Embed Size (px)
Citation preview

Clinics in Dermatology (2010) 28, 686–693
Nutrition and skin diseases in veterinary medicinePatrick Hensel, Dr. med. vet.
Department of Small Animal Medicine and Surgery, College of Veterinary Medicine of the University of Georgia,501 DW Brooks Drive, Athens, GA 30602, USA
Abstract Veterinarians are confronted with a variety of food and nutrition-related skin diseases, withcutaneous food adverse reaction the most common in small animal dermatology. In addition to canineatopic dermatitis, cutaneous food adverse reaction has been an area of interest for extensive research forthe last decade. Nutritional deficiencies and toxicoses are rare these days due to commercially availablehigh-quality diets; however, poorly stored diets, inadequate husbandry of exotic pets, or problems in afarm animal environment may result in zinc, vitamin A, vitamin C, and fatty acid, or copper deficiency.Inherited deficiencies due to abnormal zinc absorption through the gastrointestinal tract must beconsidered in Nordic breed dogs and goats.© 2010 Elsevier Inc. All rights reserved.
Introduction
Veterinary dermatologists are confronted with variousfood- and nutrition-related skin diseases. The mostcommon one is cutaneous adverse food reaction (CAFR)in dogs and cats. Skin diseases caused by nutritionaldeficiencies or toxicoses are less common, but are seenin farm animals and exotic animals due to inappropriatehusbandry. Hereditary nutritional deficiencies have beenreported in Nordic breed dogs and goats. The clinicalpresentations among these diseases vary, and lesions suchas alopecia, coat discoloration, seborrhea, hyperkerato-sis, and pruritus may be seen. These diseases can affectmany animals in a herd due to husbandry-relatedproblems, or may affect a single animal, as seen withCAFR or inherited zinc-responsive dermatosis in Northernbreed dogs.
E-mail address: [email protected].
0738-081X/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.clindermatol.2010.03.031
Cutaneous food adverse reaction
Adverse food reactions are divided into two categories:immune-mediated and non-immune-mediated reactions.Although food hypersensitivity is believed to be immune-mediated, the reactions in most dogs are non-immune-mediated, which are referred to as food intolerance. Food idio-syncrasy, food toxicity, and food poisoning, anaphylactic foodreaction, pharmacologic, and metabolic food reactions are allforms of food intolerance (Figure 1). Tolerance and exclusion offood allergens requires an intact gastrointestinal (GI) barrier,which is supported by four mechanisms within the GI wall:
1. integrity of the mucosal barrier provided by morphol-ogy and functionality of the enterocytes, presence ofimmunoglobulin (Ig) A, effective digestion, quality andcomposition of the food, and presence of inflammation;
2. immune response regulated by M cells in the Peyerpatches;
3. elimination of formed immune complex through themononuclear phagocytic system of the liver and themesenteric lymph nodes;

Fig. 1 Classification of adverse food reaction. CAFR, Cutaneousadverse food reaction; Ig, immunoglobulin.
687Nutrition, skin diseases in veterinary medicine
4. tolerance of antigens reaching the mucosa provided bythe suppressor function of the gut associated lymphoidtissue (GALT).1,2
CAFR in dogs and cats caused by a hypersensitivity hasbeen associated most commonly with a type I hypersensi-tivity reaction; however, type III and type IV hypersensitivityare possible immunologic mechanisms.3
Theoretically, any food has the potential to induce adversereactions; but so far only a limited number of food ingredientshave been identified in veterinary medicine. Many differentfood ingredients are used and are commonly combined incommercially available dog and cat foods, which makes theidentification of a specific food allergen very difficult.Several studies determined that the most common foodsresponsible for causing CAFR are beef, dairy products,wheat, and to some degree lamb, soy, and fish in companionanimals.4-11 Food additives, such as dyes and preservatives,are also a concern, but scientific evidence could beestablished only in two cats, so far.12,13 Adverse reactionsto multiple food ingredients are not unusual and have beenidentified in 35% to 50% of food-allergic dogs and cats.14,15
