Embed Size (px)
Citation preview

11/5/18
1
Nursing the proned patient is
not so hARDSARDS, mechanical ventilation and the
prone positionCastro Arias, NP, MN, CNCC(c)
Objectives•Review ARDS•History•Definition•Pathophysiology
•Lung Protective Ventilation•Foundational trials•ARDSNet
•Proning•Benefits•Mechanisms
•Newer tidbits
History Lesson• First described in 1821 by Renée Laennac in Treatise on Diseases of the Chest• Fatal idiopathic pulmonary edema
• 1967 the term “respiratory distress syndrome” was coined by Ashbaugh, Bigelow, Petty & Levine• “severe respiratory distress, refractory to
oxygen, loss of lung compliance, diffuse alveolar infiltration”

11/5/18
2
More History● American-European Consensus Conference met in 1994● Develop a standardized definition
● Facilitate research in epidemiology, pathophysiology, and treatment to combat the high mortality
● ARDSNet met in 2012 and arrived at the Berlin Definition• Clarified and address deficits identified in the
previous definitions
*Ranieri et al., 2012. Acute respiratory distress syndrome: The Berlin definition
The Berlin Definition● Acuity
● An event known to cause ARDS within 7 days of presentation
● Oxygen Stratification● Removed the term Acute Lung Injury● Mild ARDS vs Moderate ARDS vs Severe ARDS
● Chest Imaging● Bilateral opacities not explained by effusions, lobar consolidation,
or nodules
● Etiology of Edema● Must be differentiated from hydrostatic or cardiogenic eddma;
though they may be superimposed on the ARDS picture. PAOP/PAWP no longer required to diagnose
● Risk Factors● Identified risks which were previously not stated

11/5/18
3
Mortality and Morbidity● Despite our increased knowledge about ARDS,
still has huge mortality ● Criteria of the Berlin Definition are better able
to predict mortality of ARDS patients than AECC
*Ranieri et al., 2012. Acute respiratory distress syndrome: The Berlin definition
Mortality Summary● More recent estimation of mortality and morbidity range from 26-58% (Siegel, 2016)
● Surviving through ARDS does not correlate with convalescence…
Morbidity
Huge long term implications post recovery of ARDS
*Herridge et al., 2011. Functional disability 5 years after acute respiratory distress syndrome.

11/5/18
4
Morbidity
● After 5 years patients experience significant sequelae related to ARDS
● Significant costs
*Herridge et al., 2011. Functional disability 5 years after acute respiratory distress syndrome
Morbidity
● High levels of psychosocial social and physical dysfunction even after 5 years
● PTSD related syndromes post ARDS● May be amenable to ICU interventions such as
diaries
● Caregiver burden is posed as a significant issue
● Prolonged physical deconditioning related ICU-acquired weakness
Take Home Messages
• Despite being around for forever, we still are bad at treating it
• Consensus definition has helped characterize the disease, with the goal of helping research and treatment
• Huge costs: physically, psychosocially, financially

11/5/18
5
ARDS Pathophysiology
Pathophysiology● The hallmark characteristics of ARDS:● Inciting event triggers a cyclical pattern of inflammation-response-inflammation
● Increased capillary permeability due to colossal inflammatory cascade
Stages of ARDS● Three distinct phases with an anticipated trajectory and features
● Exudative● Fibroproliferative● Resolution
● There may be overlap between stages

