Embed Size (px)
Citation preview
CHHS15/093
Canberra Hospital and Health ServicesClinical GuidelineObesity: Pregnancy, Labour, Birth and Postnatal CareContents
Contents....................................................................................................................................1
Introduction..............................................................................................................................2
Scope........................................................................................................................................ 2
Background............................................................................................................................... 2
Key Objectives...........................................................................................................................2
Section 1 – Management..........................................................................................................3
Pregnancy risks associated with obesity...............................................................................4
Antenatal.......................................................................................................................... 4
Intrapartum.......................................................................................................................4
Postpartum....................................................................................................................... 4
Neonatal............................................................................................................................5
Anaesthetic....................................................................................................................... 5
Section 2 – Procedure...............................................................................................................5
Antenatal.............................................................................................................................. 5
Anaesthetic Management.....................................................................................................7
Intrapartum...........................................................................................................................7
Postpartum........................................................................................................................... 8
Implementation........................................................................................................................ 8
Evaluation................................................................................................................................. 8
Related Policies, Procedures, Guidelines and Legislation.........................................................9
References................................................................................................................................ 9
Definition of Terms...................................................................................................................9
Search Terms.......................................................................................................................... 10
Consultation............................................................................................................................10
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 1 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Introduction
The purpose of this guideline is to outline appropriate management strategies to minimise the clinical risk for women with obesity during pregnancy, labour, birth and the postnatal period.
Back to Table of Contents
Scope
This document applies to: Medical Officers; Registered midwives who are working within their scope of practice (Refer to Scope of
Practice for Nurses and Midwives Policy); Student midwives under direct supervision.
Back to Table of Contents
Background
The staff of the Centenary Hospital for Women & Children supports the philosophy of woman-centred care.
Staff acknowledge the rights of the woman and her family to be involved in the decision–making for all care involving her and her baby. Staff will, at all times and to the best of their ability ensure women are provided with all the information required for them to make an informed decision regarding care.
The woman’s informed decision will be respected and she will continue to receive the highest standard of care, no matter what her choice or decision may be. Staff will also at all times respect the sanctity of birth by ensuring a woman’s right to privacy during each episode of care and especially the woman’s birth space during the birthing process.
Key Objectives
Women with obesity will receive evidence based care.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 2 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Section 1 – Management
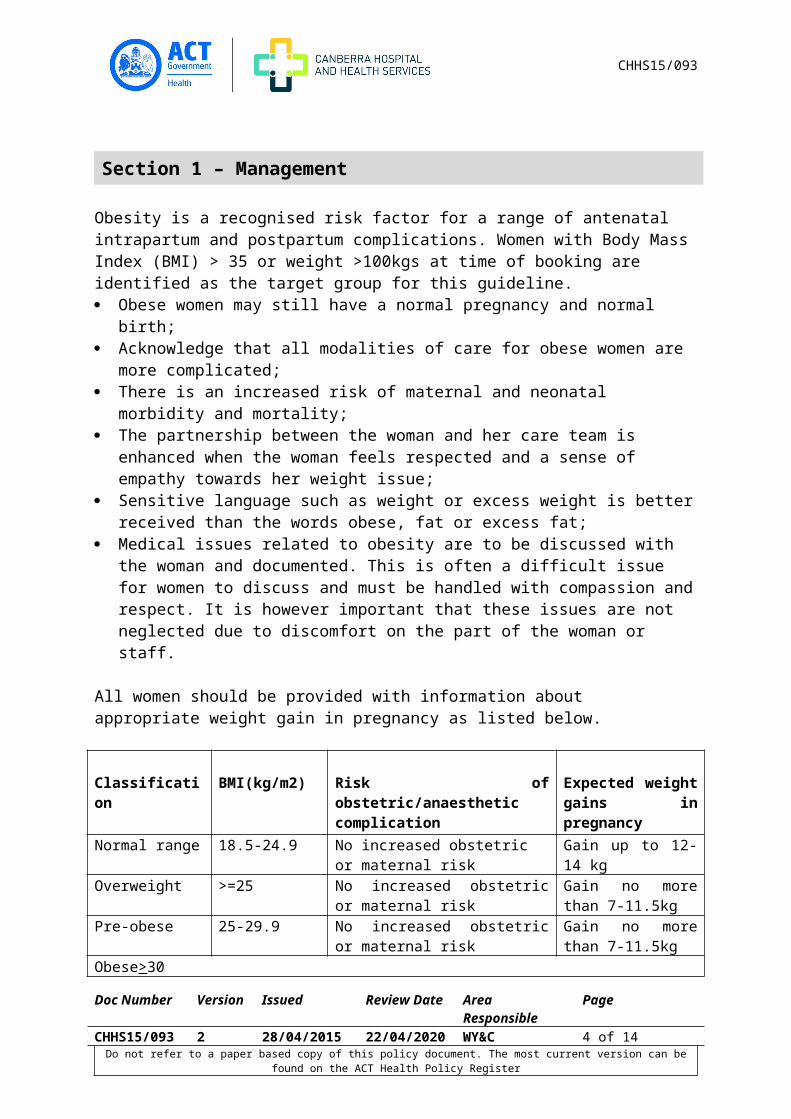
Obesity is a recognised risk factor for a range of antenatal intrapartum and postpartum complications. Women with Body Mass Index (BMI) > 35 or weight >100kgs at time of booking are identified as the target group for this guideline. Obese women may still have a normal pregnancy and normal birth; Acknowledge that all modalities of care for obese women are more complicated; There is an increased risk of maternal and neonatal morbidity and mortality; The partnership between the woman and her care team is enhanced when the woman
feels respected and a sense of empathy towards her weight issue; Sensitive language such as weight or excess weight is better received than the words
obese, fat or excess fat; Medical issues related to obesity are to be discussed with the woman and documented.
This is often a difficult issue for women to discuss and must be handled with compassion and respect. It is however important that these issues are not neglected due to discomfort on the part of the woman or staff.
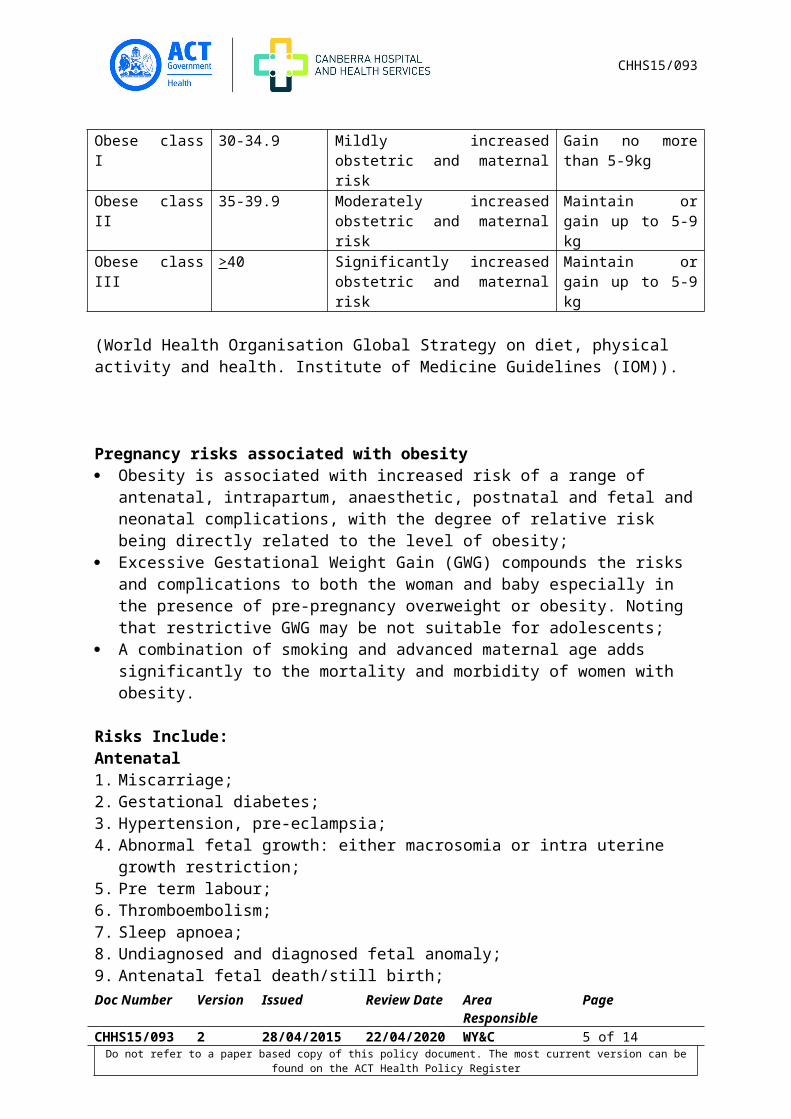
All women should be provided with information about appropriate weight gain in pregnancy as listed below.
