Embed Size (px)
Citation preview
Nursing Strategy for West London Mental Health Trust
Contents Page 1. Introduction 4 2. Nursing at West London Mental Health Trust 4 - 6 Figure 1: WLMHT Nursing Strategy 5 3. Leadership for Safe Care 6 – 8 Table 1: Leadership for Safe Care 7 – 8 4. Service User Experience and Recovery 8 – 10 Table 2: Service User Experience and Recovery 9 – 10 5. Recruit, Retain and Value High Quality Nurses 10 – 13 Table 3: Recruit, Retain and Value High Quality Nurses 12 – 13 6. Quality and Innovation in Nursing Practice 14 – 16 Table 4: Quality and Innovation in Nursing Practice 15 – 16 7. Implementation of the Nursing Strategy 17 8. Where to from here? 17
2
Foreword West London Mental Health Trust’s Strategy for Nursing has been written by nurses working in all areas of the Trust. It has drawn on the views of people using our services and carers, the views of nurses and colleagues from other professions and our local universities. People using our services want their contact with nurses to make them feel safe, cared for, respected and involved. They want to know that nurses are there for them unconditionally. They want to be assured that nurses’ actions will be in their best interests and will help them improve, recover to their full potential, feel in control of their lives and live life to the full. They want nurses who can hold onto hope when theirs is lost and who can inspire hope for a better future. The central aim of the Trust’s Nursing Strategy is to achieve a positive experience for people using our services, and in turn for the nurses providing them. There are four themed areas of work that describe what we will achieve and how we will achieve it. The ability to provide consistent high quality nursing care requires nurses to have a broad range and depth of professional nursing knowledge and skills. However, nurses also need to suspend this ‘expertise’, to enable the person-in-care to be the expert in their own experience, to make their own decisions, and to learn from their own mistakes. With this in mind, I am pleased to introduce the 2010-13 vision for nursing which outlines an ambitious programme of improvement for the next three years. All nursing staff have an important part to play in improving patient experience. There are many examples of good practice that already exist and some of these are used to illustrate innovations in practice and quality care. I would like to thank all of the people who have contributed to this strategy. I look forward to working with colleagues throughout the Trust and the local health economy to deliver on it to ensure that the experience of people using our services is a positive one. Steve Trenchard Executive Director of Nursing and Patient Experience
3
1. Introduction
1.1 The Nursing Strategy describes the nursing contribution to the care of people in the communities served by West London Mental Health NHS Trust (WLMHT) and has been written for both registered nurses and health care assistants who work within the organisation. It has been developed utilising information from a variety of sources including: feedback from nursing staff at the 3rd Annual Nursing Conference, focus groups with carers, service users and Trust staff; Chief Nursing Officer’s Mental Health Nursing Report (2005); The Ten Essential Shared Capabilities (2005); Confidence in Caring (2007); New Horizons (2009); Quality Roadmap for Nursing (2010); Workforce for London – A Strategic Framework (2008) and Front Line Care (2010). Links to these documents are available in the appendices for those that wish to know more about them.
1.2 The key messages from the consultation are summarised below and will be
incorporated into the overall thinking and outcomes of the strategy:
• Good mental health practice is fundamentally about the quality of the relationship between the nurse and the person in care. Relationships should be based on compassion, hope, mutual self regard and on optimistic attitudes that support an individual’s personal recovery. WLMHT’s vision and values sit at the heart of this.
• Nurses should be providing leadership to design and implement service improvements and innovation.
• Nurses should promote recovery and well-being to prevent the experience of ‘mental illnesses’ being seen as a list of symptoms and/or problems that the person has little control over.
• Recovery is about seeing the individual in their totality and the goal of effective nursing practice is to support the person’s aspirations, goals and wishes.
1.3 The strategy will be implemented and formally reviewed on a quarterly and annual
basis via actions which link to the Trusts priorities and values. As such it will be a dynamic and evolving document that will provide the strategic framework through which nurses and health care assistants can increase their confidence, knowledge and skills thus providing high quality care to people who use our services and their supporters of recovery and carers.
2. Nursing at West London Mental Health Trust 2.1 West London Mental Health NHS Trust is proud of its nursing workforce because of
the commitment, flexibility and care which is shown to the people of West London who receive access and use services across 24 hours every day of the year. Two thousand five hundred nurses (1500 registered, 800 unregistered and 333 students) work across all care settings and are in an influential position to effect the experience of service users and their families and/or carers. The diversity and richness of the communities and services provided to West London shape the profile of nursing roles. And yet, paradoxically nurses do not always recognise how they can influence change and have consequently reported feeling that their voice is unheard which is likely to lead to disengagement and disempowerment. This isn’t just a local but a national phenomenon and is linked into the image of the nursing
4
profession as a whole. However, in West London it is sadly commonplace to hear nurses say they do not feel valued, or that their professional views are not heard.
2.2 As a mental health organisation with a large bed base (circa 1000 beds) and with
specialist forensic services (low, medium and high secure) there may be an association between the reliance on the Mental Health Act and the oversight of the Act by consultant psychiatrists which has resulted in the dominance of more traditional ‘medical approaches’ to care and treatment. Whilst this might be contentious to some, there are some local views which support this notion, and which might have led to a deskilling and a lowering of expectation of what nurses can deliver in practice.
2.3 Equally, nursing cannot call cry to being disempowered within the legal framework of
the Mental Health Act when there is much they can and should be doing to promote peoples’ rights and recovery. The vision for recovery orientated practice, with easy access to psychological and social interventions, drawing on more preventative and well-being based models of care, has been set out in New Horizons and is reflected throughout this strategy.
2.4 As such we expect and will support nurses to be confident and to recognise the
opportunities open to them if the aims and aspirations of service users, as reflected through New Horizons, are to be fully realised. All the more reason that this strategy be seen as the central vehicle for the introduction of focused and sustained action to support, develop, and energise the whole workforce to support nurses in their work at the heart of direct care provision. Equally we recognise the significance of underpinning our practice by evidence and proven research which we will imbue throughout our strategy.
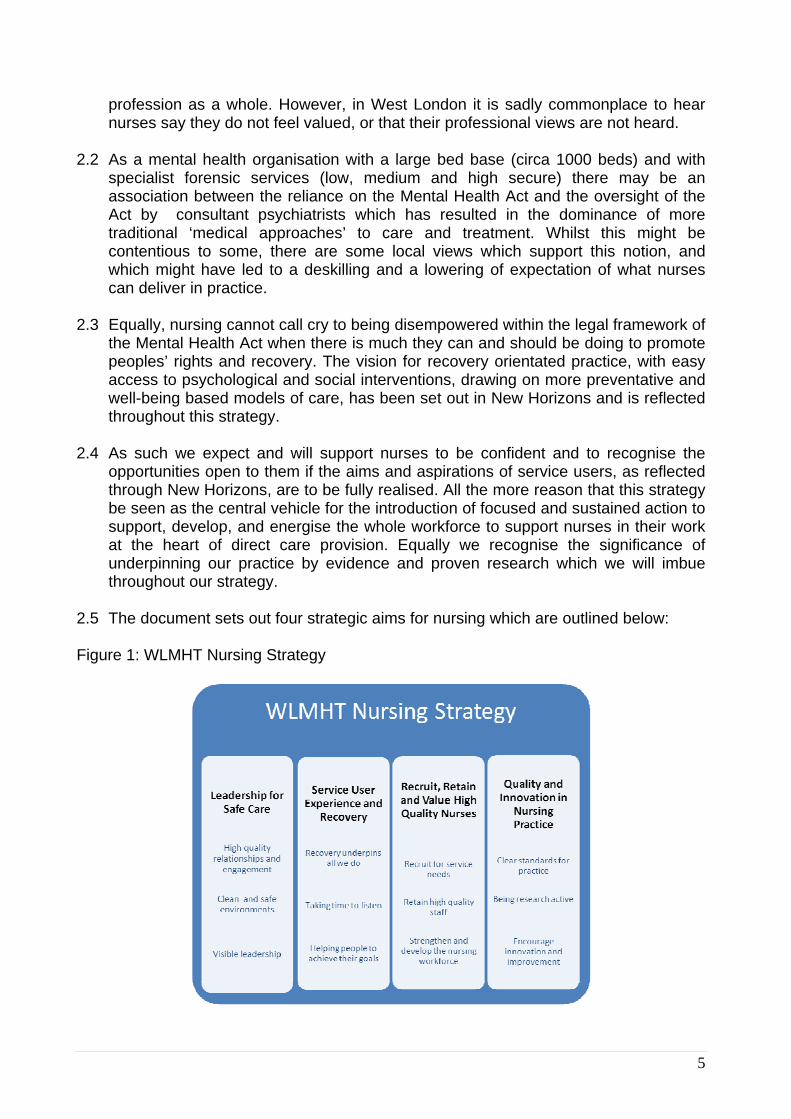
2.5 The document sets out four strategic aims for nursing which are outlined below: Figure 1: WLMHT Nursing Strategy
5
2.6 The strategy supports a repositioning of nursing ideas and practices that might be as unsettling for some as it is exciting for others. Instead of being the passive recipients of knowledge from other professions, nurses now need to seize the initiative for themselves. Senior nurses believe that other nurses in the Trust can rise to this challenge. After all, if nurses can develop their own strategy then they ought also to be engaged in delivering it in partnership with service users as the key focus of their activity.
