Embed Size (px)
Citation preview

+
Nursing Sciences
Tim Duncan; RN, CCRN, CEN, EMTP
2015 KISSPharm L.L.C
+Fluid and Electrolyte Balance
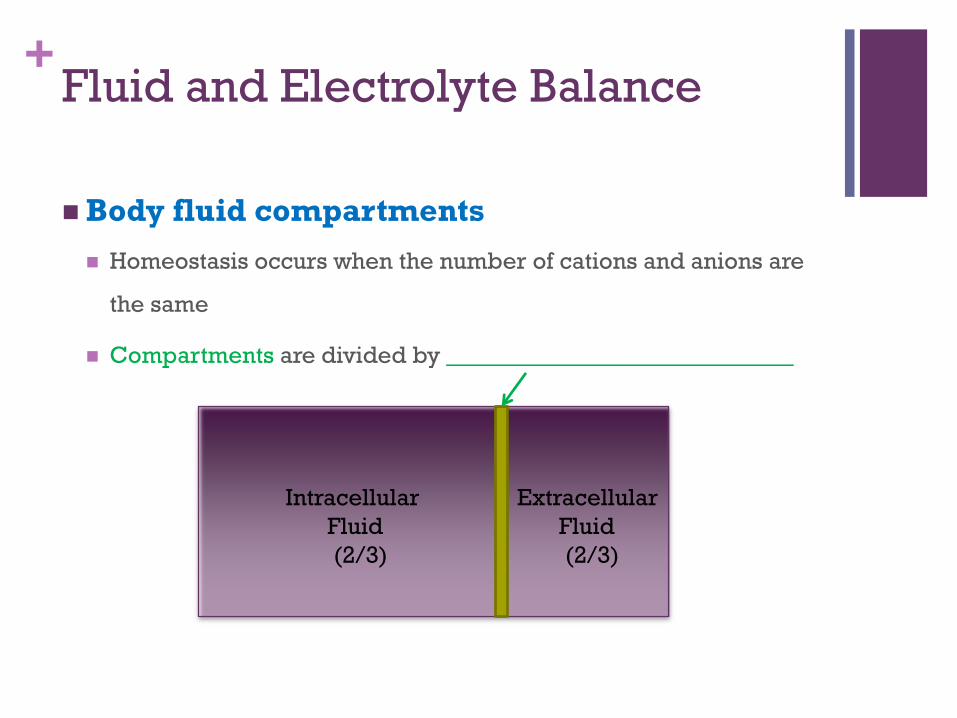
Body fluid compartments
Homeostasis occurs when the number of cations and anions are
the same
Compartments are divided by _____________________________
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid and Electrolyte Balance
Body fluid compartments
Two main compartments
Intracellular (ICF) : fluid inside the cell (2/3 of the cell)
Extracellular (ECF) : fluid outside the cell (1/3 of the cell)
Includes interstitial fluid, blood, connective tissue, water, and
transcellular fluid
+Fluid and Electrolyte Balance
Edema
Excess collection of fluid in the interstitial space
Localized edema
Trauma from accidents or surgery
Local inflammatory processes
Burns
Generalized edema
Can occur due to cardiac, renal, or liver failure
Infants and older adults are more susceptible to
fluid-related problems.
+Body fluid transport
Diffusion
Process where a solute from a higher concentration may spread
through a solution to area of lower concentration
Membranes
Permeable
Selectively permeable
Osmosis
Force that pulls the solvent from a less concentrated solute to a
more concentrated solute
+Body fluid transport
Filtration
Hydrostatic pressure
Transfer of solutes and solvents from higher pressure to area of
lower pressure
The hydrostatic pressure is higher than osmotic pressure at the
_____________ end of the capillary
Consequently fluids move out of the capillary
The osmotic pressure is higher than the hydrostatic pressure at
the ______________ end
Therefore the fluids move into the capillary
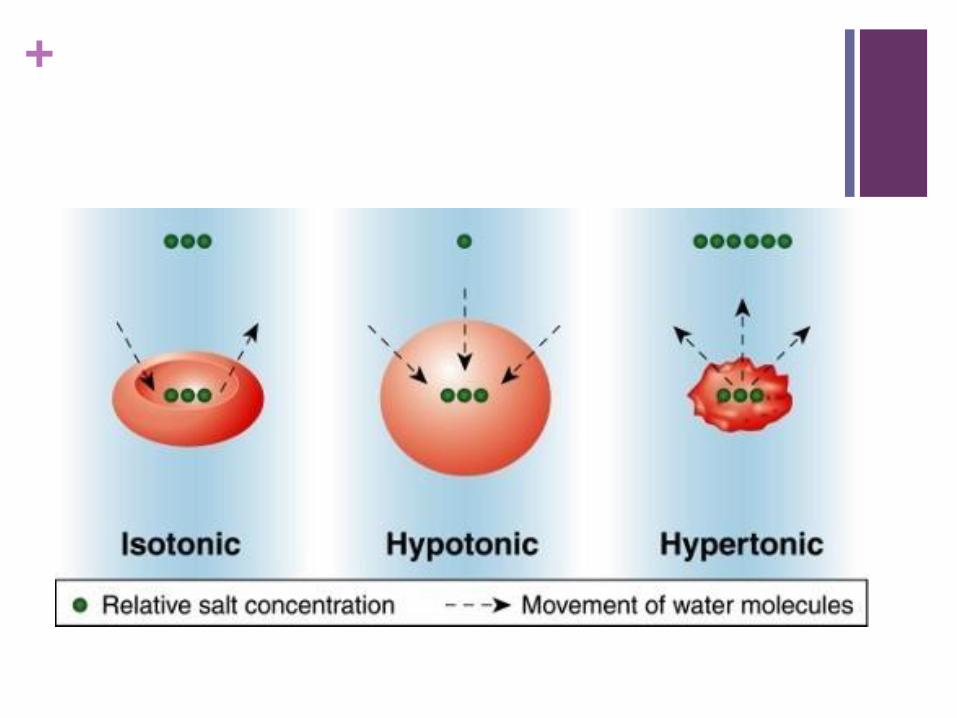
+Movement of body fluid
Isotonic solutions
Both sides are equal in concentration, very little osmosis occurs
Isotonic solutions have the same osmolality as body fluids
Hypotonic solutions
When a solution has less concentration of solute or salt compared
to another more concentrated solution
Have lower osmolality than body fluids
Hypertonic solutions
When a solution has a more concentration of solutes than other
less concentrated solutions
+
+Movement of body fluid (con’t)
Active transport
In order to have movement from a area of lower concentration to
an area of higher
Need ________
Require active transport
Ions
Sodium
Potassium
Calcium
Iron
Hydrogen
Some sugars
Amino acids
+Movement of body fluid (con’t)
Body fluid
Diarrhea can result in the loss of a lot of water and electrolytes
Most water is reabsorbed in the large colon
Kidneys regulate fluid and electrolyte balance
Adrenal glands
Regulate sodium reabsorption via secreting _________________
ADH also helps to regulate water balance
+Fluid Volume Deficit
Isotonic dehydration
Water and electrolytes are lost equally
Most common type of dehydration as known as hypovolemia
Results in decreased blood volume and therefore insufficient
tissue perfusion
+Fluid Volume Deficit
________________ dehydration
Causes
Improper intake of fluids and solutes
Fluid shifts
Dramatic loss of isotonic body fluids
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Deficit
________________ dehydration
Water loss is greater than electrolyte loss
Cell shrinks
Causes
Extreme perspiration
Hyperventilation
Ketoacidosis
Prolonged fevers
Diarrhea
Early-stage renal failure
Diabetes insipidus
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Deficit
________________ dehydration
Electrolyte loss is greater than water loss
Cells swell
Causes
Chronic illness
Extreme fluid replacement (hypotonic)
Renal failure
Chronic malnutrition
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Deficient Findings
Cardiovascular
Increased pulse
Decreased blood pressure and orthostatic hypotension
Flat neck and hand veins
Diminished peripheral pulses
Decreased CVP
Dysrhythmias
+Fluid Volume Deficient Findings
Respiratory
Increased rate and depth of respirations
Dyspnea
Neuromuscular
Decreased CNS activity
Fever
Skeletal muscle weakness
Renal
Decreased urine output
+Fluid Volume Deficit Findings
Integumentary
Dry skin
Poor turgor
Dry mouth
Gastrointestinal
Decreased motility and bowel sounds
Constipation
Thirst
Decreased body weight
+Fluid Volume Deficit Findings
Laboratory findings
Increased serum osmolality
