York. E-mail: [email protected] Shang, PhD, RN, OCN, is Assistant Professor, Columbia University School of Nursing, New York.Jianfang Liu, PhD, MAS, is Data Analyst, Columbia University School of Nursing, New York.Hermine Poghosyan, PhD, MPH, is Assistant Professor, College of Nursing and Health Sciences, University of Massachusetts Boston.Nan Liu, PhD, is Assistant Professor, Department of Health Policy and Management Mailman School of Public Health, Columbia University,New York.Bobbie Berkowitz, PhD, RN, CNAA, FAAN, is Dean and Mary O’Neil Mundinger Professor, Columbia University School of Nursing, New York.
This study was funded by the Agency for Healthcare Research and Quality, and internal funding was received from the Columbia University Schoolof Nursing. This article was presented and supported in part by the 2012Michigan Symposium on Effectiveness and Implementation Science, sponsoredby the University of Michigan School of Nursing, on September 26, 2012. The study was approved by the Institutional Review Board of ColumbiaUniversity Medical Center.
The authors have disclosed that they have no significant relationship with, or financial interest in, any commercial companies pertaining to this article.
DOI: 10.1097/HMR.0000000000000010
Health Care Manage Rev, 2014, 00(0), 00Y00Copyright B 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins
Month & 2014 1
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Descriptive statistics were computed. Multivariate analysis of variance was conducted to investigate the effect of stateand organization type on NP practice environments.Findings: Nurse practitioners reported favorable relationships with physicians, deficiencies in their relationships withadministrators, and lack of support. Nurse practitioners from MA reported better practice environments. Nursepractitioners from hospital-affiliated practices perceived poorer practice environments than did NPs practicing inphysician offices and community health centers.Practice Implications:Optimal working relations with physicians and administration, access to resources, and clarity inNP role are necessary to create practice environments where NPs can function effectively as primary care providers.
Policy makers, health care organizations, and profes-sionals are calling for the redesign of our primary caresystem to increase efficiency, promote access, and
improve patient outcomes. There are noteworthy concernsthat the existing primary care system is overburdened andlacks the effectiveness necessary to meet patients’ needs(Margolius & Bodenheimer, 2010). This insufficiency isfueled by a critical shortage of primary care providers (PCPs)and the surging demand in services related to an aging pop-ulation and the epidemic of chronic diseases (Colwill,Cultice,& Kruse, 2008; Institute of Medicine, 2012; Sargen, Hooker,& Cooper, 2011).
In addition, with the passage of the Affordable CareAct (ACA), 32 million people will gain health insurance(Patient Protection and Affordable Care Act, 2010). Thischange in the health care system brings more attention toincreasing the capacity of primary care in the country toensure that patients will have access to timely care. Similarhealth reform initiatives have been enacted in Massachusetts(MA) in 2006, which led to an influx of about a half-millionMA residents into the health care system (Commonwealthof Massachusetts, 2006), which was already experiencing ashortage of primary care physicians (Massachusetts MedicalSociety, 2009). The full implementation of the ACA willlikely have similar consequences on a national scale foroverall primary care. To accommodate the demand, MApassed new legislation in 2008 to recognize nurse practi-tioners (NPs) as PCPs (Commonwealth of Massachusetts,2008). One need only extrapolate this example from thestate to a national level to understand not only the pro-jected impact of the ACA on care demand but also theimplications it has for the future of the NP workforce. Tomeet the demand, improve patient outcomes, and ensuretimely access and cost control, many have called for ex-panding the NP workforce in primary care and promotingtheir optimal practice (Institute ofMedicine, 2010; RANDHealth, 2009).
Nurse practitioners are educated to deliver primary careto both adult and pediatric populations in a variety of caresettings, including private practices, nurse-managed cen-ters, and community health centers among others (Esperat,Hanson-Turton, Richardson, Debisette, & Rupinta, 2012;
Hing, Hooker, & Ashman, 2011). They provide a broadspectrum of care from initial contact to follow-up care andproduce clinical outcomes comparable with those of phy-sicians (Laurant et al., 2009; Newhouse et al., 2011). Thenumber of NPs in general has increased significantly overthe past several years andwill continue to do so in the future(Pearson, 2012). Nationally, it is projected that theNPwork-force will increase by 130% from 2008 to 2025 (Auerbach,2012). However, many barriers such as state-level andpractice-level restrictions placed onNP practice affect theiroptimal utilization (Pearson, 2012; Poghosyan, Nannini,Stone, & Smaldone, 2013). Limited efforts have been de-voted to systematically investigate these barriers. This studyprovides an overview of NP practice environments in pri-mary care settings; compares NPs’ perceptions of their prac-tice environments between two states with and withouthealth reform, MA and New York State (NY), respectively;and determines the influence of state and organization typeon NP practice environments. Nurse practitioner scope ofpractice varies between the two states involved in this study.For example, whereas in MA, NPs can independently diag-nose and treat patients and collaborative agreement with aphysician is required only for prescriptive authority, in NY, acollaborative agreement with a physician is required for allthree aspects of NP practice: treatment, diagnosis, and pre-scribing authority (Pearson, 2012). In NY, it is also requiredto have the practice agreement on file with the state; there isno such requirement in MA. In addition to state-level vari-ations affecting NPs, organizational policies may also createchallenges, and to date, limited evidence exists about NPpractice environments. For primary care organizations shiftingtoward a larger NP workforce, creating and maintainingfavorable practice environments for NPs are necessary andcritical for promoting their successful practice and ability todeliver high-quality patient care.
Conceptual Framework
Organizational structures in the work settings impact em-ployee performance more than inherent personal char-acteristics do (Kanter, 1976). Kanter’s (1976) theory of
2 Health Care Management Review Month & 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

structural power is fundamental in studying organizationsand suggests that organizational structures can either im-pede or promote employee performance regardless of em-ployees’ personal tendencies. Kanter (1993) argues thatworkplace structures are important in shaping organiza-tional behaviors and relationships. They also can empoweremployees, providing access to information, support, andresources. Organizations that fail to enhance the perfor-mance of employees will see reduced productivity and ad-verse outcomes. Thus, it is necessary to study organizationsemploying NPs and the NP practice environments in thoseorganizations.
