Embed Size (px)
DESCRIPTION
Nutrition Assessment The science of determining nutrition status. 1. Determine Your Nutritional Health The warning signs of poor nutritional health are often overlooked. Use this checklist to find out if you or someone you know is at nutritional risk. 2. - PowerPoint PPT Presentation
Citation preview

Nutrition Assessment
The science of determining nutrition status
1

Determine Your Nutritional Health
The warning signs of poor nutritional health are often overlooked. Use this checklist
to find out if you or someone you know is at nutritional risk.
I have an illness or condition that made me change the kind and/or
amount of food I eat.
2
I eat fewer than 2 meals per day. 3
I eat few fruits or vegetables, or milk products. 2
I have 3 or more drinks of beer, liquor or wine almost every day. 2
I have tooth or mouth problems that make it hard for me to eat. 2
2

I don't always have enough money to buy the food I need. 4
I eat alone most of the time. 1
I take 3 or more different prescribed or over-the-counter drugs a day. 1
Without wanting to, I have lost or gained 10 pounds in the last 6 months. 2
I am not always physically able to shop, cook and/or feed myself. 2
SCORES: 0–2 = good; 3–5 = moderate nutritional risk; 6 or more = high nutritional risk.
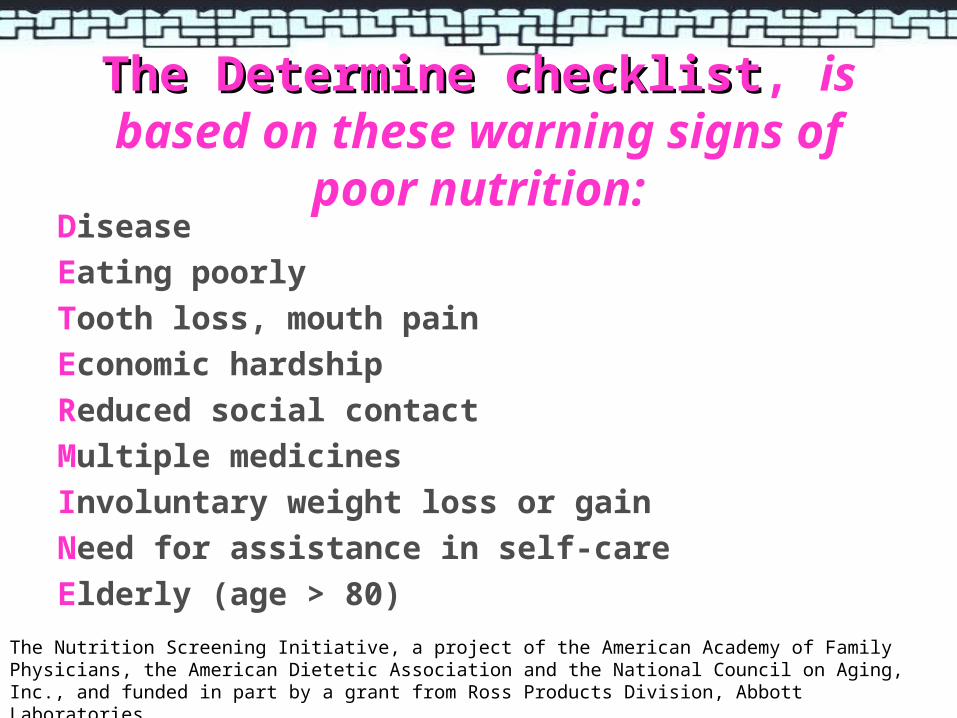
The Determine checklistThe Determine checklist, is based on these warning signs of poor nutrition:
Disease
Eating poorly
Tooth loss, mouth pain
Economic hardship
Reduced social contact
Multiple medicines
Involuntary weight loss or gain
Need for assistance in self-care
Elderly (age > 80)
The Nutrition Screening Initiative, a project of the American Academy of Family Physicians, the American Dietetic Association and the National Council on Aging, Inc., and funded in part by a grant from Ross Products Division, Abbott Laboratories.

