Embed Size (px)
Citation preview

[CANCER RESEARCH (SUPPL.) 42, 3281S-3285S, August 1982]0008-5472/82/0042-OOOOS02.00
Obesity, Androgens, Estrogens, and Cancer Risk1
M. A. Kirschner,2 G. Schneider, N. H. Ertel, and E. Worten
Newark Beth Israel Medical Center, New Jersey Medical School, Newark, New Jersey 07112, and V. A. Hospital, East Orange. New Jersey 07019
Abstract
Obesity is associated with increased incidence of cancersarising from tissues responsive to estrogenic stimulation, including endometrium, breast, and prostate. We thus wished toexplore estrogen production and its origin in obesity in anattempt to provide a possible hormonal link to explain increasedcancer risk.
Studies of the hormonal milieu of obese men and womenrevealed several abnormalities of sex hormone production andmetabolism, (a) Androstenedione production rates are elevatedand serve as prehormones of both testosterone and estrogens,(b) Extragonadal aromatization of androgens to form estrogens(androstenedione to estrone and testosterone to estradiol) iselevated, resulting in (c) increased production rates of estrogens. The obese person is thus chronically exposed to hyper-
estrogenemia. In addition, obesity is associated with otheralterations of sex hormone metabolism such as decreasedlevels of sex hormone-binding globulin and increased meta
bolic clearance rates of several hormones.After weight loss to ideal body weight, there appears to be
normalization of androgen and estrogen production rates, aswell as circulating hormone levels; however, metabolic abnormalities such as increased aromatization of androgens to estrogens and accelerated metabolic clearance rates of androstenedione remain abnormal.
Introduction
Obesity has been associated with increased incidence ratesof carcinoma of the endometrium, prostate, and colon (3, 8,18, 34-38, 56, 57). Further, studies from DeWaard (9), Choi
(6), and others (5, 7, 41, 45, 57) suggested an associationbetween obesity and increased breast cancer incidence. Indeed, some of the worldwide differences in breast cancerincidence rates may relate to life style, diet, and/or obesity (3,5, 9). Since 3 of 4 of these obesity-related cancers arise from
tissues that normally represent target organs of hormone action, it is most attractive to speculate that obesity results inabnormal hormone production, end organ hyperstimulation,and subsequent neoplasms (26, 57).
Obesity has been associated with a variety of alterations inhormone production, metabolism, and action. This subject hasbeen reviewed extensively by Glass ef al. (15) and Kirschneref al. (26). Of those cancers known to be associated withobesity, it appears that the sex hormones, notably estrogens,play a stimulatory role in growth of the normal tissue of origin.Thus, in the current report, we shall consider the relationshipbetween obesity and sex hormone metabolism, focusing on
' Presented at the Conference "Aromatase: New Perspectives for BreastCancer," December 6 to 9, 1981, Key Biscayne, Fla. Supported by National
Cancer Institute Contract CB-84229.2 To whom requests for reprints should be addressed, at Newark Beth Israel
Medical Center, 201 Lyons Avenue, Newark, N. J. 07112.
androgen production, peripheral aromatization of androgens toestrogens, and estrogen production. The studies to date demonstrate that obesity is associated with alterations of sex hormone production and metabolism, lending support for a possible hormonal link between obesity and cancer.