Increased hematocrit
Increased BUN level
Increased serum sodium level
Increased urinary specific gravity
+Fluid Volume Excess
___________ overhydration (aka hypervolemia)
The extracellular compartment is expanded
Edema
Complications
Cardiac dysfunction
CHF
Pulmonary edema
Causes
Improper IV therapy
Renal failure
Chronic corticosteroid therapy
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Excess
_______________ overhydration
The fluid goes from the intracellular compartment to ECF
Causes
Increased sodium ingestion
Rapid infusion
Extreme sodium bicarbonate therapy
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Excess
_____________ overhydration (aka water
intoxication)
All body fluid compartments are expanded
Electrolyte imbalance
Causes
Early renal failure
CHF
SIADH
Improper IV therapy
Replacement of isotonic fluid loss with hypotonic fluids
Intracellular
Fluid
(2/3)
Extracellular
Fluid
(2/3)
+Fluid Volume Excess Findings
Cardiovascular
Increased pulse
Increased blood pressure
Distended neck and hand veins
Elevated CVP
Dysrhythmias
Respiratory
Increased respiratory rate (shallow breathing)
Dyspnea
Moist Crackles
+Fluid Volume Excess Findings
Neuromuscular
Altered consciousness
Headache
Visual disturbances
Skeletal muscle weakness
Paresthesias
Renal
Increased urine output if kidneys are working
Decreased urine output if kidneys are damaged
+Fluid Volume Excess Findings
Integumentary
Pitting edema
Pale, cool skin
Gastrointestinal
Increased motility
Diarrhea
Increased body weight
Enlarged liver
Ascites
+Fluid Volume Excess Findings
Laboratory findings
Decreased serum osmolality
Decreased hematocrit
Decreased BUN
Deceased serum sodium
Decreased urine specific gravity
+Normal Electrolyte values
Sodium: 135-145 mEq/L
Potassium: 3.5-5.1 mEq/L
Chloride: 98-107 mEq/L
Bicarbonate (venous): __________ mEq/L
+Hyponatremia
Serum Na+ level less than ________ mEq/L
Food sources
Bacon
Canned food
Ketchup
Milk
Processed food
Snack food
Soy sauce
Bread
Na+ imbalance are typically related to fluid
imbalances
+Hyponatremia
Causes
Increased sodium excretion
Loss of Fluid
Sweating
Vomiting
Diarrhea
Renal disease
Dilution of serum sodium
Gain of Fluid
SIADH
CHF
Psychogenic polydipsia
DM
+Hyponatremia Findings
Cardiovascular
Normovolemic
Rapid pulse
NL BP
Hypovolemic
Weak rapid pulse
Low BP
Flat neck veins
NL or low CVP
Hypervolemic
Rapid bounding pulse
BP NL or elevated
NL or elevated CVP
+Hyponatremia Findings
Respiratory
Shallow breathing due to skeletal muscle weakness
Neuromuscular
Skeletal muscle weakness (worse in extremities)
Reduced deep tendon reflexes
Renal
Increased urinary output
+Hyponatremia Findings
CNS
Headache
Personality changes
Confusion
Seizures
Coma
Gastrointestinal
Increased motility
Hyperactive bowel sounds
Nausea
Diarrhea
Cramping
+Hyponatremia
Treatment
If there is a fluid volume deficit
Give IV sodium chloride
If due to fluid volume excess
Give osmotic diuretics
If due to SIADH
Give ADH antagonists
Increase sodium intake
Monitor patients taking lithium
Hyponatremia can hinder lithium excretion leading to ___________
+Hypernatremia
Serum Na+ levels exceed 145 mEq/L
Causes
Decreased Na+ excretion
Corticosteroids
Cushing's syndrome
Renal failure
Hyperaldosteronism
Increased Na+ intake
Decreased water intake
+Hypernatremia
Causes
Increased water loss
Increased metabolism
Fever
Hyperventilation
Infection
Extreme diaphoresis
Watery diarrhea
Diabetes insipidus
+Hypernatremia
Treatment
IV therapy
If due to fluid loss
Diuretics
If unable to excrete Na+
+Hypernatremia findings
Cardiovascular
Heart rate and BP depend on vascular volume
Respiratory
Pulmonary edema (hypervolemia)
Neuromuscular
Early manifestation
Spontaneous muscle twitches
Irregular muscle contractions
Late manifestation
Skeletal muscle weakness
deep tendon reflexes are absent
+Hypernatremia findings
CNS
Most common manifestation
Altered cerebral function
Normo-volemia or hypovolemia
Agitation
Confusion
Seizures
Hypervolemia
Lethargy
Stupor
Coma
+Hypernatremia findings
Gastrointestinal
Very thirsty
Renal
______________ urinary output
+Hypokalemia
Serum K+ level lower than 3.5 mEq/L
Food sources
Bananas
Avocado
Cantaloupe
Carrots
Meats
Mushrooms
Spinach
Life threatening because it can cause cardiac
arrhythmias!