The quality of practice environments in health caresettings and their impact on provider, patient, and orga-nizational outcomes have been well studied in recent de-cades (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002;Benzer et al., 2011). Evidence is accumulating that healthcare organizations with poor practice environments withlack of support and resources for providers and staff, a lackof collegiality, and poor relationships between cliniciansand leadership tend to have poor quality of care, resulting inhigher rates of adverse patient outcomes (Clarke, 2006;Linzer et al., 2009). These inadequacies in practice en-vironments also lead to poor provider outcomes such asdiminished effectiveness, job dissatisfaction, and turnover(Brazil, Wakefield, Cloutier, Tennen, & Hall, 2010;De Milt, Fitzpatrick, & McNulty, 2011).
Although the impact of practice environments on pro-viders and the care they deliver is generally understood, theevidence about how to create quality practice environ-ments for primary care NPs is limited. This evidence isnecessary because of the projected significant increase inthe numbers of NP in their organizations and their con-tinuously evolving and expanding scope of practice. Someprimary care organizations may not be familiar with the NProle, and their practice environments might not be de-signed to support effective NP practice. Lack of under-standing about the NP role as a PCP may limit managers’abilities to create productive NP practice environments.Suboptimal NP practice environments have been reportedin several studies where NPs expressed dissatisfaction withintrapractice partnerships (De Milt et al., 2011; Schiestel,2007) and a lack of physician support (Lindeke, Jukkala, &Tanner, 2005;Weiland, 2008). Nurse practitioners also didnot receive the same level of support as physicians did todeliver the same services (Bryant-Lukosius,DiCenso, Browne,& Pinelli, 2004). EvenwhenNPs and physicians have similarPCP roles, in some organizations, physicians may have med-ical assistant support whereas NPs might not receive the sameassistance (Poghosyan, Nannini, Stone, et al., 2013). Theseare examples of suboptimal NP practice environments thatmay prevent NPs from effectively utilizing their skills andknowledge to provide high-quality care, leading to ineffi-ciencies in their organizations (Liu, Finkelstein,&Poghosyan,2013).
Methods
This study used a cross-sectional survey design to collect datafromprimary careNPs. TheNurse Practitioner PrimaryCareOrganizational Climate Questionnaire (NP-PCOCQ), aself-report survey instrument specifically designed for NPs(Poghosyan,Nannini, Finkelstein,Mason,&Shaffer, 2013),was used to measure NP practice environments. Using a4-point Likert scale ranging from 1 (strongly disagree) to 4(strongly agree), the questionnaire asks NPs to evaluate sev-eral aspects of their practice environments: (1) NPYphysicianrelations, in terms of assessing NP perceptions about thecollaboration and team work between NPs and physicians.The tool also captured other aspects of their collaboration,such as physicians seeking NP input and suggestions in caredelivery; (2) independent practice of NPs, in terms of NPs’perceptions about whether they were able to freely applytheir knowledge and skills to provide care and if their clinicscreate an environment where they can practice indepen-dently; (3) NPYadministration relations, in terms of admin-istrators being open toNPs’ ideas to improve care and takingNPconcerns seriously.Moreover,NPswere asked to comparethe relationships they had with the administrators to thatof the physicians; (4) comprehension and visibility of NProle, in terms of whether their role was well understood andvalued in their organizations; and (5) organizational supportand resources, in terms of the support that NPs had, such asstaff help. These aspects of practice environments are crit-ical for successful NP practice (Poghosyan,Nannini, Stone,et al., 2013).
In MA, NPs were recruited from the MassachusettsHealth Quality Partners (MHQP) Massachusetts ProviderDatabase (MPD). Each year, MHQP contacts clinics inMA and requests information about primary care physi-cians and specialists practicing in those sites who are listedas providers by at least one of the five major health plans.These plans together cover over 50% of MA’s commer-cially insured residents (MHQP, 2012). In 2011, MHQPalso requested information aboutNPs.No other database orexisting list in MA allows for the identification of NPspracticing in primary care settings and their role as anNP specialist or PCP. By using practice addresses extractedfrom theMPD, surveys were mailed to the 807 primary careNPs. Included with the survey was a cover letter andconsent form describing the study purpose, its voluntarynature, and the confidentiality of their responses. Nurse prac-titioners were asked to complete the questionnaire and re-turn it to the research team in a prepaid envelope. Followingthe Dillman (2007) guide for mailed surveys to encourageresponse rate, a postcard reminder and second survey weresent to nonrespondents. Two hundred ninety-oneNPs com-pleted and returned the surveys, yielding a response rateof 39%, which is a comparable response rate with thatof other nurse surveys (Aiken et al., 2010; Smith, 2008).Nurse practitioners practiced in 148 different clinics,
Primary Care Nurse Practitioner Practice Environment 3
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and the number of NPs from each clinic ranged from oneto seven.
In NY, NPs were recruited from the membership ofThe Nurse Practitioner Association (NPA). The NPAsent an e-mail invitation to 1,950 members who had adult,pediatric, family, gerontology, orwomen’s health specialtiesbecause these NPs are likely to practice in primary caresettings. The e-mail described the study and eligibility cri-teria for participation. It asked for NP participation andprovided the link to the online survey. As the NP practicelocation and the type of the organization could not bedetermined, an additional item was included to determineNP eligibility. Only NPs who self-identified as primary careNPswere prompted to take the survey.The surveywas createdin the professional version of SurveyMonkey. Second andthird e-mail reminders were sent after the initial e-mail in-vitation to encourage a high response rate (Dillman, 2007).Overall, 342 NPs accessed the survey, 278 completed thesurvey, and 64 NPs self-identified as not practicing in pri-mary care. The accurate response rate for the NY sample wasnot calculated because the number of targeted NPs prac-ticing in primary care could not be determined. Our e-mailinvitation might have reached NPs practicing in acute orother care settings, thusmaking them ineligible for the study.