Androgen Production in Obesity
Testosterone. Although there is no a priori reason to suspecthypogonadism in normal obese men, several groups found lowplasma testosterone concentrations in this population (1, 16,29, 30, 52, 53, 58). Schneider ef al. (53) reported that plasmatestosterone averaged 350 ng/dl versus a mean of 520 ng/dlin nonobese adult men. This finding was explained when metabolic clearance rates of testosterone were observed to beelevated in proportion to the degree of obesity. Testosteroneproduction rates, as well as free "unbound testosterone," were
found to be normal in obese men, confirming normal Leydigcell function. Studies from several laboratories indicated thatobesity is associated with diminished levels of SHBG3 (1, 16,
29, 53). Whether this represents decreased production oraccelerated clearance of this particular /S-globulin is uncertain
at present. Earlier studies by Vermeulen (62) demonstratedthat the metabolic clearance rate of testosterone was inverselyrelated to SHBG. The following sequence could thus be usedto explain the testosterone findings in obese men. Obesityresults in lower levels of SHBG, leading to accelerated clearance of testosterone and lower plasma testosterone concentrations for a given degree of testosterone production. In effect,androgen production and actions are normal and the pituitary-
gonadal axis appears to be intact in obese men (15, 53, 59),but metabolism a" J mechanics of testosterone distribution are
altered.In obese women, there appears to be an increased incidence
of menstrual disturbances and hirsutism, suggesting possibleabnormalities of androgen production (12,17, 42, 48). Indeed,Hosseinan et al. (21) reported elevated "free androgens" in
obese amenorrheic (nonhirsute) women. The great majority ofobese women, however, have normal menstrual function andnone of the clinical features commonly associated with excessive androgens (25, 54). In fact, when serum testosterone wasmeasured in a group of normally menstruating nonhirsuteobese women, we observed lower than expected total plasmatestosterone concentrations in proportion to the degree ofobesity (27). As described for men (above), lower plasmatestosterone was explained by decreased levels of SHBG.Thus, it seemed reasonable to assume that low SHBG in bothobese men and women resulted in accelerated clearance andlower plasma testosterone concentrations. More recent datafrom our laboratory (50), however, suggest that testosteroneproduction rates are indeed increased in obese normally men-
3 The abbreviation used is: SHBG, sex hormone-binding globulin.
AUGUST 1982 3281S
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

M. A. Kirschner et al.
struating nonhirsute women despite the relatively low totalplasma testosterone and even normal "free testosterone" mea
surements. The elevated testosterone production rates couldnot be normalized by correction for excessive body surface.
Peripheral Aromatization of Testosterone. Although aro-matization of testosterone to estrogens in the peripheral (extra-
gonadal) circulation represents a minor pathway in its overallmetabolism, occurring to the extent of 0.2 to 0.4% (2), themagnitude of testosterone production in men makes this pathway of metabolism the major source of circulating estradiol innormal men. Schneider et al. (53) demonstrated that obesitywas associated with a 2- to 3-fold increase in aromatization of
testosterone to estradiol. This pathway of peripheral metabolism of testosterone accounted in large part for the elevatedestradiol production rates observed in obese men. These dataare confirmed by Kley et al. (30) and Zumoff et al. (65) whoreported increased plasma estrogen levels in obese men.
In women, testosterone production is small (250 jug/day).The peripheral conversion of testosterone to estradiol is thesame magnitude as described above, making this pathway aninsignificant source of the total circulating estradiol. Althoughno formal studies of peripheral aromatization of testosterone toestradiol have been performed in young obese women, it seemsreasonable to speculate that there is increased peripheralaromatization of testosterone to estradiol, and if testosteroneproduction is elevated in this population, extragonadal aromatization to estradiol may become a significant component of thetotal estradiol produced.
Androstanediol. This C19steroid represents a major metab-
GIRLS MENSTRUATING WOMEN POSTMENOPAUSE
MEN
YEARS DAYS YEARS
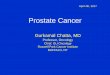
Chart 1. Estrogen production at various ages. Schematic representation ofthe role of extragonadal aromatization in the daily production rates of estrogensin various age groups. In premenarchal girls, all the estrogens produced arise viaextragonadal aromatization of androstenedione. In women of reproductive age,ovarian estrogen secretion is superimposed on extragonadal sources whichaccount for approximately 40% of basal estrogen output. In the postmenopausalstate, all estrogens rise via extragonadal metabolism of androgens. In men,approximately 80% of estrogens rise from extragonadal metabolism of androgens.
olite of the potent androgen, dihydrotestosterone. Althoughplasma 3a-diol levels were normal in obese women, Samojlik
et al. (50) found that production rates and urinary excretion ofthis androgen are elevated in obese normally menstruating(nonhirsute) women. These data suggest that adipose tissuemetabolism may become involved in the accelerated production of the potent androgen, dihydrotestosterone, as well as itsmetabolite, 3a-diol.
