Embed Size (px)
Citation preview

REVIEW
Nutritional Support in Surgical Practice: Part I Michael M. Meguid, MD, PhD, FACS, Antonio C. Campos, MD, MS, William G. Hammond, MD, Syracuse, New York
Critical evaluation of the therapeutic benefit gained from provision of nutritional support requires knowledge regarding the nutritional status of those to w h o m it was given. The apparent effect of giving parenteral nutrition or enteral nutrition depends not only on how much and how well it is given, but also on how depleted the recipient is. Thus, nutri- tional assessment requires close examinat ion before proceeding to assess the efficacy and potential benefits of the remedial measures of parenteral nu- trition or enteral nutrition.
Although preoperative malnutrition is associated with a poor operative outcome, there appears to be no consensus as to whether perioperative nutritional support can reduce postoperative complications to the level occurring in well-nourished patients un- dergoing similar procedures. This is partly because reports evaluating the effect of perioperative nutri- tional support on postoperative outcome vary wide- ly as to numbers of patients studied, primary diag- noses, and the duration and quality of perioperative nutritional support.
In Part I, these issues are explored in patients who are undergoing operations for cancer, trauma, or burns. Enteral nutrition appears to be as effec- tive as parenteral nutrition in improving operative outcome, as compared with ad libitutrt oral nutri- tion. Postoperative enteral nutrition and parenteral nutrition are equally effective in reducing postoper- ative complications.
From the Surgical Metabolism and Nutrition Laboratory, Department of Surgery, University Hospital, SUNY Health Science Center, Syra- cuse, New York. Supported in part by Grant AM36275 from the National Institute of Arthritis, Diabetes, Digestive and Kidney Dis- eases, National Institutes of Health, Bethesda, Maryland; and an edu- cational grant from Mead Johnson Nutrition Division, Evansville, Indi- ana.
Requests for reprints should be addressed to Michael M. Meguid, MD, PhD, FACS, Department of Surgery, University Hospital, SUNY Health Science Center, 750 East Adams Street, Syracuse, New York 13210.
Manuscript submitted February 13, 1989, and accepted June 12, 1989.
N " utritional support (parenteral nutrition and enteral nutrition) is both used and useful in the practice of
surgery. It continues to find application in a variety of surgical and medical situations far beyond the specula- tions of the numerous forefathers of nutritional support. Yet, its continued rational use will depend on the general perceptions of its usefulness.
In reviewing the use and usefulness of both parenteral nutrition and enteral nutrition, we have focused on the use of nutritional support in the diseases and conditions that general surgeons are commonly consulted about or asked to treat. Since most surgical patients could poten- tially also develop specific organ system failure, such as renal, hepatic, or pulmonary failure, which might modify the use of parenteral nutrition, this area is also examined. Since compositions of parenteral nutrition and enteral nutrition solutions vary, the caloric density, composition, and product name have been listed when these data were available.
Most reports reviewed have assessed the efficacy of nutritional support using various criteria for nutritional assessment. The latter is a controversial topic, in a state of flux, and has not received the full scientific attention it deserves. However, since it has been used to assess, in part, the outcome of nutritional support, we begin with a consideration of these methods. We next review the gen- eral areas and the specifically delineated disease entities in which nutritional support is frequently used, and, final- ly, the role of nutritional support in instances of acute organ system failure. Within each section and where available data permit, we have summarized the data con- cerning energy expenditure and energy requirements in each disease entity, on the assumption that nutritional support is of therapeutic benefit only when amounts given are equal to or greater than the energy requirements. Furthermore, we have summarized the frequency of mal- nutrition existing in those with a specific disease entity or associated condition to place the magnitude of disease- induced nutritional deficiency into perspective and to in- dicate that nutritional support (parenteral nutrition or enteral nutrition) would physiologically benefit these pa- tients more than it would well-nourished patients. Clear though the associations between preoperative malnutri- tion and poor surgical outcome generally are, they do not prove that nutritional support will be effective in reducing the observed excess morbidity; poor nutritional state pre- operatively and high postoperative morbidity might each be independently associated with more severe disease or more extensive operations. Lastly, the available valid data describing the usefulness and benefit of nutritional support are presented.
It is apparent that the implications of uncontrolled enthusiastic and descriptive reports of the use of nutri- tional support in association with surgical disease have often led to "vogue" therapy and to even more irrelevant discussion. Unfortunately, many publications have been
THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990 345

MEGUID ET AL
uncritical and/or anecdotal, sometimes to the point of threatening the whole subject with disrepute. Impressions as to the usefulness of parenteral or enteral nutrition can best be vindicated by adequate and well-designed pro- spective randomized trials. Although randomized con- trolled trials are accepted as the most effective way of determining the relative efficacy of therapy, its appropri- ate use may result in missing a true therapeutic benefit, characterizing a type II statistical error. The use of a sample size too small to offer a reasonable chance of successfully rejecting a null hypothesis in favor of the treatment is possibly the most common cause of its occur- rence. Limitations in resources and time and practical difficulties of carrying out such studies are usually at the root of this problem, and the investigators should be aware of the limitations of the trials when analyzing their results. Since few prospective randomized trials have in- cluded an appropriate number of patients, evidence of a true therapeutic benefit from adequate controlled trials is often lacking in most areas in which nutritional support is USed.
In preparing this review, we have critically evaluated many studies and have been quite selective so as to ac- complish our objectives of summarizing the relevant cur- rent knowledge regarding nutritional support in surgical practice. In doing this we have tried to focus primarily on prospective studies.
In areas in which further research is needed to more clearly define the use of nutritional support, we have indicated this and suggested potentially fruitful directions of inquiry.
NUTRITIONAL ASSESSMENT Most of the methods used for nutritional assessment
are designed to provide information regarding body com- position abnormalities. In addition to clinical evaluation, they include straightforward physical measurements (body weight and other anthropometric measurements), biochemical or immunologic determinations, and sophis- ticated laboratory measurements, at present useful pri- marily for research purposes.
Clinical assessment: Controlled studies by Baker et al [1] and Detsky et al [2] suggested that clinical judg- ment was superior to a single nutritional index in predict- ing the development of nutritionally associated complica- tions. The prediction was based on: (1) past nutritional intake, disease process, operative effect on future intake of nutrients, and catabolic disease (if present); and (2) the current physical state as regards weight loss, muscle wasting, functional status edema, skin rash, and neuropa- thy. Pettigrew et al [3] were unable to confirm that clinical judgment was superior to nutritional indices. In their study, the clinical status of 198 surgical patients was assessed by two surgeons, one of whom had nutritional training. They correctly identified more than 80% of the patients who were not depleted, but only identified 40% of those who actually were depleted. This study suggested that malnourished patients could not be reliably identi- fied by clinical examination alone. However, since the methods of nutritional assessment to which clinical evalu-
ation was compared were different, the true extent to which malnutrition can be assessed solely by clinical ex- amination remains open for further investigation.
Anthropometrie indices: The thickness of the triceps skinfold of the nondominant arm is taken to represent body fat mass, while the midarm muscle mass of the same arm is taken to represent the lean body mass. Despite its limitations, the usefulness of anthropometrics, and skin- fold thickness in particular, has been established by Dur- nin and Womersley [4]. They demonstrated that the den- sity of the fat-free (lean) body mass is a reasonably constant value, and that equations to calculate density and total body fat can be derived for various age and sex groups solely from the sum of four (or even one) skinfold thickness measurements. Validated by hydrodensitome- tric measurements, their equations permit an estimation of density and total body fat from skinfold thickness measurements with an accuracy of 4- 5% for men and 4- 3.5% for women.
Measurements of arm muscle circumference are thought to give an indication of the body's muscle mass and hence its main protein reserve. Arm muscle circum- ference can be derived from the total arm circumference and the triceps skinfold thickness. Heymsfield et al [5] showed a 15% to 25% overestimation of lean body mass by anthropometry in arm muscle. Jeejeebhoy et al [6] found no correlation between the circumference of arm muscle and the initial total body nitrogen content in pa- tients receiving parenteral nutrition; no changes in total body nitrogen were found after parenteral nutrition ei- ther. Collins et al [7] also found no correlation between the circumference of arm muscle and total body nitrogen in patients receiving parenteral nutrition.
Differences in arm muscle circumferences occur be- tween apparently well-nourished groups of differing eth- nic origin; changes occur throughout adult life in both sexes; and a secular trend has been observed in the values obtained in large population studies. Hence, there is no sound basis for classifying as malnourished those males with an arm circumference of less than 23 cm or those females with a circumference of less than 22 cm, as was common practice in many of the articles we reviewed.
