Embed Size (px)
Citation preview
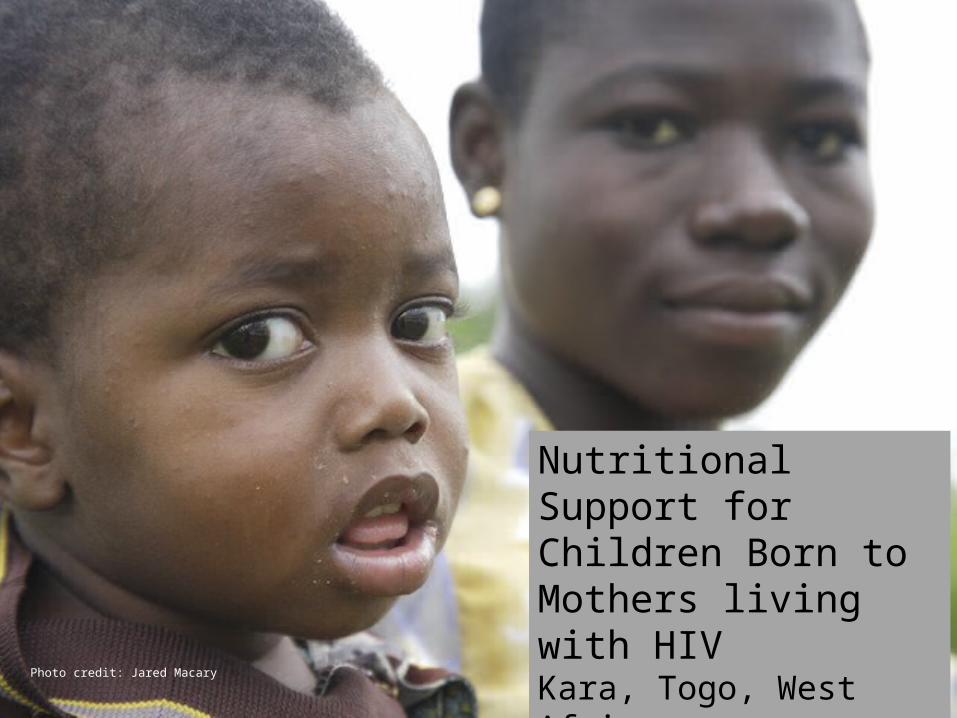
Nutritional Support for Children Born to Mothers living with HIVKara, Togo, West AfricaJennifer Schechter, Andrea Hobby, Jen Taylor, Amy BaisdenMarch 15, 2011Photo credit: Jared Macary

Overview
•Background
•Problems and Plan
•Objectives and Training
•Supervision, Monitoring and Evaluation

Photo credit: Jared Macary
Meet Irene


Demographics: 6.8 million people
Political: Long history of political corruption; Major donor governments withdrew 1990’s; Non-violent coup 2005; Presently transition to democracy
Socioeconomic: GDP per capita $900; 65% employed in agriculture; 60% have access to water (compared to 82% in neighboring Ghana)
Foreign Assistance: Financial development assistance for Health $23, compared to $202 in Ghana in 2007
Photo credit: Wikipedia
Background

Togo in Context

• Northern Togo
• Population: 669,000
• Association Espoir pour Demain (AED-Lidaw)
• Clinics in 4 of 7 sub-regions in cities of o Kara -- pop: 100,400 o Bafilo -- pop: 18,400o Ketao -- pop:
unknowno Kande -- pop: 9, 600
Kara Region

Photo credit: Jared Macary
Association Espoir pour Demain
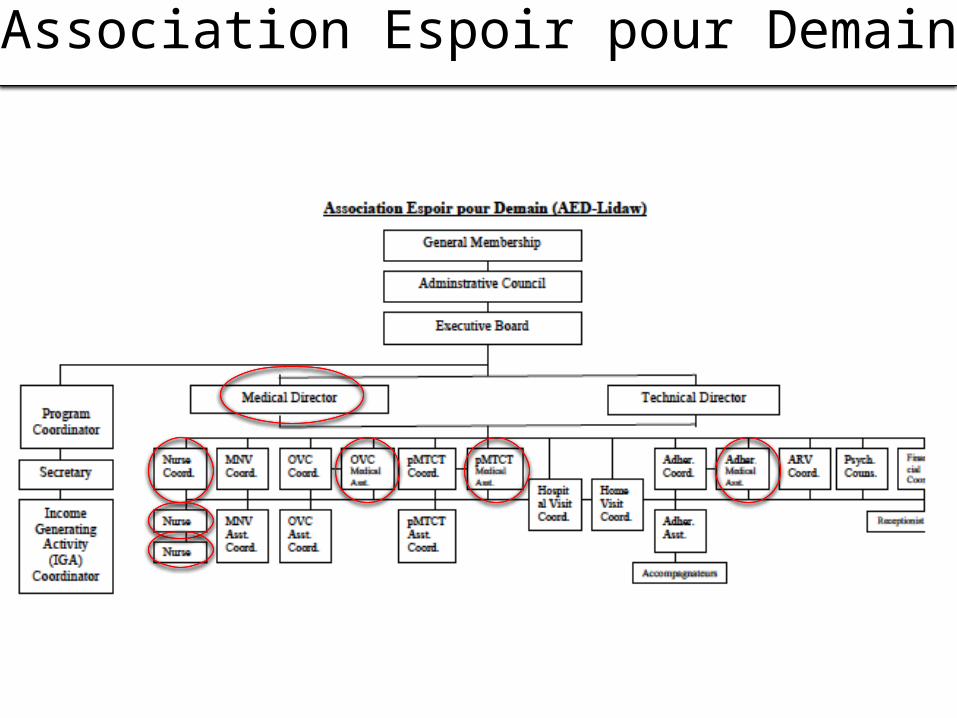
Association Espoir pour Demain