Androstenedione. Although androstenedione is not a trueandrogen (19), it serves as a prehormone of testosterone aswell as estrone via extragonadal metabolism. In men, thisprehormone serves as a minor source of testosterone, but 1 to2% is metabolized to estrone, accounting for 80% of the dailyproduction rate of estrone (Chart 1). In women, peripheralmetabolism of androstenedione to testosterone serves as amajor source of testosterone production (approximately 50%)as well as accounting for approximately 50% of the daily basalestrone production rate observed in early phases of the menstrual cycle (Chart 1).
In our study of obese men, we found androstenedione production rates to be 3- to 4-fold elevated when obesity levels
reached 200 to 250% above ideal body weight (53). Thesefindings are different from those of Kley ef al. (30), whoreported elevated metabolic clearance rates but normal production rates of androstenedione in obese men.
In a group of young obese women studied to date, weobserved that androstenedione production rates averaged 3.52mg/day versus 2.27 mg/day in normal nonobese controls. Asnoted in Table 1, plasma androstenedione levels were notsignificantly different in obese women versus normal controls;however, the metabolic clearance rates of androstenedionewere significantly elevated in the obese women. These valuesare of interest, since androstenedione appears not to be significantly bound to SHBG, and thus its accelerated clearancerate must be explained by mechanisms unrelated to plasma-
binding globulins. No formal blood production studies of androstenedione have been performed in obese postmenopausalwomen or premenarchal girls.
Aromatization of Androstenedione to Estrone. As discussed in the previous section, extragonadal metabolism ofandrostenedione to estrone represents a minor pathway ofandrostenedione metabolism, occurring to the extent of 1 to2% in the normal population. Since androstenedione production normally is in the mg range and estrogens are produced inthe fig range, this seemingly minor pathway of androstenedionemetabolism assumes considerable significance. As demonstrated in Chart 1, peripheral aromatization of androstenedioneto estrone accounts for virtually all the estrogens produced inpremenarchal children, postmenopausal women, and men (25,34, 35, 55, 61) and is a significant component of estrogensproduced in the normal menstrual cycle.
Table 1Androgen-estrogen parameters in obese young women
Obese womenNormal womenp valuePlasma
androstenedione
(ng/dl)111
121NSaMetabolic
clearance rate of androstenedione
(liter/day)3140
2140<0.05Urinary
estrone productionrateAndrostenedione
production rate<mg/day)3.52
2.27<0.05Conversion
ofandrostenedione
to estrone(%)2.52
1.50<0.05fig/day154
104<0.05%
from androstene
dione89
34<0.05%
from allother sources65
70NS
8 NS, not significant.
3282s CANCER RESEARCH VOL. 42
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Obesity, Androgens, Estrogens, and Cancer Risk
In obese men, Schneider et al. (53) and Kley ef al. (28)observed increased conversion rates of androstenedione toestrone, ranging from 1.6 to 5.4%. These findings supportedearlier observations of MacDonald ef al. (34), MacDonald andSiiteri (36), Schneider ef al. (53), and Longcope (32), whoobserved increased peripheral aromatization of androstenedione in postmenopausal women. In young obese women, Edmanef al. (10) demonstrated increased peripheral metabolism ofandrostenedione to estrone, and in our recent studies (Table1), the mean aromatization of androstenedione to estrone inobese women was 2.52% versus 1.52% in nonobese controls.The magnitude of androstenedione production and extragon-
adal conversion to estrone in young women of reproductiveage is demonstrated in Chart 2. Thus, data from the varyingage and sex groups studied clearly demonstrate that peripheralaromatization of androstenedione is elevated in obesity, leadingto increased estrone formation.
Estrone Production in Obesity
In men, Schneider ef al. (53) demonstrated that obesity wasassociated with increased urinary production rates of bothestrone and estradiol proportional to excessive body weight.The source of increased estrogens in obese men appeared tobe related to increased aromatization of their respective andro-
genic prehormones (testosterone to estradiol and androstenedione to estradiol). Data from other laboratories confirm thesefindings (30, 59).