+Hypokalemia
Causes
Total body K+ loss
Overuse of diuretics or corticosteroids
Increased secretion of aldosterone (Cushing’s syndrome)
Fluid Loss of any kind
Prolonged nasogastric suction
Excessive diaphoresis
Renal disease
Low K+ intake
+Hypokalemia
Pathophysiology
Shift of K+ from ECF to ICF
Alkalosis
_________________________
K+ dilution
Water intoxication
+Hypokalemia Findings
Cardiovascular
Weak irregular pulse
Weak peripheral pulses
Orthostatic hypotension
Respiratory
Shallow respirations
Absent breath sounds
+Hypokalemia Findings
Neuromuscular
Anxiety
Fatigue
Confusion
Coma
Skeletal muscle weakness
Paresthesias and deep tendon hyporeflexia
+Hypokalemia Findings
Gastrointestinal
Decreased motility
Absent bowel sounds
Nausea
Vomiting
Constipation
Paralytic ileus
+Hypokalemia Findings
Laboratory findings
ST depression
Shallow, flat or inverted T wave
Prominent U wave
+Hypokalemia
Treatment
Give K+ supplements
Oral supplements can cause nausea and vomiting
Do not give on an empty stomach
Liquid potassium chloride has a ______________________
So give with juice
+Hypokalemia
Treatment
K+ is never given by IV push
Intramuscular
Subcutaneous routes
IV potassium is diluted and given using an infusion device
+Hypokalemia
Treatment
Recommended infusion rate
5 to 10 mEq/hr
Do not exceed 20 mEq/hr
If patient is getting more than 10 mEq/hr place them on a
cardiac monitor
Check for phlebitis and infiltration
Nurse should also check for renal function
+Hyperkalemia
Potassium level greater than 5.1 mEq/L
Causes
Excessive K+ intake
Decreased K+ excretion
Potassium sparing diuretics
Renal failure
Addison’s disease
Shift of K+ from ICF to ECF
Tissue injury
Acidosis
Hyperuricemia
Hypercatabolism
+Hyperkalemia
Treatment
Restrict K+ diet
If kidney is functioning give K+ excreting diuretics
If kidney is nonfunctional give sodium polystyrene sulfonate
(Kayexalate)
Helps sodium absorption
K+ excretion in the gut
Dialysis
Hypertonic glucose with regular insulin (move K+ into the cells)
Blood transfusion patient should receive fresh blood
+Hyperkalemia findings
Cardiovascular
Slow and irregular pulse
Decreased BP
Gastrointestinal
Increased motility
Hyperactive bowel sounds
Diarrhea
+Hyperkalemia findings
Respiratory
_____________________________
Neuromuscular
Acute
Muscle twitches
Paresthesias
Chronic
Skeletal muscle weakness
Ascending flaccid paralysis
+Hyperkalemia findings
Laboratory findings
ECG
Tall peaked T waves
Flat P waves
Widened QRS complex
Prolonged PR intervals
+Hypocalcemia
Serum calcium level lower than 8.6 mg/dL
Food sources
Cheese
Collard greens
Milk
Sardines
Spinach
Tofu
Yogurt
+Hypocalcemia
Causes
Decreased calcium absorption in the gut
Not enough oral intake of calcium
Lactose intolerance
Malabsorption
Low vitamin D intake
End-stage renal disease
+Hypocalcemia
Causes
Increased calcium excretion
Renal failure
Diarrhea
Steatorrhea
Wound drainage
+Hypocalcemia
Causes
Decreased ionized fraction of calcium
Hyperproteinemia
Alkalosis
Medications
Acute pancreatitis
Hyperphosphatemia
Immobility
Damaged parathyroid glands
+Hypocalcemia Findings
Cardiovascular
Decreased pulse and ____________________________
Decreased BP
Respiratory
Decreased respiratory movement
+Hypocalcemia Findings
Gastrointestinal
Increased gastric motility
Hyperactive bowel sounds
Cramping
Diarrhea
Renal
Urinary output depends on the cause
+Hypocalcemia Findings
Neuromuscular
Anxiety
Irritability
Hyperactive deep tendon reflexes
Painful muscle spasms
Tetany
Seizures
Positive Trousseau’s and Chvostek’s signs
+Hypocalcemia Findings
Laboratory findings
ECG:
Prolonged ST interval
Prolonged QT interval
+Hypocalcemia Treatment
Treatment
Give calcium supplements
Warm the injections and administer slowly
Watch for ECG changes
Medications that increase calcium absorption
Aluminum hydroxide
Vitamin D
10% Calcium gluconate
+Hypercalcemia
Serum level _____________ than 10 mg/dL
Causes
Increased calcium absorption
Decreased calcium excretion (renal failure, use of thiazide
diuetics)
Increased bone reabsorption of calcium (hyperparathyroidism,
hyperthyroidism, malignancy, immobility, glucocorticoids)
Hemoconcentration (dehydration, lithium, adrenal insufficiency)
+Hypercalcemia
Treatment
Discontinue calcium containing substances or drugs
Give medications that get rid of calcium
Phosphorus
Calcitonin
Bisphosphonates
Prostaglandin synthesis inhibitors