2.7 The success of the outcomes described in this strategy will rise or fall on the support
it is afforded not only by the organisation but by nurses and other stakeholders throughout the healthcare system.
3. Leadership for Safe Care
What makes this a priority for us? 3.1 It is well recognised that many people receiving in-patient mental health care report
feeling unsafe. Nurses have a duty of care to ensure the safety and well-being of service users and this includes making sure they provide the highest quality care and that others in the multi-disciplinary team do the same. Where a nurse observes sub-standard practice this must be raised with the appropriate person and where necessary, challenged immediately.
3.2 Nurses should place safety and the service user experience at the centre of all they
do. As a component of quality, safety focuses specifically on the experience of people using services, the effectiveness of treatments being offered and the ability of the person to maintain their own safety through positive approaches to risk taking.
3.3 Nurses are central to a patient’s experience of safe care. This focus on ‘safety’
should be reflected in the manner in which nurse-patient relationships are transacted, through the formulation of care plans, risk assessments and by purposeful nursing contribution to the provision of effective psycho-social care. Ensuring a consistent approach to development of such relationships requires nurses to provide visible leadership at all levels and stages of the care pathway.
3.4 All nurses will at some stage of the day act in a leadership role. Whether it be
discussing a care plan, showing a person around the ward for the first time, providing education about psychosis, signing off a student’s placement assessment or leading an MDT discussion. All of these activities require a style of leadership that is engaging, credible, demonstrates integrity and the ability to ‘live’ the values of the NMC Code of Conduct.
3.5 Leadership for safe care enshrines the need to meet one of the most basic of
human needs. Following closely behind the need for air, water, food and sleep, the safety needs such as safe environments, safe relationships and being safe from harm (such as harassment, bullying and victimisation) are essential pre-requisites for a person’s recovery. Leadership for safe care also encompasses the skilled nursing interventions of ‘observations’ and ‘physical interventions’ (i.e. restraint)
6
which should be used minimally and only when a person has become unable to maintain their own safety or because they pose a risk to the safety of others.
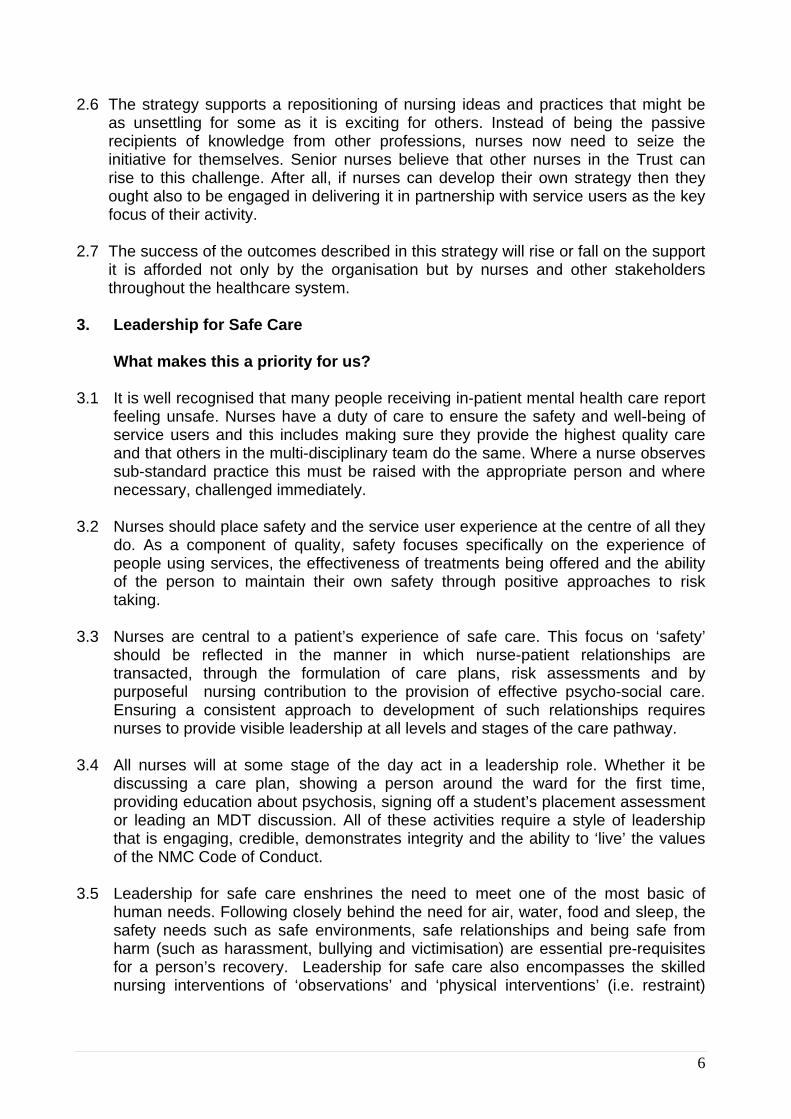
Table 1: Leadership for Safe Care
Leadership for Safe Care
We will take action to: We will see:
Improve the practice of Engagement and Observations for the most vulnerable patients so that nurses have full responsibility for the commencement, review and cessation of this nursing practice.
Safer practice in relation to observation with improved education and training. Regular audit of engagement and observation in practice. More purposeful engagement and therapeutic activities for service users. A new system of service user feedback to reinforce excellence in nursing care practice.
Raise awareness of therapeutic boundary and relationship management.
The use of self evaluation questionnaires to help understand interpersonal styles and risks to boundary violations leading to improved self awareness and seeking staff support.
Hig
h qu
ality
rela
tions
hips
and
en
gage
men
t
Respond to all concerns, comments and complaints in a timely and humane manner.
An improvement in complaints handling and closure of complaints within agreed times. Improved satisfaction with services. Capture of compliments, concerns and comments.
Implement inpatient care standards across all areas which will create safer environments, more confidence in caring, and improved privacy and dignity.
In-patient standards introduced in all areas – linked to programme of audit and internal benchmarking. Service User safety visits - linked to a forward plan of safety themes. The Confidence in Caring toolkit available and being used in areas identified to benefit from it.
Roll out ‘Time to Care‘ across all in-patient services.
