Embed Size (px)
Citation preview

Nutritional State and Exercise Tolerancein Patients With COPD*Paolo Palange, MD; Silvia Forte, MD; Aldo Felli, MD;Pietro Galassetti, MD; Pietro Serra, MD, FCCP; andStefano Carlone, MD
We hypothesized that in patients with COPD, poor nu-
tritional status adversely influences exercise toleranceby limiting aerobic capacity of exercising muscles. In 28patients with stable COPD, we correlated nutritionalstatus with gas exchange indexes obtained during max-
imal incremental cycle ergometer exercise and withrespiratory function parameters. On the basis of percentof ideal body weight (%LIBW), patients were dividedinto three groups (GP): GP1 (n=8, %IBW <90); GP2(n=13, %IBW '90<110); and GP3 (n=7, %IBW 2110).When compared with normally nourished individuals(GPs 2 and 3), malnourished GP1 patients showedgreater reduction in maximal workload and in peak 02
uptake (Vo2 peak), with earlier onset of metabolicacidosis (anaerobic threshold [AT]); in addition, indexesreflecting 02 cost of ventilation were higher in GPI.Nutritional status could be correlated with exercise tol-erance (Vo 2 peak, r=0.82, p<0.0001), with onset ofmetabolic acidosis (AT, r=0.69, p<0.0001) and withdead space/tidal volume ratio (VD/VT, r=-0.59,
limitation in exercise tolerance is one of the hall-> marks of patients with COPD.1-3 A patientwhose extent of disease is comparable with others, as
determined by clinical evaluation and pulmonaryfunction studies, may be unable to achieve the samelevel of physical effort: this probably reflects thecomplex pathogenesis of exercise intolerance, whichincludes a large number of variables from the centralnervous system to peripheral tissues.4'5 Clinical ob-servations suggest that exercise limitation in thesepatients is due not only to dyspnea but also to leg fa-tigue and more frequently to a combination of thesetwo subjective sensations.4 In the advanced stages ofthe disease, chronic hypoxemia to some degree is therule and often associated to a variable extent of pe-
ripheral muscle atrophy, related to deconditioningand to the general worsening of the patients' nutri-tional conditions.6 Patients with COPD reduce theirdaily activities to avoid exertional respiratory dis-comfort; this leads to impaired skeletal muscle func-tion that, in turn, reduces further physical activity.
*From the II Patologia Medica, University of Rome "La Sapien-za," Rome, Italy.
Manuscript received February 22, 1994; revision accepted Sep-tember 14.Reprint requests: Dr. Palange, II Patologia Medica, V.le Poli-clinico 155, 00161 Rome, Italy
p<0.001). Body weight was inversely correlated withindexes that are likely to reflect the increase in 02 costof ventilation. We conclude that in patients with stableCOPD, (1) malnutrition significantly affects muscleaerobic capacity and exercise tolerance, and (2) highwasted ventilation and 02 cost of ventilation may beresponsible for the weight loss.
(Chest 1995; 107:1206-12)
Key words: COPD; exercise; metabolic acidosis; nutri-tional status; 02 cost of breathing
Available evidence indicates that in patients withstable hypoxemic COPD, the aerobic capacity of theexercising muscles is limited: a reduced oxidativemetabolism has been observed by 02 uptake kineticsat submaximal workload7'8 and by 31P MRS9-12studies. Early occurrence of exercise metabolic aci-dosis13"14 has also been demonstrated. Possible causes
for the mentioned metabolic alteration may includethe following: (1) chronic reduction of oxygen supplyto the exercising muscles due to reduced arterial 02content and inadequate cardiovascular adaptation;5(2) elevated 02 cost of ventilation, which may inducea diversion of blood flow away from some nonvitalperipheral districts, described as "steal" phenome-non;15 and (3) impaired ability to utilize 02 becauseof structural and biochemical alterations within theperipheral muscles, ie, decreased mitochondrial num-ber, size, and function, faster glycogen utilizationwith lactic acid formation, and slower metabolism offree fatty acids.16
Malnutrition, defined as body weight <90% ofideal body weight,17 has been reported in as many as
25% of patients with COPD,'8 with the largest inci-dence among patients with emphysema. The clinicalrelevance of this observation resides in the well-known increase in mortality rate among malnour-
Clinical Investigations
ANOVA=analysis of variance; AT=anaerobic threshold;ATP=adenosine triphosphate; BMI=body mass index;Dco=diffusing capacity for carbon monoxide; GP=group;%LBW=percent of ideal body weight; SaO2=oxygen satu-ration; TLC=total lung capacity; TSF=triceps skinfoldthickness; Vco2=CO2 output; VD/VT=dead space/tidalvolume ratio; VE=minute ventilation; Vo2=oxygen uptake;Vo2max=maximal Vo2; Vo2/W/VE=Vo2 as a function ofmaximal workload and maximal ventilation; AVo2/AW=oxygen cost of work