Aspirin
Dialysis
Patient with calcium imbalance is at high risk for a fracture, so
move them carefully
Monitor for urinary stones
+Hypercalcemia findings
Cardiovascular
Increased pulse early on, later decreased heart rate can lead to
cardiac arrest
Bounding
Full peripheral pulses
Increased BP
Respiratory
Unsuccessful respiratory movement
Renal
Urinary output depends on cause
Renal calculi
Flank pain
+Hypercalcemia findings
Neuromuscular
Muscle weakness
Absent deep tendon reflexes
Disorientation
Fatigue
Coma
Gastrointestinal
Decreased motility
Hypoactive bowl sounds
Anorexia
Nausea
Constipation
Abdominal distension
+Hypercalcemia findings
Laboratory findings
ECG:
Shortened ST segment
Widened T wave
+Hypomagnesemia
Serum magnesium __________ than 1.6 mg/dL
Food sources
Avocado
Canned white tuna
Cauliflower
Green leafy vegetables
Spinach
Milk
Peanut Butter
Meat
Raisins
+Hypomagnesemia
Causes
Low magnesium
Malnutrition
Vomiting
Diarrhea
Malabsorption syndrome
Increased magnesium secretion
Medications
Chronic alcoholism
Intracellular movement of magnesium
Hyperglycemia
Insulin adminstration
Sepsis
+Hypomagnesemia
Treatment
Hypocalcemia usually occurs with hypomagnesemia
Fix calcium levels
Magnesium sulfate IV
Oral Mg
May cause diarrhea
Increase Mg loss
+Hypomagnesemia Findings
Cardiovascular
Increased HR and BP
Respiratory
Shallow respirations
CNS
Irritability
Confusion
+Hypomagnesemia Findings
Neuromuscular
Twitches
Hyperreflexia
Tetany
Seizures
Positive Trousseau’s and Chvostek’s signs
+Hypomagnesemia Findings
Laboratory findings
ECG:
Tall T waves
Depressed ST segments
+Hypermagnesemia
Serum magnesium level __________ than 2.6 ml/dL
Causes
Increased magnesium intake
Decreased excretion of magnesium
Treatment
Diuretics
Calcium chloride IV or calcium gluconate
+Hypermagnesemia Findings
Cardiovascular
Low HR and BP
Neuromuscular
Absent deep tendon reflexes
Skeletal muscle weakness
+Hypermagnesemia Findings
Respiratory
Respiratory depression
CNS
Drowsiness
Fatigue
Coma
+Hypermagnesemia Findings
Laboratory findings
ECG:
Prolonged PR interval
Widened QRS complexes
+Hypophosphatemia
Serum phosphorus level ________ than 2.7 mg/dL
Food sources:
Fish
Organ meats
Nuts
Pork
Beef
Chicken
Whole grain breads and cereals
+Hypophosphatemia
Causes
Not enough phosphorus intake
Increased phosphorus excretion (hyperparathyroidism,
malignancy, antacids)
Intracellular shift (hyperglycemia, respiratory alkalosis)
Treatment
Discontinue drugs or sources cause hypophosphatemia
Give phosphorus with a vitamin D supplement
Monitor renal function and for fractures
+Hypophosphatemia Findings
Cardiovascular
Decreased contractility and cardiac output
Low peripheral pulses
Respiratory
Shallow
Neuromuscular
Weakness
Decreased deep tendon reflexes
Decreased bone density
Rhabdomyolysis
+Hypophosphatemia Findings
CNS
Irritability
Confusion
Seizures
Hematological
Decreased platelet aggregation
Increased bleeding time
Immunosuppression
+Hyperphosphatemia
Serum phosphorus level greater than 4.5 mg/dL
Causes
Decreased renal excretion
Tumor lysis syndrome
Increased intake of phosphorus
Hypoparathyroidism
+Hyperphosphatemia
Treatment
Same as hypocalcemia
Phosphate-binding medications
Diet restriction
Drugs containing phosphate restriction
+ECG and electrolyte imbalances
Hypocalcemia
Prolonged ST interval
Prolonged QT interval
Hypercalcemia
Shortened ST segment
Widened T wave
+ECG and electrolyte imbalances
Hypokalemia
ST depression
Shallow, flat or inverted T wave
Prominent U wave
Hyperkalemia
Tall peaked T waves
Flat P waves
Widened QRS complex
Prolonged PR interval
+ECG and electrolyte imbalances
Hypomagnesemia
Tall T waves
Depressed ST segment
Hypermagnesemia
Prolonged PR interval
Widened QRS complex
+Hydrogen ions, Acids, and Bases
Hydrogen ions
Stated as pH
Has 2 forms in the body:
Volatile hydrogen of carbonic acid
Nonvolatile form of hydrogen and organic acids
+Hydrogen ions, Acids, and Bases
Acids
Contain hydrogen ions and are hydrogen ion donors
Number of hydrogen ions determines the strength of the acid
Bases
No hydrogen ions
Hydrogen ion acceptors
+Regulatory Systems
Buffers
Fastest acting regulatory system
Protect against any changes in hydrogen ions in the ECF
Transport mechanism for hydrogen to the lungs
+Regulatory Systems
Primary buffer systems
Hemoglobin system
Chloride shift
Plasma protein system
Carbonic acid-bicarbonate system