Cross-reactivity among food allergens is another concern.The results of a recent study showed that bovine IgG wasidentified as a major allergen in cow's milk and appeared tobe a source of cross-reactivity with beef and probably lamb.16
CAFR is recognized as a potential cause of nonseasonalpruritic skin disease and occasional GI signs in dogs and cats.The exact prevalence of CAFR is not well established, buta few studies determined that the prevalence of CAFR indogs with nonseasonal pruritus may range between 14%and 24%.5,17,18 Sex, breed, or age predilection could notbe confirmed, but a higher risk for certain breeds, such asBoxers, West Highland White Terriers (Figure 2, A-D),retrievers, Cocker/Springer Spaniels, and others has beenreported.5,6,14,18-20 CAFR can occur at any age, and mostauthors report an age range of as early as 4 months to 14years,11 whereas other authors suggest that a contact time of1 to 2 years is necessary to develop clinical symptoms.5,6,20
The typical clinical presentation of adverse food reactionsin dogs is nonseasonal pruritus of variable intensity affecting
face, ears, feet axillae, inguinal, or perineum.5,6,14,20 CAFRoften cannot be distinguished from canine atopic dermatitis,pyoderma, Malassezia dermatitis, and skin diseases causedby ectoparasites, such as sarcoptic and demodectic mangeand fleas.3,11 Dogs also commonly present with a combina-tion of food adverse reaction, atopy, and flea bitehypersensitivity.5,15,19
Depending on severity and duration, the following skinlesions can be found: erythema, papules, excoriations,epidermal collarettes, seborrhea, and otitis.5,6,14,19,20 Insevere, chronic cases, the skin becomes lichenified, accom-panied with marked hyperpigmentation, seborrhea, alopecia,secondary superficial pyoderma, and Malassezia dermatitis(Figure 2 A-D). The most common presentation in cats isgeneralized or localized pruritus around the neck and face(Figure 3), miliary dermatitis, traumatic alopecia, eosino-philic plaques, granulomas, and indolent ulcers.4,5,20-22
Diagnosing a food adverse reaction in veterinarymedicine can be very challenging and depends heavily oncorrect food selection, food trial duration, and ownereducation and compliance. Several attempts have beenmade to find a valuable method to diagnose CAFR, but themost effective diagnostic method in dogs and cats is still astrict elimination diet trial.7,17,23-29 Challenging the petwith its previous diet and a relapse of the clinical signs isconsidered necessary to confirm the CAFR. Because manyowners are reluctant to challenge their pet with their previousdiet, CAFR can also be identified by adding a singleingredient to the elimination diet for 1 to 2 weeks.7,26 Ifno relapse is observed, the ingredient is considered safe togive. It is very important during an elimination diet trialthat no treats, table food, flavored heartworm and fleapreventatives, or medication with gelatin capsules are fedto the animal.3,26 Although most dogs and cats respondwithin 3 to 4 weeks into a diet trial, improvement issometimes not seen for 10 to 13 weeks.5,14,15,19,30
The three groups of elimination diets used in veterinarymedicine are home-cooked diets, commercially availablenovel protein diets, and hydrolyzed protein diets. Home-cooked diets are considered superior due to the lack ofadditives and by-products but are difficult to balancenutritionally, especially for long-term management, andmay be more time consuming to prepare, which may have anegative effect on owner compliance. Study results indicatethat home-cooked diets may be more effective thancommercially available equivalents.4,6,28,31
Commercially available novel protein diets are com-posed of a single protein that is not used in over-the-counterdiets, and a carbohydrate source, such as potato and oroatmeal. Venison, duck, rabbit, and kangaroo are currentlyused as novel protein sources in commercial veterinaryprescription diets.
Commercial hydrolyzed diets are considered real hypo-allergenic diets and results from studies indicate that, forexample, dogs sensitive to soy did not develop a reactionto hydrolyzed soy.23,32 In up to 50% of dogs with CARF,

Fig. 2 A-D, Chronic cutaneous food adverse reaction in a West Highlight White Terrier: marked lichenification, hyperpigmentation,erythema, and alopecia on ventrum and front and hind legs.