1206
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

ished patients with COPD.'9-2' At the present time,the causes of malnutrition in COPD are not well un-derstood: a hypermetabolic state related to an in-crease in work of breathing and in oxygen consump-tion of the respiratory muscles has been invoked.22 Inotherwise healthy humans, malnutrition has beendemonstrated to negatively affect ventilatory andperipheral muscle strength,23 reducing the overallexercise tolerance. In patients with COPD with res-piratory failure, nutritional repletion has been provento facilitate weaning from mechanical ventilation;24in addition, nutritional repletion can improvestrength and endurance of skeletal and respiratorymuscle function in ambulatory patients with COPD.25To date, the relation between malnutrition andexercise performance has received little attention:only a few studies are available on this topic;26'27 it islikely that a compromised nutritional status canindependently worsen exercise tolerance that is al-ready reduced by ventilatory limitation.The present study was undertaken to investigate
possible interrelations between nutritional state andexercise tolerance in patients with COPD. We hy-pothesized that nutritional deficiencies adversely af-fect metabolism and function of tissues such as exer-cising muscles in a precarious biochemical andphysiologic state due to chronic 02 limitation. Clin-ical implications may be derived, indicating newtherapeutic strategies aimed at ameliorating the ex-ercise tolerance of these patients.
MATERIALS AND METHODSTwenty-eight male ambulatory patients with COPD with mild
to severe stable airways obstruction and mild hypoxemia werestudied. Admission criteria included the following: clinical diag-nosis of COPD,28 exertional dyspnea, FEV, <60% of predicted,and room air PaO2 >55 mm Hg. The pertinent clinical andfunctional characteristics of the subjects are summarized in Ta-ble 1; in 16 of the 28 patients, a physiologic pattern of predom-inant emphysema was recognizable, ie, flattening of diaphrag-matic contour and parenchymal translucency at chest radiograph,TLC >130% of predicted and RV/TLC ratio >40%, rest VD/VT>0.50. At the time of the study, no patient had sacral or ankleedema, or both. Patients also had no evidence of cor pulmonale,and of metabolic, renal, hepatic, or neuromuscular disorders. Astable regimen of bronchodilators with oral theophylline, inhaled/3-stimulant drugs, and inhaled steroids was maintained. In pa-tients receiving systemic steroids, this form of therapy was sus-
Table 1-Subjects' Pertinent Characteristics*
Characteristic Value
Age, yr 66 + 7FEV1, L/s 1.2 ±0.5FEV1, %pred 38+ 15FVC, L/s 2.7 +0.5FVC, %pred 63± 13PaO2, mm Hg 73 +11PaCO2, mm Hg 42 + 5
*Values are expressed as mean + SD.
pended at least 3 months before the experiment.The experimental protocol was approved by the Committee for
Protection of Human Subjects, University of Rome, according tothe declaration of Helsinki. Each subject signed an informedconsent prior to initiation of the study.
Nutritional Assessment
Following their arrival at the laboratory (8 AM, after a lightbreakfast), the patients voided their bladders and removed theirclothes except for underwear; weight and height were then mea-sured. In accordance with the criteria used in most studies deal-ing with patients with COPD,'9 nutritional status was assessedthrough the calculation of the percent of ideal body weight(%IBW) and of the body mass index (BMI). For %IBW, themeasured body weight was related to IBW calculated from theregression equation of weight/height for the midpoint of theweight range for a given height (from a minimal value for a smallframe size to a maximal value for a large frame), from the Met-ropolitan Insurance tables.29 To allow comparisons with otherstudies that did not use %IBW, BMI, an index independent of sex,height, and body frame, was also calculated as the ratio betweenbody weight and the square of the height (kg/m2). Triceps skin-fold thickness (TSF), determined by a skinfold caliper (HarpendenSkinfold Caliper, British Indicators Ltd), was used to estimatebody fat stores, as previously described by other authors.'8 19
Exercise Test and Measures
At 9 AM, after nutritional assessment, patients were comfortablyseated on an electrically braked cycle ergometer (Bosch, Erg 551,Germany) and fitted with nose clip and a mouthpiece with atwo-way low resistance valve. Diaphoretic electrodes were placedon the chest for monitoring of heart rate (HR) via a cardioscope(V5); a 12-lead ECG was recorded during the last 20 s of eachworkload. Arterial oxygen saturation (SaO2) was monitored by apulse oxyimeter (Biox 3740, Ohmeda, United States).