Phosphate buffer system
+Regulatory Systems
Lungs
Second defense of the body with the buffer system to maintain
acid-base balance
Acidosis:
pH decreases
Respiratory rate and depth increase in order to exhale acids
Alkalosis:
pH increases
Respiratory rate and depth decrease
CO2 is retained
Carbonic acid increases
+Regulatory systems (cont’d)
Kidneys
Fundamental correction of acid-base imbalance
Compensation
Acidosis:
Extra hydrogen ions are secreted into the tubules
Hydrogen with a buffer are excreted in the urine
Alkalosis:
Extra bicarbonate ions move into the tubules
Bicarbonate with sodium ions are excreted in the urine
Regulation of bicarbonate
+Regulatory systems (con’t)
____________________
Exchange role
Acidosis:
Hydrogen into the cell
K+ out
Alkalosis:
Hydrogen out to the blood
K+ in the cell
+Respiratory Acidosis
Causes
Primary defect in the function of the lungs or respiratory pattern
Obstruction of airway or depression of respiratory system
Asthma
Atelectasis
Brain trauma
Bronchiectasis
Bronchitis
CNS depressants
Emphysema
Hypoventilation
Pulmonary edema
Pneumonia
Pulmonary emboli
+Clinical Manifestations of
Respiratory Acidosis
Neurological
Drowsiness
Disorientation
Dizziness
Headache
Coma
+Clinical Manifestations of
Respiratory Acidosis
Cardiovascular
Decreased BP
Ventricular fibrillation
Peripheral vasodilation
Neuromuscular
Seizures
Respiratory
Hypoventilation with hypoxia
+Clinical manifestations of
Metabolic Acidosis
Neurological
Drowsiness
Confusion
Headache
Coma
Cardiovascular
Decreased BP
Dysrhythmias
Peripheral vasodilation
+Clinical manifestations of
Metabolic Acidosis
Gastrointestinal
Nausea
Vomiting
Diarrhea
Abdominal pain
Respiratory
Deep, rapid respirations
+Respiratory Alkalosis
Causes
Overstimulation of the respiratory system
Fever
Hyperventilation
Hypoxia
Hysteria
Over ventilation by mechanical ventilators
Pain
+Clinical Manifestations of
Respiratory Alkalosis
Neurological
Fatigue
Lightheadedness
Confusion
Cardiovascular
Fast HR
Dysrhythmias
Gastrointestinal
Nausea
vomiting
Epigastric pain
+Clinical Manifestations of
Respiratory Alkalosis
Neuromuscular
Tetany
Numbness
Tingling of extremities
Hyperreflexia
___________________
Respiratory
Hyperventilation
+Clinical manifestations of
Metabolic Alkalosis
Neurological
Drowsiness
Dizziness
Nervousness
Confusion
+Clinical manifestations of
Metabolic Alkalosis
Cardiovascular
Fast HR
Dysrhythmias
Gastrointestinal
Anorexia
Nausea
Vomiting
+Clinical manifestations of
Metabolic Alkalosis
Neuromuscular
Tremors
Hypertonic muscles
Muscle cramps
Tetany
Tingling of extremities
Seizures
Respiratory
Hypoventilation
+Clinical manifestations of
Metabolic Acidosis
Neurological
Drowsiness
Dizziness
Nervousness
Confusion
+Clinical manifestations of
Metabolic Acidosis
Cardiovascular
Tachycardia
Dysrhythmias
Gastrointestinal
Anorexia
_______________
Vomiting
+Clinical manifestations of
Metabolic Acidosis
Neuromuscular
Tremors
Hypertonic muscles
Muscle cramps
Tetany
Tingling of extremities
Seizures
Respiratory
Hypoventilation
+Metabolic Alkalosis
Buildup of a ________OR Loss of an _________
Deficit of carbonic acid
Decrease in hydrogen
Causes
Diuretics
Excessive vomiting or GI suctioning
Hyperaldosteronism
Ingestion
Transfusion of whole blood
+Acid-Base Imbalances
Respiratory acidosis
pH: Decreased
HCO3- : Normal
PaO2: Usually decreased
PaCO2: Increased
K+: Increased
+Acid-Base Imbalances
Respiratory alkalosis
pH: Increased
HCO3-: Normal
PaO2: Usually normal
PaCO2: Decreased
K+: Decreased
+Acid-Base Imbalances
Metabolic acidosis
pH: Decreased
HCO3-: Decreased
PaO2: Usually normal
PaCO2: Normal
K+: Increased
+Acid-Base Imbalances
Metabolic alkalosis
pH: Increased
HCO3-: ____________
PaO2: Normal
PaCO2: Normal
K+: Decreased
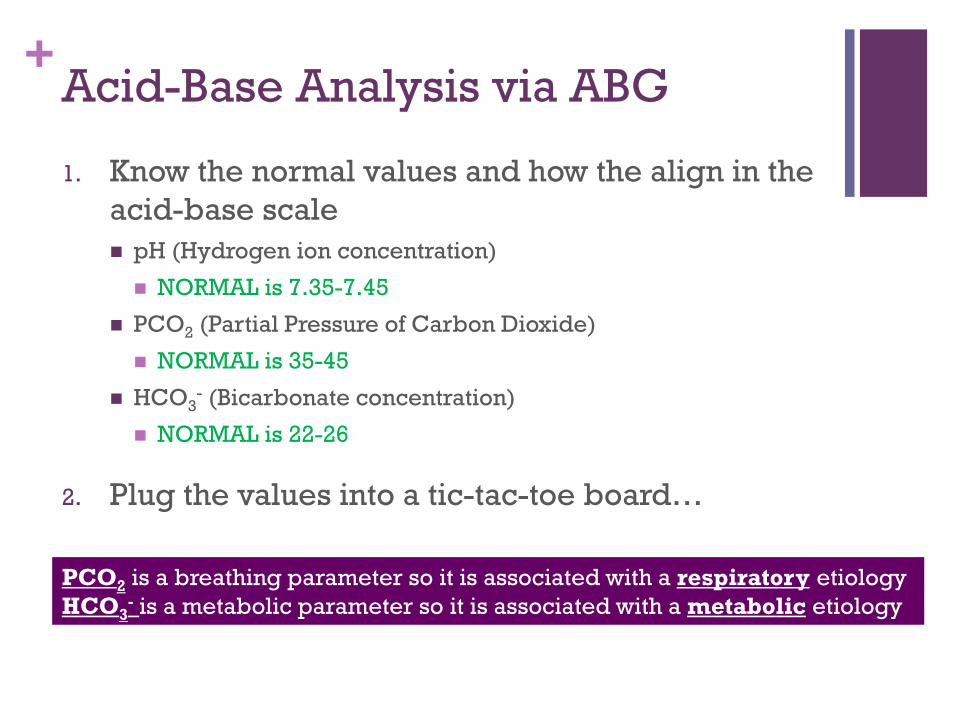
+Acid-Base Analysis via ABG
1. Know the normal values and how the align in the
acid-base scale
pH (Hydrogen ion concentration)
NORMAL is 7.35-7.45
PCO2 (Partial Pressure of Carbon Dioxide)
NORMAL is 35-45
HCO3- (Bicarbonate concentration)
NORMAL is 22-26
2. Plug the values into a tic-tac-toe board…
PCO2 is a breathing parameter so it is associated with a respiratory etiology
HCO3- is a metabolic parameter so it is associated with a metabolic etiology
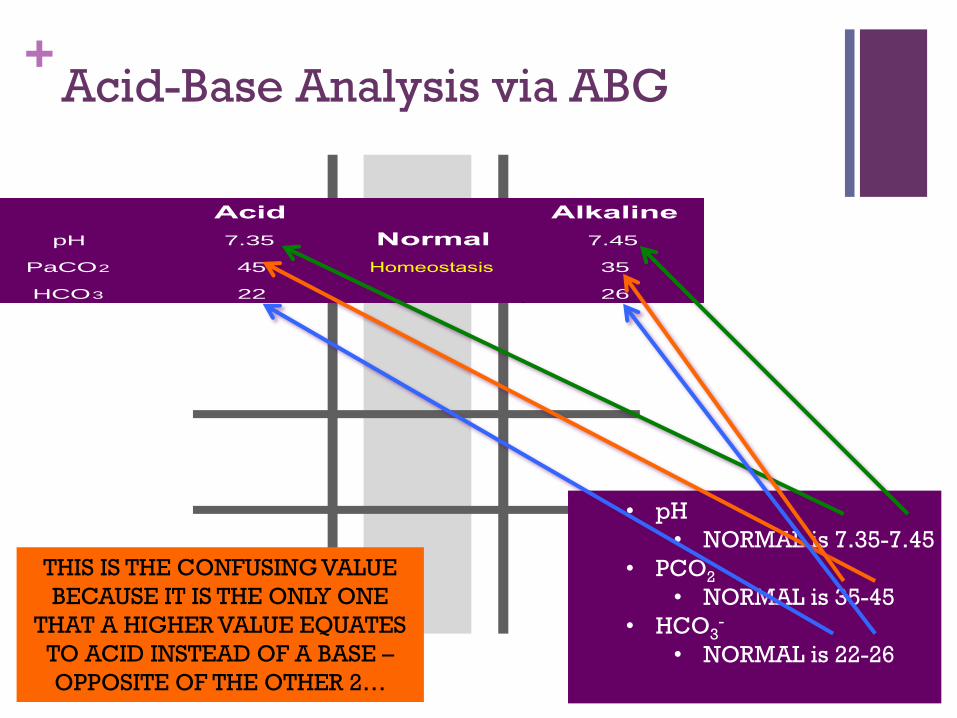
+Acid-Base Analysis via ABG
Acid Alkaline
pH 7.35 Normal 7.45
PaCO2 45 Homeostasis 35
HCO3 22 26