Both the mail and the online surveys took about15 minutes to complete. Data collection took place fromMay through September 2012. There might be differencesin response rate and data quality when the mixed-modedata collection approach is used; however, the differencesareminor, and bothmodes yield comparable results (Beebe,Locke, Barnes, Davern, & Anderson, 2006; Deutskens, deRuyter, & Wetzels, 2006). The study was approved by theInstitutional Review Board of the Columbia UniversityMedical Center.
Data Analysis
Data from the mail survey in MA were entered into a da-tabase created in SPSSVersion 18 software (SPSS Inc., 2009).New York State data were extracted from SurveyMonkey.The data in both databases were investigated for missingvalues and outliers before merging. Descriptive statisticswere computed including means and frequencies for thedemographic and work characteristics of the respondents.For group comparison between theNY andMA states, t testfor continuous variables and chi-squares for categorical var-iables were used. The overall alpha level was set at .05 tocontrol Type I error throughout the study.
We coded the single items measuring various aspectsof practice environments by combining strongly agree andagree responses into one category and strongly disagree anddisagree responses into the other category to allow for dif-ferentiation of NPs’ favorable and less favorable responseson each item and calculated the proportions. We also com-
puted the mean scores on each of the five NP-PCOCQ di-mensions to measure NP practice environments.
The effects of potential confounding variables such asNPs’ age, gender, race (two levels: White vs. non-White),location of practice site (three levels: rural, suburban, andurban), and educational degree (three levels: master’s, doctorof nursing practice, and other) were considered and ana-lyzed to investigate the effect of state and organization typein which NPs practiced on their practice environments.Bivariate correlation analyses were run first and indicated nostatistically significant relationship between age, location ofpractice site, and the outcome measures, which were themean scores on each of the five NP-PCOCQ dimensionsmeasuring NP practice environments. Higher mean scoresindicate betterNP practice environment. Nurse practitioners’educational degree was included as the only confoundingvariable because of the correlations between NPs’ educa-tional degree, gender, and race. The vast majority of NPswere women (93.4%) and White (93%). Thus, we used a3 � 2 � 3 customized multivariate analysis of variance(MANOVA) to investigate the effect of state and orga-nization type after controlling for the main effect of NPs’educational degree. The fixed factors were state (two levels:MA vs. NY), organization types (three levels: physicianoffices, community health centers, and hospital-affiliatedpractices), and degree. The responses of NPs practicing inurgent care clinics, nurse-managed clinics, school-basedclinics, and in other nondefined settings were combinedinto the ‘‘other clinic’’ category given the small number ofpracticing NPs in each individual category. Nurse practi-tioners in the ‘‘other clinic’’ category comprised less than10%of the total sample andwere excluded from the3� 2� 3MANOVA and the corresponding univariate analysis andpost hoc analysis. Assumptions were checked before theanalysis, and post hoc multiple comparison with Bonferroni’scorrection was applied when an overall statistical signifi-cance was detected.
Findings
The demographic characteristics of NPs are presentedin Table 1. The mean age of NPs was about 51 years; 6.2%self-identified as male; 7% self-identified as non-White;and 45.4% of NPs practiced in physician offices, 22.9%practiced in community health centers, 22.3% practiced inprimary care clinics affiliated with hospitals, and 9.3% prac-ticed in other settings such as urgent care clinics and nurse-managed clinics. Compared with NPs in MA, NPs in NYwere older (52.3 vs. 49.3 years; p G .001) and more likely tobemale (9.8% vs. 2.9%; p G .001).MoreNPs inNYworkedin practices affiliated with hospitals (32.3% vs. 15.2%),whereas more NPs in MA worked in community healthcenters (30.1% vs. 12.8%). The demographic characteris-tics of NPs in our sample were comparable with those of
4 Health Care Management Review Month & 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

NPs in the 2008 National Sample Survey of RegisteredNurses (NSSRN) in terms of age, education, and other char-acteristics (Health Resources and Services Administration,2008). Almost 50% of NPs in the NSSRN were 50 yearsor older.