688 P. Hensel
a partially hydrolyzed diet may worsen the clinical signsand so it must be concluded that hydrolyzed prescriptiondiets may reduce but do not eliminate immunologic andclinical allergenicity.33
Despite these concerns, the use of hydrolyzed diets forthe diagnosis of CAFR in dogs and cats became morepopular, especially because diets containing hydrolyzedchicken liver, casein, or soy have become commerciallyavailable.26 An evaluation of the efficacy of theseveterinary prescription diets reported a success rate of60% to 75%.11,34 Concurrent complications, such assuperficial pyoderma, Malassezia dermatitis, or bacterialor yeast otitis externa, often need to be treated at the sametime the elimination diet trial is instituted. Because some ofthese patients are severely pruritic, anti-inflammatorytherapy is necessary. Symptomatic therapy must bediscontinued for the last 2 to 3 weeks of the diet trial toassess effectively the response to the elimination diet.26
The prognosis of CFAR is very good if the offendingallergen is identified and as long as patient and ownercompliance is guaranteed. Occasional recurrences of theskin problems may occur because some patients maybecome sensitive to the new protein after 2 to 3 years.30
Whether animals can become tolerant to a food allergenafter an extended period of avoidance, as reported in people,has not been proven, but natural hyposensitization seems tobe rare.
Zinc-responsive dermatosis
Zinc is an important mineral for many critical biologicfunctions, such as cellular metabolism, which is crucial forthe maintenance of a healthy coat and skin.35,36 Zincdeficiency is rare but has been reported in various species,

Fig. 3 Cutaneous food adverse reaction: severe facial pruritusresulting in extensive excoriations and alopecia in a cat.
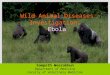
Fig. 5 Zinc-responsive dermatosis: marked lichenification,hyperpigmentation, and hyperkeratosis on the cranioventral chestof an alpaca.
689Nutrition, skin diseases in veterinary medicine
including dogs, goats, sheep, alpacas, llamas, and horses.37-44
Goats, South American camelids, and Nordic breed dogs,such as Siberian Huskies and Alaskan Malamutes, seem tobe affected more commonly.36,37,39-41
Zinc-responsive dermatosis has been divided in twosyndromes: syndrome I is considered to be a hereditary zincdeficiency resulting in decreased capability of absorbing zincfrom the intestines seen in the Nordic breed dogs andprobably in goats.40,45 Skin lesions develop despite suffi-cient dietary zinc and most commonly appear in young-adultdogs.35 Syndrome II occurs in puppies of fast-growingbreeds, such as Great Dane, Doberman Pinscher, GermanShepherd, or Labrador Retriever, or in young-adult animalsfed a zinc-deficient diet.46
Early skin lesions demonstrate erythema, followed byalopecia and crusting around the muzzle, eyes, and ears
Fig. 4 Zinc-responsive dermatosis: facial alopecia and hyper-keratosis in a Bernese Mountain Dog. (Photo courtesy of C. Sousa.)
(Figure 4). Hyperkeratosis may also develop in areas suchas the anus, vulva, prepuce, scrotum, and footpads. Ingoats, llamas, and alpacas, the hyperkeratosis tends tobe more severe, hard, and dry, affecting mainly thedorsum, legs, udder, face, and ears (Figure 5).36,40,43
Pruritus may also develop, especially after the developmentof secondary pyoderma.
In either syndrome, serum or hair zinc levels may beabnormal. Alpacas and llamas, in general, have lowerserum zinc concentrations than do sheep and goats, with noobvious difference between animals with or without skinlesions, which makes proper interpretation of serum testresults difficult.36,43
Diagnosis is made by the assessment of a completehistory, physical examination, and skin biopsy specimens.The characteristic histologic finding in dogs is a markeddiffuse and epidermal/follicular parakeratosis, whereas ingoats and alpacas/llamas, a mixed (parakeratotic andorthokeratotic) epidermal and follicular hyperkeratosis isusually present.36,40,43 Superficial perivascular dermatitiscan be found in all species.
Zinc supplementation in animals with syndrome IIusually results in a good response and resolution of the skinlesions within 2 to 6 weeks. Most common preparations forthe treatment of zinc-responsive dermatosis are elementalzinc (2 to 3 mg/kg/d), zinc sulfate (10 mg/kg/d), zincgluconate (5 mg/kg/d), or zinc methionine (1.7 mg/kg/d).36,39
In patients with lack of response to oral zinc supplementation,intravenous injection with sterile zinc sulfate (10 to 15 mg/kg) has been effective.47 Zinc supplementation for patientswith syndrome I is typically lifelong.

Fig. 7 Vitamin A deficiency: nostril distortion and rhinolith dueto squamous metaplasia in an African gray parrot. (Photo courtesyof S. Divers.)