Minute ventilation (VE), oxygen uptake (Vo2), and CO2 output(Vco2) were monitored continuously using a computerized met-abolic cart. For ventilatory measurements, a pneumotachometerwas attached to the inspiratory port of the two-way valve andconnected to a ventilation monitor (P.K. Morgan, VM 2A).Expired gases were channeled to a 4.2-L mixing chamber fromwhich a continuous sample was drawn for determination of mixedexpired 02 (P.K. Morgan, Rapid Zr 02 Analyzer) and CO2 (P.K.Morgan, Infrared C02 Analyzer 901 MK2) concentrations. Out-put signals from all analyzers were translated from analog todigital, stored by an on-line microcomputer (Amstrad PC 1640DD, Korea) and used to calculate VE (BTPS), Vo2, and Vco2(STPD) every 20 s. Two sets of corrections were made for themeasurement of the gas concentrations: (1) before every exercisetest, a computerized assessment of the phase lag time for the 02and CO2 analyzers was performed, the resulting values being usedduring each exercise session; and (2) a volume correction30 wasautomatically introduced in the calculations by our software, tocompensate for the system's tubing and mixing chamber kinetics,coupling the correct 02 and CO2 values with the measured VEvalues. Calibration of gas analyzers before each test was achievedby the use of a tank of standard gas whose concentration waspreviously determined by the micro-Scholander method. After 5min for mouthpiece adaptation, an arterial blood sample wasdrawn at rest for PaO2 and PaCO2 determination; blood wasdrawn slowly to cover one or more respiratory cycles. Physiologicdead space/tidal volume ratio (VD/VT) was calculated from theBohr-Enghoff equation corrected for apparatus dead space.3'Each subject underwent a 1-min incremental exercise test: af-
ter 3 min of rest and 3 min of unloaded pedaling, workload wasincreased until exhaustion, ie, when they could no longer keep thepedaling frequency of 50 rpm. The rate of workload increment
CHEST / 107/5/ MAY, 1995 1207
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

Table 2-Anthropometric and Respiratory Function Data by % IBW*
GP1 (n=8) GP2 (n=13) GP3 (n=7)%IBW <90 %IBW .90<110 %IBW '110
%IBW 82l2fl 100+2f 115+1BMI, kg m2 18.9+ 0.5tf 23.0 + 0.4t 26.5+0.3TSF, mm 8.1±0.5it 13.1+0.5f 16.2±0.3FEV1, %pred 25±2 40+5 40+4FRC, %pred 126±4 118±5 109+3PaO2, mm Hg 68±3 72±3 75+3PaCO2, mm Hg 42+2 41+1 40±1VD/VT rest 0.54 ± 0.03f 0.50±0.02 0.43 +0.03SaO2, % 91+1 93+1 94+1
*Values are expressed as mean ± SEM.fp<0.05 vs GP3.
1p<0.05 vs GP2.
was chosen on the basis of FEVy values: FEV1.1 L, 5 W;FEV1>1<1.5 L, 10 W; FEV1. 1.5 L, 15 W. The onset of bloodlactate accumulation (anaerobic threshold [AT]) was determinedfrom a plot of Vco2 vs Vo2 (modified "V-slope method' );32 thevalue was expressed as percentage of subjects' predicted maximalVo2 (Vo2max).33 Oxygen cost of work (AVo2/ W) was deter-mined as the ratio of the increase in Vo2 (from unloaded pedal-ing to Vo2 peak) divided by the increase in workload accordingto Wasserman et al.34 Maximal absolute values of Vo2 as a func-tion of maximal workload and maximal ventilation (Vo2/W/VE)were computed. In patients with COPD, high values of AiVo22AWand Vo2/W/VE are likely to reflect an increase in the 02 cost ofventilation.