Community Structure
Photo credit: Jared Macary

Needs Assessment
Photo credit: Jared Macary

HIV Positive Mothers and their Infants
•HIV can be transmitted through breast milk•Studies have shown poor outcomes for non-breastfed newborns of HIV positive mothers•Prenatal transmission of HIV is associated with decreased body weight, length and head circumference•48% of children are Exclusively breastfed (<6 months)•70% of children are breastfed with complementary food (6-9 months)

Breastfeeding and HIV: Conflicting Messages

1. HIV positive women fear transmitting HIV through breastfeeding.
2. Togo MOH recommendations do not match the WHO guidelines and women receive conflicting counseling• ARV's are provided by the government
3. If a woman is going to stop breastfeeding she needs to be able to provide for the nutritional needs of her child• Formula and milk are expensive
• Pumping, heat treating and storing milk is difficult and often unsanitary
4. Risks to infants associated with early breastfeeding cessation:• Neglect, Distress, Loss of appetite, Diarrhea, Malnutrition
5. In Togo, 20% of children under 5 are undernourished• 21% are underweight
• 6% suffer from wasting
• 27% suffer from stunting
Problems

Months of age
Energy needs from complementary foods for breastfed infants
Energy needs from complementary foods
for non breastfed infants
6-8 200kcal/day 600kcal/day
9-11 300kcal/day 700kcal/day
12-23 550kcal/day 900kcal/day
Nutritional Needs of Infants

• nutrition training
• enriched flour
• nutrition assessments
• children < 2 years
Our Plan

Training Mothers/Families/Caregivers• By the end of the project 75% of HIV positive pregnant women
and mothers/caregivers with children under 24 months participating in the pMTCT HIV program will attend a half-day community training session each month at the clinic regarding nutrition and other revolving pertinent topics. • Output indicator - # in attendance
•
Objectives

Training Providers and Health Workers• By the end of the project, 95% of the facility providers/health
workers interacting with HIV positive pregnant women/mothers of children under the age of 2 years will attend a 3-day training regarding the importance of proper nutrition for children.• Output indicator - # of providers/health workers in attendance
• By the end of the project, 95% of the facility providers/health workers interacting with HIV positive pregnant women/mothers of children under the age of 2 years will effectively counsel women on the on the importance of proper nutrition for children.• Output indicator - # of women reporting having received counseling
Objectives continued

Nutrition• By the end of the project 90% of HIV positive mothers
participating in the pMTCT HIV program with children 6-24 months will serve their children enriched flour porridge. • # of women reporting serving porridge
• By the end of the project 90% of fewer children born to HIV positive mothers enrolled in the pMTCT program will show physical signs of undernourishment.• # of children with signs of undernourishment
Objectives continued

Inputs OutputsActivities Participation
Outcomes – ImpactShort Term Long Term Impact
Staff Time
Classroom and Demo Supplies
Incentives for Participation
Ingredients for Porridge
Training
Supervision
Assessment
Mothers/Families
Health Workers
Children < 2
# of women receiving nutrition counseling
# of women/families and health workers recognizing the benefits of proper nutrition
# of trained health workers
# of trained mothers/families
# of children assessed in clinic
# of women serving porridge to their children
# of women/families and health workers recognizing signs of under-nourishment
Empowered Women
Reduced infant/under 2 morbidity and mortality
Reduced # of children with signs of under-nourishment
# of women correctly making porridge

• Participants will meet monthly• A nutritional topic will be discussed
at each monthly meeting including: fluid needs nutrient rich local food sources feeding frequency breastfeeding duration weaning techniques
• Demonstration - every six months including making nutrient rich porridge.
• Monthly meeting with doctor where women are given fortified flour for porridge and baby assessed.
Training – Mothers and Other Caregivers

• 3 day in-service to train medical staff regarding:• Current breastfeeding recommendations• Nutritional needs of breastfed and non-breastfed infants.
• Follow-up workshop every 6 months to address additional questions and issues that may arise.
Training – Providers and Health Workers