Embed Size (px)
Citation preview

Obesity and Pregnancy
Vanessa H. Gregg, MDAssistant Professor of OB/Gyn
University of Virginia

Objectives
Review maternal complications of obesity in pregnancy
Review fetal/neonatal complications of obesity in pregnancy
Discuss long-term implications Review practical issues in the
management of obese pregnant women

Obesity in America
Greater than 60% of Americans are overweight (BMI 25 to <30) Of those, half are obese, with a BMI of
30 or greater In Virginia, 26% of residents are
obese

Percent of adults who are obese in Virginia, 2008
http://apps.nccd.cdc.gov/DDT_STRS2/CountyPrevalenceData.aspx?mode=OBS

Defining Obesity
Overweight = BMI 25-29.9 Obesity:
Class 1 = BMI 30-34.9 Class 2 = BMI 35-39.9 Class 3 = BMI > 40

Obesity and Pregnancy
Increasing prevalence of obesity in pregnancy
Between 1993 and 2003 the rate of pre-pregnancy obesity increased 69%
Approximately 1 in 5 pregnant women in America is obese.
Kim SY, Dietz PM, England L, Morrow B, Callaghan WM. Trends in pre-pregnancy obesity in nine states, 1993-2003. Obesity (Silver Spring). 2007 Apr;15(4):986-93.

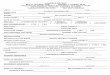
Maternal Complications
Higher Rates of Cesarean Section Gestational Hypertension Pre-eclampsia Gestational Diabetes LGA and Shoulder dystocia Stillbirth DVT/PE Anesthetic complications
Maternal Complications
Complication BMI 19.8-26 BMI 35-40 BMI >40
Pre-eclampsia 1.4% 3.4% (OR 3.90) 3.5% (OR 4.82)
Cesarean section
10.9% 21.5% (OR 2.32)
24.2% (OR 2.69)
Shoulder dystocia
0.1% 0.4% (OR 2.82) 0.4% (OR 3.14)
Large for gestational age
OR 3.11 OR 3.82
Cedergren, MI. Maternal Morbid Obesity and the Risk of Adverse Pregnancy Outcome. Obstet Gynecol, Vol 103, No 2. Feb 2004.

Risk of Cesarean Section
Increased risk due to: Dysfunctional labor Monitoring challenges Increased rates of pre-eclampsia,
hypertension and LGA babies all contribute to likelihood of cesarean section

Cesarean Section – Clinical Challenges
Access to lower uterine segment can be challenging
Higher rate of wound complications after surgery
Higher risk of anesthetic complications

Gestational Hypertension
Pre-existing hypertension is more common among obese women
Among those without hypertension at baseline, increased risk of developing gestational hypertension

Gestational Hypertension
Population-based study in the Netherlands
Increased rates of gestational hypertension among obese women (BMI >35), with odds ratio 4.67
Gaillard R et al. Associations of maternal obesity with blood pressure and the risks of gestational hypertensive disorders.
Journal of Hypertension 2011, 29:937-944.
Gestational Hypertension: A UK population-based study
Among extremely obese women (BMI >50): 1 in 5 develop hypertensive disorder in
pregnancy 1 in ten develop pre-eclampsia
Among women with less severe obesity, risk is increased but to a lesser degree
Knight, M et al. Extreme Obesity in Pregnancy in the UK. Obstet Gynecol, Vol 115, No 5. May 2010.

Pre-eclampsia
Risk of pre-eclampsia is increased in obese pregnant women
Pre-eclampsia can lead to compromised fetal perfusion and to medically-indicated preterm birth.

Pre-Eclampsia
In same population-based study in Netherlands, increased risk of pre-eclampsia was observed for obese women (BMI >35), with odds ratio of 2.5.
Gaillard R et al. Associations of maternal obesity with blood pressure and the risks of gestational hypertensive disorders. Journal of Hypertension 2011, 29:937-944.

Gestational Diabetes
Gestational diabetes is more common in obese pregnant women
In addition, there is a higher rate of pre-existing diabetes in obese pregnant women

Gestational Diabetes: A UK population-based study
Among extremely obese women, 11% developed gestational diabetes Of those, 70% required insulin Risk of developing diabetes was seven
times higher than in non-obese controls Among women with less severe
obesity, risk is increased but to a lesser degree
Knight, M et al. Extreme Obesity in Pregnancy in the UK. Obstet Gynecol, Vol 115, No 5. May 2010

Large for Gestational Age and Shoulder Dystocia
Maternal obesity predisposes to increased size of babies at birth.
Increased fetal adipose tissue, especially in the fetal abdomen, increases risk of shoulder dystocia
Shoulder dystocia carries additional morbidity to mother and baby.

Risk of Stillbirth
There is an increased risk of stillbirth associated with obesity
Risk of stillbirth increases with severity of obesity

Cohort Study of Rates of Stillbirth
One study of birth cohort in Missouri 1978-1997 examined >1.5 million births:
Obese mothers were 40% more likely to experience stillbirth
Salihu, HM et al. Extreme Obesity and Risk of Stillbirth Among Black and White Gravidas. Obstet Gynecol 2007; 110:552-7.