Classification BMI(kg/m2) Risk of obstetric/anaesthetic complication
Expected weight gains in pregnancy
Normal range 18.5-24.9 No increased obstetric or maternal risk
Gain up to 12-14 kg
Overweight >=25 No increased obstetric or maternal risk
Gain no more than 7-11.5kg
Pre-obese 25-29.9 No increased obstetric or maternal risk
Gain no more than 7-11.5kg
Obese>30Obese class I 30-34.9 Mildly increased obstetric and
maternal riskGain no more than 5-9kg
Obese class II 35-39.9 Moderately increased obstetric and maternal risk
Maintain or gain up to 5-9 kg
Obese class III >40 Significantly increased obstetric and maternal risk
Maintain or gain up to 5-9 kg
(World Health Organisation Global Strategy on diet, physical activity and health. Institute of Medicine Guidelines (IOM)).
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 3 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Pregnancy risks associated with obesity Obesity is associated with increased risk of a range of antenatal, intrapartum,
anaesthetic, postnatal and fetal and neonatal complications, with the degree of relative risk being directly related to the level of obesity;
Excessive Gestational Weight Gain (GWG) compounds the risks and complications to both the woman and baby especially in the presence of pre-pregnancy overweight or obesity. Noting that restrictive GWG may be not suitable for adolescents;
A combination of smoking and advanced maternal age adds significantly to the mortality and morbidity of women with obesity.
Risks Include:Antenatal1. Miscarriage;2. Gestational diabetes;3. Hypertension, pre-eclampsia;4. Abnormal fetal growth: either macrosomia or intra uterine growth restriction;5. Pre term labour;6. Thromboembolism;7. Sleep apnoea;8. Undiagnosed and diagnosed fetal anomaly;9. Antenatal fetal death/still birth; 10. Increased risk of gastric reflux and associated hiatus hernia;11. Stillbirth.
Intrapartum1. Prolonged /dysfunctional labour;2. Shoulder dystocia;3. Difficulties monitoring the fetus during the ante and intrapartum period;4. Inadequate analgesia;5. Post partum haemorrhage;6. Increased risk of caesarean section and assisted birth;7. Unsuccessful vaginal birth after caesarean section;8. Technically difficult caesarean section with associated increased morbidity and mortality;9. Stillbirth;10. Increased risk of perineal trauma;11. Increased risk of genital and urinary tract infection.
Postpartum1. Wound infection;2. Thrombo-embolic events;3. Postnatal depression;4. Increased breastfeeding difficulties, poor lactation, reduced breast feeding rate;5. Increased nursery admissions;6. Post caesarean birth wound infection.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 4 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Neonatal 1. Increased birth weight/macrosomia;2. Neural tube defects;3. Hypoglycaemia; 4. Meconium aspiration; 5. Child adiposity and diabetes.
AnaestheticThere is an increase in caesarean birth rate among obese women, with associated anaesthetic concerns such as:1. Increased risk of morbidity and mortality for both woman and baby;2. Increased risk of regurgitation and aspiration;3. The position of the woman (since the woman may not be able to lie flat);4. Difficulties with epidurals both for analgesia and anaesthesia at caesarean section;5. Regional anaesthesia for surgery favoured but more difficult to site, unpredictable
spread of local anaesthetics more likely to dislodge or fail;6. Airway maintenance difficult, intubation may be impossible especially in the emergency
setting;7. Oxygenation difficult due to abdominal pressure;8. Non-invasive BP (NIBP) cuffs unreliable may require intra-arterial monitoring.
