-
8/13/2019 Obesity in Children With Headaches - Anak
1/9
-
8/13/2019 Obesity in Children With Headaches - Anak
2/9
-
8/13/2019 Obesity in Children With Headaches - Anak
3/9
adjusted for age and gender.
For all comparisons and analyses, all Pvalues refer to 2-tailed
tests. Pvalue of .05).
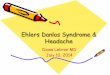
When adjusted for age and gender, the diagnosis of migraine but
not of TTH was significantly associated with being
at risk for overweight (OR = 2.37, 95% CI 1.21 4.67, P= .01) or
overweight (OR = 2.29, 95% CI 0.95 5.56, P= .04)
A significant independent risk for overweight was present in
females with migraine (OR = 4.93, 1.46 8.61, P= .006)
compared with males (OR = 0.77, 0.41 4.28, P= .56) ().
Table 2. Prevalence Odds Ratios for Body Mass Index (BMI) in
Relation to Headache Type
-
8/13/2019 Obesity in Children With Headaches - Anak
4/9
At Risk for Overweight Overweight
Total samplea OR (CI) P OR (CI) P
Migraine 2.37 (1.214.67) .01 2.29 (0.955.56) .04
TTH 0.63 (0.321.22) .17 0.49 (0.191.22) .12
Girls
Migraine 3.01 (1.247.3) .012 4.93 (1.468.61) .006
TTH 0.50 (0.211.22) .13 0.25 (0.070.95) .06
Boys
Migraine 1.02 (0.373.32) .61 0.77 (0.414.28) .56
TTH 1.67 (0.515.41) .6 2.02 (0.376.04) .3
aAdjusted for age and gender.
BMI = body mass index; CI = confidence interval; OR = odds
ratio; TTH = tension-type headache. Bold characters
highlight statistical significance.
BMI and Headache Frequency and Disability
Patients were subdivided into 3 groups according to attack
frequency: (1) 4 or less attacks per month; (2) 5 15
attacks per month; and (3) more than 15 attacks per month. A
high frequency of headaches was associated with
obesity. Frequent headaches (more than 15 attacks per month)
were significantly more common in the obese
children compared with the normal-weight children, 23% vs 12%,
P< .01. Headache duration was not significantly
different in the 2 groups, lasting less than 2 hours in 35% vs
38% of patients, 2 4 hours in 55% vs 49%, and longer
than 4 hours in 10% vs 13% (P= not significant). When asked,
"How many days per month are you using
medications for acute headache?" 43% of the obese children vs
17% of the normal-weight children reported using
analgesic medications more than 15 days per month ().
Table 3. Headache Characteristics and Impact in Normal Weight
and Obese Children
Body Mass Index (BMI) 85th Percentile 5th-85th Percentile P
Attack frequency (%)
4/month 37 63
15/month 23 12
Attack duration (%)
4 hours 10 13
Use of medications for acute treatment (%)
4/month 26 46
15/month 43 17
NS, not significant (P> .05). Bold characters highlight
statistical significance.
A percentage of children with some level of disability (PedMIDAS
grades II-IV) was assessed in relation to BMI and
-
8/13/2019 Obesity in Children With Headaches - Anak
5/9
headache type, and adjusted for age and gender (). For the total
study population, 14.7% of those with normal weight
had some level of disability compared with 20.3% of the at risk
for overweight group (OR = 1.7; CI 1.4 2.2, P< .001)
and 33.3% in the overweight group (OR = 3.1; CI 1.9 5.8, P<
.0001). Similar results were measured for both
migraine and TTH. For children with migraine, 12.5% of those
with normal weight had some level of disability
compared with 17.8% of the at risk for overweight group (OR =
1.9; CI 1.5 2.4, P< .0001) and 30.7 in the overweight
group (OR = 3.7; CI 2.2 6.1, P< .0001). For children with
TTH, 15.2% of those with normal weight had some level of
disability compared with 22.2% of the at risk for overweight
group (OR = 1.6; CI 1.3 2.0, P< .0001) and 30% in the
overweight group (OR = 2.9; CI 1.7 4.9, P< .0001).