Statistical Analyses
Group data are presented as mean values + SD or SE of meanwhere appropriate. Pearson's product-moment correlation coef-ficient (r) analysis was used to detect correlations between crite-rion variables. Differences among measured parameters were
determined by analysis of variance (ANOVA); for significant re-
sults, ANOVA was followed by unpaired t tests with Bonferronicorrection. The level of statistical significance was set at p<0.05.
RESULTS
Subjects were divided into three groups, accordingto %IBW: GP1 (n=8, %IBW <90); GP2 (n=13,%IBW 290<110); and GP3 (n=7, %IBW >110).The distribution of %IBW and resting respiratoryindexes of the patient population are described inTable 2. Mean %IBW and mean BMI were statisti-cally different among the three groups. The TSF was
markedly reduced in GP1 (8.1±0.5 mm) vs GP2(13.1±0.5 mm) as well as vs GP3 (16.2±0.3 mm),p<0.05 for both, documenting that body fat mass wasreduced. Among physiologic indexes, only restingVD/VT was significantly higher in GP1.
Analysis of exercise indexes (Table 3) revealed thatthe decrement in nutritional status paralleled theprogressive reduction in exercise tolerance; the low-est values of maximal workload and Vo2 peak were
observed in the malnourished group (workload: GP1,33±4; GP2, 48±4; and GP3, 64±7 W; Vo2 peak:GP1, 0.77±0.06; GP2, 1.09±0.07; and GP3,1.43 ± 0.07 L/min).The AT was clearly visible in the vast majority of
patients (n=21); in the remaining 7 patients, AT was
not identifiable or was questionable. For statisticalanalyses, related to AT, these seven individuals were
excluded. Nutritional status paralleled the progres-sive reduction in onset of lactic acidosis: the lowestlevels were observed in the malnourished group (AT:GP1, 31+3; GP2, 40+2; and GP3, 46+6 % pre-
dicted Vo2max).Parameters reflecting 02 cost of ventilation dis-
played the same pattern. The highest values ofAiVo2/LAW and Vo2/W/VE were observed in GPI:W\o2/AW was 13.4±0.4 mL/W in GPI, 11.6±0.4in GP2, and 10.8 ± 0.2 in GP3; VO2/W/VE was
0.96 ± 0.14 mL/W/L in GP1, 0.71 ± 0.06 in GP2, and
Table 3-Exercise Indexes by %IBW*
GP1 (n=8) GP2 (n=13) GP3 (n=7)%IBW <90 %IBW '90<110 %IBW >110
Max workload, W 33±4t 48 + 4 64 + 7Vo2 peak, L/min 0.77± 0.06t 1.09+ 0.07f 1.43+0.07AT, % pred Vo2max 31±3(n=5) 40±2(n=10) 46+6(n=6)ALo2/AW, mL/W 13.4± 0.4 t 11.6+0.4 10.8+0.2Vo2/W/VE, mL/W/L 0.96+±0.14 0.71 ±0.06 0.51 ±0.06VE/VCO2 43.0±0.82 38.4+2.33 39.4+1.32SaO2, % 90±2 92+1 93±1
*Values are expressed as mean ± SEM.fp<0.05 vs GP3.1p<0.05 vs GP2.
1208 Clinical Investigations
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

Table 4-Significant Correlations in All Patients (N=28)
r p
VO2 peak vs %IBW (BMI) 0.82 (0.81) <0.0001AT (n=21) vs %IBW (BMI) 0.69 (0.68) <0.0001Rest VD/VT VS %IBW (BMI) -0.59 (-0.60) <0.001VO2/W/VE vs %IBW (BMI) -0.59 (-0.56) <0.001 (0.02)FEV1 vs %IBW (BMI) 0.46 (0.46) <0.02 (0.02)FEV1 VS VO2 peak 0.54 <0.001
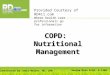
0.51 ± 0.06 in GP3. Ventilatory equivalents for CO2(VE/VCO2) and 02 sat values were the same in thethree groups. One patient (from GP1) displayed asustained 02 desaturation (7%); four more patients(one from GP1, two from GP2, and one from GP3)showed values of desaturation between 3 and 5%;variations in 02 sat <3% were not considered signif-icant. Pertinent correlations between criterion vari-ables observed in the entire study population arelisted in Table 4: some of them are also graphicallydisplayed in Figure 1.