is a comprehensive approach completed by a registered
dietitian for defining nutritional status using medical, social,
nutritional and medication histories, physical examination,
anthropometric measurements and laboratory data.
The American Dietetic Association,
Council on Practice, 1994
Nutrition Assessment

How To Assess Nutritional Status?Stages of deficiency
Inadequate food intake
Impaired absorption, utilization or transport
Decreased tissue levels
Altered physiology/biochemical functions
Signs & Symptoms of deficiency
Dietary evaluation
Biochemical & Anthropometry evaluation
Clinical evaluation
Biochemical evaluation
Assessment method
Increased requirement, destruction or excretion

Methods of Nutrition Assessment
A
B
C
D
nthropometric methods
iochemical methods
linical methods
ietary methods
Can be used alone, but more effectively in combination to provide an accurate picture of an individual’s nutrition status;Not based on a single determination but on a group or series of measurements & observations.

Nutritional Anthropometry
MeasureMeasure
1. 1. variations of the physical dimensions variations of the physical dimensions (length, weight,
proportions)
2. 2. gross composition gross composition (fat mass, fat-free mass)
of the human body at different age levels and degrees of of the human body at different age levels and degrees of
nutrition.nutrition.
Jelliffe,1966

Constructed from 2 or more raw anthropometric measurements & are ratios.
E.g. • Head circumference-for-age• Height-for-age• Weight-for-age• Weight-for-height• Weight changes
A very widely used height -weight index is body mass index (BMI)
Nutritional Assessment Indices

Body Mass Index
• For adults >20 yrs (not for pregnant / lactating )
• high correlation with estimates of body fatness, a reliable indicator of obesity (adjusted by sex, race and age)
• At the same BMI, female tend to have more body fat than male.
• At the same BMI, older people, on average, tend to have more body fat than younger adults.
• Does not distinguish excess fat from muscularity as the source of excessive body weight, so
• Highly trained athletes may have a high BMI because of ↑ muscularity rather than ↑ body fatness.
• For children 2-20 years, use BMI for age
Weight (in kilogrammes)(Height)2 (in metres)
BMI =
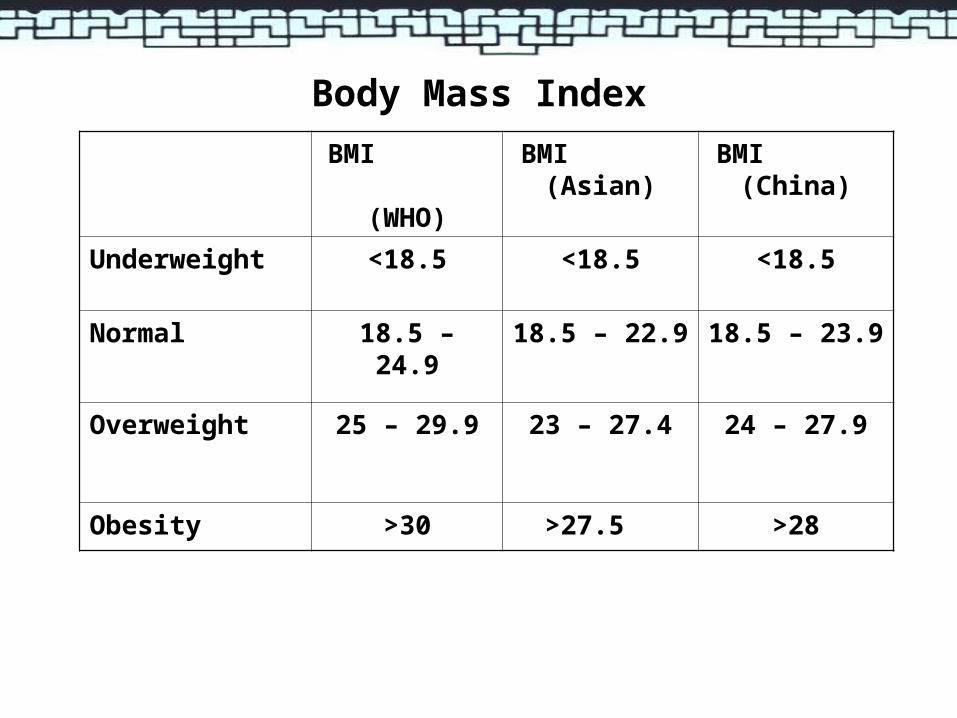
Body Mass Index
BMI (WHO)
BMI (Asian)
BMI (China)
Underweight <18.5 <18.5 <18.5
Normal 18.5 – 24.9 18.5 – 22.9 18.5 – 23.9
Overweight 25 – 29.9 23 – 27.4 24 – 27.9
Obesity >30 >27.5 >28