Cohort Study of Rates of Stillbirth
There was significant racial disparity, with higher rates of stillbirth among black women than white women
Disparity widened with increasing BMI, with disproportionately highest stillbirth among extremely obese black women (BMI > 40).
Salihu, HM et al. Extreme Obesity and Risk of Stillbirth Among Black and White Gravidas. Obstet Gynecol 2007; 110:552-7.

DVT/PE
Immobilization and pregnancy are both risk factors for DVT/PE
Obese pregnant women often have decreased mobility, particularly with extreme obesity
Cesarean delivery further increases the risk

Anesthetic Complications
Inability to establish regional block Insufficient duration of regional block Longer time to establish anesthesia Refractory hypotension from
anesthetic agents Increased postdural puncture
headache
Vricella LK et al. Anesthesia Complications During Scheduled Cesarean Delivery for Morbidly Obese Women.
Am J Obstet Gynecol 2010;203:276.e1-e5.

Fetal and Neonatal Complications
Stillbirth Fetal Distress in Labor Meconium Aspiration Neonatal Death

Fetal and Neonatal Complications
Complication BMI 19.8-26 BMI 35.1-40 BMI > 40
Stillbirth 0.3% 0.6% (OR 1.99) 0.8% (OR 2.79)
Fetal distress 2.0% 3.5% (OR 2.13) 3.9% (OR 2.52)
Meconium aspiration
0.1% 0.3% (OR 2.87) 0.3% (OR 2.85)
Neonatal death 0.1% 0.3% (OR 2.09) 0.4% (OR 3.41)
Cedergren, MI. Maternal Morbid Obesity and the Risk of Adverse Pregnancy Outcome. Obstet Gynecol, Vol 103, No 2. Feb 2004.

Fetal and Neonatal Complications
As maternal BMI has risen, there has been a significant increase in the number of babies born with high birth weight.
Larger babies have more adipose tissue.
Surkan PJ, Hsieh CC, Johansson AL, Dickman PW, Cnattingius S. Reasons for increasing trends in large for gestational age births. Obstet Gynecol 2004; 104: 720-6.

What happens later in life for children born to obese mothers?
Children born to obese mothers are twice as likely to be obese and develop type 2 diabetes in adult life.
Higher maternal gestational weight gain has been associated with high blood pressure in offspring.
http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/PregComplications.html

Contemplating the mechanism
One study showed an association between maternal BMI and the hepatic lipid content in the infants.
The increased lipid content in the liver may initiate programming of the metabolic syndrome in utero.
Modi, N et al. The Influence of Maternal Body Mass Index on Infant Adiposity and Hepatic Lipid Content. Pediatric Research; Vol. 70, No. 3, 2011.

More Evidence: Early Menarche in Female Offspring
An NICHD study looked at age of menarche and found an association between maternal obesity and earlier menarche in female offspring.
There was also a correlation between maternal BMI and daughters’ BMI at age seven.
Kleim SA, Branum, AM, Klebanoff MA, Zemel BS. Maternal Body Mass Index and Daughters’ Age at Menarche. Epidemiology. Vol 20, Number 5, Sept 2009.

Effects of Early Menarche
Early puberty is associated with Glucose intolerance Hypertension Depression Breast Cancer
Kleim SA, Branum, AM, Klebanoff MA, Zemel BS. Maternal Body Mass Index and Daughters’ Age at Menarche. Epidemiology. Vol 20, Number 5, Sept 2009.

Optimal intrauterine growth affects long-term health
Inadequate and excessive fetal growth in utero both have the potential to predispose to the metabolic syndrome in adulthood.
Goal is “optimal” fetal growth, though this can be hard to define and achieve.

Optimal intrauterine growth affects long-term health
Maternal Obesity
Fetal Programming
Offspring Obesity and Metabolic
Syndrome
Practical Considerations
Increased utilization of healthcare resources
Difficult to use some of our routine prenatal surveillance tools
Increased hospital challenges

Utilization of Resources
Obesity in pregnancy is associated with: Longer hospital stays Greater use of health care services More obstetric ultrasounds More prescribed medications in
pregnancy
http://www.cdc.gov/media/pressrel/2008/r080402.htm

Clinic Challenges
Identifying fetal heart tones Assessing fetal growth
Fundal height difficult to obtain Assessing for hypertension
Blood pressure cuffs may be of inadequate size

Hospital Challenges
Monitoring Anesthesia
Identifying epidural space Airway protection
OR table limitations, surgeries technically more challenging
Increased risk of DVT due to immobilization

Strategies for Improvement
Will be discussed further in next talk Institute of Medicine (IOM) provides
weight gain guidelines by age. Guidelines are not stratified by
obesity classes. May be that less weight gain is
better, particularly for women with BMI above 40.

Summary
Increased rates of obesity in pregnancy have led to increasing complications for mother and baby
There are long-term consequences of obesity on future health outcomes
Obesity in pregnancy contributes to increased health care costs

Optimizing maternal pre-pregnancy weight and controlling gestational weight gain can have far-reaching consequences on future health of the population and on health care costs.