Embed Size (px)
Citation preview

PREVENTIVE MEDICINE 12, 168- 174 (1983)
SPECIAL LECTURE
Nutrition in Coronary Heart Disease Prevention: A Program for the 1980s’
BARRY LEWIS
Department of Chemical Pathology and Metabolic Disorders, St. Thomas’ Hospital, London, England
Within a quarter century the convergence of geographical and prospective epidemiology, clinical research, and laboratory investigation has provided strongly attested theories of coronary heart disease (CHD) etiology. Evidence that application of these theories will reduce CHD incidence is incomplete but adequate to justify their use at clinical and popula- tion levels. Additional etiological hypotheses (HDL, hyperinsulinism, personality type) are persuasive but await comparable investigation. Risk-benefit considerations require ongoing scrutiny; current evidence, however, does not give cause for concern that attainable reduc- tion of plasma cholesterol has deleterious effects. To minimize lipoprotein-mediated CHD risk it may be necessary to attain population mean plasma cholesterol levels of less than 200 mg/dl, a target which is probably feasible by dietary modifications directed to lipid, fiber, and energy intake. A substantial obstacle to CHD prevention is the irresponsible rearguard action by small segments of the food industry and the medical profession, permitting inertia on the false grounds that scientific opinion is seriously divided.
That hypercholesterolemia due to elevated levels of low-density lipoprotein is causally related to atherosclerotic heart disease is a strongly attested theory. The evidence from epidemiology, clinical medicine, and laboratory studies is concor- dant and has been extensively reviewed (9, 10, 17). Predictive, cross-cultural, and case-control data indicate a direct dose-related association between plasma cho- lesterol and coronary heart disease (CHD) rates. In a recent case-control study of patients with angiographic evidence of gross coronary atheroma and of those with normal or minimally diseased vessels (Table 1) the two lipoprotein classes which discriminated between the groups were low-density lipoprotein (LDL) cholesterol (higher in the former) and high-density lipoprotein (HDL). The HDL difference was entirely due to the small HDL, subclass, mean HDL, cholesterol levels being 5.9 mg/dl in the former group and 10.4 mg/dl in the latter (13). Indices of remnant particle concentration did not differ significantly among the three groups.
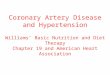
Evidence of causally significant mechanisms and considerable experimental and clinical trial data support an etiological role for high levels of LDL. Kinetic studies of LDL-apolipoprotein B have established that this lipoprotein enters the human arterial intima, the flux being directly related to plasma LDL concentration (Fig. 1) (15). This not only provides a basis for transfer of cholesterol into the arterial wall but may promote smooth muscle cell. hyperplasia (5). The development of
’ Presented at the International Symposium on Epidemiology and Prevention of Atherosclerotic Disease, June 24-26, 1981, Anacapri, Italy.
168
0091-7435/83/010168-07$03.00/O Copyright 0 1983 by Academic Press, Inc. All rights of reproduction in any form reserved.

SYMPOSIUM: ATHEROSCLEROTIC DISEASE 169
TABLE 1 LIPOPROTEIN LEVELS IN ANGIOGRAPHICALLY ASSESSED”
CORONARY ARTERY DISEASE (mg/dl) (13)
Group 1” Group 2” (n = 21) (n = 63)
Group 3” (n = 20)
Low-density lipoprotein cholesterol High-density lipoprotein cholesterol HDL, cholesterol HDL, cholesterol Cholesterol in very low and
intermediate density lipoproteins (d < 1.019)
Cholesterol: triglyceride molar ratio in d < 1.019
116k9 135 +4 133 k 8 50 t 3 48 2 2 43 t 3 10 k 1 9+1 6kl 39 k 3 39 _t 2 37 ” 3
39 2 4 46 2 3 42 k 5
1.08 k 0.09 1.08 2 0.06 1.07 + 0.14
o Angiograms were scored from 0 to 48, the highest scores reflecting the greatest severity and num- ber of stenoses. Group 1 comprised the lowest quintile of this distribution, Group 3 the highest quin- tile, and Group 2 the remaining subjects. HDL, cholesterol, Group 1 vs Group 3: P = 0.005; LDL cholesterol, Group 1 vs Group 2: P = 0.04.
atherosclerosis in primates with diet-induced hypercholesterolemia and the partial regression of such lesions when plasma cholesterol is reduced to 200 mgidl or less (18) strongly support a causal role for elevated cholesterol levels in atherosclero- sis. Regression of human atherosclerosis has been reported (1,2). In a preliminary report of a controlled trial of plasma lipid reduction by diet and drug treatment in hyperlipidemic patients with symptomatic femoral artery atheroma, angiographic evidence was obtained that plaque cross-sectional area increased to one-third of the extent in the treatment group compared with the control group; mean period between arteriograms was 19 months (4). Thus treatment favorably influenced the natural history of the disease, though regression did not occur in this severely affected group of patients within the relatively short study period.
600
1 1 .
Mean age 45 Mean age 57
0
1 . .
. . .
. . l
. .
, I 1 I
la, 150 200 250
LDL CHOLESTEROL mq I dl
FIG. 1. Flux of low-density lipoprotein (as assessed by the transfer of its apo B moiety) from plasma into human arterial intima in vivo, showing a direct relationship with plasma LDL concentration.