Implementation of Time to Care and the Star Wards Programme in all inpatient areas. All nurses working in-patient and community settings spending at least 50% of their time on direct patient care. More productive staff, working in efficient teams with reduced sickness levels, reduced bank usage and higher staff satisfaction. A more humane approach to mental health care demonstrated through:
• reduced incidents of violence and aggression, • less use of seclusion • less use of physical restraint • reduction in the repetition of complaints such as those
concerning poor staff attitude and lack of caring. C
lean
and
saf
e en
viro
nmen
ts
Maximise the benefits of medication and minimise direct side-effects, ensuring there is easy access to information and education to enable choice and personal control over medicines taken.
More nurses with supplementary and independent prescribing qualifications practising within their spheres of accountability. Access to medication leaflets and leaflets on wards and in community settings. Introduction of a medication care plan for all patients. Higher levels of medicines compliance
7
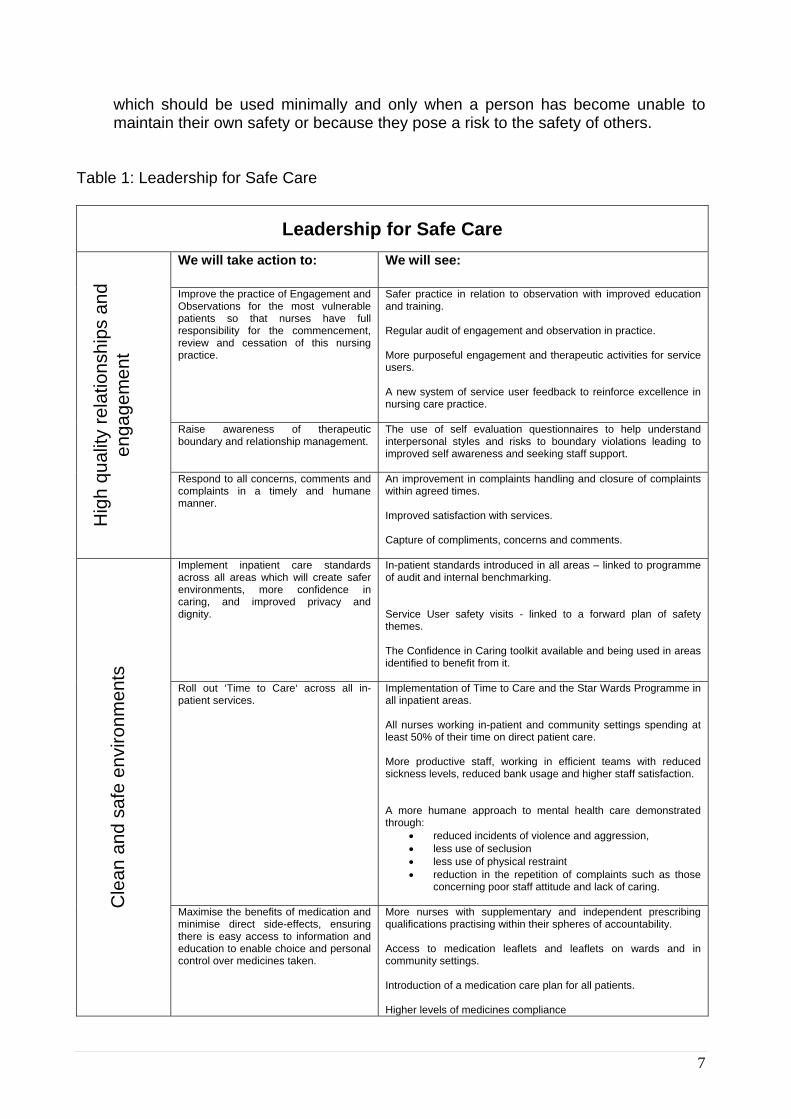
Review and strengthen the role of Ward Managers to ensure they are supported to provide leadership to maintain quality and safety.
A review of the ward manager role and job description, including a review of the administrative barriers that inhibit innovation and excellence in care delivery. A review of the in-patient nursing team skill-mix including the Clinical Team Leaders, staff nurses and health care support workers. A review of the accountability and line management of ward managers and community teams Evidence of purposeful clinical leadership amongst all Ward/Community Team Managers
Review the entire nursing structures against the recommendations in Front Line Care with respect to accountability and line of sight to the Executive Director of Nursing and Patient Experience.
Starting with the most senior nursing roles all nursing posts reviewed with respect to the quantity across the Trust, the knowledge, skills and competencies required and the value in relation to patient experience, patient safety and the professional leadership of nursing.
Vis
ible
lead
ersh
ip
Improve psychological awareness and effective communication
Star Wards principles applied to in-patient wards. Nurses leading groups and providing talking therapies across all care pathways. Nurses accessing supervision and training to engage psychologically with their practise.
4. Service User Experience and Recovery
What makes this a priority for us? 4.1 Service user experience is now the final judgement of successful care delivery.
Service users’ feedback about their experience of nursing is central both to improving quality of care and ensuring that what we deliver is responsive to actual need. It is also central to the Trust values of ‘caring’ and of ‘responsibility’ through which service users are encouraged to be active participants in their own care and in the operation of our organisation.
4.2 Feedback is currently captured by a number of internal and external sources.
External sources include national user surveys. Internal sources include complaints, community meetings and user and carer forums. From feedback already captured by these sources, there is a clear message that we need to improve the quality of interpersonal communications across a range of care domains. These include;
• The extent to which we make people feel welcome when they enter our services • How we provide information and involve people in their care • The amount and quality of interpersonal engagement • Treating people with dignity and respect at all times • Our attitude towards service users and their carers • Time taken to respond to areas where dissatisfaction is reported
4.3 In addition to the areas of interpersonal communications that need to be improved,
we need to improve the quality of the care environment in terms of cleanliness and hygiene.
8
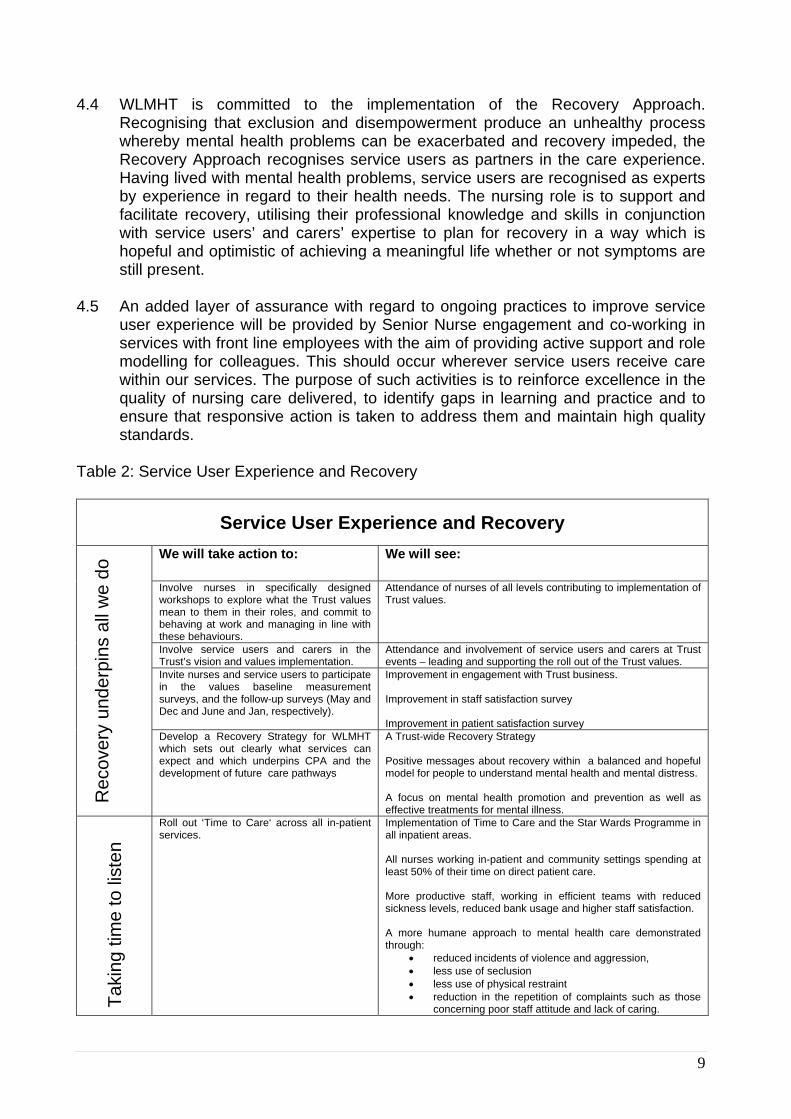
4.4 WLMHT is committed to the implementation of the Recovery Approach. Recognising that exclusion and disempowerment produce an unhealthy process whereby mental health problems can be exacerbated and recovery impeded, the Recovery Approach recognises service users as partners in the care experience. Having lived with mental health problems, service users are recognised as experts by experience in regard to their health needs. The nursing role is to support and facilitate recovery, utilising their professional knowledge and skills in conjunction with service users’ and carers’ expertise to plan for recovery in a way which is hopeful and optimistic of achieving a meaningful life whether or not symptoms are still present.