11/5/18
6
Exudative Phase● Early stage – generally up to 72 hours, up to 6
days
● Characterized by release of pro-inflammatory cytokines● TNF-⍺, IL-1, IL-6
● Neutrophils are drawn and further propagate the immune response, further release enzymes
● All of these reactions, contribute to a leaky alveolar-capillary network
● Lymphatic system attempts to compensate, however, is rapidly overwhelmed
Fibroproliferative● May occur concurrently with exudative phase;
lasts for approximately 2 weeks after insult
● Type II alveolar cells proliferate in large numbers as fibroblasts and myofibroblasts aggregate
● Lay down new matrix, and edema slowly starts to resolve
● This stage is when lungs scar down and become fibrotic:● Increased vascular resistance, leading to right sided
heart strain● Stiff, non-compliant make it more difficult to
ventiliate
Resolution● Resolution varies with regard to final recovery,
dependent on degree of initial injury● Fibroproliferative phase may progress to fibrotic
phase that culminates in long term V/Q mismatch and ventilatory dependence
● Respiratory function may recover as pneumocytes differentiate (remember: type I and type II cells), or may result in continued permanent scarring
● Despite lung recovery, there is often a profound bio-psych-social ramifications to ARDS
11/5/18
7
Intrinsic versus Extrinsic ARDSPrimary pulmonary
injuryPneumonia
Aspiration
Inhalation injury
Pulmonary contusion
VILI
Extra-pulmonary sourcesSepsis
Pancreatitis
Trauma
DIC
Burns
BypassTRALI
Lung Protective Ventilation Breathe easy, you’ll soon be able to vent all about how long this talk is…
The Birth of ‘Lung Protective Ventilation’
The ARMA trial (2000)● Large multi-center trial in which patients with
ALI/ARDS were randomized to low tidal volume (6 ml/kg)and PPLAT <30cmH2O to traditional volumes (12 ml/kg) and PPLAT<50cmH2O
● Halted trial early
● Findings corroborated by other studies

11/5/18
8
No hARMA, no foul!
Decreases in 28 day mortality
More ventilator free days
Less end organ dysfunction
*The Acute Respiratory Distress Syndrome Network. 2000
What’s the Big Deal PEEP-ple?
The ALVEOLI trial (2004)● Tried to determine what is the ideal PEEP
for patients with ARDS● Divided in to low-PEEP (8.3±3.2 cm) and
high-PEEP (13.2±3.5 cm)
● All patients were ventilated with low VTIDALs
● The results?
ALVEOLI was a BUST!
No significance was seen in any of the major outcomes!
Better oxygenation was observed, but not of
significance
So then why do we ventilate ARDS patients
with high PEEP?
* The Acute Respiratory Distress Syndrome Network. 2000