Weight loss: Ever since Studley [8] in 1936 showed that a preoperative weight loss of more than 20% was associated with a 33% mortality rate, whereas a 4% mor- tality rate occurred in those with less than a 20% weight loss, the estimation of weight loss has played a key role in the nutritional assessment of surgical patients. The loss is usually calculated by subtracting the present observed weight from either the recall "usual" weight or from the predicted normal weight taken from standard tables or equations. Morgan et al [9], in a cross-sectional study of 105 patients, found that patient recall was associated with an error as great as 3.6 kg.
Recent weight change is a commonly used index of malnutrition. More than 10% loss over any time period has been taken as evidence of malnutrition by Blackburn et al [10], who also proposed a useful correlation between the extent of weight loss and the time over which it developed (Table I). A weight loss of greater than 4.5 kg
346 THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
TABLE 1 Evaluat ion of Weight C h a n g e *
Significant Severe Time Weight Loss Weight Loss
1 week 1-2% >2% 1 month 5% > 5 % 3 months 7.5 % >7.5 % 6 months 10% > 10%
* Values charted are for percent weight change: Percent Weight Change = (Usual weight - Actual weight)/(Usual weight) X 100.
Reproduced with permission from [ 10].
has recently been reported to be highly predictive of sur- gical mortality by both Seltzer et al [11] and numerous other investigators, including Mughal and Meguid [12].
Plasma proteins: Measurement of plasma albumin levels lacks specificity and is therefore of little value in assessing the size of an individual's visceral protein com- partment. Also, the plasma albumin level is dependent on the rate of hepatic synthesis on the one hand and catabo- lism, utilization, excretion, and transvascular transfer on the other, because of the long half-life of these proteins (and thus a slow response to nutritional change).
However, several studies have revealed increased morbidity and mortality in hypoproteinemic patients, particularly those with low albumin concentrations. In a series of 500 medical/surgical admissions to a general hospital, Seltzer et al [13] found a fourfold increase in complications and a sixfold increase in mortality in pa- tients whose serum albumin levels were less than 3.5 g/ dL. Reinhardt et al [14] reported that in 50 patients with serum albumin levels of less than 2.0 g/dL, the mortality rate was 62%, whereas Bistrian et al [15] reported high mortality rates in patients with serum albumin levels of less than 3.0 g/dL.
Plasma proteins with a half-life shorter than that of albumin have been investigated as potential indicators of malnutrition. Kaminski et al [16] observed a 2.5-fold increase in hospital mortality and Blackburn et al [17] found a significantly increased risk of sepsis and death in patients with serum transferrin levels below 170 mg/dL. Transferrin as a measure of nutritional status has been reported by Fletcher et al [18] to be useful relative to pre- albumin, whereas Roza et al [19] have expressed doubts about its utility. Other short-lived serum proteins, e.g., pre-albumin and retinol-binding protein, have also been used as predictors of morbidity and mortality. That com- plications can be predicted from abnormal levels of plas- ma protein has been severely challenged by the findings of Ryan and Taft [20]. They were unable to confirm a correlation between low albumin or transferrin levels and the development of complications. Starker et al [21] stud- ied sodium and nitrogen balance in 14 patients over 13 to 14 days of parenteral nutrition. During the period of positive nitrogen balance, seven patients lost weight and had a decrease in the extracellular fluid compartment and an increase in serum albumin levels; the other seven patients gained weight and had an increase in the extra-
cellular fluid compartment, while their albumin levels remained virtually unchanged. These latter patients ei- ther had continuing infection or initial nutritional deple- tion that was unusually severe; average body weight 38% below predicted normal. This study demonstrates that serum albumin levels (or body weight change) cannot be used alone as an accurate indicator of acute change in nitrogen status, because there is too much variability in the response of body fluid compartments to the underly- ing clinical condition(s).
Indeed, concern for the misuse of these proteins as indicators for the presence of malnutrition has been in- creasing, as evidenced by the studies of Merritt et al [22] and Carpentier and Ingenbleek [23], and by the more recent reviews of Fleck [24] and McLaren [25].
Creatinine/height index: Since creatine is present almost entirely within muscle (as creatine phosphate) and is converted to creatinine at a relatively constant rate, the excretion rate of urinary creatinine may be indicative of total muscle mass. Greenblatt et al [26] and Forbes et al [27] showed that this is reasonably accurate in patients without renal failure if based on multiple measurements. In addition, Jeejeebhoy and Meguid [28] reported that urinary creatinine excretion correlates with the total body nitrogen content, except in cancer patients; in these pa- tients, creatinine excretion remained stable when total body nitrogen decreased, indicating increased creatinine loss as the disease progressed. Mullen et al [29] were unable to demonstrate that the creatinine/height index was of value in predicting complications.
Immunologic tests: The peripheral blood absolute lymphocyte count and the skin response to an injected antigen have been used as indicators of the status of the visceral protein compartment. Blackburn et al [10] dem- onstrated that a lymphocyte count below 3,000/mm 3 re- flected an immune deficiency, whereas in the study of Johnson et al [30], such a count was associated with a negative response to an injected antigen. However, both these measurements can be influenced by factors other than nutrition. Indeed, Meakins et al [31] have shown that simple drainage of an abscess can reverse anergy.
Yet, a strong association between morbidity and de- creased skin test reactivity has been shown by Daly et al [32] and Haffejee and Angorn [33]. Harvey et al [34] reported that the proportion of patients with negative skin tests who died (50%) was significantly higher than the proportion of those with normal skin test reactivity who died (23%). In surgical patients studied by Christou and Meakins [35], those considered anergic preoperatively had a 29% incidence of sepsis and a 29.9% mortality rate, compared with 7.5% and 4.6%, respectively, for those classified as immunologically normal. Attempts at cor- recting anergy with the use of parenteral nutrition have been made; although Copeland et al [36] were able to show reversal with an improved outcome, two other groups of investigators, Meguid et al and Brennan et al (unpublished data), were unsuccessful.
Although results from such tests are potentially useful as predictors of morbidity, without the ability to separate the effects of malnutrition from those of disease, it is
THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990 347

MEGUID ET AL
TABLE II Correlation of Body Composition with Nutritional Assessment
Body CompoSition 95 %
Parameter Parameter Confidence (Dependent) (Independent) No. r Mean Limits
Weight/height (kg/m) Ke 331 0,82 48.9 25.3 to 72.5 Tricep skinfold (ram) Body fat 358 0.79 17.2 3.7 to 30.7 Midarm area (din 2) Ks 358 0.68 0.54 0.10 to 0.98 Albumin (mg/dL) K/TBW 367 0.67 3.2 2.0 to 4.4 Total protein (mg/dL) KeTBW 367 0.62 6,6 5.0 to 8.2 Hand strength (kp/cm 2) KeTBW 86 0.45 0.41 0.03 to 0.79 Creatlnlne/height (mg/m) KeTBW 331 0.37 7.1 -6 .3 to 20.5
Reproduced with permission from [40]. dm 2 = square decimeter; K = potassium; Ke = exchangeable body potassium; kp = kilopascal; TBW = total body water.
difficult to justify the utilization of such results as reliable nutritional indicators in individual patients.
Muhivariable indices: In attempts to more accurate- ly predict surgical outcome as affected by nutritional variables, multiple regression equations from a number of anthropomorphic and laboratory tests have been used. Mullen et al [37] developed a prognostic nutritional in- dex (PNI) based on serum albumin, triceps skinfold, se- rum transferrin, and delayed cutaneous reactivity to three recall antigens. This index was applied prospective- ly by Buzby et al [38] to 100 patients undergoing major elective gastrointestinal surgery. Considering all compli- cations, the incidence of complications was 8% for the low-risk population (PNI less than 40%), 30% for the intermediate-risk group (PNI = 40% to 49%), and 46% for the high-risk group (PNI greater than 50%). Mortali- ty rates were 3%, 4.3%, and 33%, respectively. The grossly skewed nonlinearity of the PNI-complications relation- ship limits its use in assessing hazards in individual pa- tients.
Harvey et al [34] in 1981 developed a discriminate function test based on serum albumin, skin test response, presence of sepsis at the time of assessment, and diagnosis of cancer. This had a predictive accuracy of 72% for subsequent hospital mortality, with a sensitivity of 74% and a specificity of 66%. Another predictive nutritional index [13] used only serum albumin and total lympho- cyte count; it had a sensitivity of 75% in predicting death.
Since these indices are only mathematical manipula- tions of numbers derived from tests that at best are only secondarily related to actual nutritional status, it is not surprising that they do not provide satisfactory solutions to the problems of nutritional assessment.