690 P. Hensel
Vitamin A-responsive dermatosis andvitamin A deficiency
Deficiency, as well as excessive supplementation ofvitamin A, has been associated with skin lesions, such aspoor coat quality, alopecia, seborrhea, crusting, increasedsusceptibility of secondary pyoderma,Malassezia dermatitis,and poor wound healing in dogs, horses, caged birds,and reptiles.36,48,49
Vitamin A-responsive dermatosis in dogs is a rarecondition characterized by an abnormality of cornificationthat occurs in adult dogs, predominantly Cocker Spaniels,but also in Labrador Retrievers and miniature Schnau-zers.36,50 Owing to the breed-specific occurrence, ahereditary etiology is suspected, but the mode ofinheritance is not known. The skin lesions typically pre-sent as multifocal areas of alopecia, erythematous plaques,scaling, crusting, follicular plugging with frond-likekeratinous debris mainly localized on the ventral andlateral chest (Figure 6), and ceruminous otitis. Analysis ofskin biopsy specimens combined with vitamin A supple-mentation is routinely used to confirm the diagnosis of avitamin A-responsive dermatosis.50 The histopathologichallmark of vitamin A-responsive dermatosis is orthoker-atotic epidermal and predominantly follicular hyperkera-tosis. Therapy consists of oral supplementation of 10,000IU of vitamin A (retinol), once daily with food. Aresponse and clinical resolution to therapy should be seenwithin 3 to 8 weeks. Treatment must be continued and islifelong for most patients.
Vitamin A deficiency in captive reptiles and caged birds,especially parrots, is common when nutritional require-ments are not met. Seeds are commonly deficient in vitaminA, and so birds fed seeds exclusively often develop adeficiency resulting in hyperkeratotic skin, white plaques in
Fig. 6 Vitamin A-responsive dermatosis: marked ventral hyper-keratosis and seborrhea on the ventrum of an American CockerSpaniel. (Photo courtesy of C. Sousa.)
the oral mucosa, rhinitis, and blepharitis (Figure 7).51 Inreptiles, especially in box turtles, vitamin A deficiency ischaracterized by periocular edema, conjunctivitis, squamousmetaplasia, hyperkeratosis of the skin and mouth parts, andaural abscesses (Figure 8).49,52 Therapy consists of a dietchange (adding carrots and cod liver oil), and intramuscularinjections of vitamin A (2000 IU/kg in reptiles and 5000to 20,000 IU/kg in birds).49
Vitamin C deficiency
Almost all mammals, except humans and guinea pigs,produce L-ascorbic acid.53 Vitamin C deficiency is acommon problem in guinea pigs that are fed a commercial
Fig. 8 Vitamin A deficiency: conjunctivitis due to squamousmetaplasia in a box turtle. (Photo courtesy of S. Divers.)

Fig. 9 Vitamin C deficiency: ulcerative foot pad lesions and poorcoat quality in a guinea pig. (Photo courtesy of S. Divers.)
691Nutrition, skin diseases in veterinary medicine
rabbit chow or outdated commercial guinea pig chow as thesole diet.54 Guinea pigs are incapable of endogenoussynthesis of vitamin C because they are unable to producethe enzyme L-gulono-γ-lactone oxidase, which is necessaryto convert glucose to ascorbic acid.55 For this reason guineapigs have an absolute dietary daily requirement of 10 mg/kg,rising to 30 mg/kg in pregnancy.56 Skin lesions associatedwith vitamin C deficiency are cutaneous petechiae, ecchy-moses, hematomas, ulcerations, generalized seborrhea, andpoor coat quality (Figure 9).54,56 Treatment of vitamin Cdeficiency consists of correcting the diet and the adminis-tration of subcutaneous injections of vitamin C (50 to 100 mgdaily) until clinical manifestations resolve, followed bydaily oral supplementation.56,57
Although vitamin C deficiency is rare in reptiles, it hasbeen associated with gingival bleeding and spontaneousskin ruptures in snakes, especially boas and pythons.49
Fig. 10 Vitamin C deficiency: generalized multifocal areas oferythema and alopecia in a calf.
Surgical repair and oral or subcutaneous daily supplemen-tation of 10 to 20 mg/kg has been used successfully tomanage this condition.