11/5/18
9
Clinical Pearls from ARDSNet• Patient selection is key!• Recruitable lung volume = benefit from PEEP
• Potential benefits of using less oxygen• Less oxidative stress, decreased adsorption atelectasis
• Learned of the dangers of elevated plateau pressures • Try to keep them below 30cmH20 to avoid barotrauma
• Step-wise approach to PEEP and O2 titration
• The Ventilator Protocol Tool (see next)
The Ventilator Protocol Tool INCLUSION CRITERIA: Acute onset of 1. PaO2/FiO2 ≤ 300 (corrected for altitude) 2. Bilateral (patchy, diffuse, or homogeneous) infiltrates consistent with
pulmonary edema 3. No clinical evidence of left atrial hypertension PART I: VENTILATOR SETUP AND ADJUSTMENT 1. Calculate predicted body weight (PBW)
Males = 50 + 2.3 [height (inches) - 60] Females = 45.5 + 2.3 [height (inches) -60]
2. Select any ventilator mode 3. Set ventilator settings to achieve initial VT = 8 ml/kg PBW 4. Reduce VT by 1 ml/kg at intervals ≤ 2 hours until VT = 6ml/kg PBW. 5. Set initial rate to approximate baseline minute ventilation (not > 35
bpm). 6. Adjust VT and RR to achieve pH and plateau pressure goals below.
AARRDDSSnnee tt OXYGENATION GOAL: PaO2 55-80 mmHg or SpO2 88-95% Use a minimum PEEP of 5 cm H2O. Consider use of incremental FiO2/PEEP combinations such as shown below (not required) to achieve goal. Lower PEEP/higher FiO2
FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 PEEP 5 5 8 8 10 10 10 12
NIH NHLBI ARDS Clinical Network FiO2 0.7 0.8 0.9 0.9 0.9 1.0 PEEP 14 14 14 16 18 18-24 Mechanical Ventilation Protocol Summary Higher PEEP/lower FiO2 FiO2 0.3 0.3 0.3 0.3 0.3 0.4 0.4 0.5 PEEP 5 8 10 12 14 14 16 16 FiO2 0.5 0.5-0.8 0.8 0.9 1.0 1.0 PEEP 18 20 22 22 22 24 __________________________________________________________ PLATEAU PRESSURE GOAL: ≤ 30 cm H2O Check Pplat (0.5 second inspiratory pause), at least q 4h and after each change in PEEP or VT. If Pplat > 30 cm H2O: decrease VT by 1ml/kg steps (minimum = 4 ml/kg). If Pplat < 25 cm H2O and VT< 6 ml/kg, increase VT by 1 ml/kg until Pplat > 25 cm H2O or VT = 6 ml/kg. If Pplat < 30 and breath stacking or dys-synchrony occurs: may increase VT in 1ml/kg increments to 7 or 8 ml/kg if Pplat remains < 30 cm H2O.
*NIH-NHLBI ARDS Network (http://www.ardsnet.org/tools.shtml)
The Ventilator Protocol Tool _____________________________________________________________ pH GOAL: 7.30-7.45 Acidosis Management: (pH < 7.30)
If pH 7.15-7.30: Increase RR until pH > 7.30 or PaCO2 < 25 (Maximum set RR = 35). .
If pH < 7.15: Increase RR to 35. If pH remains < 7.15, VT may be increased in 1 ml/kg steps until pH > 7.15 (Pplat target of 30 may be exceeded). May give NaHCO3
Alkalosis Management: (pH > 7.45) Decrease vent rate if possible. ______________________________________________________
I: E RATIO GOAL: Recommend that duration of inspiration be < duration of expiration.
PART II: WEANING
A. Conduct a SPONTANEOUS BREATHING TRIAL daily when: 1. FiO2 ≤ 0.40 and PEEP ≤ 8 OR FiO2 < 0.50 and PEEP < 5. 2. PEEP and FiO2 ≤ values of previous day. 3. Patient has acceptable spontaneous breathing efforts. (May
decrease vent rate by 50% for 5 minutes to detect effort.) 4. Systolic BP ≥ 90 mmHg without vasopressor support. 5. No neuromuscular blocking agents or blockade.
B. SPONTANEOUS BREATHING TRIAL (SBT): If all above criteria are met and subject has been in the study for at least 12 hours, initiate a trial of UP TO 120 minutes of spontaneous breathing with FiO2 < 0.5 and PEEP < 5:
1. Place on T-piece, trach collar, or CPAP ≤ 5 cm H2O with PS < 5 2. Assess for tolerance as below for up to two hours.
a. SpO2 ≥ 90: and/or PaO2 ≥ 60 mmHg b. Spontaneous VT ≥ 4 ml/kg PBW c. RR ≤ 35/min d. pH ≥ 7.3 e. No respiratory distress (distress= 2 or more)
¾ HR > 120% of baseline ¾ Marked accessory muscle use ¾ Abdominal paradox ¾ Diaphoresis ¾ Marked dyspnea
3. If tolerated for at least 30 minutes, consider extubation. 4. If not tolerated resume pre-weaning settings.
Definition of UNASSISTED BREATHING(Different from the spontaneous breathing
criteria as PS is not allowed)
1. Extubated with face mask, nasal prong oxygen, or room air, OR
2. T-tube breathing, OR 3. Tracheostomy mask breathing, OR 4. CPAP less than or equal to 5 cm H20 without
pressure support or IMV assistance.
*NIH-NHLBI ARDS Network (http://www.ardsnet.org/tools.shtml)