Body composition studies: The three major com- partments of the body are fat, protein, and water. Al- though much body fat is subcutaneous, the abdomen contains a considerable quantity that is not easily mea- sured and that may not be comparably utilized during starvation. According to Moore et al [39], the relation- ship between the components within each compartment may be clearly defined during health, but these relation- ships change during depletion and disease. Body composi- tion determinations utilize a variety of techniques, i.e.,
multiple isotope dilution methods, proton-gamma-analy- sis, and neutron activation, to measure total body nitro- gen. These methods are generally complex and time- consuming and thus are not suitable for routine use in patient care or for measurement of relatively short-term changes. However, they are the standards against which simpler measurements must be validated.
Forse and Shizgal [40] measured total body potassi- um in 216 nourished and malnourished patients as an index of body cell mass. At the same time, the usually used nutritional indices were obtained. Their results, shown in Table II, indicate that all the correlation coeffi- cients were poor and the 95% confidence limits were wide, so that only gross changes could be distinguished from values within the normal range. These results and similar ones by Almond et al [41] demonstrate that anthropo- metric and biochemical evaluations do not correlate sig- nificantly with body composition data derived from mea- surements of total body potassium.
Bioeleetrieal impedance analysis (BIA): Since the standard body composition methods are complex and neither widely nor readily available, bedside techniques to assess body composition are constantly being sought. The BIA method is based on measurements of changes in the conduction of an applied electrical current through the body. Intracellular and extracellular fluids are thought to act as electro-conductors; cell membranes are considered to act as electro-capacitors, although regarded as imper- fect reactive elements.
Since lean body tissue has a far greater electrolyte content than fat, Lukaski et a l [42] showed that this marked difference in ionic content permits the estimation of lean body mass from the assessment of body electrical impedance. Recently, Meguid et al [43] developed an in vitro model that confirmed the relationship between im- pedance using BIA and electrolyte concentration. Segal et al [44] and Kushner et al [45] have also confirmed the correlation between in vivo BIA measurement of body composition and measurements by densitometry and deu- terium dilution techniques. In a normal adult population, Campos et al [46] also compared body composition esti- mates from anthropometric-derived formulas and from BIA measurements to test the potential usefulness of the
3 4 8 THE AMERICAN JOURNAL OFSURGERY VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
BIA method as an adjunct to nutritional assessment in surgical patients. In this population of healthy individuals under steady-state conditions, body densitometry, total body water, and total body fat were predicted as reliably by anthropometric-derived formulas as from BIA mea- surements. The validity of either approach in sick surgical patients with varying hydrational status was also deter- mined by Meguid's laboratory (unpublished data).
Functional tests: Muscle function has been evaluated as an index of nutritional status. It is susceptible to the effects of withdrawing nutrients and refeeding. Muscle function was assessed by Klidjian et al [47] using hand grip dynamometry. In 120 elective gastrointestinal surgi- cal patients, grip strength had a sensitivity of 90% in predicting postoperative complications. However, hand grip dynamometry involves motivation, which may not be constant from patient to patient or in the same patient during the course of an illness.
To obviate this problem in critically ill patients, Jee- jeebhoy's group adapted a technique of electrical stimula- tion of the ulnar nerve at the wrist, which results in contraction of the adductor pollicis muscle and which negates the cooperation of the patient and is not affected by sepsis, drugs, trauma, surgical intervention, or anes- thesia.
By studying two pure models of human starvation and refeeding, namely the obese subject starving and the an- orexic patient being refed, Russell et al [48-50] showed that starvation causes the forced contraction to decrease and the development of fatigue. In addition, the findings of Fraser et al [51] correlated with similar changes in the diaphragm of malnourished patients. The phenomenon is not rendered nonspecifically abnormal by surgery, anes- thesia, steroids, or sepsis, and is only mildly and tempo- rarily altered by severe trauma (crush injuries).
Meguid's group [52,53] have studied the effects of postoperative anorexia and reduced food intake on mus- cle function and plasma creatinine phosphokinase (CPK) in patients undergoing cardiac and general abdominal operations. A close correlation existed between rises in CPK and a decline in the force frequency and a prolonga- tion of the relaxation rate of the adductor pollicis muscle in both groups of patients. However, when the cardiac surgical patients started to eat enough to meet daily ener- gy requirements, as estimated by the Harris-Benedict formula, muscle function and CPK levels both normal- ized. Abdominal surgery patients continued to have ab- normal muscle functions and significantly elevated CPK levels until their caloric intake became comparable to that of the cardiac patients.
Thus, the force-frequency curve and rate of relaxation of the electrically stimulated adductor pollicis muscle are sensitive and specific measures of nutrient status in both the chronic states of obesity and anorexia, and during nutrient withdrawal and refeeding in the postoperative period. Neither muscle power nor the force-frequency spectrum is dependent on body nitrogen, body potassium, or muscle bulk as assessed by arm muscle circumference. We have also shown that muscle power in the adductor pollicis can be doubled by giving nutritional support with-
100,
901
801
7r
5ol
N 3c
2c
1c
COMP �9 099 MAL + 63 R It" 09, p<0001
j , ABE' CARCeNOMATOSJS 146) �9 ~ "
PANCREAS (15) 0 /
ESOPHAGUS (21) �9
saAco.=sl GASTRODUODENUM (331
GU-GYN 1 9 4 ) ~ RODUODE~
J �9 COLORECTUM (IOI) LYMPHO- �9 . PROLIFERATIVE' ~ r O L(VER'GALLBLADDERLIVER GALLBLADDER ((6)6) 2 " (3,5)
I I I I I
% MALNUTRITION ~oo
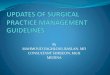
Figure 1. Frequency of malnutrition as related to disease site. Note the linear correlation between the incidence of malnutrition and complications that occurred in different disease sites. Num- bers in parentheses refer to number of patients. Reproduced with permission from Meguid MM, Meguid V. Preoperative identifica- tion of the surgical cancer patient in need of postoperative sup- portive total parenteral nutrition. Cancer 1985; 55: 258-62.
out any detectable change in thearm muscle circumfer- ence [54]. Thus, in the future, a more relevant and specif- ic way of assessing nutritional status may be through further studies of muscle function.
We have described what seems to be an internally contradictory body of information. The reason is that critical evaluation of the therapeutic benefit gained from provision of nutritional support requires knowledge re- garding the nutritional status of those to whom it was given. Thus, the apparent effect of giving parenteral or enteral nutrition depends not only on how much and how well it is given, but also on how depleted the recipient is. As is the case with evaluating any particular therapy, the true worth of the treatment can be identified only when it is tested in patients with similar degrees of the disorder under treatment. Hence, our concern regarding methods of nutritional assessment. These are the diagnostic crite- ria of the disorder for which nutritional support is the treatment, and, as such, require close examination before proceeding to assess the efficacy of the remedial mea- sures.
GENERAL AREAS Perioperative nutritional support: Numerous inves-
tigators have demonstrated that surgical patients with either benign or malignant diseases involving the gastro- intestinal tract have a high incidence of preoperative mal- nutrition, which involves from 40% to 70% of the patients at the time of operation [12,55,56]. The incidence of malnutrition is related to the disease site: 65% of the patients with pancreatic cancer and abdominal carcino- matosis and 60% of those with carcinoma of the esopha- gus and stomach are malnourished (Figure 1).
T HE A M E R I C A N J O U R N A L OF S U R G E R Y V O L U M E 159 M A R C H 1990 3 4 9

MEGUID ET AL
TABLE III Relationships Between Inadequate Oral Nutrient Intake Period (IONIP) and Involved Organ System, Nutritional Status,
and Complications In 464 Patients
Involved Well-Nourished Patients Organ No Complication Complication
System Days n Days n
Malnourished Patients No Complication Complication Days n Days n
Abdominal carclnomatosis 8 8 32 8 22 4 33 26 Esophagus 7 3 18 6 30 5 40 9 Gastroduodenum 9 11 14 7 18 8 40 18 Pancreas 10 3 42" 3 15 2 29 9 Colorectum 8 55 12 20 19 19 19 24 Uver-gallbladder 5 13 13 5 11 6 62 3 Genitourinary/gynecologic 6 58 16 31 8 16 20 20 LymphoproIIferattve 6 29 45 * 4 8 2 21 8 Other 13" 4 10 8 32 4 42 5
�9 Median IONIP disproportionately prolonged by one or more extreme Instances. Adapted from Meguld MM, Debonis D, Meguld V, Terz J. Nutritional support in cancer. Lancet 1983; 2: 230-1.
Because of the high incidence of malnutrition in surgi- cal patients and because malnutrition has long been con- sidered to adversely affect postoperative outcome, investi- gators have attempted to define the role of nutritional support in patients undergoing operations by addressing three objective questions: (1) Is it possible to identify preoperatively those patients at high risk of developing postoperative complications related to nutritional defi- cits? (2) Is preoperative parenteral nutrition effective in reducing postoperative morbidity and mortality? (3) Can postoperative nutritional support reduce mortality and complications after operations?