Vitamin C deficiency has also been reported in growingcalves, aged 2 to 10 weeks, fed a diet low in vitamin Ccontent.58 Skin lesions range from nonpruritic seborrhea,crusting, alopecia, easy hair epilation, erythema, petechiae,and ecchymoses, starting on the head and limbs (Figure 10).59
Fatty acid deficiency
Dogs and cats are unable to synthesize linoleic acid; thus,a dietary source is essential in both species. In addition, catsexhibit low δ-6 desaturase activity and cannot meet theirphysiologic requirement for arachidonic acid throughbiotransformation from linoleic acid.60 Consequently, lino-leic acid and arachidonic acid both are considered essentialnutrients for cats.61 Fatty acid deficiency has become raredue to the use of commercially available high-quality petdiets; however, commercial dry food that has been poorlypreserved or a home-cooked diet could potentially result infatty acid deficiency. Oxidation of fat during storage,especially at higher temperatures, is a great concern becausethe essential fatty acids are destroyed when fat becomesrancid. Animals may also develop fatty acid deficiency inassociation with intestinal malabsorption, pancreatic disease,and chronic hepatic disease.
Clinical signs may not be obvious for several months andusually start with mild scaling and loss of luster of the haircoat. Over time the degree of seborrhea increases (Figure 11)and the skin becomes more greasy and thickened, followedby secondary skin infections and pruritus.36
Specific testing methods to diagnose a fatty aciddeficiency are not available, and so a diagnosis must bemade according to the response to treatment. Therapy in
Fig. 11 Fatty acid deficiency: dry seborrhea with a dull hair coatin a dog.

692 P. Hensel
such patients consists of switching the diet to a food with ahigh fatty acid content or by adding an essential fatty acidsupplement composed of ω-6, ω-3, and vitamin E.Resolution of mild skin lesions should be observed duringa period of 3 to 8 weeks but may take up to 6 months insevere cases.
References
1. Guilford WG. Adverse reactions to food. In: Guilford WG, Center SA,Strombeck DR, editors. Strombeck’s small animal gastroenterology.3rd ed. Philadelphia: WB Saunders; 1996. p. 436-50.
2. Guilford WG. Gastrointestinal immune system. In: Guilford WG,Center SA, Strombeck DR, editors. Strombeck’s small animalgastroenterology. 3rd ed. Philadelphia: WB Saunders; 1996.p. 20-37.
3. Scott DW, Miller WH, Griffin CE. Skin immune system and allergicskin diseases. Muller and Kirk’s small animal dermatology. 6th ed.Philadelphia: WB Saunders; 2001. p. 543-666.
4. White SD, Sequoia D. Food hypersensitivity in cats: 14 cases(1982-1987). J Am Vet Med Assoc 1989;194:1679.
5. Denis S, Paradis M. L’allergie alimentaire chez le chien et le chat. 2.Etude retrospective. Méd Vét Québec 1994;24:15-20.
6. White SD. Food hypersensitivity in 30 dogs. J Am Vet Med Assoc1986;188:695-8.
7. Jeffers JG, Meyer EK, Sosis EJ. Responses of dogs with food allergiesto single-ingredient dietary provocation. J Am Vet Med Assoc1996;209:608-11.
8. Carlotti DN, Remy I, Prost C. Food allergy in dogs and cats: a reviewand report of 43 cases. Vet Dermatol 1990;1:55-62.
9. Vaden SL, Hammerberg B, Davenport DJ, et al. Food hypersensitivityreactions in soft coated wheaten terriers with protein-losing enteropathyor protein-losing nephropathy or both: gastroscopic food sensitivitytesting, dietary provocation, and fecal immunoglobulin. E J Vet InternMed 2000;14:60-7.
10. Reedy LM. Food hypersensitivity to lamb in a cat. J Am Vet Med Assoc1994;204:1039-40.
11. Roudebush P. Hypoallergenic diets for dogs and cats. In: Bonagura JD,editor. Kirk’s current veterinary therapy. 13th ed. Philadelphia: WBSaunders Company; 2000. p. 530-6.
12. Guilford WG, Markwell PJ, Jones BR, Harte JG, Wills JM. Prevalenceand causes of food sensitivity in cats with chronic pruritus, vomitingand diarrhea. J Nutrition 1998;128(Suppl):2790S-1S.
13. Guilford WG, Jones BR, Markwell PJ, Arthur DG, Harte JG. Foodhypersensitivity in cats with chronic idiopathic gastrointestinalproblems. J Vet Intern Med 2001;15:7-13.