11/5/18
10
VILI or VALI
● Ventilator induced lung injury versus ventilator associated lung injury ● Induced - injury cause by mechanical ventilation● Associated -injury from mechanical ventilation or
disease state
● Many types:● Barotrauma - from too much pressure● Volutrauma - from too much volume● Atelectrauma - injury from repeated opening ● Biotrauma - injury causing release of cytokines,
further exacerbating injury
VILI and the Prone Patient ● Tends to occur in dependent areas;
remember that dependent areas are less compliant
● Prone position homogenizes driving pressure● Prone position recruits more lung volume● Prone position with ARDSNet ventilation
(high PEEP, low tidal volume)● Prone position allows less oxygen usage
What is the Prone Position● Simply put, the prone position involves
placing a patient facedown. ● Not so simple to execute in reality● Many studies demonstrated this previously,
but not all demonstrated an improvement of mortality
● Previously may have been used as salvage maneuver, therefore, did not demonstrate a benefit

11/5/18
11
The PROSEVA Trial
Demonstrated improvements in oxygenation, and improvements in 28-day & 90-day mortality
*Guérin et al., 2013. Prone positioning in severe acute respiratory distress syndrome.
Prone PositioningWhat are the benefits?
● Added a protocolized approach of which to emulate which allowed for wide range implementation
● Euoxia is dependent on both improved ventilation and respiration
● Improves shunt away from the dorsal (dependent) regions of the lungs
● Improved aeration of a larger volume of lung parenchyma
Proning Benefits -Continued● Decreased in shunt, as the right ventricle is able to pump blood into a higher surface area of aerated tissue
● Utilization of endogenous nitric oxide● Improved fluid clearance● decreased compression of lymphatic vessels● recruitment maneuvers may stimulate fluid
clearance

11/5/18
12
Timing is Everything● Early rather than later cited as having the
largest benefit● Helps with secretion clearance (postural
drainage)● Reduction of edema● Prevents VILI● Reduces oxidative stress
● How long is optimal?● Unclear, but more research is being done● PROSEVA had a mean of 17 hours, durations up to
55hrs have been studied in some centers
Figure 1. Strain stress from Kallet, R. H. (2015). A comprehensive review of prone position in ARDS.
APRV with ARDS
•“APRV is a mode of mechanical ventilation that has generated enough controversy to fuel a war”
• Mireles-Cabodevila, Dugar, & Chatburn, 2018
•Putative benefits reducing atelectrauma, reducing biotrauma
•Enhanced recruitment
11/5/18
13
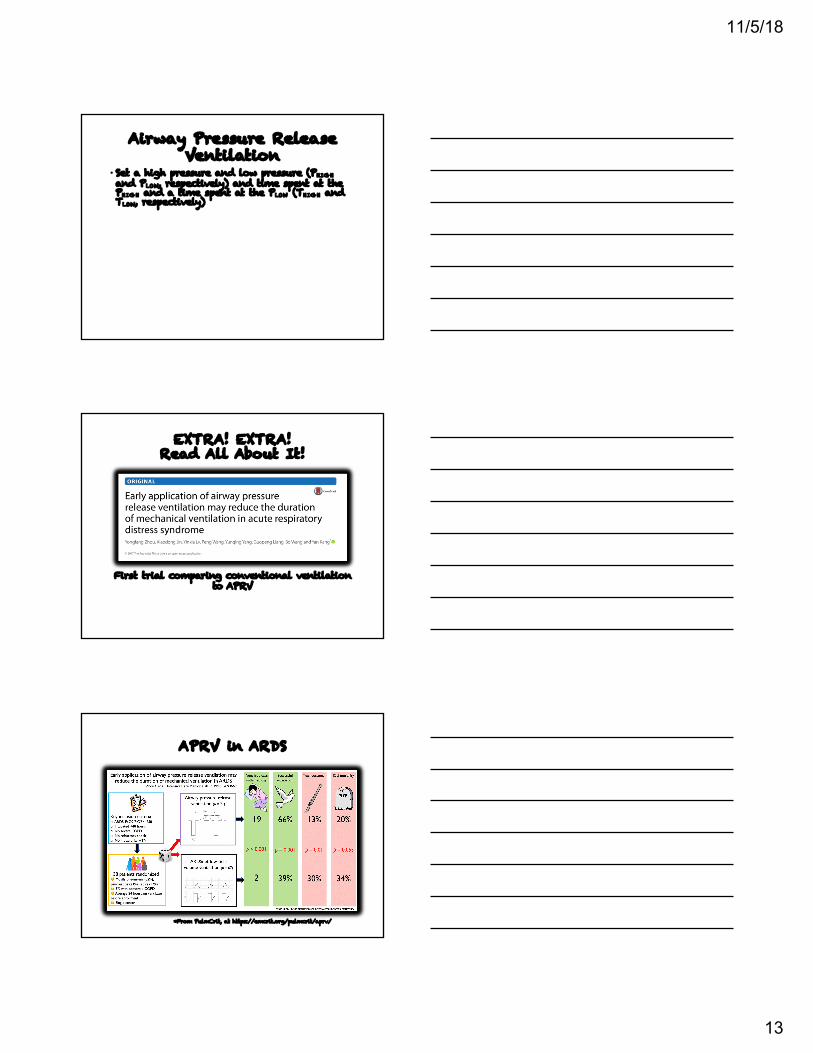
Airway Pressure Release Ventilation
• Set a high pressure and low pressure (PHIGHand PLOW, respectively) and time spent at the PHIGH and a time spent at the PLOW (THIGH and TLOW, respectively)
EXTRA! EXTRA! Read All About It!
First trial comparing conventional ventilation to APRV
APRV in ARDS
*From PulmCrit, at https://emcrit.org/pulmcrit/aprv/