4.5 An added layer of assurance with regard to ongoing practices to improve service
user experience will be provided by Senior Nurse engagement and co-working in services with front line employees with the aim of providing active support and role modelling for colleagues. This should occur wherever service users receive care within our services. The purpose of such activities is to reinforce excellence in the quality of nursing care delivered, to identify gaps in learning and practice and to ensure that responsive action is taken to address them and maintain high quality standards.
Table 2: Service User Experience and Recovery
Service User Experience and Recovery
We will take action to: We will see:
Involve nurses in specifically designed workshops to explore what the Trust values mean to them in their roles, and commit to behaving at work and managing in line with these behaviours.
Attendance of nurses of all levels contributing to implementation of Trust values.
Involve service users and carers in the Trust’s vision and values implementation.
Attendance and involvement of service users and carers at Trust events – leading and supporting the roll out of the Trust values.
Invite nurses and service users to participate in the values baseline measurement surveys, and the follow-up surveys (May and Dec and June and Jan, respectively).
Improvement in engagement with Trust business. Improvement in staff satisfaction survey Improvement in patient satisfaction survey
Rec
over
y un
derp
ins
all w
e do
Develop a Recovery Strategy for WLMHT which sets out clearly what services can expect and which underpins CPA and the development of future care pathways
A Trust-wide Recovery Strategy Positive messages about recovery within a balanced and hopeful model for people to understand mental health and mental distress. A focus on mental health promotion and prevention as well as effective treatments for mental illness.
Taki
ng ti
me
to li
sten
Roll out ‘Time to Care‘ across all in-patient services.
Implementation of Time to Care and the Star Wards Programme in all inpatient areas. All nurses working in-patient and community settings spending at least 50% of their time on direct patient care. More productive staff, working in efficient teams with reduced sickness levels, reduced bank usage and higher staff satisfaction. A more humane approach to mental health care demonstrated through:
• reduced incidents of violence and aggression, • less use of seclusion • less use of physical restraint • reduction in the repetition of complaints such as those
concerning poor staff attitude and lack of caring.
9
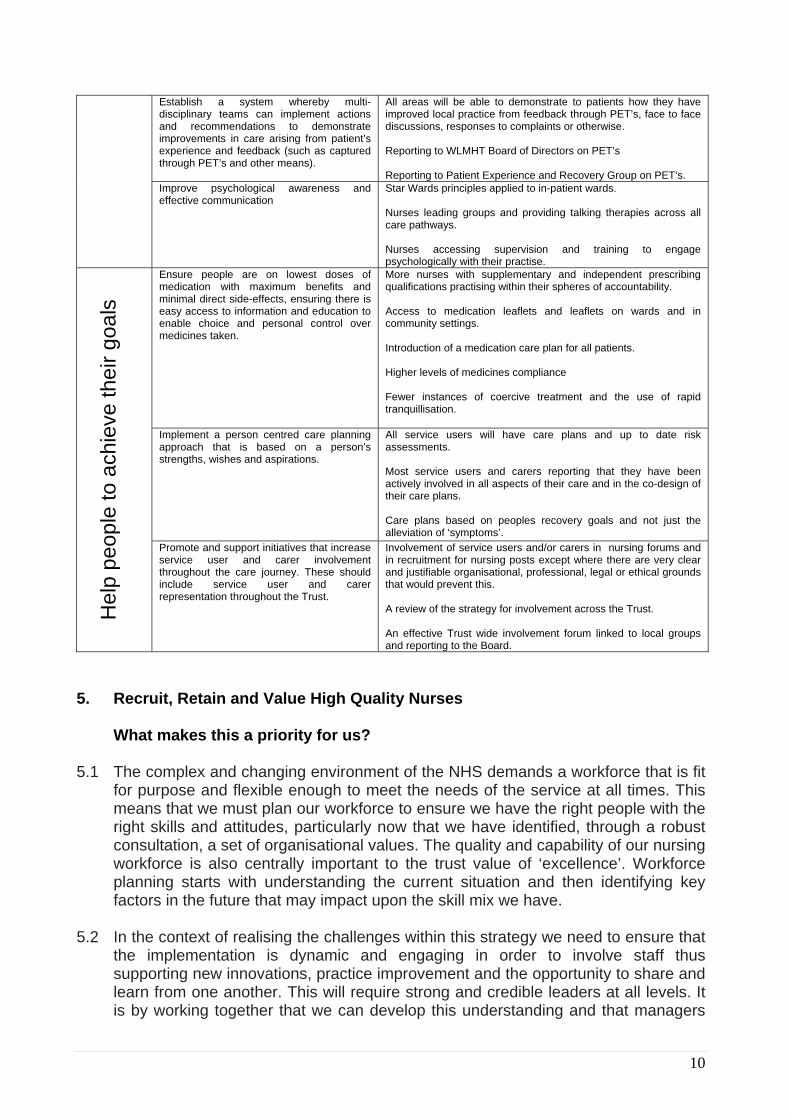
Establish a system whereby multi-disciplinary teams can implement actions and recommendations to demonstrate improvements in care arising from patient’s experience and feedback (such as captured through PET’s and other means).
All areas will be able to demonstrate to patients how they have improved local practice from feedback through PET’s, face to face discussions, responses to complaints or otherwise. Reporting to WLMHT Board of Directors on PET’s Reporting to Patient Experience and Recovery Group on PET’s.
Improve psychological awareness and effective communication
Star Wards principles applied to in-patient wards. Nurses leading groups and providing talking therapies across all care pathways. Nurses accessing supervision and training to engage psychologically with their practise.
Ensure people are on lowest doses of medication with maximum benefits and minimal direct side-effects, ensuring there is easy access to information and education to enable choice and personal control over medicines taken.
More nurses with supplementary and independent prescribing qualifications practising within their spheres of accountability. Access to medication leaflets and leaflets on wards and in community settings. Introduction of a medication care plan for all patients. Higher levels of medicines compliance Fewer instances of coercive treatment and the use of rapid tranquillisation.
Implement a person centred care planning approach that is based on a person’s strengths, wishes and aspirations.
All service users will have care plans and up to date risk assessments. Most service users and carers reporting that they have been actively involved in all aspects of their care and in the co-design of their care plans. Care plans based on peoples recovery goals and not just the alleviation of ‘symptoms’.
Hel
p pe
ople
to a
chie
ve th
eir g
oals
Promote and support initiatives that increase service user and carer involvement throughout the care journey. These should include service user and carer representation throughout the Trust.
Involvement of service users and/or carers in nursing forums and in recruitment for nursing posts except where there are very clear and justifiable organisational, professional, legal or ethical grounds that would prevent this. A review of the strategy for involvement across the Trust. An effective Trust wide involvement forum linked to local groups and reporting to the Board.