To address the first question, some investigators have attempted to combine some parameters of nutritional assessment in order to establish prognostic nutritional indices for patients undergoing major operations [34,37,38]. The validity of these indices in establishing the relationship between preoperative malnutrition and postoperative morbidity and mortality has been exam- ined in detail in the section "Nutritional Assessment" of this review.
Retrospectively utilizing age, the nutritional status at admission, the organ system involved with disease, and the length of the inadequate oral nutrient intake period (IONIP) (defined as the number of days that has elapsed after operation until the patient is eating 60% of the predicted caloric requirements), Meguid et al [57] devel- oped a stepwise linear regression analysis that was used in a large group of patients undergoing gastrointestinal op- erations to analyze the relationships between nutritional status, diagnosis, age, and IONIP (Table III). From this analysis, three mutually exclusive groups of patients were identified: Group 1 comprise high-risk patients in whom parenteral nutrition should be started perioperatively, and includes those of any age who are malnourished and who have a diagnosis of carcinoma of the esophagus, the gastroduodenum, the liver/gallbladder, or the pancreas; an intra-abdominal retroperitoneal sarcoma; or abdomi- nal carcinomatosis. Group 2 consists of well-nourished patients younger than age 40 years and with primary
carcinoma of any site or stage; usually they do not require parenteral nutrition. Group 3 comprise well-nourished patients over the age of 40 years or malnourished patients of all ages with malignancies of lymphoproliferative, genitourinary/gynecologic, or colorectal origin. Patients in this group need to be observed carefully, with the anticipation that IONIP will last from 7 to 10 days. If a complication occurs in patients in either Group 2 or 3, where IONIP is anticipated to be 10 days or longer, supportive parenteral nutrition should be started without delay.
To address the second question, using randomized prospective studies, several investigators have attempted to determine whether preoperative parenteral nutrition may correct malnutrition and consequently improve the eventual outcome of initially malnourished patients after major surgical procedures.
Holter and Fischer [55] randomized gastrointestinal tract cancer patients with a weight loss of more than 4.5 kg over a 2- to 3-month period. Thirty patients received parenteral nutrition for 72 hours before the operation; 26 did not. Twenty-eight patients with no or minimal weight loss served as controls. Major postoperative complica- tions occurred in 7.1%, 13.3%, and 19.2% of the well- nourished, malnourished patients receiving parenteral nutrition, and malnourished patients not receiving paren- teral nutrition, respectively. These differences were not significant.
Moghissi et al [58] alternately allocated patients with severe dysphagia presenting with resectable carcinoma of the esophagus to receive 5 to 7 days of preoperative par- enteral nutrition (35 kcal/kg/day and 0.18 to 0.20 g/kg of nitrogen/day; 10 patients) or an oral diet plus intrave- nous fluids, electrolytes, and dextrose with no nitrogen supply (5 patients). The distribution is skewed because some patients initially allocated to this group proved to have unresectable cancers and were then excluded from the study. No data are available regarding the nutritional status at admission, except that all patients had lost from 4 to 13 kg of weight. Nitrogen balance was negative (13
3 5 0 THE AMERICAN JOURNAL OFSURGERY VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
patients) or neutra ! (2 patients) before surgery. All pa- tients in the parenteral nutrition group reverted to a posi- tive balance preoperatively and remained so during the postoperative period. Patients on the oral diet remained in a negative nitrogen balance preoperatively and postoper- atively despite the infusion of dextrose. The number of patients was too small for adequate statistical analysis of the clinical outcomes, but the patients not treated with preoperative parenteral nutrition allegedly demonstrated inferior wound healing.
One hundred patients who were to undergo major resective surgery for gastrointestinal diseases were pro- spectively randomized by Bellantone et al [59] to receive either at least 7 days of preoperative parenteral nutrition or a standard hospital diet. Although an initial nutritional assessment was performed, the authors did not include this nutritional status data for all patients studied. When only malnourished patients were analyzed, the incidence of sepsis was lower in the group that received parenteral nutrition (21% versus 53.3%). Postoperative mortality was not significantly affected by preoperative parenteral nutrition, but there were too few high-risk patients for the observation to have meaning.
Heatley et al [60] randomly allocated 74 patients with a preoperative diagnosis of esophageal or gastric cancer to receive either a high protein calorie ward diet within the limits of oral tolerance or the same oral diet plus parenteral nutrition of 40 kcal/kg/day for 7 to 10 days preoperatively. The calorie:nitrogen ratio of the par- enteral nutrition was kept constant at 200:1; the ward diet consisted of 3,000 calories and 15 g of nitrogen daily, supplemented with oral multivitamins, and was also available in liquid form for patients in whom dysphagia prevented or limited solid food intake. There were no significant differences between the two groups as regards either preoperative weight loss, preoperative immunolog- ic status, or preoperative serum albumin levels. Among the 41 patients undergoing anastomotic procedures, no differences were found in the incidence of anastomotic leakage. Mortality was comparable between all patients in both groups. However, the wound infection rate was significantly lower in the group that received parenteral nutrition, in both normoalbuminemic and hypoalbumine- mic patients.
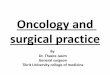
Muller et al [56] conducted a study of 125 patients with gastrointestinal carcinoma randomly assigned to re- ceive either 10 days of preoperative parenteral nutrition (1.5 g amino acids/kg/day; 11 g glucose/kg/day; 66 patients) or a regular hospital diet providing 2,400 kcai/ day (59 patients). Although 60% of all patients were considered malnourished at the time of admission, the randomization procedure did not consider this factor. Fortunately, the distribution of malnutrition was similar in both groups. The incidence of major complications (intra-abdominal abscess, peritonitis, anastomotic leak- age, and ileus) was significantly lower in the parenteral nutrition group (Figure 2). Postoperative mortality was also significantly reduced from 18% to 5% by preopera- tive parenteral nutrition. Unfortunately, the effects of
4O
30
i 20
10.
Wound infection
15
1
Pneumonia
23
20
14
N5 NS
Major N camp Jcotions
19
Mortality
11
p<O05 p < O 0 5
e lntroobd obsce:bs, peritonitis, anastornotic teokage, ileus
Controt group [ ] PPN group
Figure 2. Instances of major postoperative complications in pa- tients who received preoperative parenteral nutrition as com- pared with control subjects. Numbers on top of columns refer to number of cases. Reproduced with permission from [56],
parenteral nutrition were not separately analyzed for well-nourished and malnourished patients.
From these prospective randomized studies, it may be concluded that 2 to 3 days of intravenous nutrition prior to surgery does not improve surgical outcome, whereas parenteral nutrition for 5 to 7 day s may influence out- come. However, at least 7 to 10 days of preoperative parenteral nutrition resulted in a significant reduction of postoperative major complications and mortality. Implic- it in the use of an arbitrary fixed duration of parenteral nutrition in these studies is the assumption that all mal- nourished patients require an equal period of nutrition repletion. The logical approach to determining the neces- sary length of preoperative parenteral nutrition would be to establish a standard endpoint for adequate nutritional repletion prior to operation. Since severe malnutrition is associated with muscle wasting, adductor pollicis muscle function (assessed via electrical stimulation of the ulnar nerve) may be used to evaluate nutritional repletion. Me- guid et al [54] have shown that the force-frequency curve and relaxation rate of the adductor pollicis muscle are sensitive and specific measures of nutrient repletion; im- paired relaxation rates improve with the provision of nu- trients prior to operation.
Addressing the third question of the usefulness of postoperative nutritional support, it is well to remember that after an operation, patients undergo a period of fast- ing or inadequate oral intake for several days, because early postoperative oral feeding may cause nausea, vomit- ing, abdominal distention, and acute dilatation of the stomach because of delayed gastric emptying. Although most patients with an adequate preoperative nutritional status appear to pass through this period without deleteri- ous consequences, the question arises whether the provi- sion of nutritional support immediately following a gas-
THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990 351

MEGUID ET AL
o ~
8 8
r
.~ - ~ ~ ^ . ~ ~ ~
v ~ ~ ~ ~^
8
~ ~ ~ - ~ ~!~ ~ ~ . . . . ~ - - o
V V Z
c
UJ c . c - - ~ - ~
i i ~
| o, Z LU
A .~..~.
~ -~
o
.c
i
+
o
O 0 O 0
o
i , , ,~ ~ - ~ ~_
z O_
z z ,~, LU I.U
E E
~a ~a ~a
~< ~ ~ z z z uJ LU UJ
_ _~ .~ ~ _~
~ ~ ~8~ i
3 5 2 THE AMERICAN JOURNAL OFSURGERY "VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
Z LU
A Z 13_
_o .~_
o o c ~ ~| o~o
E
o E
._
o
. ~ ,~-
o Q-
Z
" o " o
e } a e e
~- < o E s
.s
w
+
E
~ o z C U.I
n
o
ii
II
II r~ m
II ku ILl r
&
"~= II
Z
II
g E
II
E w
g
)
II Z w
g
n
trointestinal operation might reduce postoperative morbidity and mortality, even in those who were not initially malnourished.