170 BARRY LEWIS
-London ..... .( uppsda - -Naples
4enev.a
I I 100 200 3m 4W mg I dl
SERUM CHCUSlEROL
FIG. 2. Distribution of serum cholesterol concentration in healthy persons (ages 30-49) in Naples (01, Geneva (O), London (El), and Uppsala (A).
Divergent results have been reported in the several trials of plasma lipid reduc- tion for CHD prevention. Several aspects of trial design may have contributed to this variability. One aspect may well be the extent of fall of plasma cholesterol. In trials in which the authors reported that CHD events were reduced, the mean stated change in cholesterol level was 16%, while negative or equivocal studies were associated with a change of 10.8% (8). Failure to achieve and maintain substantial lipid reduction renders several published trials unacceptable as tests of the hypothesis being investigated.
An extension of this argument is the problem of defining optimal plasma lipid and lipoprotein concentrations (3). Very low levels of LDL are compatible with health and rapid growth, as seen in human neonates, in most animal species, and in adults in low CHD risk communities. This may be due to the very high affinity of cell surface LDL receptors, permitting a supply of cholesterol to cells at low LDL concentration. The plasma cholesterol contribution seen in low-CHD, high-longevity regions such as southern Italy is a reasonable model of optimal levels, with a median of approximately 180 mg/dl in adults (Fig. 2) (7). The feasi- bility of attaining such levels in north European and north American populations (median cholesterol 210-230 mg/dl) has been investigated. A diet providing 27% energy from fat, with P/S ratio 1.0 and pectin content 5.4 g and 50% protein derived from vegetable sources (Diet C) resulted in a 29% lower plasma choles- terol than that seen during consumption of a Western diet (Diet A) in an institu- tional feeding experiment (Fig. 3) (11). The study establishes the additive nature of moderate changes in multiple dietary constituents on plasma cholesterol concen- tration.
The risk of CHD in population subgroups is directly related to serum cholesterol level (17). Hence the reasons for the wide range of serum cholesterol levels seen in

SYMPOSIUM: ATHEROSCLEROTlC DISEASE
3fJJl CHOCTSTEROC TRIGLYCERIDE HDLCHOLESTEROL
171
A BC 0 A B c D A BC 0
200 1 , LDL CHOLESTEROL VLDL TRIGLYCERIDE HDL2 CHOLESTEROL
.̂ ̂
A B C D A B C 0 A B C D
FIG. 3. Plasma lipids and lipoproteins in normal men during isocaloric dietary exchanges. (A) 40% fat, P:S 0.27, cholesterol 617 mgi2500 kcal, pectin 1.2 gi2500 kcal; (B) 27% fat, P:S 1.01, cholesterol 245 mg/2500 kcal, pectin 1.8 g/2500 kcal; (C) 27% fat, P:S 1.00, cholesterol 252 mg/2500 kcal, pectin 6.3 g/2500 kcal; (D) 40% fat, P:S 1.01, cholesterol 245 mg/2500 kcal, pectin 6.5 g/2500 kcal.
healthy populations are of great interest, but are at present incompletely iden- tified. There is considerable interindividual variation in the serum cholesterol increase induced by a short-term high-cholesterol diet (Fig. 4) (14); the magnitude of this increase is inversely related to LDL receptor activity as assessed in peripheral blood lymphocytes. Recent heritability studies on monozygotic and dizygotic twins have shown that LDL receptor activity in lymphocytes is largely genetically determined (Table 2), and hence that homeostasis, at least as affected
10
6 15mg SUPPLEMENT ,” 14 DAYS n =29 5
5
75Dmg SUPPtEMENT 3ODAYS n=14
FIG. 4. Rate of increase of serum cholesterol concentration in normal human subjects induced by dietary cholesterol supplementation.