5. Recruit, Retain and Value High Quality Nurses
What makes this a priority for us? 5.1 The complex and changing environment of the NHS demands a workforce that is fit
for purpose and flexible enough to meet the needs of the service at all times. This means that we must plan our workforce to ensure we have the right people with the right skills and attitudes, particularly now that we have identified, through a robust consultation, a set of organisational values. The quality and capability of our nursing workforce is also centrally important to the trust value of ‘excellence’. Workforce planning starts with understanding the current situation and then identifying key factors in the future that may impact upon the skill mix we have.
5.2 In the context of realising the challenges within this strategy we need to ensure that
the implementation is dynamic and engaging in order to involve staff thus supporting new innovations, practice improvement and the opportunity to share and learn from one another. This will require strong and credible leaders at all levels. It is by working together that we can develop this understanding and that managers
10
can provide the right level of support to staff. It is also important for staff to provide the right support to each other and to engage in the construction and implementation of dynamic learning environments throughout the Trust, imbued with a genuine quest to underpin best practice by contemporary evidence and learning.
5.3 We need to be clear about the direction of the nursing workforce and adapt new
ways of working. An example of this is the need to develop a workforce model for the introduction of independent nurse prescribing, for approved mental health practitioners, for nurse led services and for the appointment of additional consultant nurses. Only when nurses are deployed in visible and leading roles will the confidence and credibility of nursing as a profession be truly realised.
5.4 Nurses at all stages of their career need to have ongoing opportunities to improve
their knowledge and skills. This is essential if nurses are going to meet the challenges of the changing environments in which they are working. Nursing at pre-registration is becoming an all graduate profession at the point of registration and nurses with higher degrees are already increasingly common place in the workforce. It is important that these opportunities are extended to members of the existing nursing workforce. This is closely allied to realising our value of ‘excellence’. As such we are committed to creating a learning culture throughout the Trust that encourages personal development and creativity.
5.5 Student Nurses are the Registered Nurses of tomorrow. Therefore it is essential
that they are supported in their learning by nurse mentors who are able to educate and inspire them. Building nursing knowledge and skills will not only be about training. Nurses also need to become active producers of their own knowledge through research and reflection that is grounded in practice and in the experience of delivering compassionate and recovery orientated care.
5.6 Nurses must feel empowered in their roles and feel that their opinions and ideas
about the service we provide really do matter. We aim to improve how we engage with staff and how we utilise their expertise and knowledge to deliver on our agenda. It is important that we understand the skills and competencies of our workforce and the focus for the next three years will be to improve that understanding so that any organisational development programmes, including training, can be directed in the most appropriate manner.
5.7 Healthcare Assistants1 are central to delivering nursing care under the supervision
of Registered Nurses. The Healthcare Assistant role will be reviewed and included in all aspects of nursing development. These employees are often the key contact point for our service users and therefore require the same level of support and attention to their development as Registered Nurses. Healthcare Assistants’ development will reflect both their personal development and service specific needs.
5.8 The Executive Team of West London Mental Health Trust believes that staff are its
most important asset and is committed to promoting a positive work environment for
1 Healthcare Assistants refers to all unregistered staff who are working within nursing roles, including support workers etc.
11
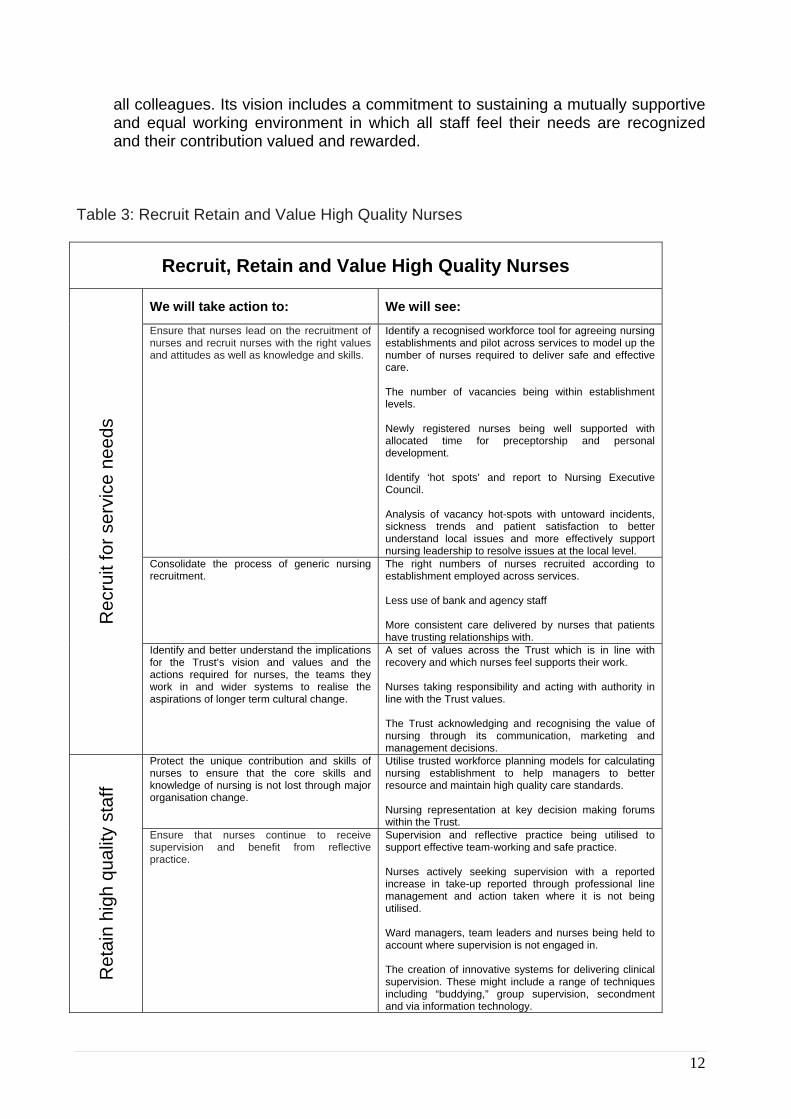
all colleagues. Its vision includes a commitment to sustaining a mutually supportive and equal working environment in which all staff feel their needs are recognized and their contribution valued and rewarded.
Table 3: Recruit Retain and Value High Quality Nurses
Recruit, Retain and Value High Quality Nurses
We will take action to: We will see:
Ensure that nurses lead on the recruitment of nurses and recruit nurses with the right values and attitudes as well as knowledge and skills.
Identify a recognised workforce tool for agreeing nursing establishments and pilot across services to model up the number of nurses required to deliver safe and effective care. The number of vacancies being within establishment levels. Newly registered nurses being well supported with allocated time for preceptorship and personal development. Identify ‘hot spots’ and report to Nursing Executive Council. Analysis of vacancy hot-spots with untoward incidents, sickness trends and patient satisfaction to better understand local issues and more effectively support nursing leadership to resolve issues at the local level.
Consolidate the process of generic nursing recruitment.
The right numbers of nurses recruited according to establishment employed across services. Less use of bank and agency staff More consistent care delivered by nurses that patients have trusting relationships with.
Rec
ruit
for s
ervi
ce n
eeds
Identify and better understand the implications for the Trust’s vision and values and the actions required for nurses, the teams they work in and wider systems to realise the aspirations of longer term cultural change.
A set of values across the Trust which is in line with recovery and which nurses feel supports their work. Nurses taking responsibility and acting with authority in line with the Trust values. The Trust acknowledging and recognising the value of nursing through its communication, marketing and management decisions.
Protect the unique contribution and skills of nurses to ensure that the core skills and knowledge of nursing is not lost through major organisation change.
Utilise trusted workforce planning models for calculating nursing establishment to help managers to better resource and maintain high quality care standards. Nursing representation at key decision making forums within the Trust.
Ret
ain
high
qua
lity
staf
f
Ensure that nurses continue to receive supervision and benefit from reflective practice.