DISCUSSION
Reduced exercise tolerance is generally acceptedas an inavoidable complication of advanced COPD;the presence of different degrees of physical limita-tion in patients with comparable lung functionimpairment, however, suggests a multifactorial ori-gin for this phenomenon. Although airways obstruc-tion has classically been considered the most impor-tant of these pathogenetic factors, studies aimed atcomparing lung function impairment and exercisetolerance in COPD failed to establish a clear corre-
2000I
E- 1
-yV 1
0Q
c0
1500
1000
500
0s5c
1.0
0.8
N 0.60
* 0.4cnL 0L.. 0.2
0.0 _50
75 100
% IBW125 150
100
% I W
lation between the two parameters, probably de-pending on differences in study populations, ie,prevalence of emphysema or chronic bronchitis. Inour patients, lung function impairment certainlyplayed an important role in reducing exercise capac-ity, as demonstrated by the correlation betweenFEV1 and Vo2 peak (r=0.54). Lower limb fatigue isanother important factor contributing to exercise in-tolerance; this is due, particularly in deconditionedelderly patients, to a variable degree of muscle atro-phy leading to a significant reduction in musclestrength and endurance.4The present study was undertaken to test the hy-
pothesis that an independent negative effect was ex-erted on our patients' exercise tolerance by their poornutritional status, through a limitation in the aerobiccapacity of the exercising muscle. From analysis ofthe interrelationships among the physiologic vari-ables studied, some important considerations can bederived. The existence of the positive correlations%IBW vs VO2 peak (r=0.82) and %IBW vs AT(r=0.69) indicates that the influence of nutritionalconditions on muscle aerobic capacity and exercisetolerance, previously demonstrated in healthy sub-jects, persists in patients with COPD. Aerobic capac-ity was progressively more compromised, parallelingthe decrease in body weight. In the past, exercise in-tolerance was almost entirely attributed to ventila-tory limitation,31'34'35 in the assumption that patientswith COPD hardly ever reached the AT. Onlyrecently the development of lactic acidosis during theearly phases of exercise in patients with COPD has
x 800EEn 600
* 40o
" 20
51
i 2.0I-
<1.0
0.5E
C4,0> 0.0
5(
L0 75 100
% IBW
0
125 150
75 100 125 150
% IBW
FIGURE 1. Effects of %IBW on Vo2 peak, AT, Vo2/W/VE, and VD/VT. Individual data for GP1 (filledsquares), GP2 (filled circles), and GP3 (filled triangles). Note that in the right upper panel, n=21, be-cause in 7 patients, AT was not clearly identified.
CHEST / 107/5 / MAY, 1995 1209
m r=0.82p<O.0001
v
(n=21)
r=0.69p<O.0001
r=-0.59XU* * p<O.001
* 0 w04
1\
I
I
r-
- r
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

been described as a common event.13'14'32 This phe-nomenon is likely to reflect an inadequate 02 supplyto peripheral exercising muscles. Reduced 02 flow inpatients with COPD may be explained by thefollowing: (1) reduced arterial 02 content; (2) in-creased pulmonary vascular resistance leading to in-adequate cardiac output;13 and (3) blood flow diver-sion to respiratory muscles ("steal" phenomenon)related to the increased work of breathing.15 What-ever the cause of the lactate generation, it determinesa further increase in the ventilatory demand and afurther reduction in exercise tolerance.The possibility that malnutrition, leading to re-
duced intramuscular adenosine triphosphate (ATP)turnover and decreased concentrations of phos-phocreatine, may force the muscles to an early switchtoward anaerobic glycolysis,36 however, has to datebeen underestimated and in our opinion deserveshigher consideration. Cellular oxidation rate in skel-etal muscle is primarily dependent on mitochondrialconcentration of adenosine diphosphate (ADP), in-organic Pi, NADH, and oxygen. In deconditionedindividuals, exercise aerobic capacity is impairedbecause of reductions in mitochondrial concentra-tion, size, and function with greater decrease of ATPand phosphocreatine and attendant increase of ADPand Pi, and smaller oxidation of fat with consequentfaster utilization of glycogen. 16 Direct 31P-MRSstudies9'12 and indirect Vo2 kinetics studies7'8 pro-vided evidence that in patients with COPD, aerobiccapacity is reduced. Using biopsy techniques, it hasbeen shown that peripheral and respiratory musclesof patients with COPD are deficient in phosphocre-atine and ATP.36 Recently it has been reported thatreduced phosphorus content in peripheral muscles isa common finding in patients with COPD and ispresumably attributable to drug-induced impair-ment of renal phosphate handling.37 Furthermore, anincreased rate of branched amino-acid degradation,indicating their use as an energy production sub-strate, and a reduction in respiratory and peripheralmuscle mass, ie, in a variable degree of muscle atro-phy, have been detected in malnourished subjects.18