172 BARRY LEWIS
TABLE 2A ANALYSIS OF VARIANCE OF LDL RECEPTOR ACTIVITY
OF DEREPRESSED BLOOD LYMPHOCYTES
Total mean square
Mean square Mean square among twin within twin
pairs pairs
Monozygotic 823,817 755,352 68,465 Dizygotic 1,344,619 953,277 391,342 Mean square ratio 1.632 1.262 5.716 P 0.24 0.29 <O.OOOl
by changes in dietary cholesterol intake, may be strongly influenced by polygenic inheritance (19).
Before advocating changes in diet for populations of high CHD risk com- munities, the safety of such recommendations must be scrutinized. Mortality rates from noncardiovascular disease and from cancers excluding respiratory cancer are presently falling in the United States, though less steeply than cardiovascular mortality (6). In cross-cultural comparisons, death rates from common malignan- cies (colon, breast, pancreas, lung) are directly related to saturated fat availability, and hence, it is reasonable to assume, to plasma cholesterol. By contrast, some (16, 21) but not all (3, 20) prospective studies show an inverse relationship be- tween cancer mortality and plasma cholesterol, demonstrable at cholesterol levels below 180 mg/dl. The statistical significance of the latter relationship decreases or disappears when deaths in the first l-6 years of follow-up are excluded, leading to uncertainty as to which variable is the primary one. No dose-response relation- ship is evident, the trend typically being confined to the lowest quintile of serum cholesterol. No plausible mechanism has been adduced by which low cholesterol levels could increase cancer risk. The notion that low LDL levels might lead to cell membrane compositional changes is implausible (except in familial hypobetalipoproteinemia) given an understanding of the physiology of LDL re- ceptor activity. This has been directly investigated in mononuclear cells: on incu- bation for 72 hr in various concentrations of LDL cholesterol, cell-associated free cholesterol is unaffected at a level down to 40 mg/dl; at 25 mg/dl and lower,
TABLE 2B ESTIMATES OF THE HERITABILITY OF LDL RECEPTOR
ACTIVITY OF DEREPRESSED BLOOD LYMPHOCYTES
Heritability
(MS,,, - WsmNMS,,z 0.825 rmz 0.828 adz 0.783 Xr,, - r*3 0.873 W mz - rd3/rmz 1.054 @IlIZ - T.&/Cl - TdZ) 0.717