We investigated the NP responses on the individualsurvey items. Compared with physicians inMA, physiciansinNYwere more likely not to collaborate with NPs (19.4%vs. 5.2%; p = .014), not to ask them for suggestions (32.4%vs. 18.6%; p = .005), or not seek NP input when deliveringpatient care (38.1% vs. 22.3%; p = .013). More NPs in NY
than in MA disagreed that in their organizations they wereable to provide all patient care within their scope (18.7%vs. 4.5%; p G .001) or that their organizations created anenvironment whereNPs can practice independently (20.1%vs. 9.6%; p = .018). In MA, administrators were more likelyto share information equally with NPs and physicians, andNPs were more likely to be included in committees withintheir organization. More than half of the NPs (53.2%) inNY reported that administration does not share informa-tion equally withNPs and physicians. About 38%ofNPs inMA report this finding. Twenty-three percent of NPs in
Table 1
Demographic and work characteristics of the study participants
CharacteristicTotal(N = 564)
New York State(n = 278)
Massachusetts(n = 291) p
DemographicsAge (years) G.001Mean (SD) 50.58 (10.4) 52.3 (9.2) 49.34 (11.1)Range 24Y75 24Y75 26Y71
Sex, n (%) G.001Female 488 (93.8) 220 (90.2) 268 (97.1)Male 32 (6.2) 24 (9.8) 8 (2.9)
Race, n (%) .507White 477 (93.0) 219 (92.8) 258 (93.1)Non-White 36 (7.0) 17 (7.2) 19 (6.9)
Highest nursing degree, n (%) .006Master’s degree 463 (88.4) 205 (84.0) 258 (92.1)Doctor of nursing practice 24 (4.6) 18 (7.4) 6 (2.1)Other 37 (7.1) 21 (8.6) 16 (5.7)
Work characteristics, n (%)Years in the current position .001Less than 1 year 55 (10.5) 37 (15.2) 18 (6.4)1Y6 years 205 (39.2) 99 (40.7) 106 (37.9)More than 7 years 263 (50.3) 107 (44.0) 156 (55.7)
Average number of hours worked inthe past month
G.001
1Y20 64 (12.2) 43 (17.6) 21 (7.5)21Y40 295 (56.4) 104 (42.6) 191 (68.5)940 164 (31.3) 97 (39.8) 67 (24.0)
Number of other nurse practitionersin their practice
G.001
0 63 (12.1) 48 (19.7) 15 (5.4)1Y5 307 (58.9) 156 (63.9) 151 (54.5)6Y10 82 (15.7) 23 (9.4) 59 (21.3)910 69 (13.2) 17 (7.0) 52 (18.8)
Main practice site G.001Physician’s office 214 (45.4) 98 (50.3) 116 (42.0)Community health center 108 (22.9) 25 (12.8) 83 (30.1)Hospital-based clinic 105 (22.3) 63 (32.3) 42 (15.2)Other 44 (9.3) 9 (4.6) 35 (12.7)
Location of practice G.001Urban 248 (47.7) 84 (34.6) 164 (59.2)Suburban 214 (41.2) 111 (45.7) 103 (37.2)Rural 58 (11.2) 48 (19.8) 10 (3.6)
Primary Care Nurse Practitioner Practice Environment 5
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
MA and 36.3% in NY disagree with the statement that theadministration is open to NPs’ ideas to improve patientcare. Therewas no statistically significant difference betweenstates in terms of communication patterns between NPs andadministration. InNY, 40% of NPs reported that their role isnot understood and 31.7% did not feel valued by theirorganizations. About 21%ofNPs inNY and 6.5%ofNPs inMA reported lack of resources. There was no statisticallysignificant difference between the states in terms of supportfor care management between NPs and physicians.
Three-way customized MANOVA compared the meanscores on eachNPpractice environment dimension betweenMA and NY, controlling for the main effect of NPs’ edu-cational level. The multivariate results indicated differenceinNPpractice environment betweenMAandNY(Wilks1=.918,F=7.37, pG .05), withmedium to large effect size ()’2 =.082). Nurse practitioner practice environment was alsodifferent among the three types of health care organizations(Wilks’ 1 = .942, F = 2.52, p G .05), with small to medium
effect size ()’2 = .030). There was no significant multi-variate interaction effect between state and organizationtype. The main effect of the confounding variable, NPs’educational level, was significant (Wilks 1 = .951, F= 2.10,p G .05), with small to medium effect size ()’2 = .025).
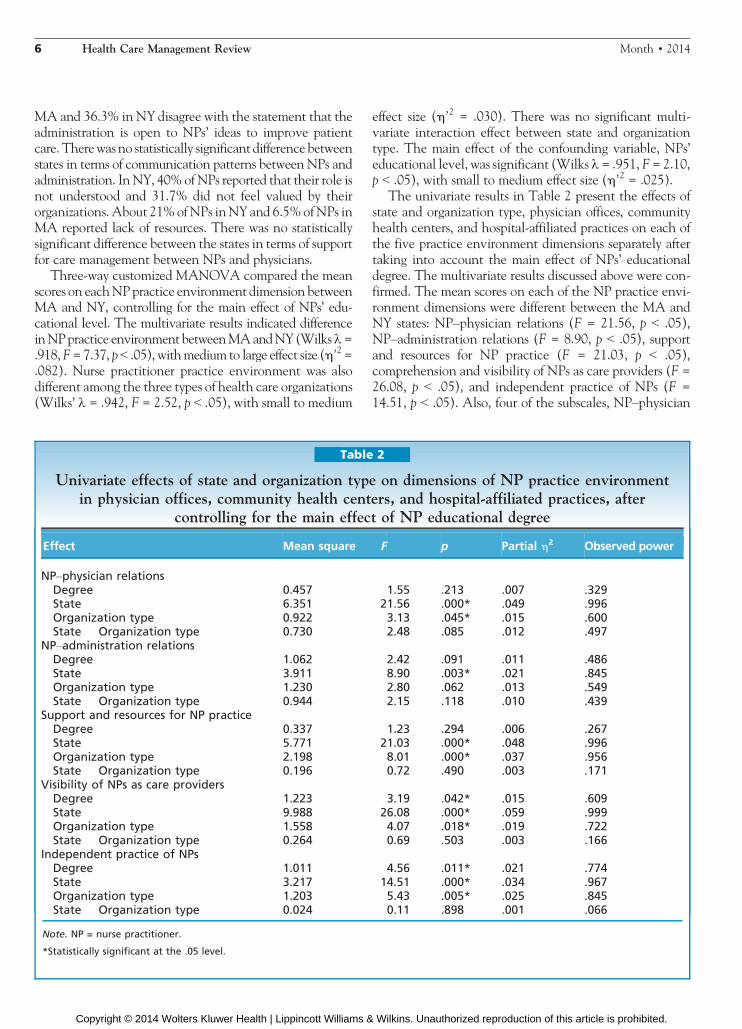
The univariate results in Table 2 present the effects ofstate and organization type, physician offices, communityhealth centers, and hospital-affiliated practices on each ofthe five practice environment dimensions separately aftertaking into account the main effect of NPs’ educationaldegree. The multivariate results discussed above were con-firmed. The mean scores on each of the NP practice envi-ronment dimensions were different between the MA andNY states: NPYphysician relations (F = 21.56, p G .05),NPYadministration relations (F = 8.90, p G .05), supportand resources for NP practice (F = 21.03, p G .05),comprehension and visibility of NPs as care providers (F =26.08, p G .05), and independent practice of NPs (F =14.51, p G .05). Also, four of the subscales, NPYphysician
Table 2
Univariate effects of state and organization type on dimensions of NP practice environmentin physician offices, community health centers, and hospital-affiliated practices, after
controlling for the main effect of NP educational degree
Effect Mean square F p Partial )2 Observed power
NPYphysician relationsDegree 0.457 1.55 .213 .007 .329State 6.351 21.56 .000* .049 .996Organization type 0.922 3.13 .045* .015 .600State � Organization type 0.730 2.48 .085 .012 .497
NPYadministration relationsDegree 1.062 2.42 .091 .011 .486State 3.911 8.90 .003* .021 .845Organization type 1.230 2.80 .062 .013 .549State � Organization type 0.944 2.15 .118 .010 .439
Support and resources for NP practiceDegree 0.337 1.23 .294 .006 .267State 5.771 21.03 .000* .048 .996Organization type 2.198 8.01 .000* .037 .956State � Organization type 0.196 0.72 .490 .003 .171
Visibility of NPs as care providersDegree 1.223 3.19 .042* .015 .609State 9.988 26.08 .000* .059 .999Organization type 1.558 4.07 .018* .019 .722State � Organization type 0.264 0.69 .503 .003 .166
Independent practice of NPsDegree 1.011 4.56 .011* .021 .774State 3.217 14.51 .000* .034 .967Organization type 1.203 5.43 .005* .025 .845State � Organization type 0.024 0.11 .898 .001 .066
Note. NP = nurse practitioner.