In light of the above considerations, it is reasonableto assume that in malnourished individuals withCOPD, energy-producing processes within the mus-cle may be less adequate to meet metabolic needsthan in normally nourished, otherwise comparablepatients. Strength and endurance of respiratory andskeletal muscles have been reported to be signifi-cantly reduced in patients with COPD with earlyperipheral muscle fatigue. In poorly nourished pa-tients, this phenomenon is more evident and, impor-tantly, nutritional repletion improves skeletal musclefunction and exercise tolerance without measurablechanges in lung function and arterial blood gas ten-
sion.25 In our study, the strong correlation existingbetween nutritional status and maximal aerobic per-formance indicates how the intramuscular metabolicalterations related to a compromised nutritional sta-tus seem to influence physical performance; thesefindings are at least in part unrelated to lung functionimpairment.The precise pathogenesis of malnutrition in COPD
has not been clearly defined. As a corollary, thepresent findings of increased wasted ventilation andhigh 02 cost of ventilation, along with previous ob-servations38 of a close correlation between cost ofventilation and Vo2 peak, are compatible with thehypothesis that in COPD, weight loss is caused by theexcessive caloric expenditures dictated by the highenergy requirements of the respiratory muscles. InCOPD, wasted ventilation is more pronounced amongindividuals with a large emphysematous component.In our study, a significant correlation was observedbetween VD/VT and nutritional state. Previous re-ports19'39 have shown a close correlation betweenweight loss and reduced diffusing capacity for carbonmonoxide (Dco) in emphysematous patients withCOPD. It is likely that the high VD/VT observed inthe present study reflects the same pathophysiologicalteration responsible for Dco reduction, ie, loss in gasexchange surface. The patients with the worse nu-tritional status had the highest values of Vo2/W/VEand AlVo2/ZAW. High values of Vo2 for given work-loads have been observed by some authors andinterpreted as a reflection of an elevated 02 cost ofbreathing.40 To our knowledge, no previous study hasanalyzed the A7Vo2/AW ratio from unloaded pedal-ing to peak exercise in patients with COPD.zVo2/AW has a predictable and consistent value innormal subjects34 and, being increased in the under-nourished subjects, is also likely to reflect the in-creased 02 consumption by the respiratory muscle. Afactor limiting the precision of the computation of A\Vo2/AW, at least in the patients with the worst ex-ercise tolerance, is the small number of available datapoints. The exclusion of unloaded pedaling Vo2 data,that in some patients could account for as much as50% of the maximal Vo2, should allow us to avoid anyartificial increase in the A'Vo2/zAW values; we cannotexclude that the analysis of a greater number of datapoints may yield slightly different results.
In conclusion, our study focused on possible linksamong respiratory physiologic indexes, exercise tol-erance, nutritional status, and onset of metabolic ac-idosis during exercise. We hypothesized that inpatients with COPD, nutritional deficiencies ad-versely affect metabolism and function of the exer-cising peripheral and respiratory muscles, tissues al-ready in a precarious biochemical and physiologicstate due to the chronic limitation in oxygen avail-
Clinical Investigations1210
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

ability. When compared with GP2 and GP3, themalnourished GP1 showed more limited exercisecapacity, earlier onset of anaerobic metabolism,larger physiologic dead space, and higher values ofindexes that are likely to reflect an increased 02 costof ventilation. Our data confirm previous observa-tions that in malnourished patients with COPD, thealterations in airways resistance, oxygen cost of ven-tilation, and exercise tolerance are more pronouncedthan in normally nourished, otherwise comparableCOPD cohorts.'9,26,27Our findings are preliminary in nature. They are,
however, sufficiently founded to suggest the need forfuture studies to validate the hypothesis that in mal-nourished patients with COPD, a measurable en-hancement of exercise tolerance can be achieved byintense rehabilitation programs, in conjunction withadequate increase in caloric intake until body mass isrecovered. In addition, consideration should be givento the administration of supplemental 02 to patientswith stable COPD during the rehabilitation sessionsand in the course of any muscular effort that exceedsroutine physical activities, even if this form of ther-apy is not indicated by current criteria.41,42 The ra-tionale for this approach is that short-term 02administration may lower the 02 cost of ventilation38and improve muscle aerobic capacity;8"11 our resultssuggest that these beneficial effects could be evenmore evident in malnourished subjects with COPD inwhom high cost of ventilation largely accounts for theincreased caloric expenditure, and in whom poormuscle energetics are associated with impaired aer-obic capacity.