Supervision and reflective practice being utilised to support effective team-working and safe practice. Nurses actively seeking supervision with a reported increase in take-up reported through professional line management and action taken where it is not being utilised. Ward managers, team leaders and nurses being held to account where supervision is not engaged in. The creation of innovative systems for delivering clinical supervision. These might include a range of techniques including “buddying,” group supervision, secondment and via information technology.
12
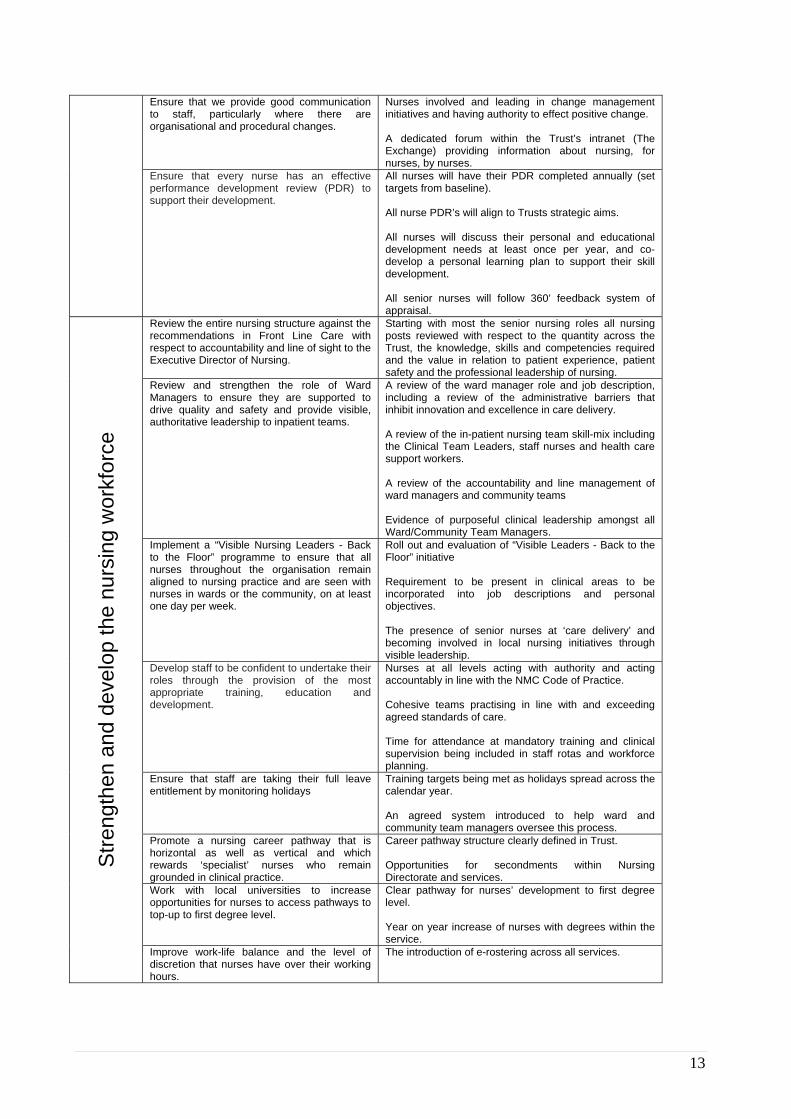
Ensure that we provide good communication to staff, particularly where there are organisational and procedural changes.
Nurses involved and leading in change management initiatives and having authority to effect positive change. A dedicated forum within the Trust’s intranet (The Exchange) providing information about nursing, for nurses, by nurses.
Ensure that every nurse has an effective performance development review (PDR) to support their development.
All nurses will have their PDR completed annually (set targets from baseline). All nurse PDR’s will align to Trusts strategic aims. All nurses will discuss their personal and educational development needs at least once per year, and co-develop a personal learning plan to support their skill development. All senior nurses will follow 360’ feedback system of appraisal.
Review the entire nursing structure against the recommendations in Front Line Care with respect to accountability and line of sight to the Executive Director of Nursing.
Starting with most the senior nursing roles all nursing posts reviewed with respect to the quantity across the Trust, the knowledge, skills and competencies required and the value in relation to patient experience, patient safety and the professional leadership of nursing.
Review and strengthen the role of Ward Managers to ensure they are supported to drive quality and safety and provide visible, authoritative leadership to inpatient teams.
A review of the ward manager role and job description, including a review of the administrative barriers that inhibit innovation and excellence in care delivery. A review of the in-patient nursing team skill-mix including the Clinical Team Leaders, staff nurses and health care support workers. A review of the accountability and line management of ward managers and community teams Evidence of purposeful clinical leadership amongst all Ward/Community Team Managers.
Implement a “Visible Nursing Leaders - Back to the Floor” programme to ensure that all nurses throughout the organisation remain aligned to nursing practice and are seen with nurses in wards or the community, on at least one day per week.
Roll out and evaluation of “Visible Leaders - Back to the Floor” initiative Requirement to be present in clinical areas to be incorporated into job descriptions and personal objectives. The presence of senior nurses at ‘care delivery’ and becoming involved in local nursing initiatives through visible leadership.
Develop staff to be confident to undertake their roles through the provision of the most appropriate training, education and development.
Nurses at all levels acting with authority and acting accountably in line with the NMC Code of Practice. Cohesive teams practising in line with and exceeding agreed standards of care. Time for attendance at mandatory training and clinical supervision being included in staff rotas and workforce planning.
Ensure that staff are taking their full leave entitlement by monitoring holidays
Training targets being met as holidays spread across the calendar year. An agreed system introduced to help ward and community team managers oversee this process.
Promote a nursing career pathway that is horizontal as well as vertical and which rewards ‘specialist’ nurses who remain grounded in clinical practice.
Career pathway structure clearly defined in Trust. Opportunities for secondments within Nursing Directorate and services.
Work with local universities to increase opportunities for nurses to access pathways to top-up to first degree level.
Clear pathway for nurses’ development to first degree level. Year on year increase of nurses with degrees within the service.
Stre
ngth
en a
nd d
evel
op th
e nu
rsin
g w
orkf
orce
Improve work-life balance and the level of discretion that nurses have over their working hours.
The introduction of e-rostering across all services.
13
6. Quality and Innovation in Nursing Practice
What makes this a priority for us? 6.1 “Putting nurses at the forefront of leading and managing services brings many
benefits” (Front Line Care, 2010). This will require a culture within the organisation that truly believes, values and enables nurses to be fully involved in the design, delivery and leadership of new service models. For this to happen nurses will need to develop a repertoire of leadership skills that extends beyond management based on a transactional model (carrot and stick) to transformational and ethical leadership based on a clear vision in line with the Trusts statement of purpose and the Trusts values and congruent with therapeutic recovery based practice.
6.2 We should not underestimate the innovative and excellent standards provided
throughout the Trust by nurses, but we need to improve how we share this so that other teams or individuals can adapt their own approaches based on others’ experience. Evidence of sub standard care, and behaviour and attitudes which are not in line with the new Trust values, will be challenged at all levels of nursing and a zero tolerance approach should be the norm.
6.3 Nurses throughout the organisation need to continue to reflect upon how they
position themselves in relation to other professions to make themselves visible and influential. To do this they will need to contest existing practices and ideologies, challenge poor practice and mediocrity, and support innovation and improvement to create better care experiences and improved productivity. Wherever nurse leaders are located in the organisation it is essential that they remain aligned to the values and practices of nursing – thus modelling credible leadership to agreed standards of practise and instilling hope and optimism for a quality service experience and consistent delivery. This links strongly to the Trust values of ‘togetherness’.
6.4 A quality based approach to healthcare affirms the value of nurses who are pivotal
in ensuring the delivery of safe, fair, personalised and effective care. This will need to involve a significant shift in thinking throughout the organisation. Quality care is experienced through high quality relationships and we aim to recruit and retain nurses who are a good fit with the WLMHT values. They should be interpersonally effective, present with strong emotional intelligence and possess good self-awareness achieved through reflective practice, continual learning and honest feedback.