• pH
• NORMAL is 7.35-7.45
• PCO2
• NORMAL is 35-45
• HCO3-
• NORMAL is 22-26
THIS IS THE CONFUSING VALUE
BECAUSE IT IS THE ONLY ONE
THAT A HIGHER VALUE EQUATES
TO ACID INSTEAD OF A BASE –
OPPOSITE OF THE OTHER 2…
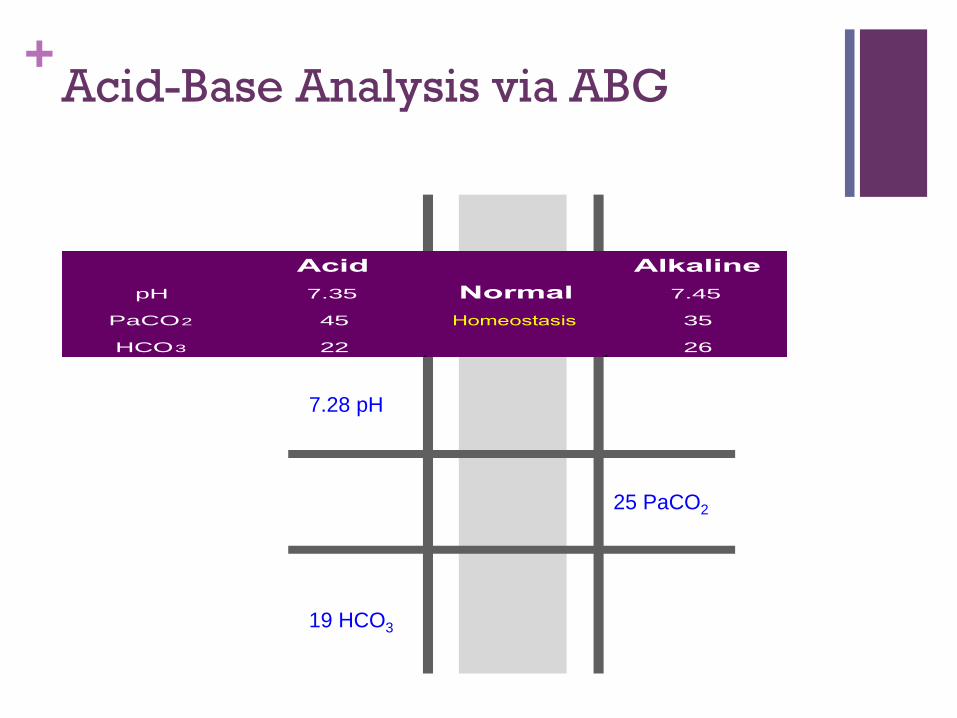
+Acid-Base Analysis via ABG
7.28 pH
25 PaCO2
19 HCO3
Acid Alkaline
pH 7.35 Normal 7.45
PaCO2 45 Homeostasis 35
HCO3 22 26
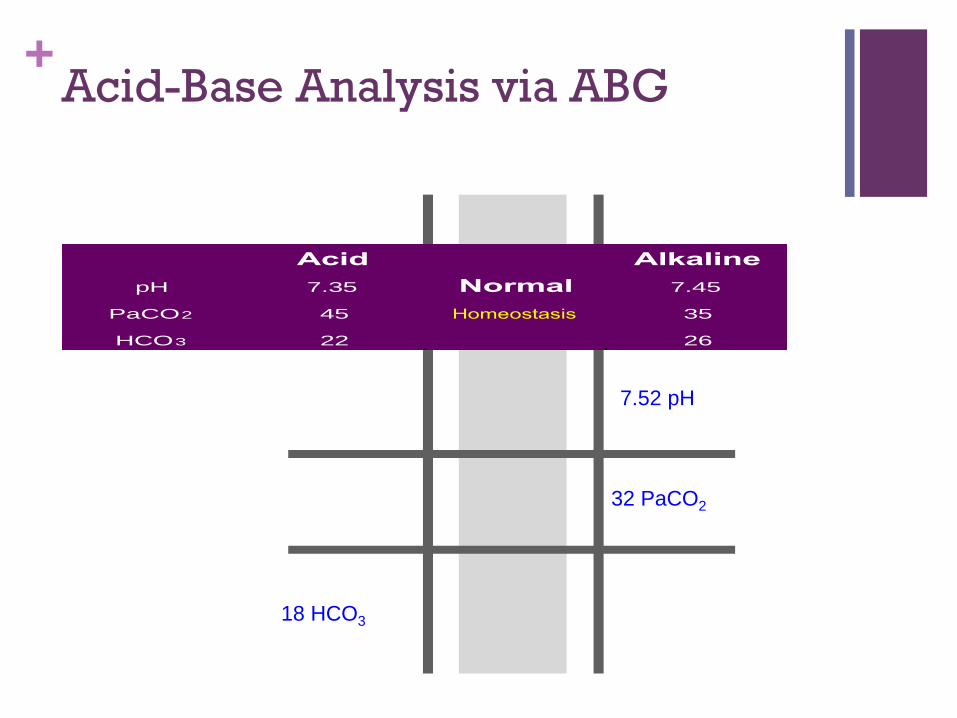
+Acid-Base Analysis via ABG
Acid Alkaline
pH 7.35 Normal 7.45
PaCO2 45 Homeostasis 35
HCO3 22 26
18 HCO3
7.52 pH
32 PaCO2
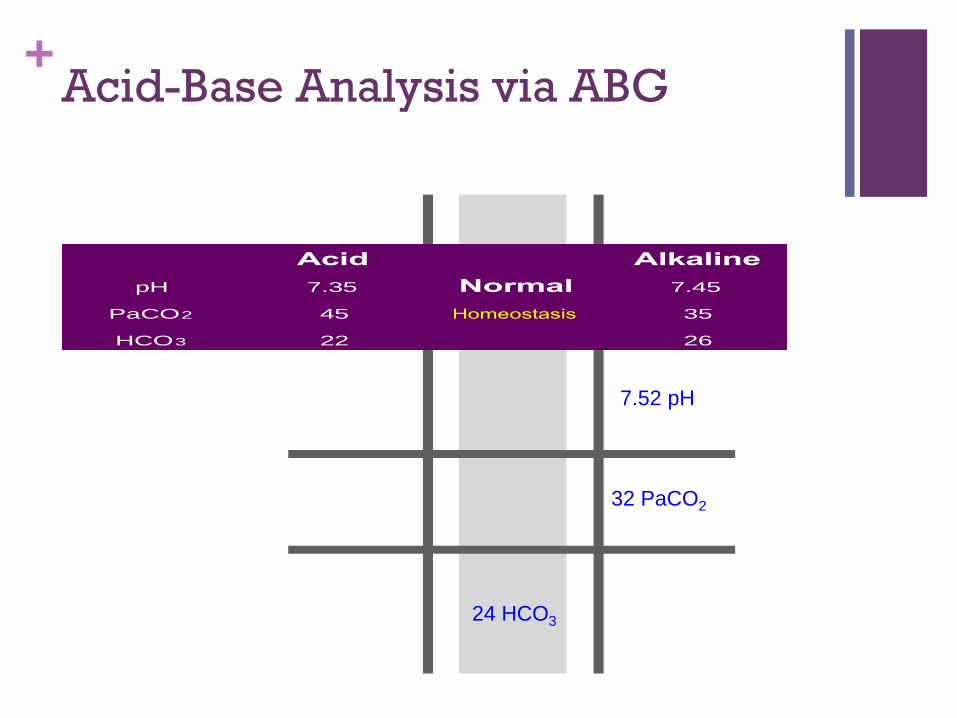
+Acid-Base Analysis via ABG
Acid Alkaline
pH 7.35 Normal 7.45
PaCO2 45 Homeostasis 35
HCO3 22 26
24 HCO3
7.52 pH
32 PaCO2
+Allen’s Test
Evaluation of collateral blood flow prior to arterial
blood draw
Nursing Intervention:
Explain the procedure
Apply pressure over the ulnar and radial arteries at the same time
Ask patient to open and close hand continually
Release ulnar artery pressure while still compressing the radial
artery
Observe the color of the extremity distal to the pressure point
Record results
Draw arterial blood sampling
+Obtaining a blood sample
Nursing Intervention:
Check physician prescription
Identify foods, medications, or other factors that could affect the
procedure
Identify the client
Explain the purpose of the test and procedure
Draw the blood sample
Apply pressure and a Band-Aid or gauze dressing to the
venipuncture
+Coagulation Studies
Activated partial thromboplastin time (________)
Evaluates how well the coagulation sequence is functioning by
measuring the amount of time it takes in seconds for recalcified
citrated plasma to clot after partial thromboplastin is added to it
Test screens for deficiencies and inhibitors of all factors except
VII and XIII
aPTT is used to monitor heparin therapy and screen for
coagulation disorders
Should be between 1.5 and 2.5 times normal when the client is
receiving heparin therapy, if the value is prolonged (longer than
90 seconds), the client is at risk for bleeding.
If the aPTT value is prolonged (>90 sec) in a client receiving IV
heparin therapy, initiate bleeding precautions.
+Coagulation studies
Prothrombin Time PT measures the amount of time (sec) for clot formation
and is used to monitor response to warfarin sodium (Coumadin) therapy or to screen for dysfunction of the extrinsic clotting system resulting from liver disease, vitamin K deficiency, or DIC
PT normal is within 2 seconds of the control
INR is used to test to measure the effects of oral anticoagulants
Values PT: 9.6 to 11.8 seconds (male adult); 9.5 to 11.3 seconds (female
adult)
INR: 2 to 3 for standard warfarin therapy
INR: 3 to 4.5 for high dose warfarin therapy
+Coagulation studies
Nursing Intervention:
A baseline PT shown be drawn before anticoagulation therapy is
initiated, note the time on the lab form
Put direct pressure to the venipuncture site for 3-5 mins
Concurrent warfarin therapy with heparin therapy can extend the
PT to 1.5 – 2 times the lab control value
A PT longer than 30 seconds can result in bleeding
+Coagulation studies
Clotting time
Time required for the interaction of all factors involved in the
clotting process
8-15 mins
No heparin therapy for 3hrs before specimen collection
Heparin therapy will affect the results
Anticoagulant therapy can falsely
Prolong the test result
Test tube agitation-?????
Exposure of the specimen to high temperatures
+Coagulation studies
Platelet count
Hemostatic plug formation
Clot retraction
Coagulation factor activation
Produced in the bone marrow
Value: 150,000 to 400,000 cells/mm3
Nurse should monitor venipuncture site for bleeding in
thrombocytopenic patients
Platelet count increased by:
High altitudes
Chronic cold weather
Exercise
+Erythrocyte studies
Erythrocute sedimentation rate
Hemoglobin and hematocrit
Serum iron
RBC count (erythrocytes)
____/_____/_____ rule (normal RBC/HGB/HCT)
+Serum enzymes and cardiac
markers
Creatinine kinase
Nurse roles:
Tell patient to avoid exercising
Troponins
Values usually lower than .6 ng/mL
Value higher than 1.5ng/mL
Could indicate myocardial infarction
Myoglobin
+Serum enzymes and cardiac
markers
Natriuretic peptides
ANP:
22 to 27 pg/mL
BNP:
Less than 100 pg/mL
The higher the BNP level
The more severe the CHF
If the BNP is raised
Dyspnea is due to CHF
If BNP is normal
Dyspnea is due to a pulmonary problem.