11/5/18
14
Everyone’s a Critic
•Populations problems
•High Failure to extubate
•RRT Protocol
•More study is needed
ECMO in ARDS
•CESAR Trial in 2009•ECMO is effective at improving outcomes at 60 days in patient with ARDS •Thought to give the lungs an opportunity to rest with ventilation to minimalize VILI
EOLIA Trial (2018)
Does early ECMO make a difference at improving outcomes/mortality?

11/5/18
15
ECMO in ARDS
• At 60 days:• 46 % survival in ECMO group• 35% in the ventilated group
• But 11% difference NOT significant
• ECMO had more bleeding requiring transfusion and severe thrombocytopenia
Combes et al., 2018
What else do we know?
•Conservative fluid volume is helpful• Fluid and Catheter Treatment Trial (FACTT)
•NMBAs are probably beneficial
• Inhaled pulmonary vasodilators• Improved oxygenation; no change in mortality
• Steroids? Early versus late. High-dose versus low-dose?
In Summary
•ARDS is bad
•Progress is being made with treatment
•Prone early, prone long, just prone
•New things are always coming

11/5/18
16
ReferencesAshbaugh, D. G., Bigelow, D. B., Petty, T. L., & Levine, B. E. (1967). Acute respiratory distress in adults. Lancet, 2(7511), 319-323.Beitler, J., Shaefi, S., Montesi, S., Devlin, A., Loring, S., Talmor, D., & Malhotra, A. (2014). Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta-analysis. Intensive Care Medicine, 40(3), 332-341. doi:10.1007/s00134-013-3194-3 Bernard, G. R., Artigas, A., Brigham, K. L., Carlet, J., Falke, K., Hudson, L., & ... Spragg, R. (1994). The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. American Journal Of Respiratory And Critical Care Medicine, 149(3), 818-824.Combes, A., Hajage, D., Capellier, G., Demoule, A., Lavoué, S., Guervilly, C., … Mercat, A. (2018). Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. The New England Journal Of Medicine, 378(21), 1965–1975. https://doi-org.login.ezproxy.library.ualberta.ca/10.1056/NEJMoa1800385Constantin, J., Cayot-Constantin, S., Roszyk, L., Futier, E., Sapin, V., Dastugue, B., & ... Rouby, J. (2007). Response to recruitment maneuver influences net alveolar fluid clearance in acute respiratory distress syndrome. Anesthesiology, 106(5), 944-951.Daoud, E. (2007). Airway pressure release ventilation. Annals Of Thoracic Medicine, Vol 2, Issue 4, 176-179 (2007), (4), 17Drahnak, D. M., Custer, N., (2015). Prone positioning of patients with acute respiratory distress syndrome. Critical Care Nurse, 35(6), 29-37. doi:10.4037/ccn2015753Gattinoni, L., Taccone, P., Carlesso, E., & Marini, J. (2013). Prone position in acute respiratory distress syndrome. Rationale, indications, and limits. American Journal Of Respiratory & Critical Care Medicine, 188(11), 1286-1293. doi:10.1164/rccm.201308-1532CIGattinoni, L., Tognoni, G., Pesenti, A., Taccone, P., Mascheroni, D., Labarta, V., & ... Latini, R. (2001). Effect of prone positioning on the survival of patients with acute respiratory failure. New England Journal Of Medicine, 345(8), 568-573.