Back to Table of Contents
Section 2 – Procedure
Antenatal1. Women are offered care through the Bariatric, Multi-disciplinary, Program (BuMP) Clinic;2. All women at their booking visit are provided with information re: appropriate weight
gain in pregnancy, diet and recommend dietician referral;3. Weight management is a discussion that the midwife/medical officer will have with all
women- Women, Youth and Children Community Nutrition will accept referrals for women with maternal obesity;
4. The woman is to be weighed at each visit and her weight documented on her antenatal card;
5. Blood pressure is to be checked with an appropriately sized cuff at each visit. A large cuff with an inflatable bladder covering 80% of the arm circumference should be used if the upper arm circumference is greater than 33 cm. This helps to minimise over-diagnosis of hypertension during pregnancy;
6. Refer woman to physiotherapy;7. Women requiring an elective caesarean section and who have a BMI>35 or weight of
100kgs or more, need to have this information documented on their booking form; 8. Antenatal thromboprophylaxsis is recommended in obese women who require bed rest
for any reason;9. Measure for and apply graduated compression stockings when in labour.
Antenatal Management
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 5 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
BMI > 30 BMI >35 BMI >40 BMI >45Doctors Clinic Refer at 36/40
with growth ultrasound report
Refer at 36/40 with growth ultrasound report
Refer at 36/40 with growth ultrasound report
Obstetric Consultation Not required routinely
Not required routinely
Refer at 20/40
Consultant Care Not required routinely
Not required routinely
Not required routinely
Refer for consultant care
Glucose Tolerance Test (GTT)
Not required routinely
Refer at 16-20/40 or at booking visit. If normal repeat at 26-28/40
Refer at 16-20/40 or at booking visit. If normal repeat at 26-28/40
Refer at 16-20/40 or at booking visit. If normal repeat at 26-28/40
Fetal Medicine Unit (FMU)
Not required routinely
Not required routinely
Refer to FMU for Fetal Morphology at 18-20/40 noting presence of obesity
Refer to FMU for Fetal Morphology at 18-20/40 noting presence of obesity
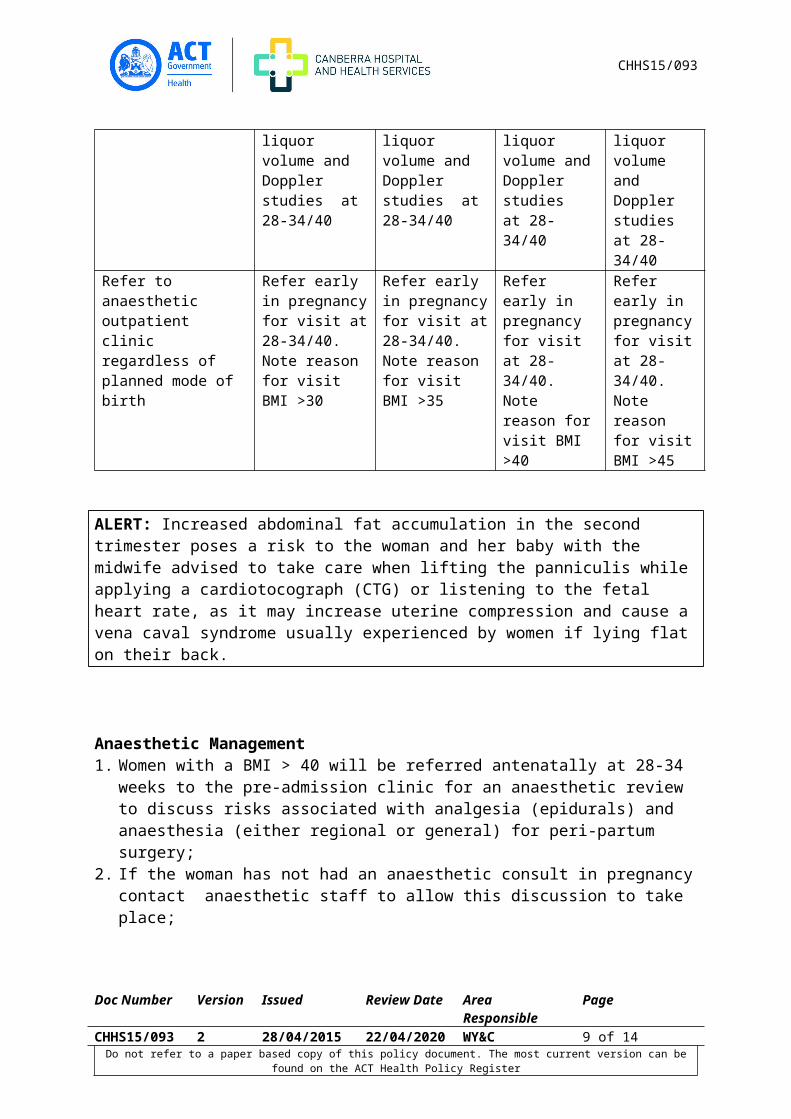
Repeat scan For fetal growth, liquor volume and Doppler studies at 28-34/40
For fetal growth, liquor volume and Doppler studies at 28-34/40