+Serum Gastrointestinal studies
Albumin
Alkaline phosphatase
Ammonia
Alanine aminotransferase (ALT)
Aspartate aminotransferase (AST)
Amylase
Lipase
Bilirubin
Lipids
Uric acid
+Glucose studies
Fasting glucose: 70-110 mg/dL
Glucose monitoring (capillary blood): 60-110 mg/dL
Glucose tolerance test (oral): Baseline fasting: 70-110 mg/dL
30-min fasting: 110-170 mg/dL
60-min fasting: 120-170 mg/dL
90-min fasting: 100-140 mg/dL
120-min fasting: 70-120 mg/dL
+Glucose studies
Glucose tolerance test
Tell patient to eat a high-carbohydrate (200-300g) diet for 3 days
before the test
Avoid
36 hours before test:
Alcohol
Coffee
Smoking
8 hours before the test:
Exercise
Fast 10 to 16 hours before test
+Glucose studies
Glucose tolerance test
Patients with diabetes mellitus
Do not take morning insulin or oral hypoglycemic drugs
Tell patient that the test may
Take ____________________
Require IV or oral administration of glucose
Require many blood samples
+Glucose studies
Glycosylated hemoglobin
Blood glucose bound to Hb
Hb A1c tells how well blood glucose levels have been controlled
for the past 3 to 4 months
Hyperglycemia
Cause of increase HbA1c in diabetic patients
Fasting is _____________________
+Glucose studies
Glycosylated serum albumin (fructosamine)
Reproduces avg. serum glucose levels over a period of 2 to 3 weeks
More sensitive to recent changes than HbA1c (hemoglobin A1c)
Values
Not diabetic:
2.5 to 2.7 mmol/L
Diabetic:
2 to 5 mmol/L
Fast for 12 hours before the test
+Glucose studies
Diabetes mellitus autoantibody panel
Assess insulin resistance
Recognize type 1 diabetes and patients with allergies to insulin
Value:
Less than 1:4 titer with no antibody detected
Avoid radioactive scans within 7 days of the test
No fasting required
+Real function studies
Serum creatinine
Avoid:
Exercise for 8 hours before the test
Extreme red meat intake for 24 hours before the test
Value:
0.6 to 1.3 mg/dL
+Real function studies
Urea
Normally freely filtered through the renal glomeruli
Some amount reabsorbed in the tubules and
The rest excreted in the urine
High levels shows a slowing of the GFR
Value:
8 to 25 mg/dL
BUN/CREAT ratio 10:1
+Elements
Calcium
Functions in bone formation
Nerve impulse transmission
Contraction of myocardial and skeletal muscles
Helps in blood clotting by converting prothrombin to thrombin
Value:
8.6 to 10 mg/dL
Nurse roles
Tell patient to eat a diet with normal calcium levels (800
mg/day) for 3 days before the test
+Elements
Magnesium
Indicative of metabolic activity and renal function
Needed for blood-clotting mechanism
Regulates neuromuscular activity
Acts as a cofactor
+Elements
Phosphorus
Functions in bone formation
Energy storage and release
Urinary acid-base buffering
Carbohydrate metabolism
Value:
2.7 to 4.5 mg/dL
Tell patient to fast before the test
+Thyroid studies
Values
TSH: 0.2 to 5.4 microunits/mL
T4: 5 to 12 mcg/dL
Free T4: .8 to 2.4 ng/dL
T3: 80 to 230 ng/dL
Avoid radionuclide scan within 7 days before the test
+White Blood Cell Count
Value 4,500 to 11,000 cells/mm3
___________________
Neutrophils: 1,800 – 7,800 cells/mm3
Bands – 0-700 cells/mm3
Eosinophils -0-450 cells/mm3
Basophils – 0-200 cells/mm3
Lymphocytes- 1000 – 48000 cells/mm3
Monocytes – 0-800 cells/mm3
+White Blood Cell Count
Nurse Roles
A low total WBC count with a left shift could indicate
A recovery from bone marrow depression
An infection of such intensity that the demand for neutrophils in
the tissue is higher than the capacity
High total WBC count with a left shift could be due to
Increased release of neutrophils by the BM in response to an
infection or inflammation
+White Blood Cell Count
Nurse Roles
A “shift to the _________” means that
An increased number of immature neutrophils
A “shift to the _________” means that
Cells have more than usual number of nuclear segments
Found in liver disease
Down syndrome
Megaloblastic and pernicious anemia
+Hepatitis testing
Radioimmunoassay
ELISA
Microparticle enzyme immunoassay
Serological tests for specific hepatitis virus
markers
Help in determining what specific type of hepatitis the patient has
+Hepatitis testing
Values
Hepatitis A
IgM antibody
Total antibody to hepatitis A
Hepatitis B
HBcAg
HBeAg
HBsAg
+Hepatitis testing
Values
Hepatitis C
Confirmed with antibodies against Hepatitis C
Hepatitis D antigen (HDAg)
Seen in Hepatitis A virus
Hepatitis E
IgM and IgG antibodies to Hepatitis E
+Hepatitis testing
Nurse role:
If the radioimmunoessay tecnique is being used
Within 1 week before blood test
Injection of radionuclides may result in false positive levels
+HIV and AIDS testing
Common tests include
ELISA
Western blot
IFA
ELISA
Used for screening
Western blot or IFA
Must be performed after as a confirmatory test
Repeat test _______________ later
+HIV and AIDS testing
CD4+ T cell count
Monitor progression of HIV
CD4+ count will go down as the disease gets worse
Immune system remains healthy with CD4+ T-cell counts higher
than 500 cells/L
Problems start occurring with CD4+ count is 200-499 cells/L
Severe immune system problems occur with CD4+ count is lower
than 200 cells/L
+HIV and AIDS testing
CD4-CD8 ratio
Monitors progression of disease
Normal ratio is 2:1
Viral load testing
Measures the occurrence of HIV viral genetic material (RNA) in
client’s blood
P24 antigen assay
counts the quantity of HIV viral core protein in the patient’s serum
+Urine Tests
Color: pale yellow
Odor: specific aromatic odor, similar to ammonia
Turbidity: clear
pH: 4.5-7.8
Specific gravity: 1.016 to 1.022
Glucose: <0.5 g/day
Ketones, protein, bilirubin, casts, crystals, bacteria: none
Red blood cells: <3 cells/HPF
White blood cells: < 4 cells/H
Chloride: 110-250 mEq/ 24 hr
Magnesium: 7.3 – 12.2 mg/dL
Potassium 25 – 125 mEq/ 24 hr
Sodium 40 – 220 mEq/ 24 hr
Uric acid: 250 – 750 mg/ 24 hr
+Serum medication levels
Acetaminophen (Tylenol) : 10-20 mcg/mL
Amikacin (Amikin) : 25-30 mcg/mL
Amitriptyline: 120-140 ng/mL
Carbamazepine (Tegretol): 5-12 mcg/mL
Chloramphenicol (Chloromycetin): 10-20 mcg/mL
Desipramine (Norpramin) : 150-300 ng/mL
Digoxin (Lanoxin): 0.5-2 ng/mL
Disopyramide (Norpace): 2-5 mcg/m
Ethosuximide (Zarontin): 40-100 mcg/mL
+Serum medication levels
Gentamicin: 5-10 mcg/mL
Imipramine (Tofranil): 150-300 ng/mL
Lidocaine (Xylocaine): 1.5-5 mcg/mL
Lithium (Lithobid): 0.5-1.2 mEq/L
Magnesium sulfate: 4-7 mg/dL
Phenobarbital (luminal) : 10-30 mcg/mL
Phenytoin (Dilantin): 10-20
Propranolol (Inderal): 50-100 ng/mL
Salicylate: 100-250 mcg/mL
Theophylline: 10-20 mcg/mL
+Nutrition
Carbohydrates
Sugars, starches, and cellulose provide ______ cal/g of energy
Advance normal fat metabolism
Spare protein
Increase lower GI function
+Nutrition
Carbohydrates
Food sources
Milk
Grains/ Starch
Fruits/ Fructose
Vegetables/ Cellulose
Glucose, lactose, sucrose
+Nutrition
Fats
Cholesterol, monounsaturated fats, polyunsaturated fats, saturated
fats provide _____ cal/g of energy
Protects
Internal organs
Maintain body temperature
Part of the plasma membrane
+Nutrition
Fats
Inadequate intake
Feeling cold
Skin lesions
Risk of infection
Amenorrhea
Increased intake
Obesity
Increase risk of cardiac diseases and some cancers
+Nutrition
Proteins
Amino acids are the building blocks of protein
Provide ______ cal/g of energy
Functions
Build and repair body tissues
Control fluid balance
Uphold acid-base balance
Make antibodies
Provide energy
Produce enzymes and hormones
+Nutrition
Proteins
Essential amino acids must be obtained through diet
Food sources:
Eggs
Diary products
Meat
Fish
Poultry
Insufficient protein intake can lead to malnutrition and extreme
wasting of fat and muscle tissue
+Nutrition
Vitamins
Good for life and growth processes
Maintain and regulate body functions
Fat-soluble vitamins are A,D,E, and K
They can be stored in body so have there is a risk of toxicity
The B and C vitamins are water-soluble
Excreted in the urine
+Nutrition
Vitamins
Vitamin K
Catalyst for enabling blood-clotting factors
Especially ___________________
Vitamin C
Helps in the production of collagen
Important in wound healing
Vitamin A
Helps with eyesight and epithelial linings
+Nutrition
Minerals
Part of hormones, cells, tissues, and bones
Catalysts for chemical reactions and enhancers of cell function
Deficiency can occur in chronically ill or in the hospitalized
+Therapeutic diets
Clear liquid diet
Fluids and some electrolytes to prevent dehydration
Initial feeding after complete bowel rest
Use to feed a malnourished person
Use for preparation of bowel surgery
Postoperatively in clients with fever, vomiting or diarrhea
Gastroenteritis or pancreatitis
+Therapeutic diets
Full liquid diet
Used after clear liquid diet after surgery
Clients who have trouble chewing, swallowing, or solid foods.