Some of the controlled studies addressing the use of nutritional support in the postoperative period are sum- marized in Table IV. In the study by Collins et al [61], parenteral nutrition was effective in reducing the length of hospital stay and in promoting perineal wound healing compared with a group of control subjects receiving oral alimentation only or a group receiving intravenous amino acids only. In a study by Yamada et al [62], parenteral nutrition was effective in maintaining nutritional status and increasing the disease-free interval in patients after gastrectomy for cancer. In the Preshaw et al [63] study of patients who were not malnourished, the provision of parenteral nutrition did not reduce the incidence of anas- tomotic leakage after colonic resection.
An alternative to parenteral nutrition in patients who undergo upper gastrointestinal tract, pancreaticobiliary, or colorectal procedures is enteral nutrition by means of an elemental diet delivered through a needle catheter jejunostomy. The rationale for this approach is that, al- though dysfunction of the stomach usually prevents oral or gastric feeding after operation, the small bowel almost immediately regains its motility and absorbs nutrients, allowing the infusion of enteral nutrition. An elemental diet seems ideal for postoperative feeding, since it is predi- gested and is almost totally absorbed [64]; a non-elemen- tal diet may be equally effective [65].
Some of the studies evaluating the use of elemental Or non-elemental diets given as enteral nutrition in the post- operative period are also summarized in Table IV. When enteral nutrition was compared with oral alimentation by Sagar et al [64] and Moore and Jones [66], it resulted in distinct nutritional advantages such as reduced weight loss and improved nitrogen balance and energy intake; it also prevented the decreases in total body potassium, serum transferrin, serum pre-albumin, and arm muscle circumference observed in control subjects. Furthermore, enteral nutrition decreased the incidence of sepsis and the hospital stay as compared with these parameters in con- trois. Finally, when postoperative parenteral nutrition was compared with postoperative enteral nutrition by Yeung et al [67], Adams et al [68], Bower et al [69], Heylen et al [70], and Muggia-Sullam et al [71], both enteral nutrition and parenteral nutrition were consid- ered equally effective as methods of nutritional support.
Thus, when compared with control patients, the provi- sion of postoperative nutritional support, either as paren- teral nutrition or enteral nutrition, is effective in improv- ing or maintaining the nutritional status. However, nutritional support is likely to reduce surgical morbidity and mortality only when given to malnourished patients.
Since comparisons of enteral nutrition or parenteral nutrition showed that both are equally effective for pro- viding nutritional support, the reduced cost of enteral nutrition as compared with parenteral nutrition and the recent evidence of Thompson et al [72] and Alverdy et al [73] that enteral nutrition is more physiologic in main- taining gastrointestinal integrity, make enteral nutrition the preferred choice of enteral support in the postopera-
T H E A M E R I C A N J O U R N A L O F S U R G E R Y V O L U M E 159 M A R C H 1990 3 5 3

MEGUID ET AL
TABLE V Surgical Trials Evaluating the Use of Parenteral Nutrition
( P N ) In Operations for Cancer
Major Complications Operative Mortality* Reference PN Counted PN Counted
[55] 4/30 (13) t 5/26 (19) 2 /30 (7) 2126 (8) [56] 11166 (17) 19/59 (32) 3/66 (5) 11/59 (19) [58] - - - - 1/25 (4) 5/27 (19) [60] 2/38 (5) 3 /36 (8) 6 /38 (16) 8/36 (22)
" Death in hospital within 30 days of surgery; PN versus control: decreased mortality (p = 0.02), major complications (p = 0.01), and wound infection (p = 0.05).
Numbers in parentheses are percentages. Adapted from [ 78l.
tive period after esophagogastric, pancreaticobiliary, or colorectal operations to malnourished patients or after laparotomy in trauma patients. Future studies should seek to identify other areas in which enteral nutrition might be preferable to parenteral nutrition.
Nutritional support in patients with cancer: Cancer patients are at high risk of developing malnutrition be- cause the presence of malignant disease is often associ- ated with reduced oral intake from anorexia and with altered metabolism. Also, cancer treatment, i.e., exten- sive surgery, chemotherapy, and radiotherapy, may pro- duee additional nutritional wasting in already nutrition- ally compromised patients.
Several retrospective studies have evaluated the use of parenteral nutrition in cancer patients. Some of these studies have reported improvements in postoperative morbidity and mortality and improvements in treatment tolerance, tumor response, and survival after radiothera- py and chemotherapy, as compared with patients not receiving parenteral nutrition. Despite the unresolved questions of potential tumor growth stimulation by exog- enous nutrients and whether nutritional support preferen- tially benefits host or tumor recently reviewed by Toro- sian et al [74], early anecdotal studies led to widespread use of parenteral nutrition in cancer patients during vari- ous forms of treatment. It has been estimated by Brennan et al [75] that about 33% of all patients receiving paren- teral nutrition every year have some form of cancer. However, many of the reported trials have been poorly designed and have included heterogeneous patient popu- lations that were frequently not stratified by stage of disease or degree of malnutrition. Some studies also in- cluded patients with advanced disease in whom there was a relative likelihood of response to cancer treatment re- gardless of nutritional status. Additionally, subjective analyses of the data have resulted in divergent conclu- sions between different authors, each reviewing the same literature [76,77].
In order to objectively combine results from compara- tive clinical trials, Klein et al [78] analyzed all the pro- spective randomized controlled trials of parenteral nutri- tion in cancer patients available in the English literature until 1986. The use of parenteral nutrition was defined as
provision of complete caloric and protein requirements through a central venous line for more than 24 hours. Of more than 100 reports identified in the initial search, 28 separate trials met these criteria. The quality of the re- ports was judged by a set of criteria regarding the quality of reporting, including the populations under study, ther- apy planned and used, study design, patient accounting, data quality, censored data, and statistical analysis. Con- sidering all these criteria for quality of reporting, in only 46% of the studies were these items reported.
The results of these studies were pooled regarding major endpoints, including survival, surgical complica- tions and mortality, chemotherapy toxicity, tolerance to radiotherapy, tumor response, and infection rates. Some of the controlled studies evaluating parenteral nutrition in surgical trials are presented in Table V. The pooled anal- ysis of parenteral nutrition use in the 11 suitable studies indicated a significant decrease in major complications, wound infection, and mortality with the use of parenteral nutrition as compared with no parenteral nutrition. The pooled analysis evaluating the use of parenterai nutrition during chemotherapy showed that parenteral nutrition had no statistical influence on survival rate, treatment toxicity, or tumor response to therapy. Furthermore, pa- tients receiving parenteral nutrition had a statistically significant increase in infection rate as compared with control subjects. Only four studies evaluating parenteral nutrition in patients receiving radiotherapy met the crite- ria of Klein et al [78] for analysis. No statistical differ- ences were found in survival rate and treatment tolerance with the use of parenteral nutrition as compared with no parenteral nutrition.
The approach used in the study of Klein et al [78] was very useful in reducing the subjective interpretation of results. However, among the risks involved in using this approach are that the reporting quality of a study may not necessarily be closely related to the scientific quality of the study, and that the small sample sizes used in individual studies and the inability to pool data on some endpoints resulted in the high probability of missing a therapeutic benefit. Additionally, because many trials excluded severely malnourished patients, the potential benefits of parenteral nutrition in severely malnourished patients could not be assessed.
Nine prospective randomized trials of the use of nutri- tional support during radiotherapy were collected in a recent review by Donaldson [79]. Analysis of these pro- spective trials showed that nutritional support failed to show a benefit in terms of either improved response to treatment, improved local disease control, improved sur- vival rates, or reduction of complications from radiation therapy.
The increased incidence of infection in chemotherapy patients receiving parenteral nutrition underscores the need for skilled nutritional teams when parenteral nutri- tion is administered [80] and argues against the routine use of parenteral nutrition in all cancer patients. A recent randomized prospective multicenter study by Evans et al [81] on the use of oral nutritional support versus ad libitum alimentation for 12 weeks during chemotherapy
3 5 4 THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
for advanced colorectal and non-small-cell lung cancer also failed to show any significant differences in response rate, median time of progression, degree of toxicity expe- rienced, or overall survival duration when the nutrition intervention groups were compared with the control group. However, it still seems likely that certain groups of malnourished patients would benefit from the effective adjuvant use of parenteral nutrition during their cancer treatment, especially when surgical treatment is planned. In that case, benefits of parenteral nutrition are more likely to be observed when parenteral nutrition is started 7 to 10 days before surgery. Future well-designed pro- spective randomized controlled trials, preferentially mul- ticenter trials, are still needed in order to identify patients with cancer who would benefit from nutritional support, particularly with the advent of newer anticancer therapy, e.g., bone marrow transplantation, since the use of paren- teral nutrition has been shown by Weisdorf et al [82] to be efficacious with this form of cancer treatment.