REFERENCES1 Belman MJ. Exercise in chronic obstructive pulmonary disease.
Clin Chest Med 1986; 7:585-972 Dillard TA, Piantadosi S, Rajagopal KR. Determinants ofmaximum exercise capacity in patients with chronic airflowobstruction. Chest 1989; 96:267-71
3 Carlson DJ, Ries AL, Kaplan RM. Prediction of maximum ex-ercise tolerance in patients with COPD. Chest 1991; 100:307-11
4 Killian KJ, Leblanc P, Martin DH, et al. Exercise capacity andventilatory, circulatory, and symptom limitation in patientswith chronic airflow limitation. Am Rev Respir Dis 1992;146:935-40
5 Corriveau ML, Rosen BJ, Dolan GF. Oxygen transport andoxygen consumption during supplemental oxygen administra-tion in patients with chronic obstructive pulmonary disease. AmJ Med 1989; 87:633-37
6 Hughes RL, Katz H, Sahgal V. Fiber size and energy metab-olites in five separate muscles from patients with chronicobstructive lung disease. Respiration 1983; 44:321-28
7 Nery LE, Wasserman K, Andrews JD, et al. Ventilatory and gasexchange kinetics during exercise in chronic airways obstruc-tion. J Appl Physiol 1982; 53:1594-1602
8 Palange P, Galassetti P, Carlone S, et al. Effect of 02 on Vo2kinetics and other cardiorespiratory parameters during exercisein COPD. Clin Res 1991; 39:753A
9 Galassetti P, Boska M, Mannix ET, et al. A magnetic resonance
spettroscopy study of ATP production in COPD patients withvarying levels of hypoxemia. Clin Res 1992; 40:698A
10 Pajen JF, Wuyam B, Reutenauer H, et al. Impairment of mus-cular metabolism in chronic respiratory failure: a human P31MRS study. NMR Biomed 1991; 4:41-5
11 Pajen JF, Wuyam B, Levy P, et al. Muscular metabolism dur-ing oxygen supplementation in patients with chronic hypox-emia. Am Rev Respir Dis 1993; 147:592-98
12 Tada H, Kato H, Misawa T, et al. 31P-nuclear magnetic reso-nance evidence of abnormal skeletal muscle metabolism inpatients with chronic lung disease and congestive heart failure.Eur Respir J 1992; 5:163-69
13 Casaburi R, Patessio A, loli F, et al. Reductions in exercise lac-tic acidosis and ventilation as a result of exercise training inpatients with obstructive lung disease. Am Rev Respir Dis 1991;143:9-18
14 Patessio A, Casaburi R, Carone M, et al. Comparison of gas ex-change lactate, and lactic acidosis threshold in patients withchronic obstructive pulmonary disease. Am Rev Respir Dis1993; 148:622-26
15 Levison H, Cherniack RM. Ventilatory cost of exercise inchronic obstructive airways disease. J Appl Physiol 1968; 25:21-7
16 Holloszy JO, Coyle EF. Adaptations of skeletal muscle toendurance exercise and their metabolic consequences. J ApplPhysiol 1984; 56:831-38
17 Hunter AMB, Carey MA, Howard WL. The nutritional statusof patients with chronic obstructive pulmonary disease. Am RevRespir Dis 1981; 124:376-81
18 Wilson DO, Rogers RM, Hoffman RM. Nutrition and chroniclung disease. Am Rev Respir Dis 1985; 132:1347-65
19 Sahebjami H, Doers JT, Render ML, et al. Anthropometric andpulmonary function test profiles of outpatients with stablechronic obstructive pulmonary disease. Am J Med 1993; 94:469-74
20 Wilson DO, Rogers RM, Wright EC, et al. Body weight inchronic obstructive pulmonary disease: The National Instituteof Health positive-pressure breathing trial. Am Rev Respir Dis1989; 139:1435-38
21 Boushy SF, Adhikair PK, Sakamoto A, et al. Factors affectingprognosis in emphysema. Dis Chest 1964; 45:402-11
22 Donahoe M, Rogers RM, Wilson DO, et al. Oxygen consump-tion of the respiratory muscles in normal and in malnourishedpatients with chronic obstructive pulmonary disease. Am RevRespir Dis 1989; 140:385-91