14. Harvey RG. Food allergy and dietary intolerance in dogs: a report of25 cases. J Small Anim Pract 1993;34:175-9.
15. Paterson S. Food hypersensitivity in 20 dogs with skin andgastrointestinal signs. J Small Anim Pract 1995;36:529-34.
16. Martín Á, Sierra M, González JL, Arevalo M. Identification of allergensresponsible for canine cutaneous adverse food reactions to lamb, beefand cow’s milk. Vet Dermatol 2004;15:349-56.
17. Kunkle G, Horner S. Validity of skin testing for diagnosis of foodallergy in dogs. J Am Vet Med Assoc 1992;200:677-80.
18. Vroom MW. Een retrospectief onderzoek bij 45 West Highland whiteterriers met huidproblem. Tijdschr Diergeneeskd 1995;119:602-4.
19. Rosser EJ. Diagnosis of food allergy in dogs. J Am Vet Med Assoc1993;203:259-62.
20. Walton GS. Skin responses in the dog and cat to ingested allergens. VetRec 1967;81:709-13.
21. Medleau L, Latimer KS, Duncan JR. Food hypersensitivity in a cat.J Am Vet Med Assoc 1986;189:692-5.
22. Stogdale L, Bomzon L. Bland van den Berg P. Food allergy in cats.J Am Anim Hosp Assoc 1982;18:188-94.
23. Jackson HA, Jackson MW, Coblentz L, Hammerberg B. Evaluation ofthe clinical and allergen specific serum immunoglobulin E responses tooral challenge with cornstarch, corn, soy and a soy hydrolysate diet indogs with spontaneous food allergy. Vet Dermatol 2003;14:181-7.
24. Ackerman L. Food hypersensitivity: A rare but manageable disorder.Vet Med 1988;83:1142-8.
25. Guilford WG, Strombeck DR, Rogers Q, Frick OL, Lawoko C.Development of gastroscopic food sensitivity testing in dogs. J VetIntern Med 1994;8:414-22.
26. Jackson HA. Diagnostic technique in dermatology: the investigationand diagnosis of adverse food reactions in dogs and cats. Clin TechSmall Anim Pract 2001;16:233-5.
27. Jackson HA. Dermatologic manifestations and nutritional managementof adverse food reactions. Vet Med 2007;102:51-64.
28. Jeffers JG, Shanley KJ, Meyer EK. Diagnostic testing of dogs for foodhypersensitivity. J Am Vet Med Assoc 1991;198:245-50.
29. Mueller R, Tsohalis J. Evaluation of serum allergen-specific IgE for thediagnosis of food adverse reactions in the dog. Vet Dermatol 1998;9:167-71.
30. Fadok VA. Diagnosing and managing the food-allergic dog. CompCont Educ Pract Vet 1994;16:1541-4.
31. Leistra MHG, Willemse T. Double-blind evaluation of two commercialhypoallergenic diets in cats with adverse food reactions. J Fel Med Surg2002;4:185-8.
32. Puigdemont A, Brazís, Serra M, Fondati A. Immunologic responsesagainst hydrolyzed soy protein in dogs with experimentally induced soyhypersensitivity. Am J Vet Res 2006;67:484-8.
33. Olivry T, Bizikova P. A systemic review of the evidence of reducedallergenicity and clinical benefit of food hydrolysates in dogs withcutaneous adverse food reactions. Vet Dermatol 2010;21:32-41.
34. Groh M, Moser E. Diagnosis of food allergy in the nonseasonallysymptomatic dog using a novel antigen, low molecular weight diet: aprospective study of 29 cases. Vet Allerg Clin Immunol 1998;6:5-6.
35. Watson T. Diet and skin disease in dogs and cat. J Nutr 1998;128:2783-2789S.
36. Scott DW, Miller WH, Griffin CE. Nutritional skin diseases. Muller andKirk’s small animal dermatology. 6th ed. Philadelphia: WB Saunders;2001. p. 1112-24.
37. Colombini S, Dunstan RW. Zinc-responsive dermatosis in northern-breed dogs: 17 cases (1990-1996). J Vet Med Assoc 1997;211:451-3.
