Embed Size (px)
Citation preview

O2 Therapy & Air way management techniques
Abdualrahman ALshehri
Lecturer
King Saud University
Riyadh Community College
RN, MSN

Respiratory Anatomy
Nose and mouth (warms, moistens, and filters air).
Pharynx
–Oropharynx
–Nasopharynx
Epiglottis
Trachea (windpipe)

Respiratory Anatomy
Cricoid cartilage (adams apple).
Larynx (voice box).
Bronchi
Lungs
–Visceral pleura (surface of lungs)
–Parietal pleura (internal chest wall)
–Interpleural space (potential space)

Respiratory Anatomy
Diaphragm
Inhalation (active process)
–Diaphragm and intercostal muscles contract, increasing the size of the thoracic cavity.
–Diaphragm moves slightly downward, ribs move upward and outward.
Air flows into the lungs creating a negative pressure in the chest cavity.

Respiratory Anatomy
Exhalation (passive process)
Diaphragm and intercostal muscles relax decreasing the size of the thoracic cavity.
–Diaphragm moves upward, ribs move downward and inward.
Air flows out of the lungs creating a positive pressure inside the chest cavity.

Respiratory Physiology
Oxygenation - blood and the cells become saturated with oxygen
Hypoxia - inadequate oxygen being delivered to the cells
Signs of Hypoxia
– Increased or decreased heart rate
– Altered mental status (early sign)
– Agitation
– Initial elevation of B.P. followed by a decrease
– Cyanosis (often a late sign)

Alveolar/Capillary Exchange
Oxygen-rich air enters the alveoli during each inspiration.
Oxygen-poor blood in the capillaries passes into the alveoli.
Oxygen enters the capillaries as carbon dioxide enters the alveoli.

Capillary/Cellular Exchange
Cells give up carbon dioxide to the capillaries.
Capillaries give up oxygen to the cells.

Functions of the Respiratory System: Overview
Exchange O2
–Air to blood
–Blood to cells
Exchange CO2
–Cells to blood
–Blood to air
Regulate blood pH
Vocalizations
Protect alveoli

Factors Affecting Ventilation
Airway Resistance
Diameter
Mucous blockage
Bronchoconstriction
Bronchodilation
Alveolar compliance
1. Surfactants
2. Surface tension
Alveolar elasticity

Page 11
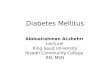
Gas Exchange in the Alveoli
Thin cells: exchange
Surfactant cells
Elastic fibers
– Recoil
– Push air out
Thin basement membrane
Capillaries cover 90% of surface

Page 12
Gas Exchange in the Alveoli

Page 13
Oxygen movement

Page 14
Oxygen movement

Page 15
Oxygen movement

Page 16
Oxygen Therapy
For over 200 years oxygen therapy has often been used and sometimes misused (Hough 2001)

Page 17
Oxygen Therapy
Should be prescribed
Acute and chronic respiratory conditions
Personnel should be trained in its use
Protocols

Page 18
Oxygen Therapy - Indications
Hypoxaemia (PaO2<8KPA, O2sats<90%)
Acute or chronic respiratory condition
Pre and post suction
Routinely post operatively
Optimise oxygen delivery

Page 19
Oxygen therapy - limitations
Giving oxygen does not guarantee it’s arrival at the mitochondria
Oxygen does not improve ventilation directly
(Hough 2001)

Page 20
Oxygen therapy – complications/cautions
Respiratory depression if hypoxic drive
Pulmonary oxygen toxicity
Tracheobronchitis
Absorption atelectasis
Fire
Variable delivery

Page 21
Oxygen Therapy - Monitoring
Oxygen saturations continuous/intermittent
Arterial blood gases
Observation

Page 22
Oxygen therapy – delivery devices
Low Flow masks (variable performance)
High flow masks (fixed flow)/venturi
Nasal cannulae
Mask and reservoir bag
Tracheal mask/t-piece
Tracheal speaking valves
Mechanical ventilator

Page 23
Oxygen Therapy - low flow masks
Commonly used
Variable performance

Page 24
Oxygen therapy – high flow masks
Guaranteed percentage of oxygen
Venturi system
More expensive
Up to 60%

Page 25
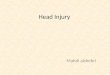
Nasal cannulae
1l/min 24% oxygen
2l/min 28% oxygen
3l/min 32% oxygen
4l/min 36% oxygen

Page 26
Oxygen therapy – bag and mask
High concentrations of oxygen
Mask and reservoir bag
55-90%

Page 27
Oxygen Therapy tracheostomy
T-piece
Mask
Swedish nose
Speaking valve

Page 28
Long term oxygen therapy
Chronic hypoxaemia
Increases survival
Aim to raise PaO2 to >8Kpa
Worn as much as possible >15hours
Cylinders/concentrators/liquid

Page 29
Humidification
Mucocillary escalator
Adequate hydration is vital
Bacterial contamination!!!

Page 30
Humidification - indications
URT bypassed
Thick retained secretions
High flow oxygen/non-invasive mechanical aids

Page 31
Humidification - Cautions
Hyper-reactive airways - bronchospasm
Infection
Burns

Page 32
Humidification - Types
Nebulisers Large/Small/Ultrasonic
Steam

Page 33
Humidification - Humidifiers
Hot - Increases moisture content
- Increases risk of infection
Cold - Poor moisture content

Page 34
Non-invasive ventilation
BiPAP
CPAP
IPPB

Page 35