As discussed above, earlier studies established that postmenopausal women with obesity exhibited increased urinaryestrone production rates, arising from increased extragonadalaromatization of androstenedione. Current data from our laboratory obtained in 83 young women ages 20 to 40 with varyingdegrees of obesity have corroborated the earlier study ofEdman ef al. (10) demonstrating increased urinary estroneproduction rates in this age group. In our studies, urinaryestrone production rates, performed on Days 5 to 8 of themenstrual cycle, averaged 154 fig/day in the obese womenversus 104 ¿tg/dayin nonobese control subjects of similar age.As noted in Table 1, the increment of estrone production is
4.0
I
200
3.0
3oo£2.0Ulzoo
£I0
Chart 2. Extragonadal origin of estrone in obese young women. Comparisonof androstenedione production, extragonadal metabolism of androstenedione toestrone, and estrone production rates in normal versus obese women of reproductive age. Obese women overproduce androstenedione, exhibit increasedconversion of androstenedione to estrone, and increased estrone productionrates. Ovarian estrone secretion appears to be the same in obese and normalwomen.
YEARS DAYS YEARS
Chart 3. Estrogen production in obesity. Schematic comparison of estrogenproduction and its extragonadal origin in obesity compared with normal womenand men at varying age groups. The obese person is subjected to chronichyperestrogenism.
explained entirely from increased peripheral aromatization ofcirculating androstenedione.
Although estrogen production rates have not been formallyassessed in children or adolescents, it has been commonlyobserved that obesity in children is associated with early onsetof pubertal changes (13, 14). It seems entirely reasonable toassume that childhood obesity is similarly associated withaccelerated conversion of prehormones to estrogens. It isintriguing to speculate on whether increased peripheral aromatization of circulating prehormones to form excessive estrogens may be a triggering mechanism leading to acceleratedpubertal changes.
From studies of peripheral aromatization and estrogen formation in men, postmenopausal women, young women of reproductive age, and extrapolating data for children, it appearsthat obesity is associated with lifelong increased estrogenproduction, as portrayed in Chart 3. Superimposed upon thisincreased estrogen level arising from extragonadal sources isthe normal estrogen output secreted by the functioning ovaryand minimal estrogen secretion from the testes. Followingmenopause, the extragonadal pathway becomes the solesource of estrogens.
Estrogens and Cancer Risk
From the data surveyed to date, it seems entirely reasonableto postulate that obesity is associated with hyperestrogenism,possibly leading to excessive chronic stimulation of estrogen-responsive target organs. Stimulation of target organs couldlead to hyperplasia and subsequently neoplasia. Further, estrogens may serve as promoters of neoplastic transformationsoccurring within these stimulated target organs.
Although a direct link between endogenous and exogenoushyperestrogenism and carcinoma of the endometrium appearsto be reasonably well established (4, 7, 18, 34-38, 40, 47, 56,57, 64), the same relationship to breast cancer cannot beconfidently stated at present (6, 7, 39, 41). Available datalinking exogenous estrogen usage and breast cancer aresuggestive but uncertain. Oral contraceptive use in youngwomen has not been associated with increased risk of breastcancer (11, 22, 45, 63); but use of these agents by womenapproaching menopause seems to increase breast cancer risk(11, 22). The relationship of menopausal estrogen usage andbreast cancer risk is unclear. Although there is some suggestion that exogenous estrogens in this age group may increasebreast cancer risk, the risk ratios are small and more data areneeded (20, 23, 41, 49).
AUGUST 1982 3283s
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

M. A. Kirschner et al.
DeWaard (9) suggested that obesity is related to an increased incidence of postmenopausal breast cancer. Paffen-barger et al. (45) suggested that weight gain during reproductive life may also influence postmenopausal breast cancer risk.Since the postmenopausal period is associated with fallingendogenous estrogen production, obesity at this time of lifewould seem to have little effect upon the initiation of breastcancer, unless perhaps estrogens were artificially elevated byexogenous sources, as described above. It was thus of considerable importance to establish that obesity occurring in youngwomen (of reproductive age) results in hyperestrogenism. Iftumor induction is associated with a prolonged latent or pre-detection period, then it is the obesity occurring in youngerwomen and its associated hyperestrogenism which may account for the breast cancer later in life.