For fetal growth, liquor volume and Doppler studies at 28-34/40
For fetal growth, liquor volume and Doppler studies at 28-34/40
Refer to anaesthetic outpatient clinic regardless of planned mode of birth
Refer early in pregnancy for visit at 28-34/40. Note reason for visit BMI >30
Refer early in pregnancy for visit at 28-34/40. Note reason for visit BMI >35
Refer early in pregnancy for visit at 28-34/40. Note reason for visit BMI >40
Refer early in pregnancy for visit at 28-34/40. Note reason for visit BMI >45
ALERT: Increased abdominal fat accumulation in the second trimester poses a risk to the woman and her baby with the midwife advised to take care when lifting the panniculis while applying a cardiotocograph (CTG) or listening to the fetal heart rate, as it may increase uterine compression and cause a vena caval syndrome usually experienced by women if lying flat on their back.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 6 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Anaesthetic Management1. Women with a BMI > 40 will be referred antenatally at 28-34 weeks to the pre-admission
clinic for an anaesthetic review to discuss risks associated with analgesia (epidurals) and anaesthesia (either regional or general) for peri-partum surgery;
2. If the woman has not had an anaesthetic consult in pregnancy contact anaesthetic staff to allow this discussion to take place;
3. If the woman needs to be transferred to the operating theatre, the theatre staff should be given as much notice as possible in order for them to prepare appropriate equipment.
4. When a woman with a BMI >40 is admitted the anaesthetic staff should be notified of her admission and the anaesthetic plan reviewed;
Alert:Manual handling considerationsComplete manual handling assessment to ensure correct equipment is available and used include issues such as:
Positioning and moving the woman safely The safe use of equipment such as:
o Lithotomy stirrupso Operating table
Appropriately sized equipmento Trolleyo Bedo Wheel chairo Commode seating
As per ACT Health Manual Handling Policy.
Where a woman is 100kg or more, or at staff request, a hover mat will be used to assist in the transfer. Placement of the hover mat prior to epidural procedure is mandatory.
Note: Maximum weight equipment is: Theatre Trolley =200kgBirth Suite Bed (Affiniti 1127 kg)Usual Hospital Bed: up to 250kgBariatric Bed >250kg if the woman is unable to roll comfortably in the usual hospital bed.