Hypereatabolie states: The nutritional status of pa- tients with acute trauma was studied by Moore and Jones [66] in 100 consecutive patients. Mean triceps skinfold thickness was 98% of normal. Arm muscle circumference was greater than 90% of normal in 94 patients; the mean was 108%. The creatinine/height index ranged from 73% to 149%; the mean was 116%. Seventeen of these patients had a creatinine/height index greater than 100%. Serum transferrin was less than 200 mg/dL in 49 patients, and the mean was 192 4- 6 mg/dL for the entire group. Total lymphocyte counts varied considerably, but the mean value was 1,973 4- 134/mm 3. Delayed hypersensitivity testing revealed anergy in 38% in patients, relative anergy in 33%, and normal reactivity in 29%. Serum albumin levels were generally low after laparotomy for trauma. The mean albumin level was 3.3 4- 0.1 g/dL for the 100 patients; 60 patients had values below 3.5 g/dL. The average nitrogen loss in the 24 hours after laparotomy was 12.8 g, and 32 of the patients had losses greater than 15 g. The prognostic nutritional index ranged from 14 to 86, and 50 patients had values in excess of 50.
Because earlier work had established that initial sup- port can minimize nutritional losses in hypercatabolic patients, it is not ethically acceptable to randomly assign patients to nutritional support versus starvation. As soon as hemodynamic stability is reached, nutritional support is generally given to reduce the otherwise inevitable con- siderable loss of body protein.
The results of the study by Moore and Jones [66] comparing enteral nutrition versus oral feeding after lap- arotomy for acute trauma and of the study by Adams et al [68] comparing enteral nutrition versus parenteral nu- trition after laparotomy for trauma are also summarized in Table IV.
Some studies have evaluated the best route to deliver nutrients in trauma patients. The overall results indicated that early postoperative enteral nutrition feeding via je- junostomy was as efficacious as parenteral nutrition for patients with multiple trauma undergoing laparotomy. Additionally, it was less expensive and therefore clearly cost-effective.
There is currently much concern as to the appropriate composition of the nutrient solution and its effects on body composition. Although several studies have exam- ined the amino acid composition that should be used in stressed patients with respect to the proportion of branched-chain amino acids (BCAA) present in the solu- tion, others have examined the nonprotein caloric sources, especially the use of parenteral lipids in stressed and trauma patients.
One of the many prospective randomized double- blind trials concerning the effects of varying BCAA con- tent was conducted by Cerra et al [83] in 23 hypercatabo- lic surgical patients. The group receiving a 45% BCAA-enriched parenteral nutrition solution had im- proved nitrogen retention, elevation of their absolute lym- phocyte count, improved plasma transferrin levels, and reversal of anergy to skin test antigens in 60% of the patients. However, no difference in morbidity or mortali- ty was observed in the group receiving the BCAA-en- riched parenteral nutrition solution as compared with the group receiving conventional parenteral nutrition solu- tions. Bonau and co-workers [84] conducted a prospec- tive clinical study in 13 patients who underwent radical cystectomy and ileal conduit diversion. Postoperatively, one group received a 45% BCAA-enriched solution and the other group received a 25% BCAA-enriched solution. Although there was increased muscle uptake of BCAA in the BCAA-enriched parenteral nutrition solution group, no difference was found in whole body nitrogen dynamics and no difference was observed in postoperative morbid- ity or mortality between the two groups. In a recent workshop reviewing the use of BCAA solutions in stress and injury, Brennan et al [85] concluded, from a review of cumulative data, that the use of BCAA-enriched solu- tions did not have a major effect on outcome, despite the positive results on indices of nitrogen metabolism noted in recent studies.
Sources of energy for patients undergoing surgical stress should include both carbohydrates and lipids. In the prospective randomized study of Meguid et al [86], it was observed that glucose tolerance with parenteral nu- trition was optimal when 30% to 50% of the caloric source was delivered as fat. Similar conclusions were reached by Burke et al [87], who determined the maximum rate of glucose utilization to be 15 g/hour in a variety of patho- physiologic conditions.
The use of lipid in parenteral nutrition is designed both to meet essential fatty acid needs and to avoid the undesirable effects of glucose overloading. Studies by Askanazi et al [88] and subsequently Nordenstrom et al [89] recommended that only the minimal amount of glu- cose (50 to 150 g or about 2 g/kg/day) should be sup- plied, using lipids for the remaining caloric requirements. With this amount of glucose, the central nervous system is adequately supplied with an essential energy source, and systemic acidosis and ketosis are prevented while the insulin levels remain low. Gluconeogenesis is reduced and mobilization of lipids is enhanced. A comprehensive re- view of this subject has recently been published by Gilder [901.
THE AMERICAN JOURNAL OFSURGERY VOLUME 159 MARCH 1990 355

MEGUID ET AL
Burns: No controlled trials have been done compar- ing parenteral isotonic glucose (D5W) with parenteral nutrition in patients with major burns (more than 40% total body surface area [TBSA]), and it is doubtful that such trials are ethical. However, a randomized prospec- tive study was done by Herndon et al [91] to ascertain whether supplementation of maximally tolerated oral cal- ories with parenteral nutrition during the first 10 days after the burn affected mortality.
Twenty-eight patients with burns of more than 50% TBSA who initially had poor gastrointestinal function (making it difficult for them to receive sufficient enteral nutrients to meet energy requirements) were randomly assigned to receive parenteral nutrition supplementation or no parenteral nutrition supplementation. The mean burn size of both groups was between 65% and 75%. Caloric requirements were calculated according to the Curreri formula: 25 kcal/kg body weight + 40 kcal • percent TBSA. After resuscitative fluid therapy was sta- bilized, 15 patients received hourly enteral feeding of milk or commercially prepared solutions, and 13 patients received supplementation of their oral caloric intake by parenteral nutrition. The supplemented group received significantly more calories per day versus the orally fed group, but in neither group was the total intake sufficient to meet the estimated caloric requirements of 4,550 kcal/ day, based on the mean burn size of 70%. Not surprising- ly, there was no difference in the survival rate between the two groups.
Alexander et al [92] randomly assigned 18 burned children to a control or a high protein group. The average burned TBSA was 60% in each group. Control patients were encouraged to voluntarily take as much of a normal balanced diet as they could; the diet was supplemented with a nutritionally complete liquid formula (Ensure or Osmolite, Ross Laboratories, Columbus, OH). Those who were unable to ingest sufficient calories voluntarily were tube fed; and when the gastrointestinal tract was intolerant of the needed caloric load, the intake was sup- plemented by parenteral nutrition. Patients assigned to the high protein group were also encouraged to take as much of a normal hospital diet as they could; their oral diet was supplemented with whey protein to the extent that approximately 25% of oral intake was protein. Sup- plemental parenteral nutrition was given to meet total caloric requirements.
The normal protein group received 87.1% of the de- sired total caloric intake, with 16.5% of the calories from protein, compared with 77.7% of desired total caloric intake, with 23.0% of calories from protein for the high protein group. Despite a slightly higher total caloric in- take in the control group, as compared with the high protein group, the normal protein control group had a significantly worse opsonic index, lower levels of IgG, lower levels of transferrin and/or serum protein, more bacteremic days, and poorer survival. These studies pro- vide evidence that many immunologic functions are de- pendent upon adequate protein intake, and that routine diets may not provide sufficient protein to satisfy the needs of seriously burned children.