Evaluating Indices & Data Of Nutritional Assessment
Classification: “at risk” or “not at risk”
E.g. disease risk for type 2 diabetes, hypertension & CVDWaist Circumference (NIH): high risk in adult males > 102 cm adult females > 88 cm (NIH)
Systems available1. Reference limits from appropriate reference data: “at risk” of
malnutrition
• 2 SD above & below median reference data• below 3rd / 5th percentiles or above 97th / 95th percentiles (e.g.
growth charts)
2. Cut-off points E.g. WHO cutoff points for anemia (Hb < 120 g/L)

AnthropometryAdvantages Procedure
• Simple, safe, non-invasive
• Applicable to large sample size
Equipment – portable, inexpensive
Unskilled personnel/minimal training
Evaluate changes in nutritional status over time
Limitations
Insensitive – cannot detect
disturbance over short
periods of time
Unable to distinguish
between specific nutrient
deficiencies
Lack of appropriate
standards to compare
results

Biochemical Assessment
Lab measurements done on available body tissues, usually blood or urine
Measures
Nutrients
Nutrients metabolites
Substances that contain the nutrient (e.g. Hb for iron)
Enzymes that require the nutrient (e.g. transketolase for thiamin)
Substances that result from abnormal metabolism from a deficiency of the nutrient (e.g. elevated pyruvate levels in thiamin deficiency)
Biochemical Assessment
Provide the most objective and quantitative data on nutritional status
Can detect sub-clinical deficiency = uncovers early signs of malnutrition before alterations in anthropometric measures or clinical signs/symptoms of a deficiency disease appear
Sufficiently accurate to use as a validation method in dietary surveys
May be influenced by non-nutrition factors like disease or medication use
Clinical Assessment

Clinical Assessment
Consists of a routine medical history + nutrition-focused
physical examination
to detect signs and symptoms associated with malnutrition
Most useful during advanced stages of nutritional depletion,
usually when overt signs already present
Many physical signs are non-specific
need to interpret together with laboratory, anthropometric
and dietary data to identify the specific nutritional deficiency

☻ Non specificity of the physical signs
some may be produced by >1 nutrient deficiency or by non-nutritional factors
☻ Multiple physical signs
may exhibit multiple physical signs due to co-existing nutrient deficiencies confusion
☻ Signs may be two-directional
occur during the development of a deficiency and/or recovery
☻ Examiner inconsistencies
bias
Limitations Of Physical Examination

Dietary Assessment
To determine an individual or population’s usual dietary intake
To identify potential dietary inadequacies
To provide data on intake of nutrients or specific classes of food
Involves surveys:
measures quantity of individual foods consumed in one to several days
assesses the pattern of food used during the previous several months

Assessment methods provide qualitative or
quantitative information from food consumption
surveys
Data collected at:
National level
Household level
Individual level
Measuring Food Consumption

Methods Of Dietary Assessment Of Individuals
24-hour recall method
Estimated food records
Weighed food records
Diet history
Food Frequency Questionnaire