Table 4. Children With Some Level of Disability, as Measured by
the PedMIDAS Scale,ain Relation to Headache Type and
BMI Category
Total Migraine TTH
% With Disability ORb(CI) % With Disability ORb(CI) % With
Disability ORb(CI)
Normal weight 14.7 1 (ref) 12.5 1 (ref) 15.2 1 (ref)
At risk for overweight 20.3 1.7 (1.42.2) 17.8 1.9 (1.52.4) 22.2
1.6 (1.32)
Overweight 33.3 3.1 (1.95.8) 30.7 3.7 (2.26.1) 30 2.9
(1.74.7)
P for trend
-
8/13/2019 Obesity in Children With Headaches - Anak
6/9
migraine headache.[28, 29]In a recent study of 273 children and
adolescents, 50% of obese patients suffered from
migraine compared with only 25% in the normal-weight
group.[18]
Several possible mechanisms that may account for the association
between obesity and frequent migraine have been
suggested.[30]Obesity is recognized as a pro-inflammatory state.
Markers of inflammation, including leukocyte
count, tumor necrosis factor-, and interleukin-6, increase in
obesity and may be associated with neurovascular
inflammation in patients with migraine.[31]Plasma calcitonin
gene-related peptide levels, an important post-synaptic
mediator of trigeminovascular inflammation in migraine, are
elevated in obese individuals, particularly in women. [32]
Finally, recent data suggest that dismodulation in hypothalamic
neuropeptides orexin in obese persons may beassociated with
increased susceptibility to neurogenic inflammation causing
migraine attacks.[30, 33]
Information regarding the association between obesity and
headache-related disability in children is limited. In his
study on 913 children with headache, Hershey et al found a
significantly positive correlation between BMI percentile
and headache frequency and headache-related disability scores.
At follow up, a reduction in BMI was associated with
a reduction in headache frequency, but not with headache-related
disability. [16]In another recent study on 124
children with migraine, obesity was associated with frequency,
but not severity of migraine attacks. [28]
Headache frequency, duration, and disability were considered in
trying to assess the headache-related burden in our
study. Obese children in our study had a significantly higher
rate of very frequent headaches (more than 15 attacks
per month) as well as higher disability grades compared with
normal-weight children. The association between BMIpercentile and
higher disability grades was similar for both migraine and TTH.
There was no significant difference in
duration of attacks between obese and normal-weight children.
Additionally, we found a significantly higher rate of
acute drug treatment in our patients with obesity compared with
normal-weight children, similar for both migraineurs
and children with TTH. This may also reflect the more frequent
and disabling attacks among the obese children.
These results are compatible with prior results in adult
studies.[15, 23]In their population study of adults with CDH,
Bigal and Lipton found that obese patients not only had a higher
rate of headache, but also suffered from increased
severity of headaches and missed more school and work days than
non-obese patients. [13]It was hypothesized that
increased attack frequency may cause neuronal sensitization that
reduces response to therapy and that obesity
contributed toward the development of this sensitivity. In
adults with episodic headaches, obesity was associated
with higher disability grades only in patients with migraine,
but not in those with other types of episodic headaches.[41]
Some caution is required in assessing the type of relationship
between obesity and headache frequency and
disability in children. Current data are not sufficient to
establish a significant causal relation, and both physiological
and environmental factors are probably playing a role. Obesity
was found to be associated with increased prevalence
and severity of other chronic pain disorders besides headache,
such as musculoskeletal and abdominal pain. [35, 36]
Both conditions are associated with psychiatric comorbidities,
such as depression and anxiety, [10, 37]that can furthe
increase headache frequency and disability.[38]Lifestyle may
have an impact on both weight and headache. In a
population-based study by Molarius et al,[39]physical inactivity
was strongly associated with headache disorders
independent of economic and psychosocial factors. On the other
hand, recurrent headaches were found to be
associated with low physical activity[40]that can further
contribute to overweight and further increase headache
frequency.[17]Sleep problems such as short sleep duration and
poor sleep quality may also play a role in bothobesity and
recurrent headaches.[41, 42]
No matter what the leading explanations for the correlation
between obesity and headaches are, given our evidence
as well as others, weight is a modifiable risk factor for
recurrent headaches in children. Weight and BMI should be
measured and calculated in all children presenting with
headache, and weight control should be part of the treatment
of chronic headache in children.
Some limitations should be considered in the present study.
First, our sample cannot be considered as
representative of pediatric headache patients because of
selection bias. Subjects who are referred to a hospital clinic
might have more health-related problems compared with children
with headaches treated within the community.