R E F E R E N C E S 1. Baker JP, Detsky AS, Wesson DE, et al. Nutritional assessment: a comparison of clinical judgment and objective measurements. N Engl J Med 1982; 306: 969-72. 2. Detsky AS, Baker JP, Mendelson RA, Wolman SL, Wesson DE, Jeejeebhoy KN. Evaluation of accuracy of nutritional assessment techniques applied to hospitalized patients: methodology and com- parisons. JPEN J Parenter Enteral Nutr 1984; 8: 153-9. 3. Pettigrew RA, Charlesworth PM, Farmilo RW, Hill GL. As- sessment of nutritional depletion and immune competence: a com- parison of clinical examination and objective measurements. JPEN J Parenter Enteral Nutr 1984; 8: 21-4. 4. Durnin JUGA, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr 1974; 32: 77-97. 5. Heymsfield SB, Olafson RP, Utner MH, Nixon DW. A radio- graphic method of quantifying protein-calorie malnutrition. Am J Clin Nutr 1979; 32: 693-702. 6. Jeejeebhoy KN, Baker JP, Wolman SL, et al. Critical evaluation of the role of clinical assessment and body composition studies in patients with malnutrition and after total parenteral nutrition. Am J Clin Nutr 1982; 35 (suppl): 1117-27. 7. Collins JP, McCarthy ID, Hill GL. Assessment of protein nutri- tion in surgical patients--the value of anthropometrics. Am J Clin Nutr 1979; 32: 1527-30. 8. Studley HO. Percentage of weight loss: a basic indicator of surgical risk in patients with chronic peptic ulcer. JAMA 1936; 106: 458-60. 9. Morgan DB, Hill GL, Burkenshaw L. The assessment of weight loss from a single measurement of body weight: the problems and limitations. Am J Clin Nutr 1980; 33: 2101-5. 10. Blackburn GL, Bistrian BR, Maini BS, Schlamm HT, Smith MF. Nutritional and metabolic assessment of the hospitalized pa- tient. JPEN J Parenter Enteral Nutr 1977; 1: 11-22. 11. Seltzer MH, Sloeum BA, Cataldi-Betcher EL, et al. Instant assessment: absolute weight loss and surgical mortality. JPEN J Parenter Enteral Nutr 1982; 6: 218-21. 12. Mughal MM, Meguid MM. The effect of nutritional status on morbidity after elective surgery for benign gastrointestinal disease. JPEN J Parenter Enteral Nutr 1987; 11: 140-3. 13. Seltzer MH, Bastidas JA, Cooper DM, Engler P, Slocum B, Fletcher SH. Instant nutritional assessment. JPEN J Parenter En- teral Nutr 1979; 3: 157-9, 14. Reinhardt GF, Mycofski JW, Wilkens DB, et al. Incidence and mortality of hypoalbuminemic patients and hospitalized veterans. JPEN J Parenter Enteral Nutr 1980; 4: 357-9. 15. Bistrian BR, Blackburn GL, Hollwell H, Heddle R. Protein status of general surgical patients. JAMA 1974; 230: 858-60. 16. Kaminski MV, Fitzgerald M J, Murphy R J, et al. Correlation of mortality with serum transferrin and anergy (abstr). JPEN J Parenter Enteral Nutr 1977; 1: 40. 17. Blackburn GL, Bistrian BR, Harvey K. Indices of protein- calorie malnutrition as predictors of survival. In: Levenson SM, ed. Nutritional assessment--present status, future directions and pros- pects. Columbus, OH: Ross Laboratories, 1981: 131-7. 18. Fletcher JP, Little JM, Guest PK. A comparison of serum transferrin and serum prealbumin as nutritional parameters. JPEN J Parenter Enteral Nutr 1987; 11: 144-8. 19. Roza AM, Tuitt D, Shizgal HM. Transferrin--a poor measure of nutritional status. JPEN J Parenter Enteral Nutr 1984; 8: 523-8. 20. Ryan JA, Taft DA. Preoperative nutritional assessment does not predict morbidity and mortality in abdominal operations. Surg Forum 1980; 31: 96-8. 21. Starker PM, Gump FE, Askanazi J, Elwyn DH, Kinney JM. Serum albumin levels as an index of nutritional support. Surgery 1982; 91: 194-9. 22. Merritt R J, Kalsch M, Roux LD, Ashley-Mius J, Siegel SS. Significance of hypoalbuminemia in pediatric oncology patients--
356 THE AMERICAN JOURNAL OF SURGERY VOLUME 159 MARCH 1990

NUTRITIONAL SUPPORT IN SURGICAL PRACTICE
malnutrition or infection? JPEN J Parenter Enteral Nutr 1985; 9: 303-6. 23. Carpentier YA, Ingenbleek Y. Utilization of prealbumin as a nutritional parameter (letter). JPEN J Parenter Enteral Nutr 1986; 10: 435. 24. Fleck A. Acute phase response: implications for nutrition and recovery. Nutrition 1988; 4: 109-17. 25. McLaren DS. A fresh look at protein-energy malnutrition in the hospitalized patient. Nutrition 1988; 4: 1-12. 26. Greenblatt D J, Ransil B J, Harmatz JS, Smith W, Duhme DW, Koch-Weser J. Variability of 24-hour urinary creatinine excretion by normal subjects. J Clin Pharmacol 1976; 16: 321-328. 27. Forbes GB, Bruining GJ. Urinary creatinine excretion and lean body mass. Am J Clin Nutr 1976; 20: 1359-66. 28. Jeejeebhoy KN, Meguid MM. Assessment of nutritional status in the oncologic patient. Surg Clin North Am 1986; 66: 1077- 90. 29. Mullen JL, Gertner MH, Buzby GP, Goodhart GL, Rosato EF. Implications of malnutrition in the surgical patient. Arch Surg 1979; 114: 121-5. 30. Johnson WC, Ulrich F, Meguid MM, et al. Role of delayed hypersensitivity in predicting postoperative morbidity and mortali- ty. Am J Surg 1979; 137: 536-42. 31. Meakins JL, Christou NV, Shizgal HM, MacLean LD. Thera- peutic approaches to anergy in surgical patients. Ann Surg 1979; 190: 286-96. 32. Daly JM, Dudrick S J, Copeland EM. Effects of protein deple- tion and repletion on cell mediated immunity in experimental ani- mals. Ann Surg 1978; 188: 791-6. 33. Haffejee AA, Angorn lB. Nutritional status and the nonspecif- ic cellular and humoral immune response in esophageal carcinoma. Ann Surg 1979; 189: 475-79. 34. Harvey KB, Moldawer LL, Bistrian BR, Blackburn GL. Bio- logical measures for the formulation of a hospital prognostic index. Am J Clin Nutr 1981; 34: 2013-22. 35. Christou NV, Meakins JL. Neutrophil function in anergic surgical patients: neutrophil adherence and chemotaxis. Ann Surg 1979; 190: 557-64. 36. Copeland EM, MacFadyen BV, Dudrick SJ. Effect of intrave- nous hyperalimentation on established delayed hypersensitivity in the cancer patient. Ann Surg 1976; 184: 60-4. 37. Mullen JL, Buzby GP, Waldman MT, Gertner MH, Hobbs CL, Rosato EF. Prediction of operative morbidity and mortality by preoperative nutritional assessment. Surg Forum 1979; 30: 80-2. 38. Buzby GP, Mullen JP, Matthews DC, Hobbs CL, Rosato EF. Prognostic nutritional index in gastrointestinal surgery. Am J Surg 1980; 139: 160-7. 39. Moore FD, Oleson KH, McMurphy JD, Parker HV, Ball MR, Boyden CM. The body cell mass and its supporting environment. Body composition in health and disease. Philadelphia: WB Saun- ders, 1963. 40. Forse RA, Shizgal HM. The assessment of malnutrition. Sur- gery 1980; 88: 17-24. 41. Almond DJ, Burkinshaw L, Laughland A, McMahon M. Po- tassium depletion in surgical patients: intracellular action deficien- cy is independent of loss of body protein. Clin Nutr 1987; 6: 45-50. 4,2. Lukaski HC, Bolonchuk WW, Hall CB, Siders WA. Estima- tion of fat free mass in humans using the bioelectrical impedance method: a validation study. J Appl Physiol 1986; 60: 1327-32. 4,3. Meguid MM, Campos AC, Lukaski HC, Kiell C. A new single cell in vitro model to determine volume and sodium concentration changes by bioelectrical impedance analysis. Nutrition 1988; 4: 363-6. 44. Segal KR, Butin B, Presta E, Wang J, Vanltallie TB. Estima- tions of human body composition by bioelectrical impedance meth- ods: a comparative study. J Appl Physiol 1985; 58: 1565-71. 45. Kushner RF, Schoeller DA. Estimation of total body water by bioelectrical impedance analysis. Am J Clin Nutr 1986; 44: 417- 24.