The relationship of obesity, extraglandular estrogen production, and carcinoma of the prostate is uncertain. Estrogenreceptors have been found in both normal and neoplasticprostatic tissue (43). The potential modulating role of estrogensand estrogen receptors on the growth of normal and neoplasticprostatic tissue represents an area of great potential.
Effect of Weight Loss on Hormone Production andMetabolism
The effect of weight loss on production and metabolism ofsex hormones has been examined by a number of groups.Perel and Killinger (46) and Takaki et al. (60) reported nochange in urinary estrone production or in androstenedioneconversion to estrone in subjects studied before and aftersignificant weight loss. These findings seemed reasonable,since adipocytes and/or supporting stroma which representthe likely sites of most of these hormonal alterations (33, 44,46, 51) are not appreciably altered by weight reduction.Schneider ef al. (52), however, reported prompt return ofdepressed serum testosterone levels to normal in a group ofobese men undergoing supplemented starvation and suggested that SHBG abnormalities could be reversed after 1 to 2weeks of dieting. Similarly, Stanik et al. (58) reported restoration of plasma testosterone levels, as well as decreased plasmaestrogen levels, in obese men after 10 weeks of weight loss. Inour ongoing studies, sex hormone production and metabolismwere studied in young women both before and after majorweight loss with stabilization of weight and return of normalmenstrual function. Studies to date suggest that hormone production rates tend to be restored toward normal levels; however, several aspects of peripheral metabolism of androgens-estrogens such as metabolic clearance rates of androstenedione and aromatization of androstenedione to estrone remainelevated. These data suggest that adrenal and/or gonadalsecretion of the sex hormones and their prehormones can bealtered by restoration of body weight to more ideal levels.Metabolic alterations may not be reversed by shrinkage ofhyperplastic fat tissue. These findings present some hope thatcorrection of the obese state may have some beneficial effecton the abnormal hormonal milieu despite metabolic alterationsthat may be fixed.
References
1. Amatruda, J. M.. Harman, S. M., Pourmotabbed, G., and Lockwood, D. H.Depressed plasma testosterone and fractional binding of testosterone in
obese males. J. Clin. Endocrinol. Metab., 47: 268-271, 1978.2. Baird, D. T., Morton, R., Longcope, C.. and Tait, J. F. Steroid dynamics
under steady state conditions. Ree. Prog. Horm. Res., 25. 611 -656, 1969.3. Berg, J. W. Can nutrition explain the pattern of international epidemiology of
hormone-dependent cancers? Cancer Res., 35: 3345-3350, 1975.4. Calaong, A., Sail, S., Gordon, G. G., and Southren. A. L. Androstenedione
metabolism in patients with endometrial cancer. Am. J. Obstet. Gynecol.,729: 553-556, 1977.
5. Carroll, K. K., Gammel. E. B., and Plunkett, E. R. Dietary fat and mammarycancer. Can. Med. Assoc. J., 23: 590-594, 1968.
6. Choi, N. W., Howe, G. R., and Miller, A. B. An epidemiological study ofbreast cancer. Am. J. Epidemici., 107: 510-521, 1978.
7. Cole, P., and Cramer, D. Diet and cancer of endocrine target organs. Cancer(Phila.), 40: 434-437, 1977.
8. Correa, P. Epidemiological correlations between diet and cancer frequency.Cancer Res., 41: 3685-3690, 1981.
9. DeWaard, F. W. Breast cancer incidence and nutritional status with particularreference to body weight and height. Cancer Res., 35. 3351-3356, 1975.
10. Edman, C. D., Aiman. E. J., Porter, J. C., and MacDonald, P. C. Identificationof the estrogen product of extraglandular aromatization of plasma androstenedione. Am. J. Obstet. Gynecol., 730: 439-447, 1978.
11. Fasal, E., and Paffenbarger, R. S., Jr. Oral contraceptives as related tocancer and benign lesion of the breast. J. Nati. Cancer Inst., 55: 767-773,1975.