-
8/13/2019 Obesity in Children With Headaches - Anak
7/9
Second, stratification of data according to headache diagnosis
and gender resulted in relatively small groups that
could underpower the analyses. Finally, as mentioned before, we
cannot infer causality between obesity and
headache frequency and disability.
In summary, our data show a high rate of obesity in children
with primary headaches compared with the general
population. The strongest association with obesity was found for
females and for children with migraine headaches. In
all the children with primary headaches, a high BMI percentile
was associated with increased headache frequency
and disability. Although we were unable to adequately address
the question of causal relationship, we believe in and
emphasize the importance of obesity prevention and treatment in
children with headaches.
References
1. Brna PM, Dooley JM. Headaches in the pediatric population.
Semin Pediatr Neurol. 2006;13:222 230.
2. Wang Y, Lim H. The global childhood obesity epidemic and the
association between socio-economic status
and childhood obesity. Int Rev Psychiatry. 2012;24:176 188.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of
obesity and trends in body mass index among US
children and adolescents, 1999 2010. JAMA. 2012;307:483 490.
4. World Health Organization.Obesity and overweight. 2009.
Available at: http://www.who.int/media-
centre/factsheets/fs311/en/(accessed September 21, 2012).
5. Speiser PW, Rudolf MC, Anhalt H, et al; Obesity Consensus
Working Group. Childhood obesity. J Clin
Endocrinol Metab. 2005;90:1871 1887.
6. Organization for Economic Co-operation and Development.
Organization for Economic Cooperation and
Development family database. 2010. Available at:
http://www.oecd.org/els/social/family/database (accessed
October 26, 2012).
7. Bandell-Hoekstra I, Abu-Saad HH, Passchier J, Knipschild P.
Recurrent headache, coping, and quality of life
in children: A review. Headache. 2000;40:357370.
8. Strine TW, Okoro CA, McGuire LC, Balluz LS. The associations
among childhood headaches, emotional and
behavioral difficulties, and health care use. Pediatrics.
2006;117:17281735.
9. Barlow SE, Dietz WH. Management of child and adolescent
obesity: Summary and recommendations based
on reports from pediatricians, pediatric nurse practitioners,
and registered dietitians. Pediatrics. 2002;110:236
238.
10. Kalarchian MA, Marcus MD. Psychiatric comorbidity of
childhood obesity. Int Rev Psychiatry. 2012; 24:241
246.
11. Balott in U, Nicoli F, Piti llo G, Ginevra OF, Borgatti R,
Lanzi G. Migraine and tension headache in children
under six years of age. Eur J Pain. 2004;8:307- 314.
12. Scher AI, Stewart WF, Ricci JA, Lipton RB. Factors
associated with the onset and remission of chronic daily
headaches in a population-based study. Pain. 2003;106:8189.
13. Bigal ME, Lipton RB. Obesity is a risk factor for
transformed migraine but not for chronic tensiontype
headache. Neurology. 2006;67:252257.
14. Vo M, Ainalem A, Qiu C, Peterlin BL, Aurora SK, Williams MA.
Body mass index and adult weight gain
-
8/13/2019 Obesity in Children With Headaches - Anak
8/9
among reproductive age woman with migraine. Headache.
2011;51:559569.
15. Bigal MF, Liberman JN, Lipton RB. Obesity and migraine: A
population based study. Neurology. 2006;66:545
550.
16. Hershey AD, Powers SW, Nelson TD, et al; American Headache
Society Pediatric Adolescent Section.
Obesity in pediatric headache population: A multicenter study.
Headache. 2009;49:170177.
17. Robberstad L, Dyb G, Hagen K, Stovner LJ, Holman TL, Zwarts
JA. An unfavorable lifestyle and recurrent
headaches among adolescents. The HUNT study. Neurology.
2010;75:712717.
18. Pinhas-Hamiel O, Frumin K, Gabis L, et al. Headaches in
overweight children and adolescents referred to a
tertiary-care center in Israel. Obesity. 2008;16:659663.
19. Hershey AD, Powers SW, Vockell A. PedMIDAS: Development of
questionnaire to assess disability of
migraine in children. Neurology. 2001;57:20342039.