+Therapeutic diets
Mechanically altered diet
Texture is altered to require minimal chewing
For those who have dental problems, surgery of head and neck, or
dysphagia
Soft diet
For those who have difficulty chewing or swallowing
Clients with mouth sores should be served food at colder temp
Sour candy can increase salivary flow for those with dry mouth
+Therapeutic diets
Low-residue, _______________ diet
Least likely to form an obstruction when intestinal tract is
narrowed by inflammation or scarring or when GI motility is slow
Use in inflammatory bowel disease, partial obstructions of the
intestinal tract, gastroenteritis, diarrhea and other GI problems
+Therapeutic diets
High-residue, high-fiber diet
Used for constipation, irritable bowel syndrome, and
asymptomatic diverticular disease
Give 20 to 35 g of dietary fiber daily
Fruits, vegetables, and whole grain products are high-residue
foods
Increase fiber slowly and give adequate fluids so to avoid
abdominal discomfort
+Therapeutic diets
Cardiac diet
Atherosclerosis, DM, hyperlipidemia, hypertension, MI, nephrotic
syndrome, and renal failure
Restrict fat amount, cholesterol and salt
+Therapeutic diets
Fat-restricted diet
Use to reduce abdominal pain, steatorrhea, flatulence, and
diarrhea
Used for patients with malabsorption disorder, pancreatitis,
gallbladder disease, and GI reflux
High-calorie, _________________ diet
Used for severe stress, burns, wound healing, cancer, HIV, AIDS,
COPD, respiratory failure, or any other debilitating disease
Encourage snacks between meals
+Therapeutic diets
Carbohydrate-consistent diet
Used for patients with diabetes mellitus, hypoglycemia,
hyperglycemia, and obesity
Sodium-restricted diet
Used for hypertension, heart failure, renal disease, cardiac
disease, and liver disease
+Therapeutic diets
Protein-restricted diet
Used for renal disease and liver disease
Renal diet
Patient with acute or chronic renal failure, hemodialysis, or
peritoneal dialysis patients
+Therapeutic diets
Potassium-modified diet
Low- potassium diet
Hyperkalemia
Impaired renal function
Hypoaldosteronism
Addison’s disease
ACE inhibitor medications
Immunosuppressive meds
K+ sparing diuretics
Chronic hyperkalemia
+Therapeutic diets
Potassium-modified diet
High- potassium diet
Hypokalemia
Renal tubular acidosis
GI losses
Intracellular shifts
K+ wasting diuretics
Antibotics
Glucocorticoid excess from primary or secondary aldosteronism
Cushing’s syndrome or exogenous corticosteroid use
+Therapeutic diets
High- calcium diet Needed during bone growth and in adulthood to avoid
osteoporosis and to enable vascular contraction, vasodilation, muscle contraction, and nerve transmission
Low-Purine diet Used for gout, kidney stones, and elevated uric acid levels
Food restrictions include anchovies, herring, mackerel, sardines, scallops, and glandular meats
High- Iron diet Anemia
Organ meats, meat, egg yolks, whole wheat, dark green leafy vegetables, dried fruit, and legumes
+Therapeutic diets
___________________ diets
Lacto-Ovo
Lacto
Vegan
Pesco
Enternal Nutrition
Liquefied foods into the GI tract via a tube
Used for patients with swallowing problems, burns, major trauma,
liver or other organ failure, or severe malnutrition
+Parenteral Nutrition (PN)
Supplies nutrients thru the veins
Supplies carbohydrates in form of dextrose, fats in
an emulsified form, proteins in the form of amino
acids, vitamins, minerals, electrolytes, and water
Prevents subcutaneous fat and muscle protein from
being catabolized by the body for energy
PN is least desirable form of nutrition and used
when there is no alternative.
+Administration and discontinuation
Types of administration
Continuously over 24 hours
Most commonly used in a hospital setting
Less risk of complications when administered continuously
Intermittent PN
Generally 12-hour infusions that are usually given at night
Discontinuing PN therapy
Gradually decrease the flow rate for 1 to 2 hours while increasing
oral (this assists in preventing hypoglycemia)
+Complications
Air embolism Associated with tubing changes and central line placement
Pneumothorax Associated with central line placement
Hyperglycemia
Hypervolemia
Hypoglycemia
Infection
+Intravenous therapy
Used to sustain clients who are unable to take
substances orally
Replaces water, electrolytes, and nutrients more
rapidly than oral administration
Types of solutions
Isotonic
Hypotonic
Hypertonic
Colloids
+Intravenous devices
IV cannulas
Steel needles or butterfly sets
Plastic cannulas
The needle is .5 to 1.5 inches in length, with needle gauge sizes
from 16 to 26
IV containers
+Intravenous devices
IV gauges
For rapid emergency fluid administration, blood products, or
anesthetics
Large-diameter lumen needles or cannulas are used
14,16,18, or 19 gauge
Peripheral fat infusions (lipids)
20 or 21 gauge lumen or cannula is used
For standard IV fluid and clear liquid IV medications
22 or 24 gauge lumen or cannula
If client has small veins
24 to 25 gauge lumen or cannula is used
+Intravenous devices
IV tubing
Drip chambers Macrodrip chamber
Microdrip chamber
Filters
Needleless infusion devices
Intermittent infusion devices
Electronic IV infusion devices

+Intravenous devices
Complications
Air embolism
Catheter embolism
Circulatory overload
Electrolyte overload
Hematoma
Infection
Infiltration
Phlebitis and thrombophlebitis
Tissue damage
+Central venous catheters
Used to deliver hyperosmolar solutions, measure
central venous pressure, infuse parenteral
nutrition, or infuse multiple IV solutions or
medications
Tunneled central venous catheters
Vascular access ports
PICC line
+Epidural Catheter
Catheter is placed in the epidural space for the
administration of analgesics, this method of
administration reduces the amount needed to
control pain, therefore the client experiences
fewer side effects
Get client’s vital signs, level of consciousness, and
motor and sensory function
+Types of blood components
Packed RBC
_________________
Used to treat thrombocytopenia and platelet coagulation studies
and fibrinogen levels
White blood cells (WBCs)
Types of blood donations
Autologous
Blood salvage
Designated donor
+Compatibility
ABO type and Rh type
An antibody screen is done to determine the
presence of antibodies other than anti-A and anti-B
Crossmatching
Universal RBC donor is O negative, the universal
recipient is AB positive
+Compatibility
Complications
Transfusion reactions
Signs of an immediate transfusion reaction:
Chills and diaphoresis
Muscle aches
Back or chest pain
Allergic reactions
Hives
Itching
Swelling
Rapid, thready pulse
+Compatibility
Complications
Signs of an immediate transfusion reaction:
Dyspnea
Cough or wheezing
Pallow and cyanosis
Apprehension
Tingling and numbness
Headache
Nausea/ Vomiting/ Diarrhea
Abdominal cramping
+Compatibility complications
Signs of a transfusion reaction in an unconscious client
Weak pulse, fever, tachycardia or bradycardia, hypotension, visible
hemoglobinuria, oliguria or anuria
Delayed transfusion reactions
Signs include fever, mild jaundice, and a decreased hematocrit level
Circulatory overload
Caused by the infusion of blood at a rate too rapid for the client to tolerate
Assessment: cough, dyspnea, chest pain, and wheezing on auscultation of
the lungs, headache, hypertension, tachycardia and a bounding pulse,
distended neck veins
+Compatibility complications
Septicemia
Occurs with the transfusion of blood that is contaminated with
microorganisms
Rapid onset of chills, high fever, vomiting, diarrhea, hypotension,
shock
Iron overload
After receiving multiple blood transfusions
Vomiting, diarrhea, hypotension, altered hematological values
Tx: ___________________ (Desferal)
+Compatibility complications
Disease transmission
Hypocalcemia
Hyperkalemia





























