Embed Size (px)
Citation preview

NVAC Vaccine Finance Working Group Update
Gus Birkhead, MD, MPH
Chair, NVAC Vaccine Working Group
September 26, 2006

Charge to Working Group
• Obtain input from stakeholders …on the challenges in creating optimal approaches to vaccine financing in both the public and private sectors, and their impact on access.
• Establish a process for selecting and addressing 2 – 3 key topics per year with input from the subcommittee chairs
• By the end of each year, have developed specific and targeted policy options for the first 2 – 3 topics, and be prepared to address another 2 – 3 topics in the following year.
• Present findings and policy options to the full NVAC for discussion and recommendations.

Working Group Membership
• NVAC– Gus Birkhead, chair– Jon Abramson– Jon Almquist– Mark Feinberg– Gary Freed– Lance Gordon– Alan Hinman– Calvin Johnson– Jerome Klein
• AHIP – Alan Rosenberg • Nat’l Business Group on
Health - Liz Greenbaum/Ron Finch
• Health Economist - Mark Pauley
• Academia - Walt Orenstein• Agency liaisons
– CDC – Lance Rodewald– CMS – Randy Ferris
• NVPO– Bruce Gellin, Angela
Shen, Ray Strikas, Emma English

IOM process• Study supported by CDC• Committee formed in 2002• Frank Sloan, chair• Four meetings• Commissioned survey of state vaccine
finance practices (Gary Freed)• Commissioned 8 background papers• Report previewed in late 2003• Report issued in 2004

Background papers - 1• Trends in vaccine prices, 1992-2002 (Frank
Lichtenberg)• Overview of market for vaccines in US
(Richard Arnold/Larry DeBrock)• How insurance companies and health
plans are planning for new vaccines (Kathy Swartz)
• Vaccine purchase and distribution: Proposed changes in vaccine supply and delivery policies
(Gerry Fairbrother/Arfana Haidery)
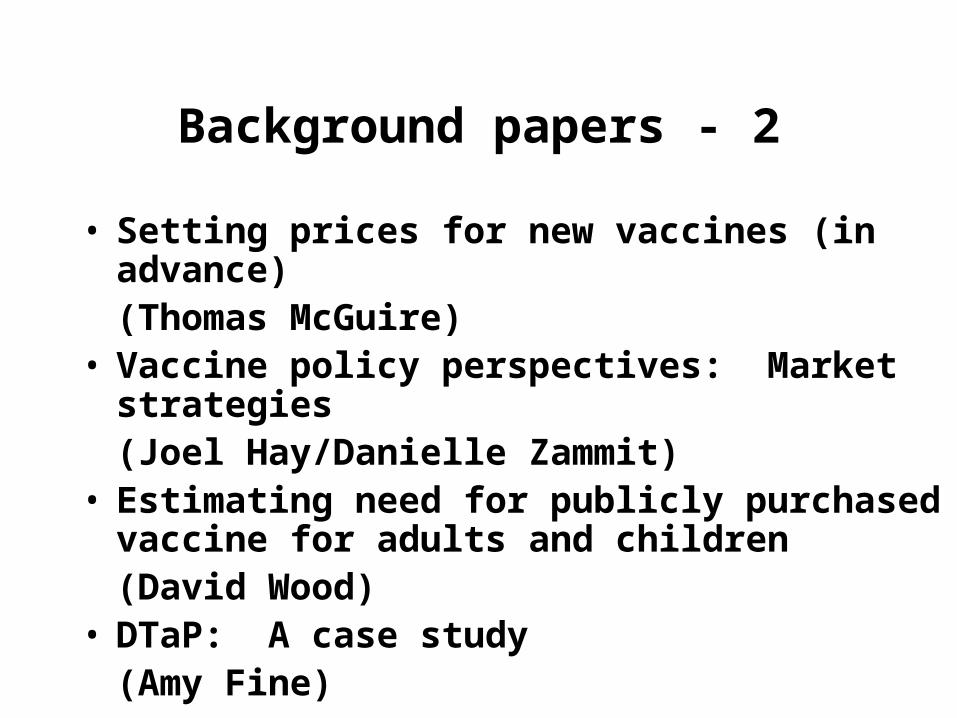
Background papers - 2
• Setting prices for new vaccines (in advance)(Thomas McGuire)
• Vaccine policy perspectives: Market strategies(Joel Hay/Danielle Zammit)
• Estimating need for publicly purchased vaccine for adults and children(David Wood)
• DTaP: A case study(Amy Fine)

IOM Recommendations
• New insurance mandate, government subsidy, and voucher plan for vaccines recommended by ACIP;
• Alter ACIP membership to associate vaccine coverage decisions with social benefits and costs, including price;
• NVPO convene stakeholders;• CDC initiate a research program to improve
measurement of the societal value of vaccines

2004 NVAC Workgroup
NVAC
Alan Hinman (co-chair)
Bruce Gellin (co-chair)
Ann Arvin
Jerry Klein
Pat Whitley-Williams
Non-NVAC
Steve Black (AHIP)
Ronan Gannon (GSK)
Bronwen Kaye (Wyeth)
Sarah Landry (NVPO)
David Neumann (PfP)
Lance Rodewald (CDC/NIP)
Una Ryan (AVANT)
Don Williamson (ASTHO)

Initial “environmental scan” of stakeholders
• “Informal”30-60 minute telephone interviews
• Vaccine companies (6)• Federal government agencies (2)• Public Health Agency organizations (3)• Provider organizations (3)• Payers/insurers (1)

NVAC Vaccine Financing MeetingJune 28-29, 2004
• 61 participants– Large manufacturers and biotech firms– Fed, state, local health departments– Distributors/purchasers– Health care providers– Consumers
• Pros and cons of options?• Additional options?• Which option supported and why?