23 Arora NS, Rochester DF. Respiratory muscle strength andmaximal voluntary ventilation in undernourished patients. AmRev Respir Dis 1982; 126:5-8
24 Bassili HR, Deitel M. Effect of nutritional support on weaningpatients off mechanical ventilators. JPEN 1981; 5:161-63
25 Efthimiou J, Fleming J, Gomes C, et al. The effect of supple-mentary oral nutrition in poorly nourished patients withchronic obstructive pulmonary disease. Am Rev Respir Dis1988; 137:1075-82
26 Gray-Donald K, Gibbons L, Shapiro SH, et al. Effect of nutri-tional status on exercise performance in patients with chronicobstructive pulmonary disease. Am Rev Respir Dis 1989; 140:1544-48
27 Schols AMWJ, Mostert R, Soeters PB, et al. Nutritional state andexercise performance in patients with chronic obstructive lungdisease. Thorax 1989; 44:937-41
28 Meneely GR, Renzetti AD, Steele JD, et al. Chronic bronchitis,asthma and pulmonary emphysema: a statement by the Com-mittee on Diagnostic Standards for Nontubercolosis RespiratoryDisease. Am Rev Respir Dis 1962; 85:762-68
29 Metropolitan Life Insurance Company. New weight standardsfor men and women. New York: Metropolitan Life, 1983
CHEST / 107/5/ MAY, 1995 1211
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017

30 Hughson RL, Kowalchuk JM, Prime WM, et al. Open-circuitgas exchange analysis in the non-steady-state. Can J Appl SportsSci 1980; 5:15-8
31 Heigenhasuer JF, Jones NL. Measurements of cardiac outputby carbon dioxide rebreathing method. Clin Chest Med 1989;10:255-64
32 Sue DY, Wasserman K, Moricca RB, et al. Metabolic acidosisduring exercise in patients with chronic obstructive pulmonarydisease: use of the V-slope method for anaerobic threshold de-termination. Chest 1988; 94:931-38
33 Hansen JE, Sue DY, Wasserman K. Predicted values for clin-ical exercise testing. Am Rev Respir Dis 1984; 129:S49-55
34 Wasserman K, Hansen JE, Sue DY, et al. Principles of exercisetesting and interpretation. Philadelphia: Lea & Febiger, 1987;78-9
35 Loke J, Mahler DA, Man SFP, et al. Exercise impairment inchronic obstructive pulmonary disease. Clin Chest Med 1984;5:121-43
36 Gertz I, Hedenstierna G, Hellers G, et al. Muscle metabolismin patients with chronic obstructive lung disease and acute res-
piratory failure. Clin Sci Mol Med 1977; 52:395-40337 Fiaccadori E, Coffrini E, Ronda N, et al. Hypophosphatemia in
course of chronic obstructive pulmonary disease: prevalence,mechanisms, and relationships with skeletal muscle phosphoruscontent. Chest 1990; 97:857-68
38 Mannix ET, Manfredi F, Palange P, et al. Oxygen may lowerthe 02 cost of ventilation in chronic obstructive lung disease.Chest 1992; 101:910-15
39 Openbrier D, Irwin M, Rogers RM, et al. Nutritional status andlung function in patients with emphysema and chronic bron-chitis. Chest 1983; 83:17-22
40 Younes M. Interpretation of clinical exercise testing in respira-tory disease. Clin Chest Med 1984; 5:189-206
41 Nocturnal Oxygen Therapy Trial Group. Continuous or noc-turnal oxygen therapy in hypoxemic chronic obstructive lungdisease. Ann Intern Med 1980; 93:391-98
42 Dean NC, Brown JK, Himelman RB, et al. Oxygen mayimprove dyspnea and endurance in patients with chronic ob-structive pulmonary disease and only mild hypoxemia. Am RevRespir Dis 1992; 146:941-45
S __X_SsUsIPOSTGRADUATE COURSE
surgery foremphysema
May 12, 1995
Northbrook, Illinois
For information: 800-343-2227 or 708-498-1400
Clinical Investigations1212
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21713/ on 04/07/2017