14
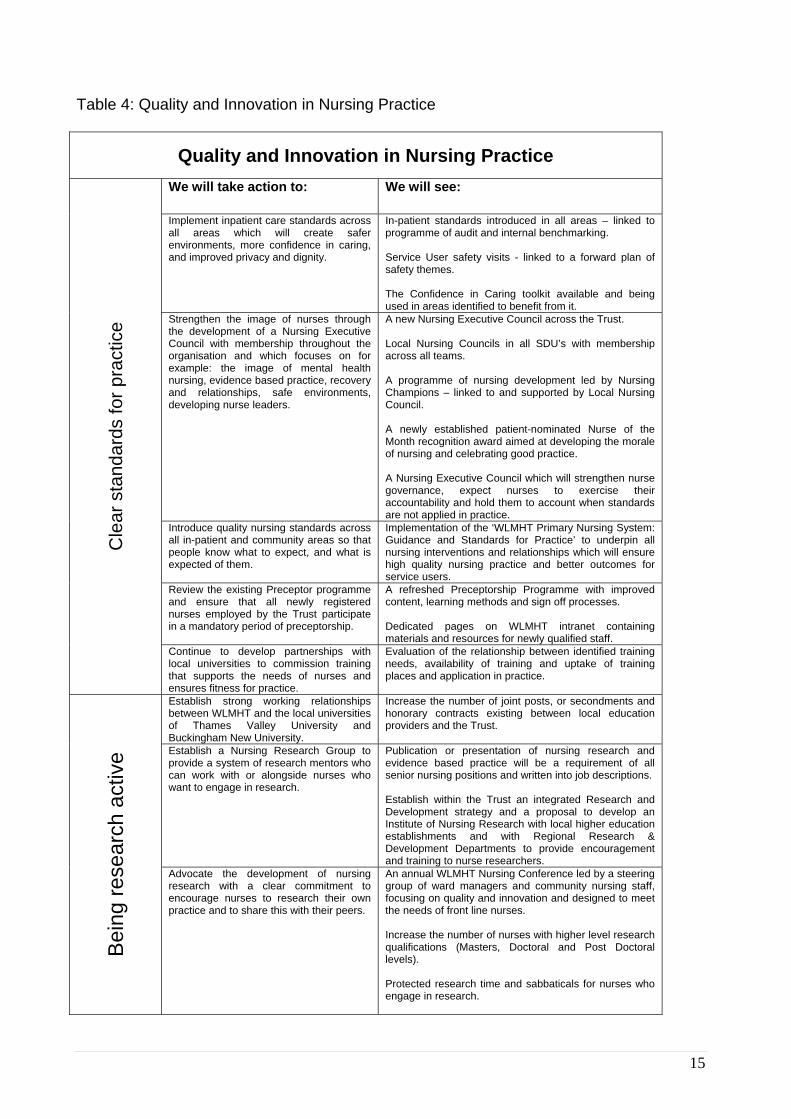
Table 4: Quality and Innovation in Nursing Practice
Quality and Innovation in Nursing Practice
We will take action to: We will see:
Implement inpatient care standards across all areas which will create safer environments, more confidence in caring, and improved privacy and dignity.
In-patient standards introduced in all areas – linked to programme of audit and internal benchmarking. Service User safety visits - linked to a forward plan of safety themes. The Confidence in Caring toolkit available and being used in areas identified to benefit from it.
Strengthen the image of nurses through the development of a Nursing Executive Council with membership throughout the organisation and which focuses on for example: the image of mental health nursing, evidence based practice, recovery and relationships, safe environments, developing nurse leaders.
A new Nursing Executive Council across the Trust. Local Nursing Councils in all SDU’s with membership across all teams. A programme of nursing development led by Nursing Champions – linked to and supported by Local Nursing Council. A newly established patient-nominated Nurse of the Month recognition award aimed at developing the morale of nursing and celebrating good practice. A Nursing Executive Council which will strengthen nurse governance, expect nurses to exercise their accountability and hold them to account when standards are not applied in practice.
Introduce quality nursing standards across all in-patient and community areas so that people know what to expect, and what is expected of them.
Implementation of the ‘WLMHT Primary Nursing System: Guidance and Standards for Practice’ to underpin all nursing interventions and relationships which will ensure high quality nursing practice and better outcomes for service users.
Review the existing Preceptor programme and ensure that all newly registered nurses employed by the Trust participate in a mandatory period of preceptorship.
A refreshed Preceptorship Programme with improved content, learning methods and sign off processes. Dedicated pages on WLMHT intranet containing materials and resources for newly qualified staff.
Cle
ar s
tand
ards
for p
ract
ice
Continue to develop partnerships with local universities to commission training that supports the needs of nurses and ensures fitness for practice.
Evaluation of the relationship between identified training needs, availability of training and uptake of training places and application in practice.
Establish strong working relationships between WLMHT and the local universities of Thames Valley University and Buckingham New University.
Increase the number of joint posts, or secondments and honorary contracts existing between local education providers and the Trust.
Establish a Nursing Research Group to provide a system of research mentors who can work with or alongside nurses who want to engage in research.
Publication or presentation of nursing research and evidence based practice will be a requirement of all senior nursing positions and written into job descriptions. Establish within the Trust an integrated Research and Development strategy and a proposal to develop an Institute of Nursing Research with local higher education establishments and with Regional Research & Development Departments to provide encouragement and training to nurse researchers.
Bei
ng re
sear
ch a
ctiv
e
Advocate the development of nursing research with a clear commitment to encourage nurses to research their own practice and to share this with their peers.
An annual WLMHT Nursing Conference led by a steering group of ward managers and community nursing staff, focusing on quality and innovation and designed to meet the needs of front line nurses. Increase the number of nurses with higher level research qualifications (Masters, Doctoral and Post Doctoral levels).
Protected research time and sabbaticals for nurses who engage in research.
15
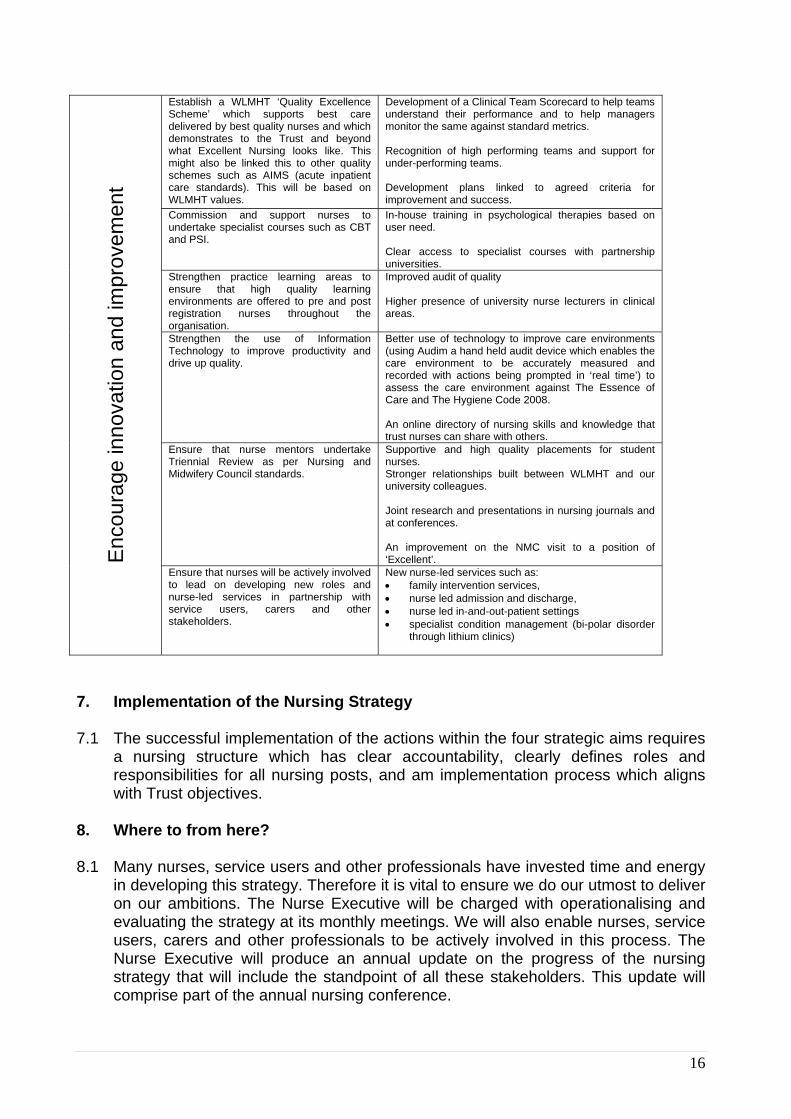
Establish a WLMHT ‘Quality Excellence Scheme’ which supports best care delivered by best quality nurses and which demonstrates to the Trust and beyond what Excellent Nursing looks like. This might also be linked this to other quality schemes such as AIMS (acute inpatient care standards). This will be based on WLMHT values.