46. Campos ACL, Chen M, Meguid MM. Comparisons of body composition derived from anthropomorphic and bioelectrical im- pedance methods. J Am Coil Nutr 1989; 8: 484-9. 47. Klidjian AM, Foster K J, Kammerling RM, Cooper A, Karran SJ. Anthropometric and dynamometric variables to serious postop- erative complications. Br Med J 1980; 281: 899-901. 48. Russell DMcR, Leiter LA, Whitwell J, Marliss EB, Jeejeebhoy KN. Skeletal muscle function during hypocaloric diets and fasting: a comparison with standard nutritional assessment parameters. Am J Clin Nutr 1983; 37: 133-8. 49. Russell DMcR, Pendergast P J, Darby PL, Garfinkel PE, Waitwell J, Jeejeebhoy KN. A comparison between muscle func- tion and body composition in anorexia nervosa: the effect of refeed- ing. Am J Clin Nutr 1983; 38: 229-37. 50. Russell DMcR, Walker PM, Leiter LA, et al. Metabolic and structural changes in skeletal muscle during hypocaloric dieting. Am J Clin Nutr 1984; 39: 503-13. 51. Fraser IM, Russell DMcR, Whittaker JS, et al. Skeletal and diaphragmatic muscle function in malnourished patients with chronic obstructive lung disease (abstr). Am Rev Respir Dis 1984; 129: A269. 52. Antonas KN, Curtas S, Meguid MM. Use of serum CPK-MM to monitor response to nutritional intervention in catabolic surgical patients. J Surg Res 1987; 42: 219-26. 53. DeLone JB, Curtas S, Jeejeebhoy JN, Meguid MM. Effect of operation and nutrient intake on muscle function and enzymes. Surg Forum 1987; 37: 36-9. 54. Meguid MM, Curtas S, Chen M, Nole E. Adductor pollicis muscle tests to detect and correct subclinical malnutrition in preop- erative cancer patients (abstr). Am J Clin Nutr 1987; 45: 843. 55. Holter AR, Fischer JE. The effects of perioperative hyperali- mentation on complications in patients with carcinoma and weight loss. J Surg Res 1977; 23: 31-4. 56. Muller JM, Dienst C, Brenner U, Pichlmaier H. Preoperative parenteral feeding in patients with gastrointestinal carcinoma. Lan- cet 1982; 1: 68-71. 57. Meguid MM, Campos ACL, Meguid V, Debonis D, Terz JJ. IONIP: a criterion of surgical outcome and patient selection for perioperative nutritional support. Br J Clin Prac 1988; 42: 8-14. 58. Moghissi K, Hornshaw J, Teasdale PR, Dawes EA. Parenteral nutrition in carcinoma of the esophagus treated by surgery: nitro- gen balance and clinical studies. Br J Surg 1977; 64: 125-128. 59. Bellantone R, Doglietto GB, Bossola M, et al. Preoperative parenteral nutrition in the high risk surgical patient. JPEN J Par- enter Enteral Nutr 1988; 12: 195-7. 60. Heatley RV, Williams RHP, Lewis MH. Preoperative intrave- nous feeding: a controlled trial. Postgrad Med J 1979; 55: 541-5. 61. Collins JP, Oxby CB, Hill GL. Intravenous amino acids and intravenous hyperalimentation as protein-sparing therapy after ma- jor surgery. A controlled clinical trial. Lancet 1978; 1: 788-91. 62. Yamada N, Koyama H, Hioki K, Yamada T, Yamamoto M. Effect of postoperative total parenteral nutrition (TPN) as an ad- junct to gastrectomy for advanced gastric carcinoma. Br J Surg 1983; 70: 267-74. 63. Preshaw RM, Attisha RP, Hollingsworth W J, Todd JD. Ran- domized sequential trial of parenteral nutrition in healing of colonic anastomoses in man. Can J Surg 1979; 22: 437-9. 64. Sagar S, Harland P, Shields R. Early postoperative feeding with elemental diet. Br Med J 1979; 1: 293-5. 65. Fick TE, van Rooyen W, Schattenkerk ME, Steller EP, Feen- stra BWA, Bruining HA. A nonelemental versus an elemental diet for early postoperative enteral feeding by needle catheter jejunos- tomy. Clin Nur 1986; 5: 105-7. 66. Moore EE, Jones TN. Nutritional assessment and preliminary report on early support of the trauma patient. J Am Coll Nutr 1983; 2: 45-54. 67. Yeung CK, Smith RD, Hill GL. Effect of an elemental diet on body composition. Comparison with intravenous nutrition. Gastro- enterology 1979; 77: 652-7.
THE AMERICAN JOURNAL OFSURGERY VOLUME 159 MARCH 1990 357

MEGUID ET AL
68. Adams S, Dellinger EP, Wertz M J, Oreskovich MR, Si- monowitz D, Johansen K. Enteral versus parenteral nutritional support following laparotomy for trauma: a randomized prospec- tive trial. J Trauma 1986; 26: 882-91. 69. Bower RH, Talamini MA, Sax HC, Hamilton F, Fischer JE. Postoperative enteral nutrition: a randomized controlled trial. Arch Surg 1986; 121: 1040-5. 70. Heylen AM, Lybeer MB, Penninckx FM, Kerremans RP, Frost PG. Parenteral versus needle jejunostomy nutrition after total gastrectomy. Clin Nutr 1987; 6: 131-6. 71. Muggia-Sullam M, Bower RH, Murphy RF, Joffe SN, Fischer JE. Postoperative enteral versus parenteral nutritional support in gastrointestinal surgery. A matched prospective study. Am J Surg 1985; 149: 106-12. 72. Thompson JS, Vaughan WP, Forst CF, Jacobs DL, Weekly JS, Rikkers LF. The effect of the route of nutrient delivery on gut structure and diamine oxidase levels. JPEN J Parenter Enteral Nutr 1987; 11: 28-32. 73. Alverdy JC, Aoys E, Moss GS. Total parenteral nutrition promotes bacterial translocation from the gut. Surgery 1988; 104: 185-90. 74. Torosian MH, Daly JM. Nutritional support in the cancer- bearing host. Effects on host and tumor. Cancer 1986; 58:1915-29. 75. Brennan MF. Total parenteral nutrition in the cancer patient. N Engl J Med 1981; 305: 375-82. 76. Koretz RL. Parenteral nutrition: is it oncologically logical? J Clin Oncol 1984; 2: 534-8. 77. Apelgren KN, Wilmore DW. Parenteral nutrition: is it oncolo- gically logical? A response. J Clin Oncol 1984; 2: 539-41. 78. Klein S, Simes J, Blackburn GL. Total parenteral nutrition and cancer clinical trials. Cancer 1986; 58: 1378-86. 79. Donaldson SS. Nutritional support as an adjunct to radiation therapy. JPEN J Parenter Enteral Nutr 1984; 8: 302-10. 80. Dalton M J, Schepers G, Gee JP, Alberts CC, Eckhauser FE, Kirking DM. Consultative total parenteral nutrition teams: the effect on the incidence of total parenteral nutrition-related compli- cations. JPEN J Parenter Enteral Nutr 1984; 8: 146-152.
81. Evans WK, Nixon DW, Daly JM, et al. A randomized study of oral nutritional support versus ad lib nutritional intake during che- motherapy for advanced colorectal and non-small-cell lung cancer. J Clin Oncol 1987; 5: 113-24. 82. Weisdorf SA, Lysne J, Wind D, et al. Positive effect of prophy- lactic total parenteral nutrition on long-term outcome of bone mar- row transplantation. Transplantation 1987; 43: 833-8. 83. Cerra FB, Mazuski JE, Chute E, et al. Branched chain meta- bolic support. A prospective, randomized, double-blind trial in sur- gical stress. Ann Surg 1984; 199: 286-91. 84. Bonau RA, Jeevanandam M, Moldawer L, et al. Muscle amino acid flux in patients receiving branched chain amino acid solutions after surgery. Surgery 1987; 101: 400-7. 85. Brennan MF, Cerra F, Daly JM, et al. Report of a research workshop: branched chain amino acid in stress and injury. JPEN J Parenter Enteral Nutr 1986; 10: 446-52. 86. Meguid MM, Akahoshi MP, Jeffers S, Hayaski R, Hammond WG. Amelioration of metabolic complications of conventional total parenteral nutrition. Arch Surg 1984; 119: 1294-8. 87. Burke JF, Wolfe RR, Mullany C J, Mathews DE, Bier DM. Glucose requirements following burn injury. Ann Surg 1979; 190: 274-85. 88. Askanazi J, Carpenter YA, Elwyn DH, et al. Influence of total parenteral nutrition on fuel utilization in injury and sepsis. Ann Surg 1980; 191: 40-6. 89. Nordenstrom J, Askanazi J, Elwyn DH, et al. Nitrogen bal- ance during total parenteral nutrition. Ann Surg 1983; 197: 27-33. 90. Gilder H. Parenteral nourishment of patients undergoing surgi- cal or traumatic stress. JPEN J Parenter Enteral Nutr 1986; 10: 88-9. 91. Herndon DN, Stein MD, Rutan TC, Abston S, Linares H. Failure of TPN supplementation to improve liver function, immuni- ty and mortality in thermally injured patients. J Trauma 1987; 27: 195-204. 92. Alexander JW, MacMillan BG, Stinett JO, et al. Beneficial effects of aggressive protein feeding in severely burned children. Ann Surg 1980; 505-17.
358 THE AMERICAN JOURNAL OFSURGERY VOLUME 159 MARCH 1990