Summary of June 28-29 meeting
• Agreement on:– Vaccines are
undervalued;– Assure access– Adequate reimbursement– Regulatory harmonization– Strengthen liability
protection– Better understand
insurance coverage– Better understand factors
responsible for low immunization coverage in adolescents and adults
• Little support for IOM proposal for mandate, subsidy, and voucher;
• Many favored improvements in current system:– Expanding VFC for
underinsured children– Removing VFC price caps– “Vaccine for Adults”– Increase Section 317 for
children, adolescents and adults.

NVAC recommendations - 2004
• Expand Section 317 and rapid appropriation when new vaccines recommended;
• Expand VFC: underinsured children in settings, remove price caps;
• Regulatory harmonization to facilitate vaccines licensed in other countries; increase communication;
• Promote “first dollar” insurance vaccine coverage, administration fees, and prompt coverage of new vaccines.

Where are we now?
• IOM proposal for mandate/subsidy/voucher has not been implemented
• ACIP procedures/membership remain the same (includes health economist)
• NVAC recommendations:– 317 essentially the same– VFC expansion proposed but not passed– Foreign vaccines not yet implemented
• Vaccine coverage rates still high (?)

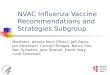
Vaccine financing stresses• Number of new, expensive vaccines
– Federal Contract Prices for Recommended Vaccines, Age 0-18, 1985 – 2006
– Private Sector Price - 2006
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
1985 Public 1995 Public 2006 Public 2006 Private
Dol
lars
Rotavirus
Influenza
2 Hep A
1 MCV
1 Td/ Tdap
4 PCV7
1 Var
3 Hep B
4 Hib
1 - 2 MMR
4 Polio
5 DTaP
$45$155
$837
$1214

Finance Working Group Focus
• September 7 – 1 ½ hour conference call• September 25 – 4 hour in-person meeting
• Issues impacting financing of pediatric vaccinations by practitioners
• Section 317 issues

Pediatric immunization delivery system
60.4%
24.2%
14.2%
Private PractitionersMixed Private/PublicPublic Health Depts.
Source: National Immunization Survey, 2004www.cdc.gov/nip/data
Private providers vaccinate most US children

Pediatric immunization delivery system
• Childhood vaccine doses in FY2004
Private Sector45%
State programs
7%
Federal Vaccines for
Children40%
Federal Section 317
8%
Source: Biologics Surveillance Data 2004 from vaccine manufacturers

Reimbursement Issues Impacting Practitioners
• Practices tie up capital in vaccine inventories
• Vaccine reimbursement uncertain– Uninsured or under insured– Insured children
• Delayed reimbursement• Inadequate reimbursement
• Vaccine administration variable

True Vaccination Costs• Purchase price of the vaccine. • Personnel costs for ordering and inventory. • Storage costs since the vaccines must be stored
in a refrigerator or freezer, which is depreciated. • Possible re-vaccination costs due to problems
with storage.• Insurance to insure against loss.• A 5% estimated wastage/non-payment due to
office collection rates, HMO discounts, bad debt, etc.
• Large sums tied up in vaccine inventory (e.g. 10 member pediatric group had $100,000 in vaccine inventory in 2005)

Vaccine Administration• Maximum allowable fee set by HCFA for each
state– Published in Federal Register September 2,
1994– Has never been updated or changed – No minimum administration fee– States match federal funding using their FMAP
rate• VFC providers are not allowed to turn away a
child for inability to pay the admin fee

Vaccine financing stresses
• True costs– Vaccine administration: current state
and CMS administration fees with max cap (2005)
$0
$2
$4
$6
$8
$10
$12
$14
$16
$18
CMS Contribution
State Contribution
Maximum Cap

Uncertainty of Reimbursement
• AHIP survey (61/140 - 44% response rate)– 91.8% follow ACIP recommendations– 62% of plans reimburse based on Thompson’s Average
Wholesale Price (published quarterly)– Only 47% of PPO’s who responded can act on ACIP
recommendations within 3 months– Most plans wait until final CDC recommendations are
published in MMWR
Source: AHIP Coverage. Immunization Practices and Policies. Jan-Feb 2006.
• Dual standard of care: VFC vaccine available first

American Academy of Pediatrics Vaccine Finance Task Force
• Key stakeholders meeting– Collaborating with AMA to address
comprehensive approach to financing– Holding conference calls prior to the
meeting to determine areas for negotiation
• ?involvement of NVPO/NVAC

Working Group Discussion• Government
– Establish Medicaid minimum administration fee– Folding administration fees into VFC
• Private Insurance– Timing of insurance coverage (?MMWR)
– Define “appropriate reimbursement”: • Vaccine Manufacturers
– Financing initial inventory costs e.g. just in time inventory (deferred payment)
– Deferred payment through a “revolving fund”
• Need for more data– Physician survey on impact of financing issues– State survey of Section 317 issues

Next Steps
• Additional presentations:– ERISA, – business perspective
• Exploration of discussion ideas– Minimum administration fee– Financing initial inventory
• Section 317 issues• AAP Vaccine Finance Taskforce












![Vaccine Safety Activities: National Vaccine Advisory ... · NVAC [National Vaccine Advisory Committee] thatthat includesincludes representatives representatives of a wide variety](https://img.pdfslide.net/doc/110x75/5e877b900e33286fbe50e6a3/vaccine-safety-activities-national-vaccine-advisory-nvac-national-vaccine.jpg)