ReferencesGirard, R., Baboi, L., Ayzac, L., Richard, J., & Guérin, C. (2014). The impact of patient positioning on pressure ulcers in patients with severe ARDS: Results from a multicentre randomised controlled trial on prone positioning. Intensive Care Medicine, 40(3), 397-403. doi:10.1007/s00134-013-3188-1Grissom, C. K., Hirshberg, E. L., Dickerson, J. B., Brown, S. M., Lanspa, M. J., Liu, K. D., & ... Miller, R. (2015). Fluid management with a simplified conservative protocol for the acute respiratory distress syndrome. Critical Care Medicine, 43(2), 288-295. doi:10.1097/CCM.0000000000000715Guérin, C., Reignier, J., Richard, J., Beuret, P., Gacouin, A., Boulain, T., … Ayzac, L. (2013). Prone positioning in severe acute respiratory distress syndrome. The New England Journal of Medicine, 368(23), 2159-2168. doi:10.1056/NEJMoa1214103Herridge, M. S., Tansey, C. M., Matte, A., Tomlinson, G., Diaz-Granados, N., Cooper, A., & ... Cheung, A. M. (2011). Functional disability 5 years after acute respiratory distress syndrome. The New England Journal Of Medicine, 364(13), 1293-1304.Kallet, R. H. (2015). A comprehensive review of prone position in ARDS. Respiratory Care, 60(11), 1660-1687. doi:10.4187/respcare.04271.Luks, A. M. (2013). Ventilatory strategies and supportive care in acute respiratory distress syndrome. Influenza & Other Respiratory Viruses, 3(7), 8-17. doi:10.1111/irv.12178Matthay, M. A., & Zemans, R. L. (2011). The acute respiratory distress syndrome: pathogenesis and treatment. Annual Review Of Pathology, 6. 147-163. doi:10.1146/annurev-pathol-011110-130158Maung, A. A., & Kaplan, L. J. (2011). Airway pressure release ventilation in acute respiratory distress syndrome. Critical Care Clinics, 27(3), 501-509. doi:10.1016/j.ccc.2011.05.003
ReferencesMireles-Cabodevila, E., Dugar, S., & Chatburn, R. L. (2018). APRV for ARDS: the complexities of a mode and how it affects even the best trials. Journal Of Thoracic Disease, 10S1058-S1063. doi:10.21037/jtd.2018.03.156Modrykamien, A., Chatburn, R. L., & Ashton, R. W. (2011). Airway pressure release ventilation: an alternative mode of mechanical ventilation in acute respiratory distress syndrome. Cleveland Clinic Journal Of Medicine, 78(2), 101-110. doi:10.3949/ccjm.78a.10032Neto, A. S., Pereira, V. M., Espósito, D. C., Damasceno, M. T., & Schultz, M. J. (2012). Neuromuscular blocking agents in patients with acute respiratory distress syndrome: a summary of the current evidence from three randomized controlled trials. Annals Of Intensive Care, 2(1), 33-41. doi:10.1186/2110-5820-2-33Pierrakos, C., Karanikolas, M., Scolletta, S., Karamouzos, V., & Velissaris, D. (2012). Acute respiratory distress syndrome: Pathophysiology and therapeutic options. Journal Of Clinical Medicine Research, 4(1), 7-16. doi:10.4021/jocmr761wRanieri, V., Rubenfeld, G. D., Thompson, T. B., Ferguson, N. D., Caldwell, E., Fan, E., & ... Slutsky, A. S. (2012). Acute respiratory distress syndrome: The Berlin definition. Journal Of The American Medical Association, 307(23), 2526-2533.Slutsky, A. S. (2012). Acute respiratory distress syndrome: The Berlin definition. Journal Of The American Medical Association, 307(23), 2526-2533.Rimeika, D., Nyrén, S., Wiklund, N. P., Koskela, L. R., Tørring, A., Gustafsson, L. E., & ... Wiklund, C. U. (2004). Regulation of regional lung perfusion by nitric oxide. American Journal Of Respiratory And Critical Care Medicine, 170(4), 450-455.Rubenfeld, G. D., Caldwell, E., Granton, J., Hudson, L. D., & Matthay, M. A. (1999). Clinical Investigations in Critical Care: Interobserver Variability in Applying a Radiographic Definition for ARDS. Chest, 116(5), 1347-1353. doi:10.1378/chest.116.5.1347Santa Cruz, R., Rojas, J. I., Nervi, R., Heredia, R., & Ciapponi, A. (2013). High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome. The Cochrane Database Of Systematic Reviews, 6(6), 1-61. CD009098. doi:10.1002/14651858.CD009098.pub2