*Statistically significant at the .05 level.
6 Health Care Management Review Month & 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
relations (F = 3.13, p G .05), support and resources for NPpractice (F= 8.01, p G .05), comprehension and visibility ofNPs as care providers (F = 4.07, p G .05), and independentpractice of NPs (F = 5.43, p G .05), had different scores inthe three types of health care organizations. None of theunivariate interaction effects on the five subscales were sta-tistically significant, which was consistent with the multi-variate results.
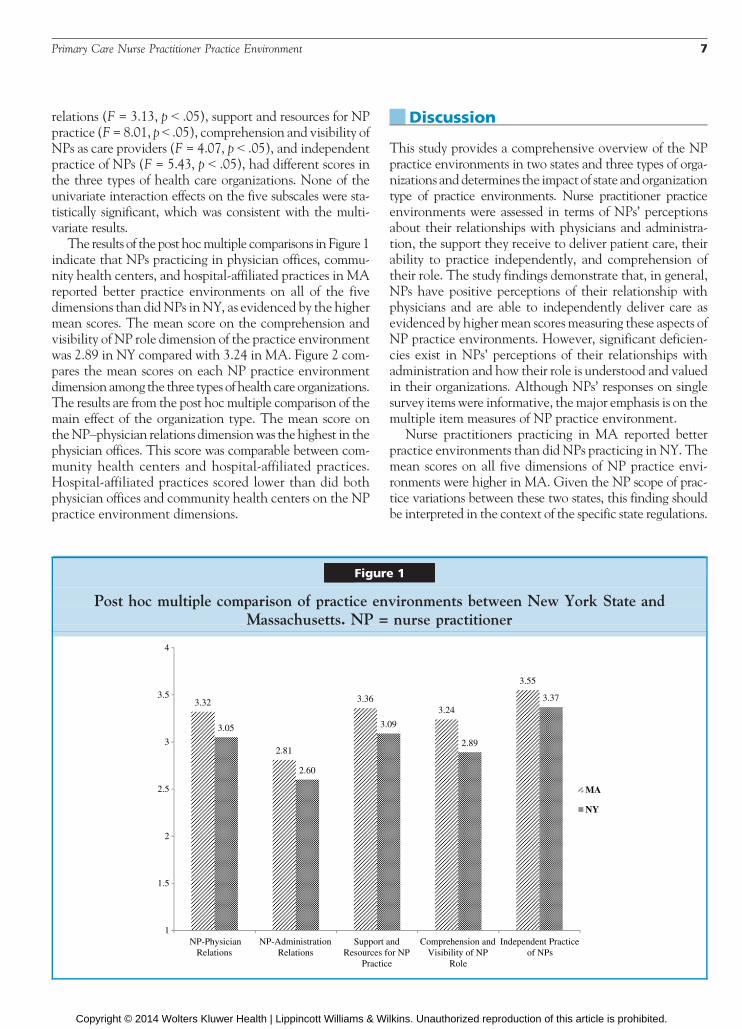
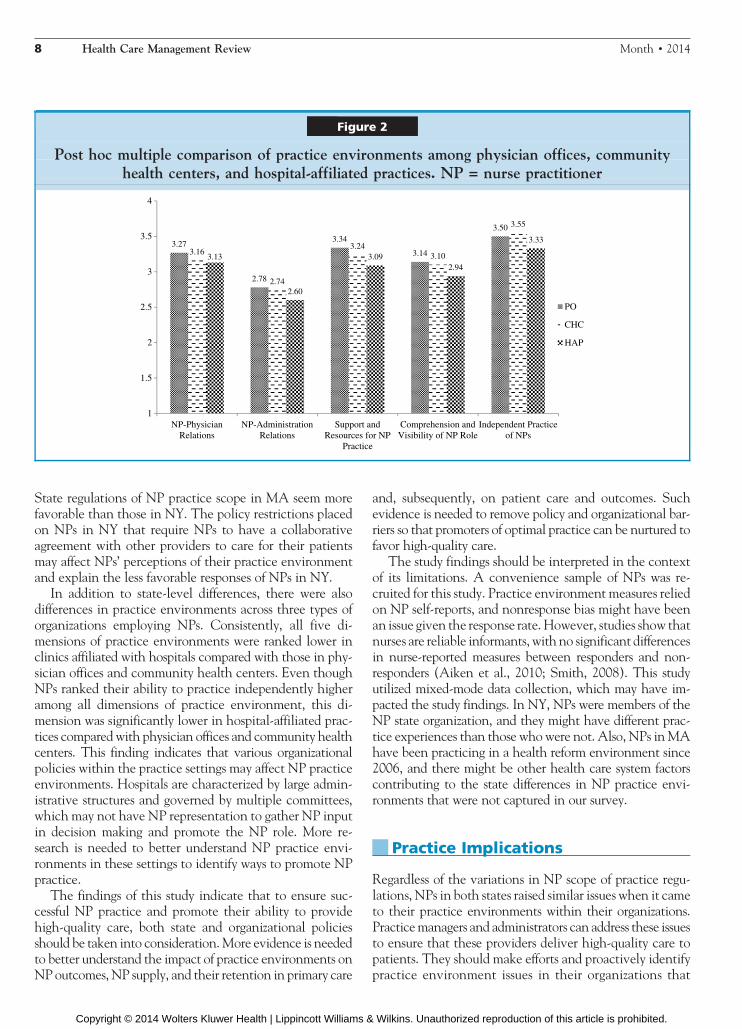
The results of the post hocmultiple comparisons in Figure 1indicate that NPs practicing in physician offices, commu-nity health centers, and hospital-affiliated practices in MAreported better practice environments on all of the fivedimensions than didNPs inNY, as evidenced by the highermean scores. The mean score on the comprehension andvisibility of NP role dimension of the practice environmentwas 2.89 in NY compared with 3.24 in MA. Figure 2 com-pares the mean scores on each NP practice environmentdimension among the three types of health care organizations.The results are from the post hoc multiple comparison of themain effect of the organization type. The mean score ontheNPYphysician relations dimensionwas the highest in thephysician offices. This score was comparable between com-munity health centers and hospital-affiliated practices.Hospital-affiliated practices scored lower than did bothphysician offices and community health centers on the NPpractice environment dimensions.