Intrapartum1. Careful thought needs to be given to an induction of labour for any woman with a BMI
>35 as the best possible outcome for women with BMI > 30 is to labour spontaneously and to have a normal birth;
2. The active phase of labour can be increased from a median of 6.2 hours in the normal range BMI to 7.9 in BMI > 30;
3. Women in the Obese II classification are at significantly higher risk of assisted births including caesarean birth;
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 7 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/093
4. For women undergoing elective caesarean birth their weight (kg) should be recorded on the booking form for the operating theatre to be aware to have appropriate equipment available if possible;
5. For women with a BMI>40 in labour an IV cannula should be inserted early in labour and blood taken for group and hold and FBC;
6. There is no requirement for continuous fetal monitoring based on weight alone, however if there are indications for electronic fetal monitoring a scalp electrode may improve the recording;
7. Assess pressure areas and maintain skin integrity. If decreased mobility check pressure areas 2hrly and document findings.
Postpartum1. Consider transferring back to the peripheral hospital if the woman has no other
complications after the birth;2. Early mobilisation;3. Venous thromboembolism prophylaxis (VTE) should be given to all women with high BMI
after a caesarean birth and considered after a vaginal birth if there are any other VTE risk factors;
4. Ensure vigilance regarding the signs of a secondary postpartum haemorrhage;5. Involution of the uterus may be difficult to palpate therefore vigilant monitoring of blood
loss is essential; 6. Obese women are to be encouraged to breastfeed which will enhance weight loss and
reduce the likelihood of childhood obesity in the baby.
Implementation
This guideline will be: discussed at maternity in-service education; discussed at maternity multidisciplinary education; placed on notice boards in tea and work rooms; distributed to maternity staff via email.
Back to Table of Contents
References
Australian College of Midwives Inc. 2008. National Midwifery Guidelines for Consultation and Referral. ACT Australia. Avail at http://www.midwives.org.au
CEMACH. 2007. Saving Mothers Lives: Reviewing maternal deaths to make motherhood safer 2003-2005. UK
Datford and Gravesham NHS trust 2009. Obesity in Pregnancy Guidelines. UK
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 8 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Groth, S. (2007) Are the institute of Medicine Recommendations for Gestational Weight Gain Appropriate for Adolescents? JOGNN Clinical Research
Guelinckx, I, Devlieger, R., Beckers, K. & Vansant, G. (2007).Maternal Obesity: Pregnancy
Morin, H & Reilly L. Caring for Obese Pregnant Women. JOGNN Sept/Oct 2007 Vol 36, No 5. pp 482-489.
National Institute for Health and Clinical Excellence. 2014. Intrapartum care guidelines. Avail at http://www.nice.org.uk/
National Institute for Health and Clinical Excellence. 2008. Antenatal care guidelines.Avail at http://www.nice.org.uk/
World Health Organisation Global Strategy on diet, physical activity and health.Downloaded from http://www.who.int/dietphysicalactivity/childhood_what/en/ on 18.2.2011
Back to Table of Contents
Definition of Terms
Panniculis: a dense layer of fatty tissue growth, consisting of subcutaneous fat in the lower abdominal area.
Macrosomia: The term macrosomia is used to describe a newborn with an excessive birth weight. Neonatal macrosomia has been defined in several different ways, including birth weight of 4000-4500 g or greater than 90% for gestational age after correcting for neonatal sex and ethnicity. Based on these definitions, macrosomia affects 1-10% of all pregnancies.
Back to Table of Contents
Search Terms
Bariatric womanObese woman Overweight womanObesity in pregnancyObesity in labourObesity and birthing
Back to Table of Contents
Consultation
Name/position/ Feedback Feedback Comment
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 9 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS15/093
Division of person(s) consulted
ReceivedYes/No
incorporatedYes/No
Jacky DobsonPharmacy TeamLeader for WY&C
Yes Yes
Deborah DavisProfessor ofMidwifery
Yes Yes
Pip GolleyNutrition ManagerCommunity Health
Yes Yes
Madeline ClarkSocial Work
Yes Yes
Lynelle BoisseauDiabetes Educator
No comments
Back to Table of Contents
Disclaimer: This document has been developed by Health Directorate, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and Health Directorate assumes no responsibility whatsoever.
Date Amended Section Amended Approved By15 December 2015
Doc Number Version Issued Review Date Area Responsible PageCHHS15/093 2 28/04/2015 22/04/2020 WY&C 10 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register





