12. Fisher. E. R., Gregorio, R., Stephan, T., era/. Ovarian changes in womenwith morbid obesity. Obstet. Gynecol., 44: 839-844, 1974.
13. Frisch, R. E., and McArthur, J. W. Menstrual cycles: fatness as a determinantof minimum weight necessary for maintenance or onset. Science (Wash.D. C.). 785: 949-951, 1974.
14. Frisch, R. E., and Revelle, R. Height and weight at menarche and a hypothesis of critical body weights and adolescent events. Science (Wash. D. C.),769:397-399, 1970.
15. Glass, A. R., Burman. K. D., Dahms. W. T., and Boehm, T. M. Endocrinefunction in human obesity. Metabolism Clin. Exp., 30: 89-104, 1981.
16. Glass, A. R., Swerdloff, R. S., Bray. G. A., ef al. Low serum testosteroneand sex-hormone binding globulin in massively obese men. J. Clin. Endocrinol. Metab., 45: 1211-1219, 1977.
17. Hartz, A. J., Barboriak, P. N., Wong, A., ef al. The association of obesitywith infertility and related menstrual abnormalities in women. Int. J. Obes.,3:57-73, 1979.
18. Hausknecht, R. U., and Gusberg, S. B. Estrogen metabolism in patients athigh risk for endometrial carcinoma. II. The role of androstenedione as anestrogen precursor in post menopausal women with endometrial carcinoma.Am. J. Obstet. Gynecol., 7776. 981 -984, 1973.
19. Hilgar, A. G., and Hummel, D. J. In: Endocrine Bioassay Data, Androgenicand Myogenic, p. 39. Bethesda, Md.: USPHS, 1964.
20. Hoover, R., Gray, L. A., Cole. P., et al. Menopausal estrogens and breastcancer. N. Engl. J. Med.. 295: 401-405, 1976.
21. Hosseinan, A. H., Kim, M. H., and Rosenfeld, R. L. Obesity and oligomenor-rhea are associated with hyperandrogenism independent of hirsutism. J.Clin. Endocrinol. Metab., 42: 765-769, 1976.
22. Jick, H., Walker, A. M., Watkins, R. N., ef al. Oral contraceptives and breastcancer. Am. J. Epidemiol., 772: 577-585, 1980.
23. Jick, H., Walker, A. M., Watkins, R. N., et al. Replacement estrogens andbreast cancer. Am. J. Epidemiol., 772: 586-594, 1980.
24. Judd. H. L., Judd, G. E.. Lucas, W. E., et al. Endocrine function of thepostmenopause ovary: concentrations of androgens and estrogens in ovarian and peripheral bein blood. J. Clin. Endocrinol. Metab., 39: 1020-1024,1974.
25. Kirschner, M. A. Virilism in the female. In: J. J. Gold and J. B. Josimovich(eds.). Gynecologic Endocrinology, Ed. 3. pp. 594-609. Hagerstown, Md.:Harper & Row, Publishers, 1980.
_3. Kirschner, M. A., Ertel, N., and Schneider, G. Obesity, hormones andcancer. Cancer Res., 41: 3711 -3717, 1981.
27. Kirschner, M. A., Mazzeotti, Winter, J., and Keizer, M. Obesity distortsandrogen measurements in hirsute women. Submitted for publication.
28. Kley, H. K., Deselaers, T., Peerenboom, H., et al. Enhanced conversion ofandrostenedione to estrogens in obese males. J. Clin. Endocrinol. Metab..57: 1128-1132, 1980.
29. Kley, H. K., Edelmann, P., and Kruskemper. H. L. Relationship of plasmasex hormones to different parameters of obesity in male subjects. Metabolism Clin. Exp., 29: 1041-1045. 1980.
30. Kley, H. K., Solbach, H. G., McKinnan, J. C., era/. Testosterone decreaseand estrogen increase in male patients with obesity. Acta Endocrinol., 97:553-563, 1979.
31. Lipsett, M. B. Hormones, nutrition and cancer. Cancer Res., 35:3359-3361,1975.
32. Longcope, C. Steroid production in pre- and post-menopausal women. In:R. B. Greenblatt, V. B. Mahesh, and P. C. MacDonald (eds). The MenopausalSyndrome, p. 6, New York: Medcom, Inc., 1974.