Discussion
This study provides a comprehensive overview of the NPpractice environments in two states and three types of orga-nizations and determines the impact of state and organizationtype of practice environments. Nurse practitioner practiceenvironments were assessed in terms of NPs’ perceptionsabout their relationships with physicians and administra-tion, the support they receive to deliver patient care, theirability to practice independently, and comprehension oftheir role. The study findings demonstrate that, in general,NPs have positive perceptions of their relationship withphysicians and are able to independently deliver care asevidenced by highermean scoresmeasuring these aspects ofNP practice environments. However, significant deficien-cies exist in NPs’ perceptions of their relationships withadministration and how their role is understood and valuedin their organizations. Although NPs’ responses on singlesurvey items were informative, themajor emphasis is on themultiple item measures of NP practice environment.
Nurse practitioners practicing in MA reported betterpractice environments than did NPs practicing in NY. Themean scores on all five dimensions of NP practice envi-ronments were higher in MA. Given the NP scope of prac-tice variations between these two states, this finding shouldbe interpreted in the context of the specific state regulations.
Figure 1
Post hoc multiple comparison of practice environments between New York State andMassachusetts. NP = nurse practitioner
Primary Care Nurse Practitioner Practice Environment 7
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
State regulations of NP practice scope in MA seem morefavorable than those in NY. The policy restrictions placedon NPs in NY that require NPs to have a collaborativeagreement with other providers to care for their patientsmay affect NPs’ perceptions of their practice environmentand explain the less favorable responses of NPs in NY.
In addition to state-level differences, there were alsodifferences in practice environments across three types oforganizations employing NPs. Consistently, all five di-mensions of practice environments were ranked lower inclinics affiliated with hospitals compared with those in phy-sician offices and community health centers. Even thoughNPs ranked their ability to practice independently higheramong all dimensions of practice environment, this di-mension was significantly lower in hospital-affiliated prac-tices compared with physician offices and community healthcenters. This finding indicates that various organizationalpolicies within the practice settings may affect NP practiceenvironments. Hospitals are characterized by large admin-istrative structures and governed by multiple committees,which may not have NP representation to gather NP inputin decision making and promote the NP role. More re-search is needed to better understand NP practice envi-ronments in these settings to identify ways to promote NPpractice.
The findings of this study indicate that to ensure suc-cessful NP practice and promote their ability to providehigh-quality care, both state and organizational policiesshould be taken into consideration.More evidence is neededto better understand the impact of practice environments onNPoutcomes, NP supply, and their retention in primary care
and, subsequently, on patient care and outcomes. Suchevidence is needed to remove policy and organizational bar-riers so that promoters of optimal practice can be nurtured tofavor high-quality care.
The study findings should be interpreted in the contextof its limitations. A convenience sample of NPs was re-cruited for this study. Practice environment measures reliedon NP self-reports, and nonresponse bias might have beenan issue given the response rate. However, studies show thatnurses are reliable informants, with no significant differencesin nurse-reported measures between responders and non-responders (Aiken et al., 2010; Smith, 2008). This studyutilized mixed-mode data collection, which may have im-pacted the study findings. In NY, NPs were members of theNP state organization, and they might have different prac-tice experiences than those who were not. Also, NPs inMAhave been practicing in a health reform environment since2006, and there might be other health care system factorscontributing to the state differences in NP practice envi-ronments that were not captured in our survey.
Practice Implications
Regardless of the variations in NP scope of practice regu-lations, NPs in both states raised similar issues when it cameto their practice environments within their organizations.Practicemanagers and administrators can address these issuesto ensure that these providers deliver high-quality care topatients. They should make efforts and proactively identifypractice environment issues in their organizations that
Figure 2
Post hoc multiple comparison of practice environments among physician offices, communityhealth centers, and hospital-affiliated practices. NP = nurse practitioner
8 Health Care Management Review Month & 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

affect NPs and create infrastructures that support NPpractice and allow them to practice to the fullest extent oftheir scope. Optimal utilization of all PCPs within orga-nizations will ensure better patient care, improve patientoutcomes, and maintain safety.