38. Colombini S. Canine zinc-responsive dermatosis. Vet Clin North AmSmall Anim Pract 1999;29:1373-83.
39. White SD, Bourdeau P, Rosychuk RA, et al. Zinc-responsive dermatosisin dogs: 41 cases and literature review. Vet Dermatol 2001;12:101-9.
40. Krametter-Froetscher R, Hauser S, Baumgartner W. Zinc-responsivedermatosis in goats suggestive of hereditary malabsorption: two fieldcases. Vet Dermatol 2005;16:269-75.
41. Nelson DR, Wolff WA, Blodgett DJ, Luecke B, Ely RW, Zachary JF.Zinc deficiency in sheep and goats: three field cases. J Am Vet MedAssoc 1984;184:1480-5.
42. Harrington DD. Clinical and pathological findings on horses fed zinc-deficient diets. Proc Symp Eq Nutr Physiol 1973;3:51.
43. Foster A, Jackson A, D’Alterio GL. Skin diseases of South Americancamelids. In Practice 2007;29:216-23.
44. Clauss M, Lendl Ch, Schramel P, Streich WJ. Skin lesions in alpacasand llamas with low zinc and copper status—a preliminary report. Vet J2004;167:302-5.
45. Kunkle GA. Zinc-responsive dermatoses in dogs. In: Kirk RW, editor.Current veterinary therapy. 7th ed. Philadelphia: WB Saunders; 1980.p. 472.
46. Ohlen B, Scott DW. Zinc responsive dermatitis in puppies. Canine Pract1986;13:2.
47. Willemse T. Zinc-responsive disorders of the dog. In: Kirk RW,Bonagura JD, editors. Kirk’s current veterinary therapy. 11th ed.Philadelphia: WB Saunders; 1992. p. 532.

693Nutrition, skin diseases in veterinary medicine
48. Hintz HF. Nutrition and skin diseases. Current therapy in equinemedicine III. Philadelphia: WB Saunders; 1992. p. 687.
49. Harkewicz KA. Dermatology of reptiles: a clinical approach todiagnosis and treatment. In: Schmidt RE, editor. The Veterinary Clinicsof North America: exotic animal practice. Philadelphia: WB Saunders;2001. p. 441-61.
50. Ihrke PJ, Goldschmidt MH. Vitamin A-responsive dermatosis in thedog. J Am Vet Med Assoc 1983;182:687-90.
51. Girling S. Skin diseases and treatment of caged birds. In: Paterson S,editor. Skin diseases of exotic pets. Oxford: Blackwell Science; 2006.p. 22-47.
52. Goodman G. Skin diseases and treatment of chelonia. In: Paterson S,editor. Skin diseases of exotic pets. Oxford: Blackwell Science; 2006.p. 118-37.
53. Horning D. Metabolism of ascorbic acid. World Rev Nutr Diet 1975;23:225-58.
54. Scott DW, Miller WH, Griffin CE. Dermatoses of pet rodents, rabbits,and ferrets. Muller and Kirk’s small animal dermatology. 6th ed.Philadelphia: WB Saunders; 2001. p. 1415-8.
55. NishikimiM,Kawai T,YagiK.Guinea pigs possess a highlymutated genefor L-gluono-(gamma)-lactone oxidase, the key enzyme for L-ascorbicacid biosynthesismissing in this species. J Biol Chem1992;267:21967-72.
56. Meredith A. Skin diseases and treatment of guinea pigs. In: Paterson S,editor. Skin diseases of exotic pets. Oxford: Blackwell Science; 2006.p. 232-50.
57. Ellis Ch, Mori M. Skin diseases of rodents and small exotic animals. In:Schmidt RE, editor. The Veterinary Clinics of North America: exoticanimal practice. Philadelphia: WB Saunders; 2001. p. 493-542.
58. Scott DW. Vitamin C-responsive dermatoses in calves. Bovine Pract1981;2:22-7.
59. Scott DW. Nutritional skin diseases. In: Scott DW, editor. Color atlasof farm animal dermatology. Malden, MA: Blackwell Publishing; 2007.p. 83-6.
60. Rivers JPW, Sinclair AJ, Crawford MA. Inability of the cat todesaturate essential fatty acids. Nature 1975;258:171-3.
61. MacDonald ML, Rogers QR, Morris JG. Role of linoleate as anessential fatty acid for the cat independent of arachidonate synthesis.J Nutr 1983;113:1422-33.