11/5/18
17
ReferencesSiegel, M.D., (2016). Acute respiratory distress syndrome: Prognosis and outcomes in adults. In P.E. Parsons (Ed.), UpToDate. Retrieved from http://www.uptodate.com/contents/acute-respiratory-distress-syndrome-prognosis-and-outcomes-in-adults#referencesSud, S., Sud, M., Friedrich, J. O., & Adhikari, N. J. (2008). Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: A systematic review and meta-analysis. Canadian Medical Association Journal, 178(9). 1153.Sud, S., Sud, M., Friedrich, J. O., Meade, M. O., Ferguson, N. D., Wunsch, H., & Adhikari, N. J. (2010). High frequency oscillation in patients with acute lung injury and acute respiratory distress syndrome (ARDS): systematic review and meta-analysis. BMJ: British Medical Journal, 340(7759), 1-11Sud, S., Friedrich, J. O., Taccone, P., Polli, F., Adhikari, N. J., Latini, R., & ... Gattinoni, L. (2010). Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Medicine, 36(4), 585-599. doi:10.1007/s00134 Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. (2000). The New England Journal Of Medicine, 342(18), 1301-1308.Walkey, A. J., Summer, R., Ho, V., & Alkana, P. (2012). Acute respiratory distress syndrome: epidemiology and management approaches. Clinical Epidemiology, (1)159-169. doi:10.2147/CLERS2880 Wiedemann, H. P., Wheeler, A. P., Bernard, G. R., Thompson, B. T., Hayden, D., deBoisblanc, B., & ... Harabin, A. L. (2006). Comparison of two fluid-management strategies in acute lung injury. The New England Journal Of Medicine, 354(24), 2564-2575.





