20. Headache Classification Committee of the International
Headache Society. The international classification of
headache disorders: 2nd edition. Cephalalgia. 2004;24(Suppl.
1):9160.
21. Centers for Disease Control and Prevention. CDC growth
charts.US national center for health statistics.
Available at:
http://www.cdc.gov/nchs/about/major/nhanes/growthcharts/charts.htm
(accessed September 21,
2012).
22. Goldstein A, Haelyon U, Krolic E, Sack J. Comparison of body
weight and height of Israeli schoolchildren with
the Tanner and Centers for Disease Control and Prevention growth
charts. Pediatrics. 2001;108:E108.
23. Ford ES, Li C, Zhao G, Strine TW, Mokdad AH. Body mass index
and headaches: Findings from a national
sample of US adults. Cephalalgia. 2008;28: 12701276.
24. Pakalnis A, Kring D. Chronic daily headache, medication
overuse, and obesity in children and adolescents. J
Child Neurol. 2012;27:577580.
25. Peres MF, Lerario DD, Garrido AB, Zukerman E. Primary
headaches in obese patients.Arq Neuropsiquiatr.
2005;63:931933.
26. Kaplan Y. Effects of obesity on migraine in woman. J Neurol
Sci. 2006;23:295302.
27. Horev A,Wirguin I, Lantsberg L, Ifergane G.Ahigh incidence
of migraine with aura among morbidity obese
woman. Headache. 2005;45:936938.
28. Kinik ST, Alehan F, Erol I, Karna AR. Obesity and pediatric
migraine. Cephalalgia. 2009;30:105109.
29. Verrotti A, Fonzo AD, Agost inelli S, Coppola G, Margiotta
M, Parisi P. Obese children suffer more often from
migraine.Acta Paediatr. 2012;101:416421.
30. Bigal ME, Lipton RB, Holland PR, Goadsby PJ. Obesity,
migraine and chronic migraine. Neurology.
2007;68:18511861.
31. Perini F, D'Andrea G, Galloni A, et al. Plasma cytokine
levels in migraineurs and controls. Headache.
2005;45:926931.
32. Zelissen PM, Koppeschaar HP, Lip CJ, Hackeng WH. Calcitonin
gene-related peptide in human obesity.
-
8/13/2019 Obesity in Children With Headaches - Anak
9/9
Headache. 2013;53(6):954-961. 2013 Blackwell Publishing
Peptides. 1991;12:861863.
33. Holland HR, Akerman S, Goadsby PJ. Orexin 1 receptor
activation attenuates neurogenic dural vasodilatation
in an animal model of trigeminovascular nociception. J Pharmacol
Exp Ther. 2005;315: 13801385.
34. Yunus MB, Arslan S, Aldag JC. Relationship between body mass
index and fibromyalgia features. Scand J
Rheumatol. 2002;31:2731.
35. Deere KC, Clinch J, Holliday K, et al. Obesity is a risk
factor for musculoskeletal pain in adolescents:
Findings from a population-based cohort. Pain.
2012;153:19321938.
36. Anttila P, Sourander A, Metsahonkala L, Aromaa M, Helenius
H, Sillanp M. Psychiatric symptoms in
children with primary headache. JAmAcad Child Adolesc
Psychiatry. 2004;43:412419.
37. Tietjen GE, Peterlin BL, Brandes JL, et al. Depression and
anxiety: Effect on the migraine obesity relationship
Headache. 2007;4:866875.
38. Molarius A, Tegelberg A, Ohrvik J. Socio-economic factors,
life-style, and headache disordersa population-
based study in Sweden. Headache. 2008; 48:14261437.
39. Varkey E, Hagen K, Zwart JA, Linde M. Physical activity and
headache: Results from the Nord- Trondelag
Health Study (HUNT). Cephalalgia. 2008;28:12921297.
40. Van Cauter E, Knutson AL. Sleep and the epidemic of obesity
in children and adults. Eur J Endocrinol.
2008;159:5966.
41. Bigal ME, Tsang A, Loder E, Serrano D, Reed ML, Lipton RB.
Body mass index and episodic headaches.
Arch Intern Med. 2007;167:19641970.
42. Bruni O, Russo PM, Ferri R, Novelli L, Galli F, Guidetty V.
Relationships between headache and sleep in a
non-clinical population of children and adolescents. Sleep Med.
2008;9:542548.