Subjects (their parents or caregivers) are asked to recall exact food intake
during the previous 24 hour period
Detailed description of all foods & beverages consumed, including cooking
methods and brand names (if possible) are recorded
Quantities of foods consumed are usually estimated in household measures
Photographs, food models & utensils of various types can be used as
memory aids and/or to assist in assessing portion size
The interviewer records the information for later coding and analysis
24-hour Recall Method

Conducted in 4 stages using a standardised protocol
1) recall of foods and drinks consumed
2) description of foods and drinks consumed
3) estimation of amounts – food models
4) review of interview data
24-hour Recall Method

Success depends on:
subject’s memory
ability of the respondent to convey accurate estimates
of portion size consumed
degree of motivation of the respondent
persistence of the interviewer

low respondent burden, high compliance
low cost
ease and speed of use
its administration does not alter the usual diet
can provide detailed information on types of food consumed
ideal for illiterate respondents
can be used to estimate nutrient intake of groups
reliance on memory difficult for the elderly and young children
estimation errors of food portion sizes occur (can be reduced by using graduated food models)
one recall is seldom representative of a person’s usual intake
over-report low intakes & under-report high intakes
withold/alter information because of embarrassment
data entry can be labour intensive
Advantages Limitations

The respondent records, at the time of consumption, the
identity and amounts of all foods and liquids consumed
Period of time usually 3 - 7 days
Includes information on time, place and situation of eating
Food Record / Diary

Record - time of consumption for each food
Detail description - brand names, method of preparation
Composite dish - raw ingredients, final weight of dish
Portion size – in household measurement
Convert to gram for analysis
EstimatedEstimated food recordsfood records

Most precise – requires weighing scale
Weigh all foods and beverages consumed by the subject
Details - preparation, brand names
Method is same as estimated food records except the weighing
Weighed food recordsWeighed food records
Does not depend on memory
Provides detailed intake data
Provides data about eating
habits
Multiple-day data is more
representative of usual
intake
Requires lots of co-operation
Respondent burden low
response rates
Subject must be literate
Time-consuming
Analysis is labor-intensive &
expensive
Act of recording may alter
diet
Advantages Limitations

A detailed dietary assessment
Assess individual’s usual dietary intake over extended period of time
(past month or year)
Burke’s original method involved 4 steps:
General info about health habits – smoking, exercise, appetite, use
of supplements, food dislikes, intolerances, weight history etc
24 hr recall - actual intake and general information on the overall
eating pattern
Cross check on data with specific questions about
preferences/habits e.g. diet changes
3-day food record (additional means to check the usual intake,
many omit this step)
Diet History

Assesses usual nutrient
intake
Can detect seasonal
changes
Data on all nutrients
obtained
Correlates well with
biochemical measures
Lengthy interview
Requires trained
interviewers
Difficult & expensive to
analyse
May over-estimate
nutrient intake
Requires respondent’s co-
operation
Advantages Limitations

Assesses energy/nutrient intake by determining how frequently a
person consumes a limited number of foods that are major sources
of the nutrient in question
Questionnaire consist of a list of individual food/good groups that are
important contributors to the population’s intake of energy and
nutrients
Respondents indicate how many times a day/week/month/year they
consume the foods
Food Frequency Questionnaire

Simple/non-quantitative formatSimple/non-quantitative format
• Choice of portion sizes not given, generally use ‘standard’ portion sizes –
the amount customarily eaten per serving for various age/sex groups
• E.g. how many times one eats dark bread or ice cream
Semi-quantitative formatSemi-quantitative format
• Gives respondent an idea of portion sizes
• E.g. how many times one eats a slice of dark bread or ½ cup serving of ice
cream
Quantitative formatQuantitative format
• The respondent needs to describe the size of his/her usual serving as small,
medium or large relative to a standard serving
• The information is then entered into a database which multiples the
nutrients content and arrives at an estimated nutrient intake