33. Longcope, C., Pratt, J. H., Schneider, S. H., and Fineberg, S. E. Aromatization of androgens by muscle and adipose tissue in vivo. J. Clin. Endocrinol.Metab., 46: 146-152, 1978.
3284s CANCER RESEARCH VOL. 42
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Obesity, Androgens, Estrogens, and Cancer Risk
34. MacDonald, P. C., Edman, C. D., Hensell, D. L, Porter, J. C., and Siiteri, P.C. Effect of obesity on conversion of plasma androstenedione to estrone inpostmenopausal women with and without endometrial cancer. Am. J. Obstet.Gynecol., 730: 448-455, 1978.
35. MacDonald, P. C., Grodin, J. M., Edman, C. D., Vellios, F., and Siiteri, P. K.Origin of estrogen in a post-menopausal woman with a non endocrine tumorof the ovary and endometrial hyperplasia. Obstet. Gynecol., 47: 644-650,
1976.36. MacDonald, P. C., and Siiteri, P. K. The relationship between extraglandular
production of estrone and the occurrence of endometrial neoplasia. Gynecol.Oncol., 2. 259, 1974.
37. Mack.T. M., Pike, M. C., Henderson, B. E.,efa/. Estrogens and endometrialcancer in a retirement community. N. Engl. J. Med., 294.- 1262-1267,
1976.38. MacMahon, B. Risk factors for endometrial cancer. Gynecol. Oncol., 2:
122-129, 1974.39. MacMahon, B.. Cole, P., and Brown, J. B. Etiology of human breast cancer:
a review. J. Nati. Cancer Inst., 50. 21-42, 1973.40. McDonald, T. W.. Annegers. J. F., O'Fallow, W. M., et al. Exogenous
estrogens and endometrial carcinoma: case control and incidence study.Am. J. Obstet. Gynecol., »27.572-580, 1977.
41. Miller, A. B. An overview of hormone-associated cancer. Cancer Res., 38.3985-3990, 1978.
42. Mitchell, A. W., and Rogers. J. The influence of weight reduction on amen-orrhea in obese women. N. Engl. J. Med., 249. 835-837, 1953.
43. Murphy, J. B., Emmott, R. C., Hicks, L. L., et al. Estrogen receptors in thehuman prostate, seminal vesicle, epididymis, testes, genital skin: a markerfor estrogen-responsive tissues. J. Clin. Endocrinol. Metab., 50. 938-948,
1980.44. Nimrod, A., and Ryan, K. S. Aromatization of androgens by human abdominal
and fat breast tissue. J. Clin. Endocrinol. Metab., 40: 367-372, 1975.45. Paffenbarger, R. S.. Jr., Kampert, J. B., and Chang, H. G. Characteristics
that predict rise of breast cancer before and after the menopause. Am. J.Epidemici., 112: 250-268, 1980.
46. Perel, E., and Killinger, D. W. The interconversion and aromatization ofandrogens by human adipose tissue. J. Steroid Biochem., 10: 623-627,
1979.47. Rizkallah. T. H., Tovell, H. M. M., and Kelly, W. G. Production of estrone
and fractional conversion of circulation, androstenedione to estrone inwomen with endometrial carcinoma. J. Clin. Endocrinol. Metab., 40:1045-1056. 1975.
48. Rogers, J., and Mitchell, G. W., Jr. The relation of obesity to menstrualdisturbances. N. Engl. J. Med., 247: 53-55, 1952.
49. Ross, R. K., Paganini-Hill, A., Gerkins, V. R.. et al. A case-control study ofmenopausal estrogen therapy and breast cancer. J. Am. Med. Assoc.. 243.1635-1639, 1980.
50. Samojlik, E., Drejka, M., Schneider, G., and Kirschner, M. A. Obese women
excrete excessive amounts of 3 alpha-androstanediol. In: Proceedings of63rd Endocrine Society, Cincinnati, Ohio, 1981, Abstract 31.