SYMPOSIUM: ATHEROSCLEROTIC DISEASE 173
I I I t 40 &I 120
LDL CHOLESTEROL mg/l
FIG. 5. Effect of LDL concentration on free cholesterol content of blood lymphocytes following 72 hr incubation.
cell-free cholesterol content begins to decrease (Fig. 5) (12). LDL concentrations of this magnitude are not, of course, seen in normal human adults and could not be produced by diets such as described in the foregoing paragraph.
The three classical risk factors for CHD, diet-induced hypercholesterolemia due to raised LDL concentration, cigarette smoking, and hypertension can be ac- cepted on available evidence as potentially preventable and reversible causes of CHD. Implementation of this hard-won knowledge in CHD prevention, at com- munity and clinical levels, is a major task for the 1980s. Research into further risk factors, into the development of improved methods for reduction of hypercholes- terolemia and hypertension by changes in lifestyle, and into smoking cessation are among the obvious outstanding problems.
REFERENCES
1. Barndt, R., Jr., Blankenhorn, D. H., Crawford, D. W., and Brooks, S. H. Regression and progres- sion of early femoral atherosclerosis in treated hyperlipoproteinemic patients. Amer. Inr. Med. 86, l39- 146 (1977).
2. Basta, L. L., Williams, C., Kioschos, J. M., and Spector, A. A. Regression of atherosclerotic stenosing lesion of the renal arteries and spontaneous cure of systemic hypertension through control of hyperlipidemia. Amer. .I. Med. 61, 420-423 (1976).
3. Blackbum, H., Lewis, B., Wissler, R. W., and Wynder, E. L. Conference on the Health Effects of Blood Lipids. Optimal distributions for populations. Prev. Med. 8, 609-732 (1979).
4. Duffield, R. G. M., Miller, N. E., Jamieson, C. W., and Lewis, B. A controlled trial of lipid reduction in peripheral atherosclerosis. Brit. J. Surg. 69, 53-55 (1982).
5. Fischer-Dzoga, K., and Wissler, R. W. Stimulation of proliferation in stationary cultures of mon- key aortic smooth muscle cells. Atherosclerosis 24, 515-525 (1976).
6. Havlik, R. J., and Feinleib, M. (Eds.) “Proceedings of the Conference on the Decline in Coronary Heart Disease Mortality.” National Institutes of Health, Bethesda, Md., 1979.
7. Lewis, B., Chait, A., Sigurdsson, G., Mancini, M., Farinaro, E., et al. Serum lipoproteins in four European communities: A quantitative comparison. Eur. J. C/in. Invest. 8, 165% 173 (1978).
8. Lewis, B. The LDL theory and the HDL hypothesis, in “Diet and Drugs in Atherosclerosis” (G. Noseda, B. Lewis, and R. Paoletti, Eds.), pp. l-8. Raven Press, New York, 1980.
9. Lewis, B. Diet and ischaemic heart disease prevention: A policy for the eighties. Brit. Med. J. 281, 177- 180 (1980).

174 BARRY LEWIS
10. Lewis, B. Ischaemic heart disease-The scientific bases for prevention, in “Progress in Cardiol- ogy” (P. N. Yu, and J. F. Goodwin, Eds.), Vol. 10. Lea & Febiger, Philadelphia, 1981.
11. Lewis, B., Hammett, F., Katan, M., Kay, R. M., Merkx, I., et al. Towards an improved lipid- lowering diet: Additive effects of changes in nutrient intake. Lancet 2, 1310- 1313 (1981).
12. Marenah, C. B., Lewis, B., Cortese, C., Miller, N. E. and Sule, B. In preparation. 13. Miller, N. E., Hammett, F., Saltissi, S., Rao, S., van Zeller, H., et al. Relation of angiographically
defined coronary artery disease to plasma lipoprotein subfractions and apolipoproteins. Brit. Med. J. 282, 1741-1744 (1981).
14. Mistry, P., Miller, N. E., Laker, M., Hazzard, W. R., and Lewis, B. Individual variation in the effects of dietary cholesterol on plasma lipoproteins and cellular cholesterol homeostasis in man. J. C/in. Invest. 67, 493-502 (1981).
15. Niehaus, C. E., Nicoll, A., Wootton, R., Williams, B., Lewis, J., et al. Influence of lipid concen- trations and age on transfer of plasma lipoprotein into human arterial intima. Lancet 2,469-471 (1977).
16. Rose, G., Blackbum, H., Keys, A., Taylor, H. L., Kannel, W. B., et al. Colon cancer and blood cholesterol. Lancer 1, 181- 183 (1974).
17. Stamler, J. Lifestyles, major risk factors, proof and public policy. Circulation 58, 3- 19 (1978). 18. Wagner, W. D., St. Clair, R. W., and Clarkson, T. B. A study of atherosclerosis regression in
Macaca Mulatta. II. Amer. J. Pathol. 100, 633-645 (1980). 19. Weight, M., Cortese, C., Sule, U., Miller, N. E., and Lewis, B. Heritability of the low density
lipoprotein receptor activity of human blood mononuclear cells: Studies in normolipidaemic adult male twins. Chin. Sci. 62, 397-401 (1982).
20. Westlund, K., and Nicolaysen, R. Ten year mortality and morbidity related to serum cholesterol. Rand. J. Chin. Lab. Invest. 30, (Suppl. 127), l-24 (1972).
21. Williams, R. R., Sorlie, P. D., Feinleib, M., McNamara, P. M., Kannel, W. B., and Dawber, T. R. Cancer incidence by levels of cholesterol. JAMA 245, 247-252 (1981).