FFQs known as screenersscreeners have been developed to assess intake of
calcium, dietary fiber, fruits and vegetable, and percent energy
from fat.
Useful in situations that do not require assessment of the total diet
or quantitative accuracy in dietary estimates or when financial
resources are limited
Commonly used in epidemiologic research investigating the
relationship between diet and such conditions as cancer or CVD
Can be self-administered and machine readable – cost effective for
measuring diet in large epidemiologic studies

can be self-administered
machine readable
modest demand on respondents
inexpensive for large sample sizes
more representative of usual intake
than a few days of diet records
design can be based on large
population data
Considered by some to be the method
of choice for research on diet-disease
relationships
may not represent usual foods or
portion sizes chosen by
respondents
intake data can be compromised
when multiple foods are grouped
with single listings
depends on ability of subject to
describe diet
Advantages Limitations

Food Consumption Data
To calculate nutrient intakes of individuals or population
groups if quantitative methods were used to collect data
Calculation of nutrient intakes:
Manual calculations using food composition tables
Computer calculation using nutrient databases stored in
computer
Nutrient data banks or computer-stored nutrient databases are
from food composition tables transferred to and maintained on
a computer

Food Composition Tables
Printed tables contain lists of thousands of foods with the
quantities of each nutrient (values) in a standard amount
(e.g. 100g) for each food
Nutrient values are based on a quantitative analysis of
samples of each food
Data is representative of the average composition of a
particular foodstuff on a year-round, nationwide basis
Values expressed in terms of the nutrient content of the
edible portion of the food per 100g and /or per common
household measures

To compare the nutritive value of one food with another
To calculate nutritive value of any diet so as to compare that
diet with the RDA
To plan diets that must meet specific requirements e.g.
250mg sodium or 100g protein, etc
To provide a ready reference to answer questions that
people ask about foods. Proper use of
the tables can counteract much nutritional
misinformation
Uses Of Food Composition Tables

Errors in data
- random e.g. due to natural variability in the composition of the foods / processing techniques
-systematic e.g. sampling procedures or method of analysis of the foods
Limited range of foods covered Recipe variations Effect of storage on nutrient content Incorrect/ambiguous description of individual food item e.g.
prawn paste, flat bread Inconsistencies in terminology used to express certain
nutrients
Limitations Of Food Composition Tables

select appropriate food composition table
record each type of food listed during the recall
calculate the edible portion : grams or household
measures
convert into decimal fraction
multiply the nutrient values from food
composition table
total
Nutrient Analysisa) Manual calculationsa) Manual calculations

Completeness depends on range of listed food &
availability of nutrient values
Steps
• select appropriate database / nutrient
• calculate edible portion consumed
• enter data
• check input data for transcription errors
• total, averages & comparisons to RDAs can be
displayed
b) Computer calculationsb) Computer calculations

Reference values that are quantitative estimates of
nutrient intakes to be used for planning and assessing
diets for apparently healthy people
The Dietary Reference Intakes (DRIs)

The Dietary Reference Intakes (DRIs)
Include 4 reference intakes
EAR
NRI
AI = adequate intake, an observational standard that is used when
insufficient data is available to determine RDA
UL = tolerable upper intake level, highest level of daily nutrient intake that
is likely to pose no risk of adverse healthy effects to almost all apparently
healthy individuals in the general population

EARRNI
UL
Safe range of intake

USES FOR AN INDIVIDUAL FOR A GROUP
ASSESSING
INTAKES
OF APPARENTLY HEALTHY INDIVIDUALS &
GROUPS
EAR : use to examine the probability that usual intake is inadequate
RDA & AI : usual intake at or above this level has a low probability of inadequacy
UL : usual intake above this level may place an individual at risk of adverse effects from excessive nutrient intake
EAR : use to estimate prevalence of inadequate intakes within a group
RDA : do not use to assess intakes of groups
AI : mean usual intake at or above this level implies a low prevalence of inadequate intakes
UL : use to estimate the % of the population at potential risk of adverse effects from excessive nutrient intake