Development of a Clinical Team Scorecard to help teams understand their performance and to help managers monitor the same against standard metrics. Recognition of high performing teams and support for under-performing teams. Development plans linked to agreed criteria for improvement and success.
Commission and support nurses to undertake specialist courses such as CBT and PSI.
In-house training in psychological therapies based on user need. Clear access to specialist courses with partnership universities.
Strengthen practice learning areas to ensure that high quality learning environments are offered to pre and post registration nurses throughout the organisation.
Improved audit of quality Higher presence of university nurse lecturers in clinical areas.
Strengthen the use of Information Technology to improve productivity and drive up quality.
Better use of technology to improve care environments (using Audim a hand held audit device which enables the care environment to be accurately measured and recorded with actions being prompted in ‘real time’) to assess the care environment against The Essence of Care and The Hygiene Code 2008. An online directory of nursing skills and knowledge that trust nurses can share with others.
Ensure that nurse mentors undertake Triennial Review as per Nursing and Midwifery Council standards.
Supportive and high quality placements for student nurses. Stronger relationships built between WLMHT and our university colleagues. Joint research and presentations in nursing journals and at conferences. An improvement on the NMC visit to a position of ‘Excellent’. E
ncou
rage
inno
vatio
n an
d im
prov
emen
t
Ensure that nurses will be actively involved to lead on developing new roles and nurse-led services in partnership with service users, carers and other stakeholders.
New nurse-led services such as: • family intervention services, • nurse led admission and discharge, • nurse led in-and-out-patient settings • specialist condition management (bi-polar disorder
through lithium clinics)
7. Implementation of the Nursing Strategy 7.1 The successful implementation of the actions within the four strategic aims requires
a nursing structure which has clear accountability, clearly defines roles and responsibilities for all nursing posts, and am implementation process which aligns with Trust objectives.
8. Where to from here? 8.1 Many nurses, service users and other professionals have invested time and energy
in developing this strategy. Therefore it is vital to ensure we do our utmost to deliver on our ambitions. The Nurse Executive will be charged with operationalising and evaluating the strategy at its monthly meetings. We will also enable nurses, service users, carers and other professionals to be actively involved in this process. The Nurse Executive will produce an annual update on the progress of the nursing strategy that will include the standpoint of all these stakeholders. This update will comprise part of the annual nursing conference.
16
8.2 The development of this Nursing Strategy, as outlined in the introduction, is based on the areas our nurses felt we needed to focus on. The process of implementing the strategy will aim to continue to engage nurses in the development of nursing, and we will encourage as many nurses as possible to get involved with the quality agenda for improving care within the Trust. By improving communication within the nursing community we hope to strengthen the involvement and engagement nurses have in the belief that by making this happen it will benefit nurses and the patients they care for.
8.3 We also expect this to raise levels of pride and enthusiasm about being part of the
nursing team in this organisation through the realisation of the excellent work we do and the support available to help us overcome the challenges we face. Every nurse should feel that they are heard and that their ideas, questions or concerns will be listened to.
17
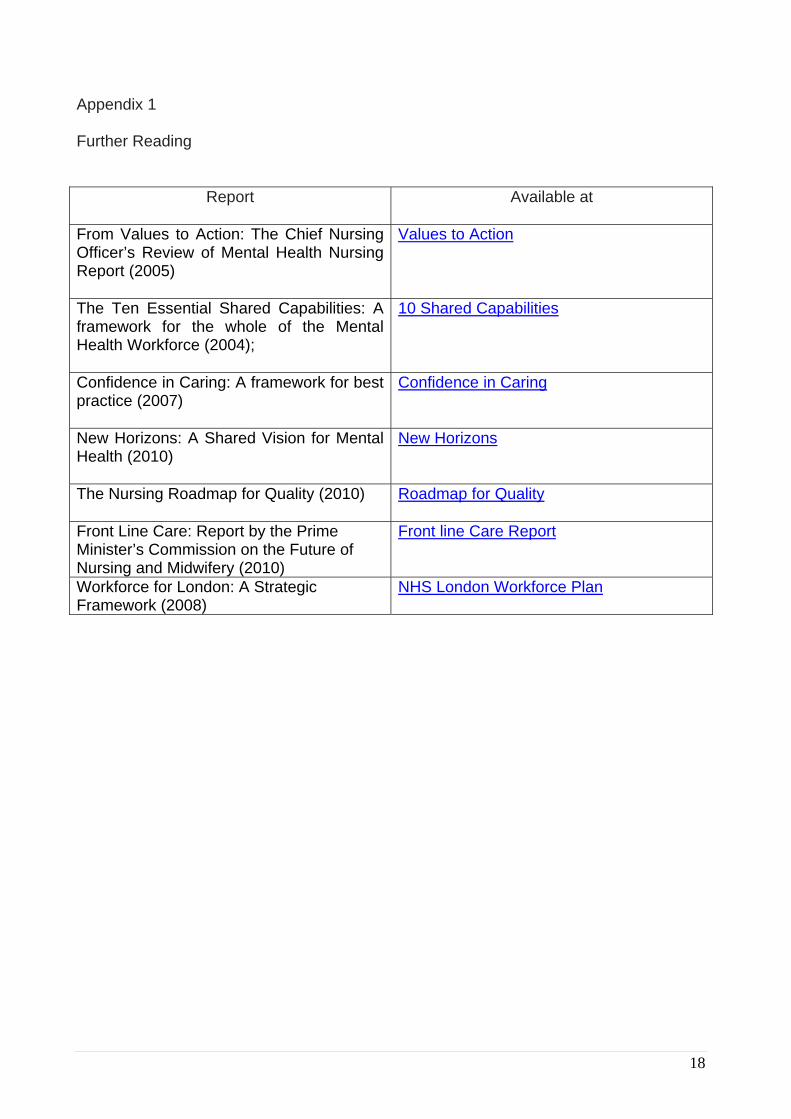
Appendix 1 Further Reading
Report
Available at
From Values to Action: The Chief Nursing Officer’s Review of Mental Health Nursing Report (2005)
Values to Action
The Ten Essential Shared Capabilities: A framework for the whole of the Mental Health Workforce (2004);
10 Shared Capabilities
Confidence in Caring: A framework for best practice (2007)
Confidence in Caring
New Horizons: A Shared Vision for Mental Health (2010)
New Horizons
The Nursing Roadmap for Quality (2010)
Roadmap for Quality
Front Line Care: Report by the Prime Minister’s Commission on the Future of Nursing and Midwifery (2010)
Front line Care Report
Workforce for London: A Strategic Framework (2008)
NHS London Workforce Plan
18





