51. Schindler, A. E., Ebert, A., and Friedrich, E. Conversion of androstenedioneto estrone by human fat tissue. J. Clin. Endocrinol. Metab., 36: 627-630,
1972.52. Schneider, G.. Gherman, M., Winter, J., and Kirschner, M. A. Acute effects
of weight loss on sex hormone binding globulin levels in obese men. In:Program of 6th International Congress of Endocrinology, Melbourne, Australia, 1980.
53. Schneider, G., Kirschrier, M. A., Berkowitz, R., and Ertel, N. H. Increasedestrogen production in obese men. J. Clin. Endocrinol. Metab., 48:633-638, 1979.
54. Sherman, B. M., Wallace, R. B., Treloar, A. E., Chang, Y., and Bean, J. A.Body mass and menstrual cycle patterns: relationship to breast cancer risk.Clin. Res., 2/V 681A, 1979.
55. Siiteri, P. K., and MacDonald, P. C. The role of extraglandular estrogens Inhuman endocrinology. In: S. R. Geiger, E. B. Astwood, and R. O. Greep(eds.), Handbook of Physiology. Sect. 7, pp. 615-629. New York: AmericanPhysiological Society, 1973.
56. Siiteri, P. K., Prentice, R., Thompson. D. J., et al. Association of exogenousestrogens and endometrial carcinoma. N. Engl. J. Med., 293. 1164-1167,
1975.57. Siiteri, P. K., Williams, J. E., and Takaki, N. K. Steroid abnormalities in
endometrial and breast carcinoma: a unifying hypothesis. J. Steroid Biochem., 7. 897-903, 1976.
58. Stanik, S., Dornfeld, L. P., Maxwell, M. H., et al. The effect of weight loss onreproductive hormones in obese men. J. Clin. Endocrinol. Metab.. 53.828-832, 1981.
59. Suryanarayana, B. V., Kent, J. R., Meister, L., et al. Pituitary gonadal axisduring prolonged total starvation in obese men. Am. J. Clin. Nutr., 22:767-770, 1969.
60. Takaki, N. K., Siiteri, P. K., Williams, J., et al. The effect of weight loss onperipheral estrogen synthesis in obese women. Int. J. Obes., 2. 386, 1978.
61. Vermeulen, A. Plasma levels and origin of sexual hormones in postmenopausal women. In: R. Scholler (ed.). Endocrinology of the Ovary, pp.317-326. Paris: Sepe. 1978.
62. Vermeulen, A., Verdone, C. M.. Van der Straeton, M., and Orie, N. Capacityof testosterone binding globulins in human plasma and influence of specificbinding of testosterone on its metabolic clearance rate. J. Clin. Endocrinol.Metab., 29. 1470-1479, 1969.
63. Vessey, M. P.. Doll, R., James. K., ef al. An epidemiologie study of oralcontraceptives and breast cancer. Br. Med. J., ÃŽ.1757-1760, 1979.
64. Ziel, H. K., and Finkle, W. D. Increased risk of endometrial carcinoma amongusers of conjugated estrogens. N. Engl. J. Med., 293. 1167-1170. 1975.
65. Zumoff. B., Strain, F. W., Kream, J., ef al. Obese young men have elevatedplasma estrogen levels, but obese premenopausal women do not. Metabolism Clin. Exp., 30: 1011-1014, 1981.
AUGUST 1982 3285s
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1982;42:3281s-3285s. Cancer Res M. A. Kirschner, G. Schneider, N. H. Ertel, et al. Obesity, Androgens, Estrogens, and Cancer Risk
Updated version
http://cancerres.aacrjournals.org/content/42/8_Supplement/3281s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/42/8_Supplement/3281sTo request permission to re-use all or part of this article, use this link
on July 9, 2020. © 1982 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from









![Review Article - synapse.koreamed.org€¦ · mately erectile dysfunction (ED) [1,4,5]. Androgens play an important ro le in erectile physiology. It is believed that androgens are](https://img.pdfslide.net/doc/110x75/600b0ca745705852d3696029/review-article-mately-erectile-dysfunction-ed-145-androgens-play-an-important.jpg)