Indices of Diet Quality
• Refers to a food’s vitamin & mineral content relative to its energy content i.e. a nutrient dense food is one that is a good source of vitamins & minerals but relatively low in energy
• Expressed as the amount of a nutrient per 1000kcal• E.g. the deep fried broccoli will have many of the same vitamins & minerals
as the steamed one but the sauces & oil will add extra calories
• Nutrient density allows easy & quick evaluation of quality of foods & diets independently of serving size
Nutrient densityNutrient density
High nutrient dense foods Low nutrient dense foods
Broccoli, steamed, served with lemon wedges
Broccoli, batter-dipped, deep fried served with cheese sauce
Milk, nonfat, plain Milk, whole, plain
Potato, baked Potato, French fried

represents an index of adequacy for a nutrient based on the corresponding RDA for that nutrientNAR = subject’s daily intake of a nutrient
age-specific RDA of that nutrient
Example: Sally, a 15 year old teenager, has an average daily intake of 12 mg iron. The RNI for iron for teenage girls (14-16 years) is 18 mg/day.NAR = 12/18 = 0.67
Mean adequacy ratio = sum of NARs for all evaluated nutrients divided by the number of nutrients evaluated. A composite indicator for micronutrient adequacy, allows evaluation of overall adequacy of selected nutrients in the diet. Nutrient intake considered adequate if NAR > 0.67
Nutrient Adequacy Ratio (NAR)Nutrient Adequacy Ratio (NAR)

a measure of an individual’s nutrient intake in relation to the distribution of nutrient intakes of the group
does not evaluate nutrient intakes in relation to the recommended nutrient intakes
useful in longitudinal studies
Standard deviation or Z scoreStandard deviation or Z score
Average intake for nutrient X
+2 SD-2 SD
Intake values for nutrient X

• INQ = nutrient per 100 g food / RDA for the nutrient
energy per 100 g food / energy requirement
Example: Is egg or cheddar cheese a better source of protein?
Data: 100 g cheddar cheese has 25 g protein, 403 kcal
100 g eggs has 12.4 g protein, 141 kcal
For ♂ 18-30 years, NRI for protein = 65g, energy = 2100 kcal/day)
INQ (egg) = 12.4/65 INQ (c cheese) = 25/65
141/2100 403/2100
= 2.84 = 2.00
Index of Nutritional Quality (INQ)Index of Nutritional Quality (INQ)

INQ = 1 indicates that the food is an adequate source of the nutrient
INQ = 2-6 indicates that the food is a good source of the nutrient
INQ > 6 indicates that the food is an excellent source of the nutrient
→Both are good sources of protein, with eggs first, second cheddar
cheese
• Excellent rating for a single nutrient does not reflect equivalent
rating for other nutrient

Diet Quality Index (DQI)Diet Quality Index (DQI)10 indicators of quality Scoring Criteria
Total fat < 30% energy intake < 30% = 10 points, 31-40% = 5 points, > 40% = 0 points
Sat fat < 10% energy intake < 10% = 10 points, 11-13% = 5 points, > 13% = 0 points
Dietary cholesterol < 300 mg/day
< 300 mg = 10 points, 300-400 mg = 5 points, > 400 mg = 0 points
2-4 servings of fruit/day 10-0 points, proportional to % of recommended servings
3-5 servings of vegie/day
6-11 servings of grains/day
Calcium intake as % of AI 10-0 points, proportional to % of AI or RDA
Iron intake as % NRI
Dietary diversity score 10-0 points, proportional to consumption of food across 23 food group categories
Dietary moderation score 10-0 points, based on intake of added sugars, discretionary fat, sodium & alcohol in excess of recommended levels of intake
Evaluates intake of various nutrients & food components, assesses consumption of foods & food groups

Overall Evaluation
comparison of individual intakes with tables of
recommended nutrient intakes
comparison of individual food habits in relation to the
nutrition guidelines
Dietary data alone can estimate the risk for nutrient
inadequacies
Anthropometric, biochemical and clinical assessments
carried out with dietary investigation to identify
nutrient deficiency

谢谢!
资料由 PPT 中国 (www.1ppt.com) 收集提供下载,版权归原作者所有