Nurse practitioners face challenges in significant aspectsof their practice environments, such as clarity of the NProle in their organization and the relationship with admin-istration. Kanter (1993) states that organizations can em-power employees by placing them in positions that highlightthe value of their role and its relevance to the organization.Managers should make efforts to establish a clear NP rolewithin their organization and promote the visibility of theNP role. Even though NPs’ perceptions about their rela-tionshipwith physicians seem satisfactory, the teamwork andcollaboration aspects rather than physicians seeking NPinput and the lack of clarity in NP role in the organizationsmay challenge effective teamwork between these differenttypes of PCPs.
Managers should focus on improving the relationshipbetween NPs and administrators and opening the channelsof communication. This will help to create mechanisms forinformation dissemination and will ensure that providershave necessary information to make care decisions, espe-cially when NPs report that administration is not open toNP ideas to improve patient care. Having access to infor-mation and resources empowers employees (Kanter, 1993).In addition, NP underrepresentation in their organization’sdecision-making committees may further their perceptionof being less visible.Oneway to successfully integrateNPs isto provide avenues for NPs to become involved in orga-nizational governance, such as being members of committees.
Managers should create infrastructures to provide sup-port for NPs. Having adequate support will promote theeffective use of NPs’ advanced skills and knowledge. Lackof adequate use of their skills in their organizations increasescost and decreases the efficiency of care (Liu et al., 2013).Furthermore, supportive practice environments are neces-sary for the implementation of new primary care models,suchasPatientCenteredMedical,which fostermultidisciplinaryteam-based care homes Patient-Centered Medical Home(PCMH) (National Committee for Quality Assurance, 2011).
Nurse practitioner responses indicated less favorablepractice environments in hospital-affiliated practices com-pared with physician offices and community health cen-ters, which may lead to future difficulties in recruiting andretaining NPs in this type of practices. With the expand-ing of NP roles and the increasing care demand, hospitaladministrators should consider modification of the admin-istrative structures to involve NPs in decision-making pro-cesses. In addition, a regular assessment of NPs’ needs willhelp to identify concerns and deficiencies in hospital-affiliatedclinics. By doing this, administrators would be actively in-volved in a dynamic understanding of NP practice in theirorganizations and be poised to address problems on a timely
manner. This would enable them to provide a healthy prac-tice environment for a more effective expansion of the NPworkforce in their organizations and ultimately improvepatient care.
Acknowledgments
We thank NPA and the New York and MassachusettsHealth Quality Partners for assisting with the data col-lection.We also thank KristineM. Kulage, MA, for editingthe manuscript.
References
Aiken, L. H., Clarke, S. P., Sloane, D.M., Sochalski, J., & Silber,J. H. (2002). Hospital nurse staffing and patient mortality,nurse burnout, and job dissatisfaction. Journal of the AmericanMedical Association, 288(16), 1987Y1993. doi: 10.1001/jama.288.16.1987
Aiken, L.H. S., Douglas,M.,Cimiotti, J. P., Clarke, S. P., Flynn, L.,Seago, J. A., I Smith, H. L. (2010). Implications of theCalifornia nurse staffing mandate for other states. Health Ser-vices Research, 45(4), 904Y921. doi: 10.1111/j.1475-6773.2010.01114.x
Auerbach, D. I. (2012). Will the NP workforce grow in thefuture? New forecasts and implications for healthcare delivery.Medical Care, 50(7), 606Y610. doi: 10.1097/MLR.0b013e318249d6e7
Beebe, T. J., Locke, G. R., Barnes, S. A., Davern, M. E., &Anderson, K. J. (2006). Mixing web and mail methods in asurvey of physicians. Health Services Research, 42(3 Pt. 1),1219Y1234.
Benzer, J. K., Young,G., Stolzmann, K.,Osatuke, K.,Meterko,M.,Caso, A., I Mohr, D. C. (2011). The relationship betweenorganizational climate and quality of chronic disease manage-ment. Health Services Research, 46(3), 691Y711.
Brazil, K., Wakefield, D., Cloutier, M., Tennen, H., & Hall, C.(2010). Organizational culture predicts job satisfaction andperceived clinical effectiveness in pediatric primary care prac-tices.HealthCareManagement Review, 35(4), 365Y371. doi: 10.1097/HMR.0b013e3181edd957
Bryant-Lukosius, D., DiCenso, A., Browne, G., & Pinelli, J.(2004).Advanced practice nursing roles:Development, imple-mentation and evaluation. Journal of Advanced Nursing, 48(5),519Y529. doi: 10.1111/j.1365-2648.2004.03234.x
Clarke, S. P. (2006). The relationship between safety climate andsafety performance: A meta-analytic review. Journal of Occu-pational Health Psychology, 11, 315Y327.
Colwill, J. M., Cultice, J. M., & Kruse, R. L. (2008). Will gen-eralist physician supply meet demands of an increasing andaging population? Health Affairs, 27(3), w232Yw241.
Commonwealth ofMassachusetts. (2006). Chapter 58 of theActsof 2006: An act providing access to affordable, quality, ac-countable health care. RetrievedMarch 25, 2013, from http://www.mass.gov/legis/laws/seslaw06/sl060058.htm
Commonwealth of Massachusetts. (2008). Chapter 305 of theActs of 2008: An act to promote cost containment, trans-parency and efficiency in the delivery of quality health care.Retrieved August 10, 2012, from http://www.mass.gov/legis/laws/seslaw08/sl080305.htm
Primary Care Nurse Practitioner Practice Environment 9
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

De Milt, D. G., Fitzpatrick, J. J., & McNulty, R. (2011). Nursepractitioners’ job satisfaction and intent to leave currentpositions, the nursing profession, and the nurse practitionerrole as a direct care provider.The Journal of American Academyof Nurse Practitioners, 23(1), 42Y50. doi: 10.1111/j.1745-7599.2010.00570.x
Deutskens, E., de Ruyter, K., & Wetzels, M. (2006). An assess-ment of equivalence between online and mail surveys in ser-vice research. Journal of Service Research, 8(4), 346Y355.
Dillman, D. A. (2007). Mail and Internet surveys: The tailoreddesign method (2nd ed.). New York, NY: John Wiley & SonsInc.
Esperat,M.C.R.,Hanson-Turton, T., Richardson,M., Debisette,A. T., & Rupinta, C. (2012). Nurse-managed health centers:Safety-net care through advanced nursing practice. Nurse-managed health centers as safety nets. Journal of the AmericanAcademy of Nurse Practitioners, 24(1), 24Y31. doi: 10.1111/j.1745-7599.2011.00677.x
Health Resources and Services Administration. (2008). Nationalsample survey of registered nurses. Retrieved March 1, 2012,from http://datawarehouse.hrsa.gov/nursingsurvey.aspx
Hing, E., Hooker, R. S., & Ashman, J. J. (2011). Primary healthcare in community health centers and comparison with office-based practice. Journal of Community Health, 36(3), 406Y413.doi: 10.1007/s10900-010-9322-x
Institute of Medicine. (2010). The future of nursing: Leadingchange, advancing health. Retrieved from http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-Change-Advancing-Health.aspx
Institute of Medicine. (2012). Living well with chronic illness: Acall for public health action. Retrieved February 1, 2013, fromhttp://iom.edu/Reports/2012/Living-Well-with-Chronic-Illness.aspx
Kanter, R. M. (1976). The impact of hierarchical structures onthe work behavior of women and men. Social Problems, 23(4),415Y430.
Kanter, R.M. (1993).Menandwomen of the corporation (Second ed.).New York, NY: Basic Books.
Laurant, M., Reeves, D., Hermens, R., Braspenning, J., Grol, R.,& Sibbald, B. (2009). Substitution of doctors by nurses inprimary care: Cochrane Review. Cochrane Database of Sys-tematic Reviews, 1, 1Y39.
Lindeke, L., Jukkala, A., &Tanner,M. (2005). Perceived barriersto nurse practitioner practice in rural settings. Journal of RuralHealth, 21(2), 178Y181. doi: 10.1111/j.1748-0361.2005.tb00079.x
Linzer,M.,Manwell, L.,Williams, E. S., Bobula, J.A., Brown,R. L.,Varkey, A. B., I Schwartz, M. D. (2009). Working condi-tions in primary care: Physician reactions and care quality.Annals of Internal Medicine, 151(1), 28Y36.
Liu, N., Finkelstein, S. R., & Poghosyan, L. (2013). A newmodelfor nurse practitioner utilization in primary care: Increasedefficiency and implications. Health Care Management andReview, 39(1), 10Y20.
Margolius, D., & Bodenheimer, T. (2010). Transforming primary
care: From past practice to the practice of the future. HealthAffairs, 29(5), 779Y784. doi: 10.1377/hlthaff.2010.0045
Massachusetts Health Quality Partners. (2012). Quality in-sights: Clinical quality in primary care, 2011. RetrievedDecember 10, 2012, from http://www.mhqp.org/quality/clinical/cqMeasInfo.asp?nav=032400&MeasureID=33
Massachusetts Medical Society. (2009). Physician workforcestudy. Retrieved January 10, 2012, from http://www.massmed.org/AM/Template.cfm?Section=Home6&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=31511
National Committee for Quality Assurance. (2011). Patient-centered medical home. Retrieved May 16, 2012, from http://www.ncqa.org/tabid/631/default.aspx
Newhouse, R. P., Stanik-Hutt, J., White, K. M., Johantgen, M.,Bass, E. B., Zangaro, G., I Weiner, J. P. (2011). Advancedpractice nurse outcomes 1990Y2008: A systematic review.Nurs-ing Economics, 29(5), 1Y22. doi: 10.1234/12345678
Patient Protection and Affordable Care Act. (2010, March 23).Act of 2010. Public Law 111-148, 124 Stat. 119 thru 124 Stat.1025.
Pearson, L. P. (2012). The 2012 Pearson Report: A NationalOverview of Nurse Practitioner Legislation andHealth Care Issues.Retrieved March 12, 2013, from www.webnponline.com
Poghosyan, L., Nannini, A., Finkelstein, S. R., Mason, E., &Shaffer, J. (2013). Development and psychometric testing ofthe Nurse Practitioner Primary Care Organizational ClimateQuestionnaire (NP-PCOCQ). Nursing Research, 62(5), 325Y334.
Poghosyan, L., Nannini, A., Stone, P., & Smaldone, A. (2013).Nurse practitioner organizational climate in primary caresettings: Implications for professional practice. Journal of Pro-fessional Nursing, 29(6), 338Y349.
RAND Health. (2009). Controlling health care costs inMassachusetts: An analysis of options. Retrieved February 5,2011, from http://www.rand.org/pubs/technical_reports/2009/RAND_TR733.pdf
Sargen, M., Hooker, R. S., & Cooper, R. A. (2011). Gaps in thesupply of physicians, advance practice nurses, and physicianassistants. Journal of the American College of Surgeons, 212(6),991Y999. doi: 10.1016/j.jamcollsurg.2011.03.005
Schiestel, C. (2007). Job satisfaction among Arizona adult nursepractitioners. Journal of the American Academy of Nurse Prac-titioners, 19(1), 30Y34. doi: 10.1111/j.1745-7599.2006.00187.x
Smith, H. L. (2008). Double sample to minimize bias due to non-response in a mail survey. In A. Ruiz-Gazen, P. Guilbert, D.Haziza, & Y. Tille (Eds.), Survey methods: Applications tolongitudinal studies, to health, to electoral studies and to studies indeveloping countries (pp. 334Y339). Paris, France: Dunod.
SPSS Inc. (2009). PASW statistics for windows, version 18.0.Chicago, IL: SPSS Inc.
Weiland, S. A. (2008). Reflections on independence in nursepractitioner practice. Journal of the American Academy ofNurse Practitioners, 20(7), 345Y352. doi: 10.1111/j.1745-7599.2008.00330.x
10 Health Care Management Review Month & 2014
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.





























